
Abstract
Objective
There is no consensus on the follow-up modalities in patients with head and neck cancer. This study aims to describe the pattern and survival outcomes of recurrences/second primary cancers in patients undergoing an intensive radiologic and clinical follow-up.
Study Design
Retrospective analysis.
Setting
Single academic tertiary care center.
Subjects and Methods
All patients with stage III-IV head and neck cancer treated with chemoradiotherapy at our institution between 1998 and 2010 were retrospectively reviewed. Persistent/recurrent disease within 6 months since the curative treatment and second primary cancers outside the upper aerodigestive tract were excluded. Data were analyzed by descriptive statistics. Surveillance was planned every 3 months in the first year, then with increasing intervals till the fifth year.
Results
A total of 326 patients were included. Out of all detected cancer recurrences (n = 106, 32%), 38 (36%) were locoregional, 44 (41%) were distant, and 24 (23%) were second primary cancers. Approximately 70% of recurrences were clinically and/or radiologically discovered, while 30% were diagnosed due to the patients’ symptoms. Of all clinically and/or radiologically discovered recurrences/second primary cancers (n = 74), 26 (35%) were curatively treated, with respect to 9 of the 32 (28%) diagnosed by symptoms. Median overall survival of recurrent curable cases did not significantly differ according to the detection modality (89 months by clinical/radiologic examination vs 85 by symptoms).
Conclusions
Clinical and radiologic follow-up identified more recurrences/second primary cancers than the symptom-driven monitoring, but the curability of cancer recurrence was similar regardless of detection modality. Prospective trials are needed to define the most effective follow-up strategy in head and neck cancer.
Concurrent cisplatin-based chemoradiation is the standard therapy for patients with locally advanced head and neck cancer (HNC), either as exclusive treatment or with adjuvant intent in patients with high-risk pathologic findings.1,2
After receiving curative treatment, patients initiate a follow-up program to timely detect any disease recurrences or second primary cancers (SPCs) to favor the feasibility and effectiveness of a salvage treatment. Surveillance programs are also useful to evaluate long-term treatment-related side effects, restore the nutritional status, and monitor the psychosocial status and the rehabilitation process.3-8
With advances of primary treatment techniques and the human papilloma virus (HPV)–related epidemiologic changes in HNC, we have witnessed increasing survival figures and more and more patients included in follow-up programs. To facilitate a rational allocation of resources, it is necessary to prove the clinical utility of health care procedures involving those included in follow-up programs. 9
Routine radiologic surveillance is supposed to have limited influence on survival.10-15 In the HNC setting, some conflicting retrospective studies have been published; therefore, various surveillance regimens and radiologic imaging have been investigated for routine follow-up.3-8,16,17 Guidelines by the National Comprehensive Cancer Network suggest frequent physical examinations and 1 radiologic assessment of the head and neck area within 6 months since completion of treatment, while further imaging is not routinely recommended for patients who are asymptomatic. 18
The UK national multidisciplinary guidelines recommend frequent physical examinations, while imaging is indicated only when a recurrence is suspected. 19
However, due to the absence of well-conducted trials, no uniform approach is applied for follow-up in patients with HNC. In our institution, the follow-up program was more intensive as compared with current guidelines. Therefore, we conducted a retrospective analysis of the follow-up program for patients with HNC treated at our institution to describe the pattern of diagnosis and associated treatments provided to patients with recurrences/SPCs detected by an intensive clinical/radiologic follow-up program. Moreover, we investigated the association between modality of recurrence/SPC discovery and clinical outcomes.
Subjects and Methods
Study Setting and Design
This retrospective study was conducted at the Fondazione IRCCS Istituto Nazionale Tumori (Milan, Italy) and approved by the internal ethical committee.
Medical charts were reviewed of all patients treated between 1998 and 2010 for stage III or IV (American Joint Committee on Cancer TNM classification, fifth and sixth editions) histologically confirmed nonglandular epithelial carcinoma of the oral cavity, oropharynx, larynx, hypopharynx, nasopharynx, and paranasal sinus.
