
Abstract
Objective
To examine if attending surgeon presence at the preinduction briefing is associated with a shorter time to incision.
Study Design
Retrospective cohort study and survey.
Setting
Tertiary academic medical center.
Subjects and Methods
A retrospective cohort study was conducted of 22,857 operations by 141 attending surgeons across 12 specialties between August 3, 2016, and June 21, 2018. The independent variable was attending surgeon presence at the preinduction briefing. Linear regression models compared time from room entry to incision overall, by service line, and by surgeon. We hypothesized a shorter time to incision when the attending surgeon was present and a larger effect for cases with complex surgical equipment or positioning. A survey was administered to evaluate attending surgeons’ perceptions of the briefing, with a response rate of 68% (64 of 94 attending surgeons).
Results
Cases for which the attending surgeon was present at the preinduction briefing had a statistically significant yet operationally minor reduction in mean time to incision when compared with cases when the attending surgeon was absent. After covariate adjustment, the mean time to incision was associated with an efficiency gain of 1.8 ± 0.5 minutes (mean ± SD; P < .001). There were no statistically significant differences in the subgroups of complex surgical equipment and complex positioning or in secondary analysis comparing service lines. The surgeon was the strongest confounding variable. Survey results demonstrated mild support: 55% of attending surgeons highly prioritized attending the preinduction briefing.
Conclusion
Attending surgeon presence at the preinduction briefing has only a minor effect on efficiency as measured by time to incision.
Hospital leaders continue to seek initiatives to improve efficiency due to increasing financial pressures and compliance regulations. The operating room (OR) is an important target for process improvements, as it is estimated to account for 40% of hospital expenses; an idle minute is estimated to cost between $30 and $100.1-4 Surgical checklists have been demonstrated to improve quality of care.5-8 However, only a limited number of studies have explored whether surgical checklists also improve efficiency. Clark et al found a significant decrease in time to incision (40 vs 63 minutes) when the attending was present in the OR earlier. 9 Deldar et al identified that the most common etiology for delays in 4492 first-start cases was surgeon related. 10 By implementing a lean process improvement, they were able to improve on-time starts (69% vs 57%) with fewer surgeon-related delays. In a study of hand surgeons, Gottshchalk et al found that turnover time was significantly shorter in cases in which the surgeon remained in the OR during turnover (27.5 vs 30.4 minutes) and when the surgeon incentivized OR staff (24 vs 29 minutes). 11
However, other larger studies have demonstrated no effect of surgical checklists on case efficiency. In a large published study, Papaconstantinou et al analyzed the effect of a surgical safety checklist on efficiency of 35,570 operations and found no difference for total OR time (P = .93), surgical time (P = .66), on-time first starts (P = .15), and same-day cancellations (P = .57). 12 While the mean OR disposable cost as measured was lower at $70 per surgery, there was no operational improvement in efficiency with the checklist. 12
The preinduction briefing is increasingly a standard component of an extended surgical timeout.13-15 Over 50 hospitals in Washington State currently employ the SCOAP system (Surgical Comparison Outcomes Assessment Program), a data-driven quality improvement program. 16 Our institution utilizes the SCOAP 4-part checklist system. SCOAP 1 is the preinduction briefing performed on arrival to the OR (focus of this study), and the timing is shown in Figure 1 . SCOAP 2 is the preincision timeout. SCOAP 3 is performed at surgical closing, and SCOAP 4 is performed at the completion of the case. Conducting SCOAP 1 (herein, the preinduction briefing) is mandatory; however, attending surgeon presence at this briefing is elective. 16
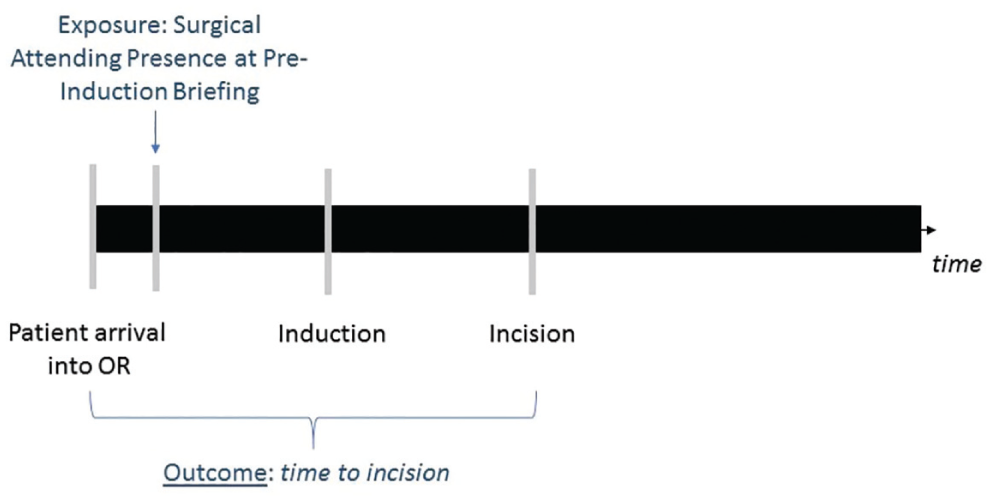
Timeline with the preinduction briefing and outcome. OR, operating room.
