
Abstract
Tracheoesophageal puncture with voice prosthesis placement is used to restore vocal function after total laryngectomy. However, closure of the fistula is sometimes needed. At our department, a simple and effective technique for closure was developed. It does not require interposed tissues or materials. Moreover, our procedure allows for a short rehabilitation time for swallowing and a short hospitalization. We describe advantages, pitfalls, and errors to avoid. This technique should not be performed for patients who are irradiated and those with large fistulas.
The placement of a voice prosthesis after a tracheoesophageal puncture (TEP) is one possibility to restore vocal function after total laryngectomy. 1 However, TEP closure may be needed in some cases. In particular, it becomes mandatory when complications occur that are not solvable with conservative treatment (ie, periprosthetic leak, recurrent granulation tissue, dilatation of a TEP). 2 Moreover, some patients do not use the voice prosthesis, and they ask the surgeon to remove it.
Different surgical techniques have been described, most of them with tissues or synthetic materials interposed between the esophagus and trachea.3-5 The majority of these treatments require extensive and demolitive surgery.
At our department, we developed a simple and effective technique for TEP closure that does not require interposed tissues or materials. It allows for a short rehabilitation time for swallowing and a short hospitalization. Written informed consent was obtained by every patient. Institutional review board (Santa Croce Hospital of Moncalieri) approval was obtained.
Surgical Technique
The procedure is performed under general anesthesia with tracheal intubation, even if local anesthesia with profound sedation can be used for selected patients and those with a high risk related to general anesthesia.
An endotracheal tube is inserted into the esophagus to allow its identification during the entire procedure. The voice prosthesis is removed. Four cardinal points are used to pull the tracheal opening of the fistula outward ( Figure 1A ). Then a semicircular incision immediately above the TEP is performed from 9 to 3 o’clock to increase the protrusion and to obtain more tissue for the suture of the TEP tracheal opening ( Figure 1B ). This incision should not cut the fistula. Tracheal protrusion of the fistula is mandatory to avoid injuries to the esophageal mucosa that may lead to esophageal stenosis. After freshening of the fistula with near total removal of the mucosa inside it, the fistulous route is identified with a blunt instrument ( Figure 1C ). The rigid instrument allows performance of a circular suture around the fistula without resecting it ( Figure 1D ).
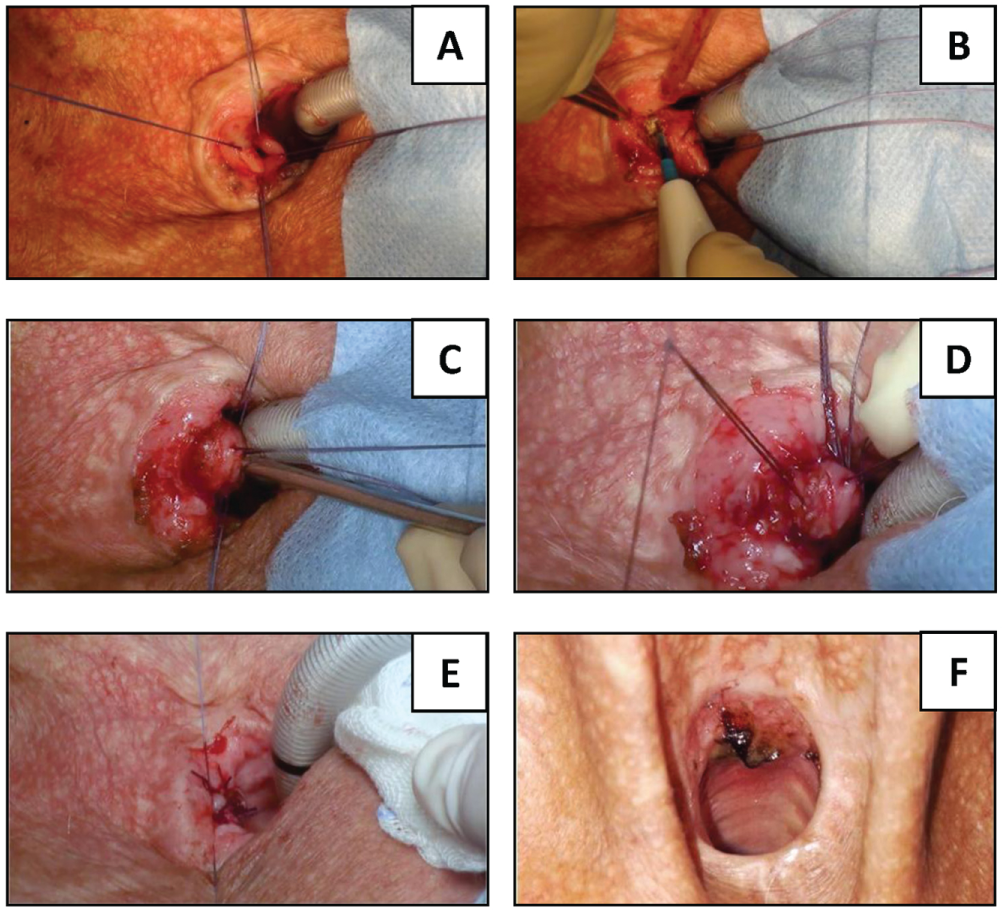
(A) Four cardinal points. (B) Semicircular incision. (C) Blunt instrument in the fistula. (D) Circular suture. (E) Suture of incision and tracheal opening of the fistula. (F) Postoperative result: 48 hours. The head is on the left side of panels A-E.