We included all patients treated with curative or postoperative chemoradiotherapy and without evidence of disease 6 months after treatment completion, as evaluated through radiologic imaging performed according to clinical practice at that time. For each patient, we collected demographic data, stage at diagnosis, recurrence, date and site of relapse/SPC, salvage and palliative treatments, outcome, and date of last follow-up. We included only SPCs arising in the upper aerodigestive tract and lung due to their possible common risk factors with HNC.
HPV status was determined in oropharyngeal squamous cell carcinomas by p16 expression (>50% of cells showing strong nuclear and cytoplasmic immune labeling) 20 ; in p16-positive cases, HPV DNA in situ hybridization 21 and/or E6/7 mRNA expression was performed to confirm the positivity. 22 A case was considered HPV positive if there was concordance between determinations. All nasopharyngeal cases were assessed for Epstein-Barr-encoded small RNAs in the tumor specimen.
Follow-up Plan
According to our institutional guidelines at that time, the follow-up plan for patients with HNC, independently from the specific subsite, consisted of ear, nose, and throat (ENT) examination by white light endoscopy every 3 months for the first year after treatment completion, every 4 to 6 months from the second to the fourth year, then once in the fifth year. Patients missing a scheduled visit were regularly contacted (by phone call), and a new appointment was rescheduled. A locoregional radiologic evaluation was performed with a magnetic resonance imaging (MRI) or computed tomography (CT) scan at least twice yearly for the first 2 years and yearly in the following 2 years. A whole-body CT scan was performed yearly during the first 5 years since treatment completion.
Since 2006, a positron emission tomography (PET) scan was routinely introduced in local practice and included in the follow-up plan as an alternative to CT scan. Furthermore, all patients with oral cavity cancer with clinically and radiologically negative lymph nodes were treated according to depth of invasion of their radically resected primary tumors. In fact, elective neck dissection was performed with invasion >3 mm and a strict ultrasound-based follow-up with invasion ≤3 mm.
The total duration of follow-up with outpatient visits was limited to the first 5 years after treatment completion; after that, patients were referred to the general practitioner and informed about signs and/or symptoms that should prompt to ask for a specialist visit.
Data Handling
Tumor relapses and identification of second tumors were analyzed and divided between clinically (by ENT examination) and/or radiologically detected cases and patient-detected cases (ie, those in which patients were symptomatic at a scheduled appointment or had self-referred themselves to the clinic because of self-perceived symptoms).
We analyzed cases according to the site of recurrence (locoregional relapse or distant metastases) or SPC. Patients with local or regional recurrence and a metastatic relapse were considered in the distant metastasis group.
In case of a single pulmonary lesion, a biopsy was performed, and TP53 mutational status, Epstein-Barr-encoded small RNA, and HPV status were compared with the primary tumor to distinguish between metastases and primary lung cancer.
We divided the series according to the treatment intent (curative vs palliative) among locoregional recurrences and SPCs.
Data Analysis
The main aims of the study were to describe the following:
Site and timing of recurrence/SPC within an intensive follow-up program
Outcomes in patients diagnosed with a recurrence/SPC according to the modality of discovery
Modality of detection of relapse/SPC in patients treated with a curative intent for relapse/SPC and their outcome
Data were analyzed by descriptive statistics: Fisher’s exact test was used to detect association between characteristics and a nonparametric K-sample test for the equality of medians.
Furthermore, overall survival (OS) of the patients, defined as time from the end of treatment to death or last follow-up, was evaluated by Kaplan-Meier analysis, and log-rank test was used to identify differences in the survival curves of different groups. Data were processed with Stata 13 (StataCorp, College Station, Texas).
Results
Patient Population
A total of 326 patients were included (245 men, 75%; median age, 58 years; range, 22-83 years; Table 1 ). Oropharynx was the most prevalent subsite (n = 104, 32%). Of these subjects, 58 patients were HPV positive (56%). In total, 72 (22%) patients had stage III disease and 254 (78%) stage IV.