Communication among surgery, anesthesia, and nursing teams is critical for optimal and efficient case setup. Early attending surgeon involvement in the OR may result in earlier recognition of missed surgical supplies, complex positioning, and equipment setup, while possibly enhancing the speed of other staff. 17 The purpose of this study was to investigate whether the presence of the attending surgeon at the preinduction briefing was associated with a shorter time to incision—a measure of operational efficiency.
No study has examined the relationship of the preinduction briefing on time to incision among multiple surgical specialties within a hospital. Furthermore, prior studies have not controlled for multiple patient, procedure, and personnel confounders. For example, preincision procedures, such an arterial or central line performed by an anesthesiologist or equipment setup required for a type of surgery, directly increase time to incision. Given these gaps, we performed an in-depth analysis examining >22,000 cases across 12 surgical specialties. We hypothesized that surgical attending presence at the preinduction briefing was associated with a decreased time to incision as measured by room entry to incision time. We hypothesized a stronger effect in 2 subgroups: cases with complex surgical equipment and complex positioning. In addition, we administered a survey to attending surgeons to assess perspectives on the importance of participation in the preinduction briefing.
Methods
A retrospective cohort study and survey were performed.
Study Design and Variables
In the cohort study, the independent variable was surgical attending presence at the preinduction briefing. The outcome was the time from room entry to incision ( Figure 1 ). The University of Washington Institutional Review Board determined that review was not indicated (STUDY00003255).
Inclusion criteria were noncanceled closed surgical cases on the schedule that were performed in the OR at a single academic medical center, beginning when surgical attending presence at the preinduction briefing was recorded (August 3, 2016–June 21, 2018). Twelve surgical service lines were included: otolaryngology, cardiac surgery, general surgery, gynecology, neurosurgery, oral and maxillofacial surgery, orthopedic surgery, plastic surgery, thoracic surgery, transplant surgery, urology, and vascular surgery. Emergency cases, patients <18 years old, and cases scheduled beyond normal hours (outside of 7
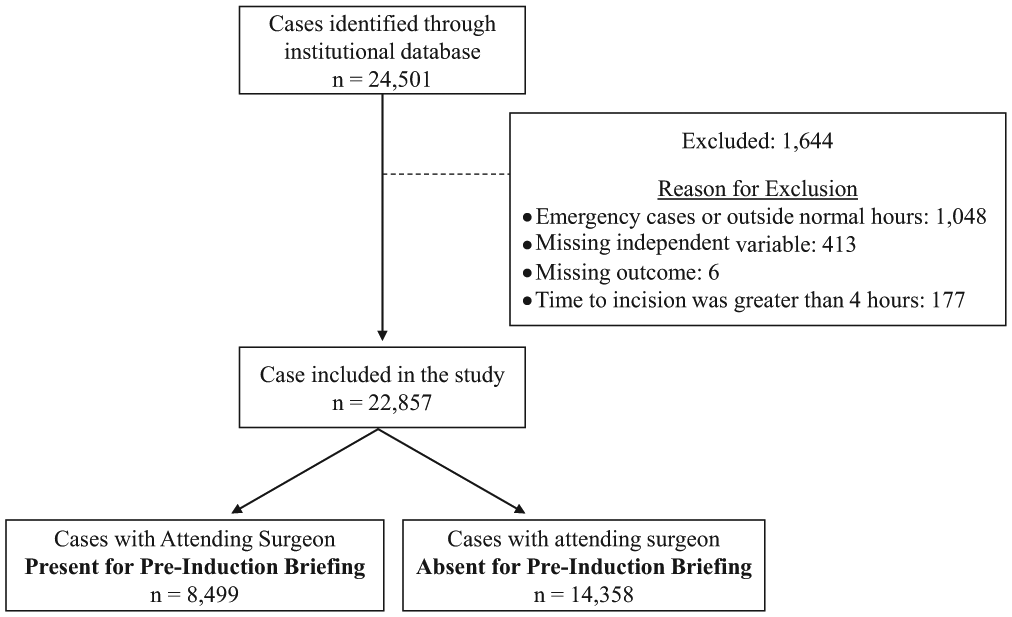
Study inclusion and exclusion criteria.