A 5/8th needle is used with nonabsorbable wire (ie, silk) to reduce the risk of failure. The blunt instrument is then removed from the TEP, and the circular suture is tightened. The tracheal protrusion of the fistula allows better identification of the fistulous route, with the possibility to perform the circular suture without going too deep and damaging the esophagus. During performance of the circular suture around the fistula, the needle should not stay attached to the blunt instrument but at 1 to 2 mm from it, to obtain a correct suture all around the fistula. The superior semicircular incision and the tracheal opening of the fistula are sutured with cross stitches ( Figure 1E ). The esophageal tube is removed. The main steps are highlighted in Figure 2 .
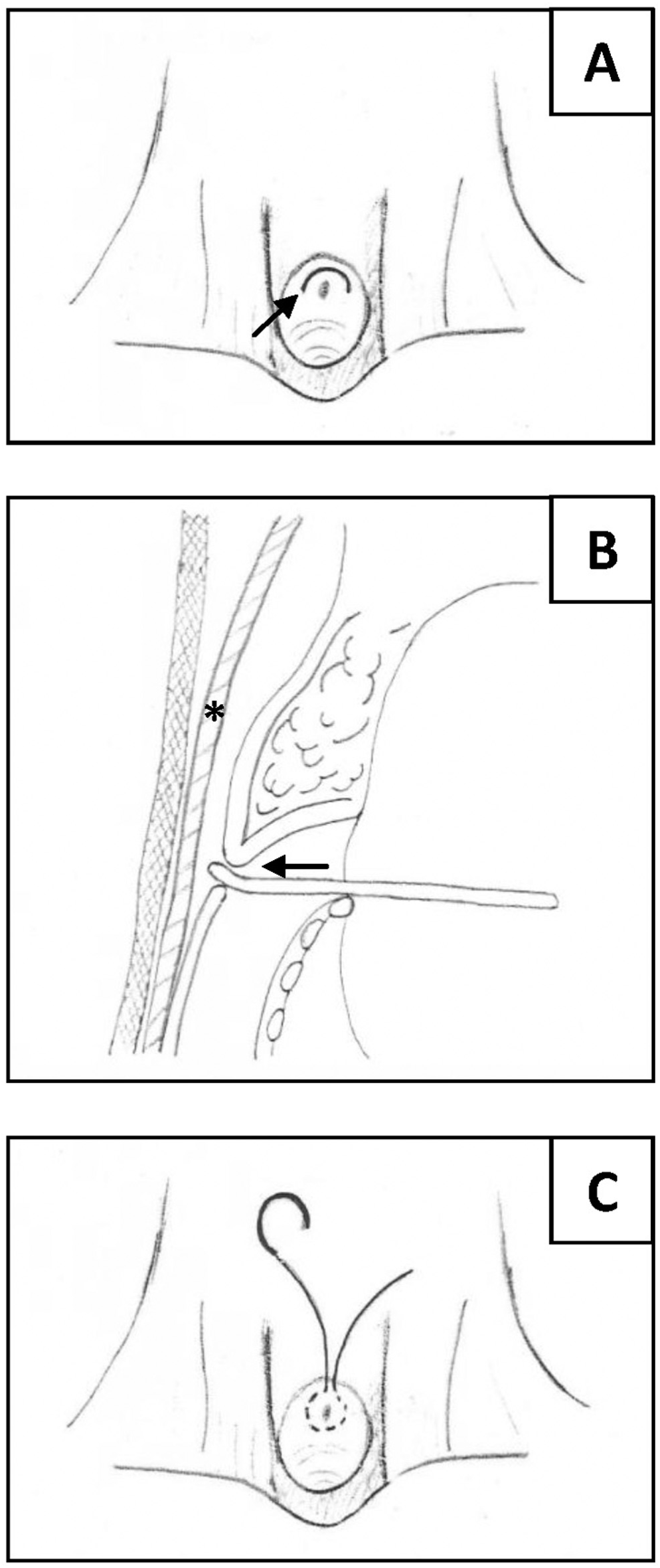
(A) Semicircular incision above the tracheoesophageal puncture (arrow). (B) The fistulous route is identified with a blunt instrument (arrow). Asterisk: endotracheal tube in the esophagus. (C) Circular suture around the fistula with a 5/8th needle.