Patient Characteristics (N = 326).
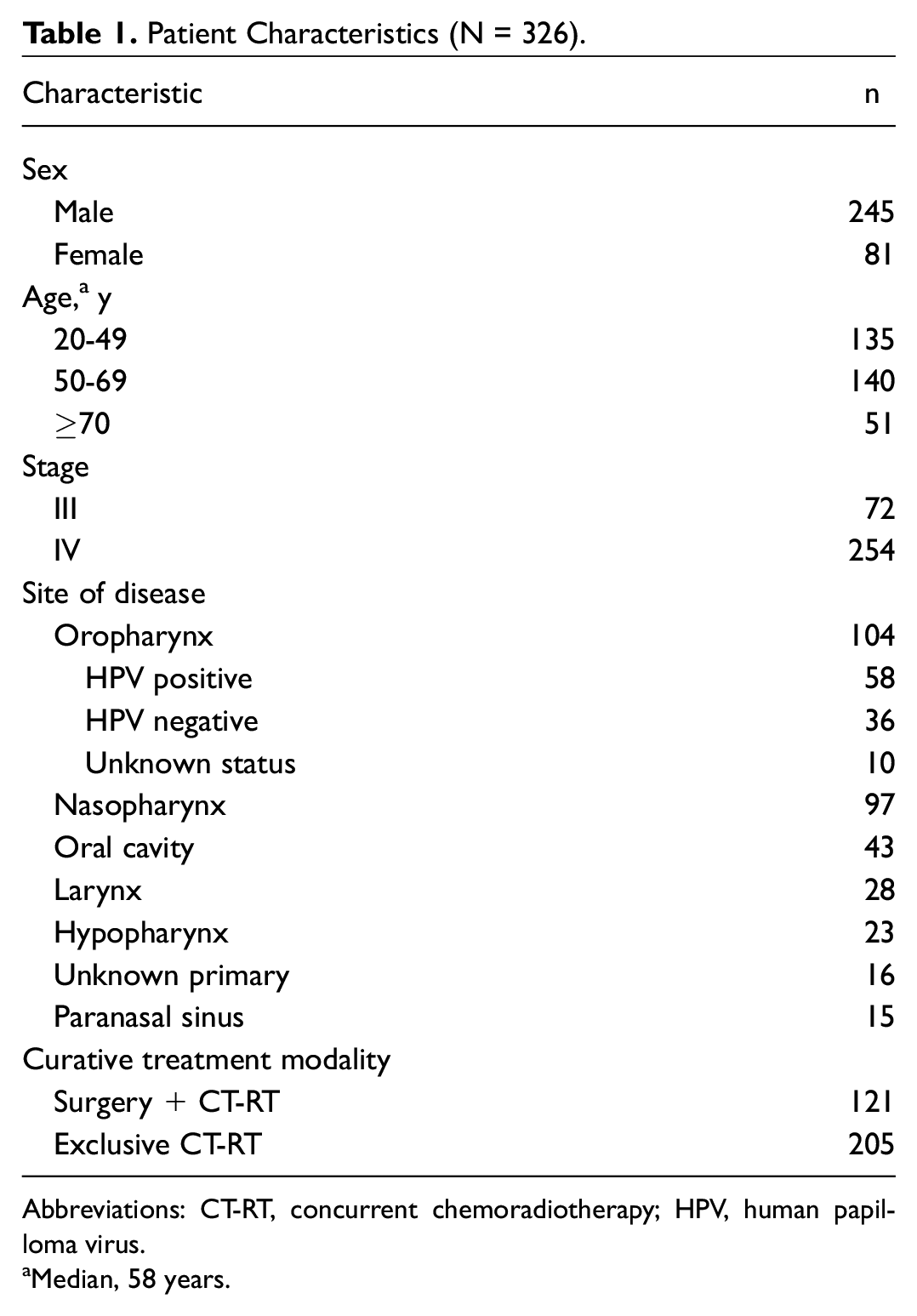
Abbreviations: CT-RT, concurrent chemoradiotherapy; HPV, human papilloma virus.