The primary hypothesis was that attending presence at the preinduction briefing would be associated with a shorter time to incision when compared with cases for which the attending was absent. We additionally defined a priori primary hypotheses that attending presence at the briefing would have a larger effect on efficiency for cases with complex surgical equipment (Da Vinci robot, microscope, laser, and navigation) or cases with complex positioning (Fowlers, semi-Fowlers, decubitus, prone, jackknife, or use of Mayfield pins) versus standard cases. Our secondary analysis included studying this effect by service line and by surgeon. Complex surgical equipment and complex positioning were specified by the surgery (M.E.W.) and anesthesiology (S.S. and J.D.L.) authors of this study, respectively. These defined variables were binary (ie, complex or noncomplex surgical equipment/positioning).
Difficult airway, a potential confounder, was composed of grade 3 or grade 4 Cormack-Lehane classifications on direct laryngoscopy or if the number of intubation attempts was ≥3. Missing data in this variable were classified as nondifficult airway due to the assumption that providers were more likely to omit documenting this field if the airway was not perceived to be difficult.
Survey
The survey examined attending surgeons’ perceptions of presence at the preinduction briefing. On a 5-point Likert scale, attending surgeons were asked to rank if the metric was a high priority to them, if the metric was a high priority to their colleagues, and if complying with the metric was a core responsibility.
Statistical Methods
Descriptive statistics for surgical case characteristics are presented as mean ± standard deviation (range) for continuous variables and count (percentage) for categorical variables. We compared mean time to incision between cases with the attending surgeon present and absent using linear regression (unadjusted analysis) and the doubly robust method (adjusted analysis). 18 The adjusted analysis controlled for the following: American Society of Anesthesiologists (ASA) class, comorbidities, age, sex, body mass index, difficult airway, patient disposition (intensive care unit/inpatient/outpatient), scheduled case duration, arterial line placement, central line placement, type of anesthetic, surgical service line, primary anesthesiologist, primary surgeon, complex position, complex surgical equipment, and difficult airway.
The difference of the effects across subgroups was evaluated by the test of the interaction of surgical attending presence and the subgroup variable. A sensitivity analysis with multivariable linear regression found no substantive differences from the primary analysis. All calculations were carried out in R (version 3.5.0; R Foundation, Austria, Vienna). P < .05 denoted statistical significance.
Results
A total of 141 attending surgeons performed 22,857 cases during the study period. Surgical case characteristics (overall and by the presence of the attending surgeon) are described in Table 1 . In 8499 cases, the attending surgeon was absent for the preinduction briefing; in 14,358 cases, the attending surgeon was present.
Surgical Case Characteristics.