Swallowing attempts with liquid are started after 24 hours. In case of success, a diet with soft foods is immediately started. Figure 1F shows postoperative results after 48 hours. In the absence of complications, the patient is discharged after 48 hours. Severe crusting is gently removed before hospital discharge to avoid inhalation. Hard solid foods are reintroduced after 7 days. Postoperative pain is adequately controlled with acetaminophen.
Discussion
The closure of a TEP represents a difficult procedure with the risk of failure. TEP closure is required for periprosthetic leak due to enlargement of the TEP or when the patient no longer wishes to continue voice production with the prosthesis. 2 Other than transposition of the tracheostomy, 2 types of surgical techniques for TEP closure have been described:
With the interposition of tissues or synthetic materials between the esophagus and trachea (ie, sternocleidomastoideus muscle flap, sternocleidomastoideus fascia flap, deltopectoral flap, radial free forearm flap, Vicryl mesh)3,4
Without the interposition of tissues or synthetic materials between the esophagus and trachea 5
The main limits of techniques with interposition of tissues are the reduction of tracheal and esophageal lumen by the bulky flap and the high morbidity of such interventions. These techniques, with local or distant tissue interposition, may be useful for patients who are irradiated, where a higher risk of failure of the TEP closure is present.
In 2001, Hosal and Meyer proposed a technique without the interposition of tissues. The fistula was divided, and the esophageal mucosa was closed with inverted sutures. The tracheal mucosa was closed with everted sutures. 5 However, it requires a peristomal skin incision and a multilayer closure of the resected fistula. On the contrary, our surgical intervention consists of a smaller mucosal incision immediately above the TEP, without cutting it. Therefore, it can be performed in a short time. Moreover, by operating near the tracheal wall, there are low risks for esophageal complications.
Between 2017 and 2018, 4 men and 1 woman (range, 55-71 years) with TEP in previous total laryngectomy underwent our procedure for fistula closure. Four patients required the removal of the voice prosthesis because of absent use. One patient who was irradiated had an enlargement of the fistula (7 mm, diameter) with risk of prosthesis inhalation. No postoperative bleeding and pulmonary complications occurred. The closure of the fistula did not show increased tension. Fistula reopening occurred after 4 days in 1 patient who was irradiated. Therefore, the definitive closure of the TEP with swallowing restoration was achieved in 80% of cases. Excluding the irradiated case, all interventions were successful. No patient had postoperative esophageal stenosis at a follow-up of 8 months.
In conclusion, our technique for TEP closure after total laryngectomy is a safe and effective procedure with a low risk of failure, a short operative time and hospital stay, and early swallowing restoration. Patients should be appropriately selected to obtain a lower failure rate versus other techniques. In particular, patients who are irradiated are more at risk of failure and should undergo surgery with interposition of tissues. Patients with large fistulas (>7 mm) are not candidates for our technique. Therefore, the size limitation represents a limit of our technique. The procedure may be difficult for patients with stenosis of the tracheostoma. Further studies with a greater sample are needed to confirm our encouraging results.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.