Median, 58 years.
Treatment and Response Outcomes
Concurrent radiation therapy and platinum-based chemotherapy were used as curative treatment for 205 patients (63%), while 121 patients (37%) were treated with surgery, followed by adjuvant chemoradiotherapy.
In total, 106 patients (32%) were diagnosed with a recurrence or a second primary tumor. Specifically, 38 of 106 (36%) cases presented locoregional recurrences and 44 (41%) distant metastases. Median time to locoregional recurrence was 14 months (range, 6-79), and 84% (32 of 38) were diagnosed in the first 3 years of follow-up. Until December 2005, when PET was occasionally prescribed, 13 patients were diagnosed with a recurrence. Of these, 8 (62%) were diagnosed because of symptoms occurrence, while for 5 (38%) diagnosis was made by scheduled clinical and/or radiologic examinations (1 by ENT examination and 4 by radiologic examinations other than PET).
From 2006 to 2011, 93 recurrences/SPCs were identified. In this period, occurrence of symptoms led to diagnosis in 24 cases (26%), while in 69 (74%) cases, clinical and/or radiologic scheduled follow-up led to diagnosis of recurrences/SPCs, with PET being the most diagnostic examination (8 by ENT, 33 by PET, and 28 by other radiologic examinations).
In total, 24 (23%) patients were diagnosed with SPC: 13 lung cancer, 8 HNC, and 3 esophageal cancer. Median time to second tumor detection was 30.5 months (range, 6-109), and 14 (58%) were detected in the first 3 years.
Patient versus Clinical/Radiologic Detection
The global number of visits performed to all patients was 2520. In total, 70% (74 of 106) of all relapses/SPCs was detected by ENT and/or radiologic examination, whereas 30% (32 of 106) were self-detected by patients.
In 9% of the relapsing cases (10 of 106), the ENT examination was the first examination leading to diagnosis; the observed detection rate—defined as the number of ENT visits performed to detect relapse or SPC—was 0.5% (1 of 200).
Out of 32 self-detected cases, only 13 (41%) had available data about the type of symptoms. All of them were related to cancer recurrence, and 77% (10 of 13) led patients to an earlier visit and the diagnosis of relapse. Pain (54%), dyspnea (23%), dysphagia (15%), and growth of an asymptomatic lump on the neck (8%) were reported. Out of 74 recurrences/SPCs discovered by clinical and/or radiologic follow-up, 26 (35%) were treated with curative intent. Of the 32 patients in which symptoms led to diagnosis, 9 (28%) were treated with curative intent.
When the analysis was restricted to the group of locoregional recurrences (n = 38), we did not observe differences in curability rates according to modality of detection. In fact, of the 24 locoregional recurrences identified by clinical/radiologic follow-up, 14 (58%) were treated with curative intent, while of the 14 identified by symptoms, 7 of 13 (54%) received a curative approach (1 patient refused treatment).
With regard to the 24 SPCs, a slightly higher number of cases discovered by clinical/radiologic follow-up was curatively retreated (8 of 17, 47%) as compared with those found by symptoms (2 of 7, 29%).
Treatment after Recurrence/SPC Diagnosis
Among the 38 patients who were diagnosed with a locoregional recurrence, 21 underwent a salvage treatment (reirradiation in 5 patients, surgery in 16), while 17 underwent palliative chemotherapy or best supportive care. In 14 of 21 patients who received a salvage treatment (66%), diagnosis of potentially curable relapse was made by clinical-radiologic follow-up, with PET being the most diagnostic examination (n = 7), followed by MRI (n = 5) and ENT (n = 2). Pattern of detection and characteristics of locoregional recurrences treated with potentially curative intent are shown in Table 2 . No significant association was found between the groups regarding all the characteristics analyzed.