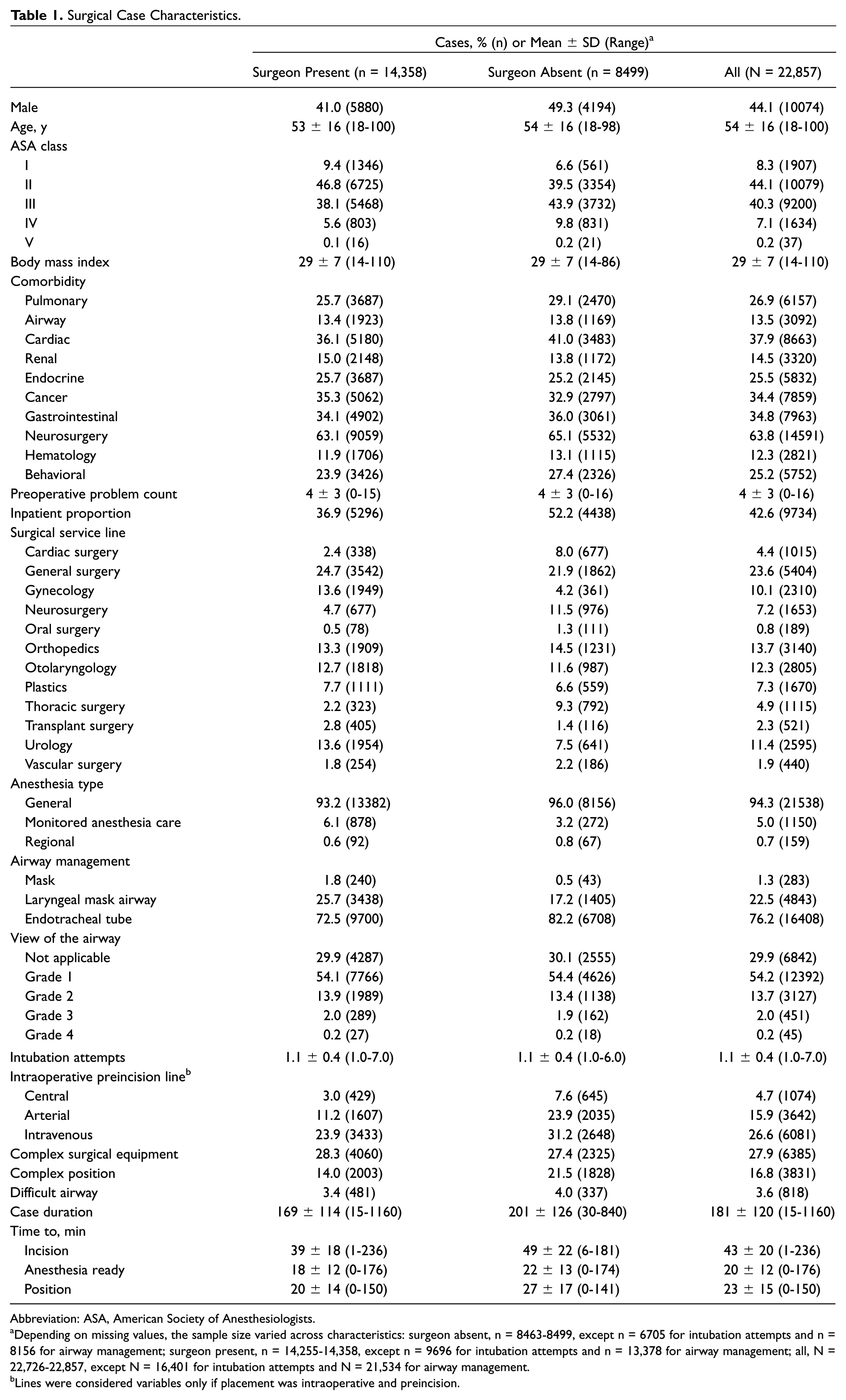
Abbreviation: ASA, American Society of Anesthesiologists.
Depending on missing values, the sample size varied across characteristics: surgeon absent, n = 8463-8499, except n = 6705 for intubation attempts and n = 8156 for airway management; surgeon present, n = 14,255-14,358, except n = 9696 for intubation attempts and n = 13,378 for airway management; all, N = 22,726-22,857, except N = 16,401 for intubation attempts and N = 21,534 for airway management.
Lines were considered variables only if placement was intraoperative and preincision.
Table 2 shows the unadjusted and adjusted differences in the mean time to incision between the 2 groups of cases (attending surgeon present vs absent). The unadjusted efficiency gain (faster time to incision) for cases in which the attending surgeon was present at the preinduction briefing, as compared with those in which he or she was absent, was 9.8 minutes (95% CI, 9.3-10.3 minutes; P < .001). This difference was equivalent to a potential reduction in time to incision of 20% relative to the unadjusted overall mean time to incision of 50 minutes. However, after adjusting for covariates, the association was notably smaller, with an adjusted difference of means of 1.8 minutes (95% CI, 1.4-2.2 minutes; P < .001).
Pre- and Postadjustment Differences in the Mean Time to Incision Overall and in the Subgroups of Complex Surgical Equipment and Complex Position. a
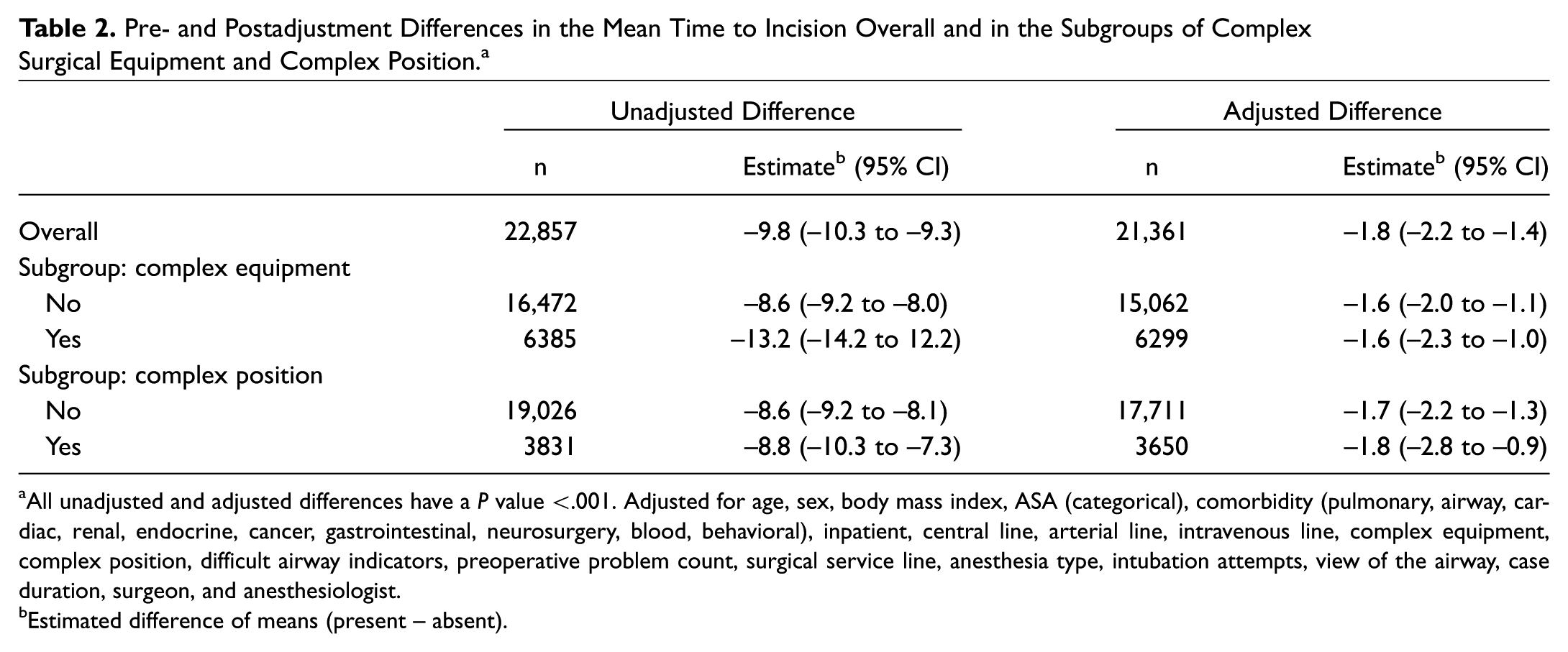
All unadjusted and adjusted differences have a P value <.001. Adjusted for age, sex, body mass index, ASA (categorical), comorbidity (pulmonary, airway, cardiac, renal, endocrine, cancer, gastrointestinal, neurosurgery, blood, behavioral), inpatient, central line, arterial line, intravenous line, complex equipment, complex position, difficult airway indicators, preoperative problem count, surgical service line, anesthesia type, intubation attempts, view of the airway, case duration, surgeon, and anesthesiologist.
Estimated difference of means (present – absent).
A sensitivity analysis to understand the role of the individual adjustment variables showed that the adjustment for the surgeon had the highest impact on the estimated difference. After adjusting for the surgeon, the difference in mean time to incision decreased from 9.7 to 2.7 minutes. This major difference between the unadjusted and surgeon-adjusted difference suggests that most of the unadjusted difference in time to incision was attributable to differences among surgeons. Surgeons with a higher rate of presence at the preinduction briefing had shorter mean times to incision (Pearson correlation, –0.55).
The surgical case characteristics for included cases (22,857 cases) were compared to those of normal working hours/nonemergency excluded cases (596 cases) to evaluate if there was a bias based on the exclusion criteria. There did not appear to be substantive differences between the groups, and the time to incision overall was 44 ± 38 minutes for the included group and 43 ± 27 minutes for the excluded group.