Pattern of Detection and Characteristics of Cancer Recurrences in Patients Treated with Potentially Curative Intent.
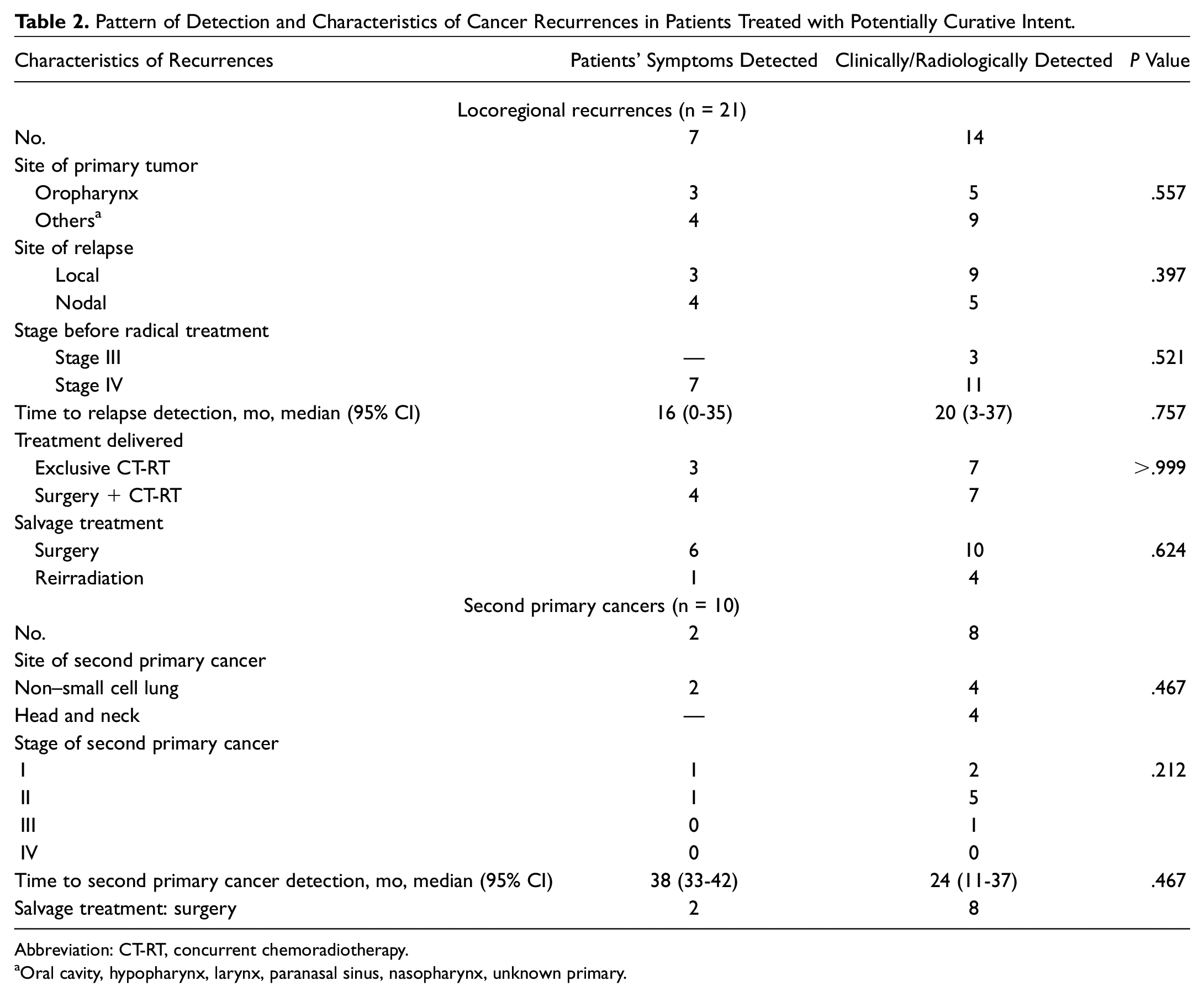
Abbreviation: CT-RT, concurrent chemoradiotherapy.
Oral cavity, hypopharynx, larynx, paranasal sinus, nasopharynx, unknown primary.
Out of the 24 patients diagnosed with an SPC, 10 (42%) were treated with a potentially curative intent. In 8 of 10 (80%) cases, diagnosis was made by clinical-radiologic follow-up, with PET being the most informative examination (4 patients), followed by CT scan (n = 2) and ENT (n = 2). Pattern of detection and characteristics of SPC treated with potentially curative intent are shown in Table 2 .
Among the 44 patients with distant relapses, only 2, who had been treated for HPV-positive oropharyngeal carcinoma, were eligible for a potentially curative resection of a single lung lesion, which was also assessed to be HPV positive. In both cases, diagnosis was made by radiologic follow-up. Overall, in 32 cases (72%), metastases were detected by clinical-radiologic follow-up: diagnosis was made more frequently with PET (16 patients), followed by CT scan (n = 13), MRI (n = 2), and ENT (n = 1).
Survival
Median OS of the whole group of patients with relapse/SPC was 46 months (95% CI, 39-72), 54 months (32-89) in case of locoregional recurrence, 37 months (21-47) with distant relapse, and 84 months (46-124) with SPC. For all patients with locoregional relapse/SPC, median OS was 74 months (95% CI, 43-85), but it was 54 months (28-110) versus 74 months (43-111) in the symptom-driven cohort versus the clinically/radiologically detected group, respectively (P = .5787). Among only those patients with locoregional relapse/SPC treated with a curative intent, OS did not differ according to the type of detection: the median OS was 85 months (5-year OS, 73.5%; 95% CI, 28%-93%) in the symptom-driven group versus 89 months (5-year OS, 61.3%; 95% CI, 37%-78%) in the clinically/radiologically detected 1 ( Figure 1 ; P = .7203).
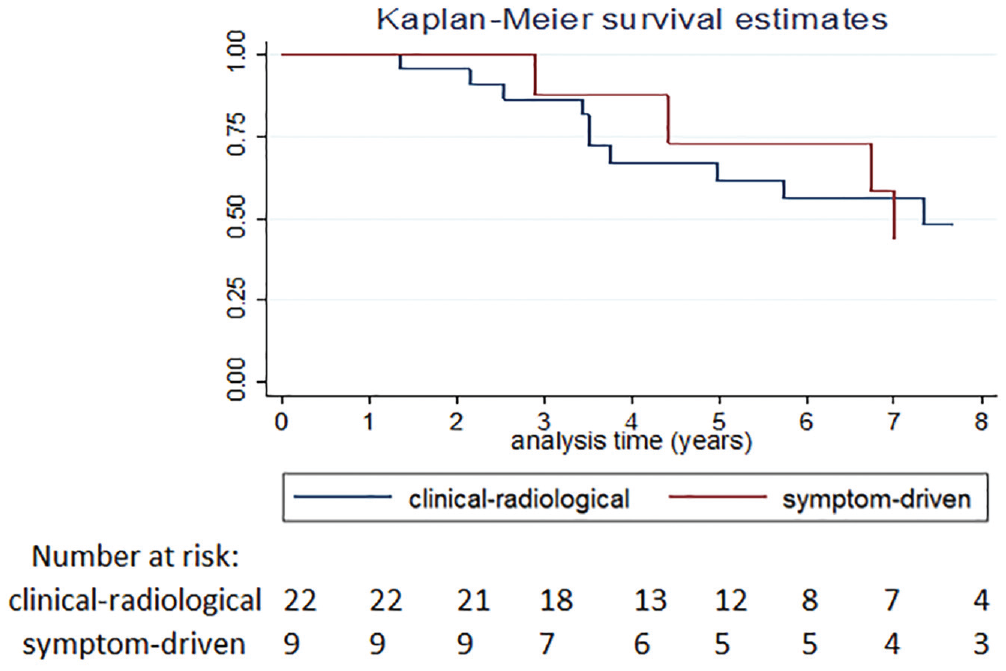
Kaplan-Meier survival analysis of patients with a diagnosis of locoregional recurrence or second primary cancers (treated with curative intent) according to the type of detection (by clinical/radiologic examinations or by patients’ symptoms).
These findings were similar when the analyses were conducted only with patients with locoregional recurrences (P ≥ .1) or SPC (P ≥ .1).
Discussion
In this monoinstitutional series considering the follow-up of patients with locally advanced HNC, when the diagnosis of recurrence was made through clinical and radiologic follow-up or because of the symptoms’ appearance, there was no difference in the rate of patients treated with a curative intent (35% and 28%, respectively). It differed only in patients found with an SPC: more cases were diagnosed by clinical/radiologic follow-up (47% vs 29% discovered by symptoms, P = .6).
However, regarding the global number of recurrent cases with curative treatment, clinical and/or radiologic examinations allowed us to discover a higher number of relapses and therefore more potentially curable diseases. Notwithstanding the possible early diagnosis, this did not translate to a survival benefit.
Usefulness of routine follow-up after curative treatment is a hot topic in oncology, also representing one of the most recommended aims of the Choosing Wisely campaign. 22 This initiative is focused on curbing the common use of diagnostic/staging examinations or unnecessary treatments to a certain clinical situation that are not supported by sufficient evidence. 22
Several studies (mostly retrospective) in HNC have tried to investigate the actual utility of follow-up programs aimed at assessing the frequency of recurrences in patients who had undergone strict surveillance versus those on less intensive programs, sometimes also evaluating the outcomes of the 2 groups. Methods and timing of follow-up among these studies were similar and mainly based on clinical examination, more frequent in the first 2 years and covering a total duration of 5 years. In some studies, an annual chest radiograph was used to diagnose distant metastases and/or pulmonary second tumors, while no trial has investigated a more modern radiologic strategy with CT, MRI, and/or PET scan.3-8,16,17,23-25
Overall, no study has ever shown any benefit of surveillance strategies, with the exception of the analysis by de Visscher et al, 6 which was affected by a lead time bias, however. All other studies did not confirm this trend, reporting the absence of survival difference between patients whose recurrence was detected by new signs/symptoms and by clinical examination.5,17,23-25
In clinical practice, no standardized follow-up strategy has been broadly defined with respect to timing and type of radiologic and clinical visits. This inconsistency is also witnessed by the large variability of existing practices.23,26-28
Patients with locally advanced HNC are at high risk of locoregional recurrences, the majority during the first 3 years after treatment and the main cause of mortality in this period.5,6,8,29 These patients are also at higher risk of developing an SPC, with a major impact on survival.23,30
Therefore, the importance of early detection and treatment of locoregional recurrences or SPCs is paramount. However, to date, surveillance programs were not able to improve outcomes in HNC. One could alternatively argue that the potential of surveillance programs has not been fully explored and that the follow-up programs were limited by insufficient or outdated surveillance techniques and/or inadequate follow-up frequency.
In fact, while some sites, such as the oral cavity, are easily investigated by physical examination, other anatomic regions (eg, paranasal sinuses, skull base, laryngeal ventricles, and subglottis) are particularly difficult to evaluate. Furthermore, recurrent carcinomas do not often present as exophytic or ulcerated tumors, but they may be hidden beneath an intact edematous mucosa, especially in previously resected and/or reconstructed and/or irradiated cases. Thus, theoretically, the early detection of locoregional relapses could be improved by regular preplanned CT or MRI of head and neck area.
Data of our retrospective analysis regarding median time of locoregional recurrence (14 months), rates of relapse in the first 3 years (84%), SPC incidence (3 cases per 100 patients/year), and rate of potentially curable locoregional recurrences/SPCs (n = 31, 29%) are consistent with prior data.5,7,8,17,29-33
In our series, we did not find any difference in survival between patients whose recurrence was “self-diagnosed” and those asymptomatic patients in which diagnosis was detected by an intensive follow-up. There are several reasons that may explain this lack of survival benefit. First, although discovered in a potentially curable stage, any relapse or SPC has a more aggressive behavior than the primary tumor. The lack of survival improvement could also be due to the poor stratification of patients, which indeed could lead to the detection of those who are more likely to benefit from a surveillance program in terms of better prognosis, such as virus-related cancers. In this regard, consistent data suggest that HPV-positive tumors and Epstein-Barr virus–positive nasopharyngeal cancers harbor a better prognosis, also in the recurrent setting.34-36
Another possible limitation is that patients were staged according to the fifth and sixth editions of American Joint Committee on Cancer, which do not take into account the important prognosis-dictated revision of the eighth edition, such as the separate staging system for HPV-related oropharyngeal cancer, the addition of extracapsular nodal spreading to N classification in nonviral-related cancers, and the depth of invasion in primary tumors of the oral cavity with possible upstaging in these groups of patients.
The strength of our analysis is the homogeneous population of a single institution with locally advanced HNC, followed with the first radiologic imaging within 6 months since treatment end, according to the National Comprehensive Cancer Network guidelines, 17 allowing exclusion of persistent disease or early progression. However, with the known limit of any retrospective analysis, these data should be considered only as hypothesis generating.
In the next 10 years, there will be marked increased access to medical visits for oncologic patients, 37 mainly in the continuing care phase, therefore making it mandatory to evaluate the cost-effectiveness of follow-up programs.
Radiologic examinations and clinical visits are both time- and resource-consuming procedures. Surveillance imaging also implies potentially harmful repeated radiation exposure 38 and sometimes leads to unnecessary imaging and/or biopsy. The anxiety that patients experience during clinical and radiologic follow-up is also not negligible.39,40 Therefore, prospective trials assessing the most effective follow-up strategy are needed, both from a clinical point of view and from the perspective of the impact on health care system. Therefore, we started an academic-funded multicenter trial on health and economic outcomes of 2 follow-up strategies in radically cured advanced HNC (clinicaltrials.gov NCT02262221) 41 to compare a more intensive follow-up program with a symptom-based one. The endpoints are the cost-effectiveness of the 2 strategies, the cause-specific survival and OS in the 2 arms, the percentage of potentially salvageable recurrences and/or second primaries in both groups, and the quality of life before and after diagnosis of cancer recurrence. In this trial, we will also try to overcome some limitations highlighted by this retrospective analysis, such as the need for a specific follow-up plan according to subsites and the need for a screening program for lung cancer in high-risk smokers.41,42
We acknowledge that the importance of follow-up programs does not rely only on discovery of recurrence but also on engagement with patient’s needs after cancer treatments. In this regard, the start of physical rehabilitation programs, the attention to nutritional issues, and the support of psychological needs are a fundamental part of this program, thus leading all involved health care professionals to work together in a multidisciplinary context.
Conclusions
In a single-institution HNC population, the clinical and radiologic follow-up allowed identification of a higher number of recurrences/SPCs (arising from the upper aerodigestive tract) than the symptom-driven monitoring. The curability rate was similar regardless of detection modality. Prospective trials are awaited to define the most effective follow-up strategy in the HNC setting and its specific role in the virus-related cohort.
Author Contributions
Disclosures
Footnotes
Acknowledgements
Editorial assistance was provided by Luca Giacomelli, PhD, Lilia Biscaglia, PhD, and Aashni Shah (Polistudium); this assistance was supported by internal funds. The manuscript is in memory of Claudia Massoni. Her family strongly sustained head and neck cancer research.
No sponsorships or competing interests have been disclosed for this article.