The effect of attending surgeon presence at the preinduction briefing by surgical service line is illustrated in Figure 3 . The within-surgeon differences (mean time when present minus absent) for individual surgeons are shown in Figure 4 . For clarity, the figure is limited to surgeons with at least 10 cases overall (5 in the present group and 5 in the absent group). Among the 108 surgeons in Figure 4 , 82 (76%) had a faster time to incision when the attending surgeon was present, and 26 (24%) had a slower time to incision when the attending surgeon was present.
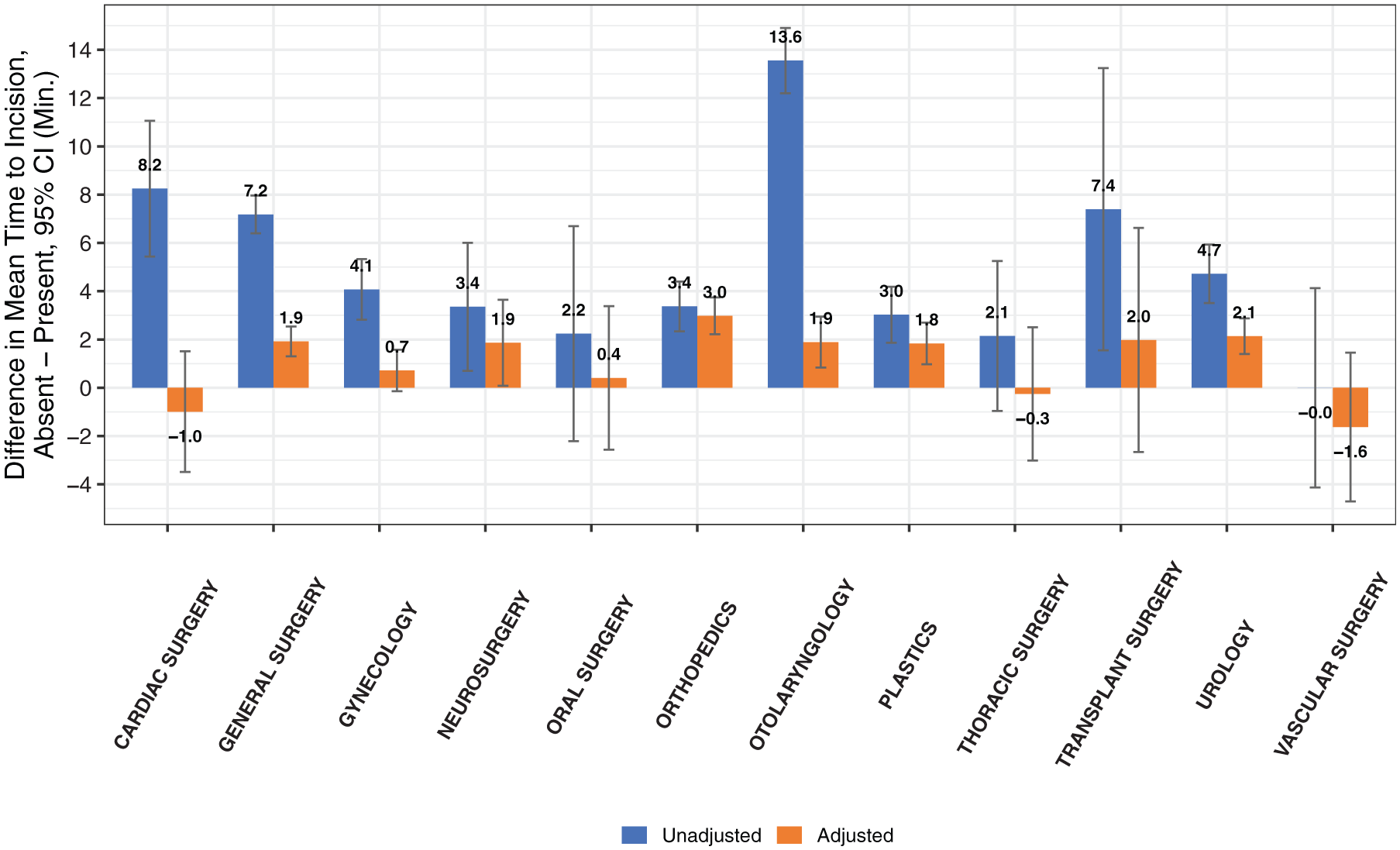
By surgical service line: pre- and postadjustment differences in mean time to incision.
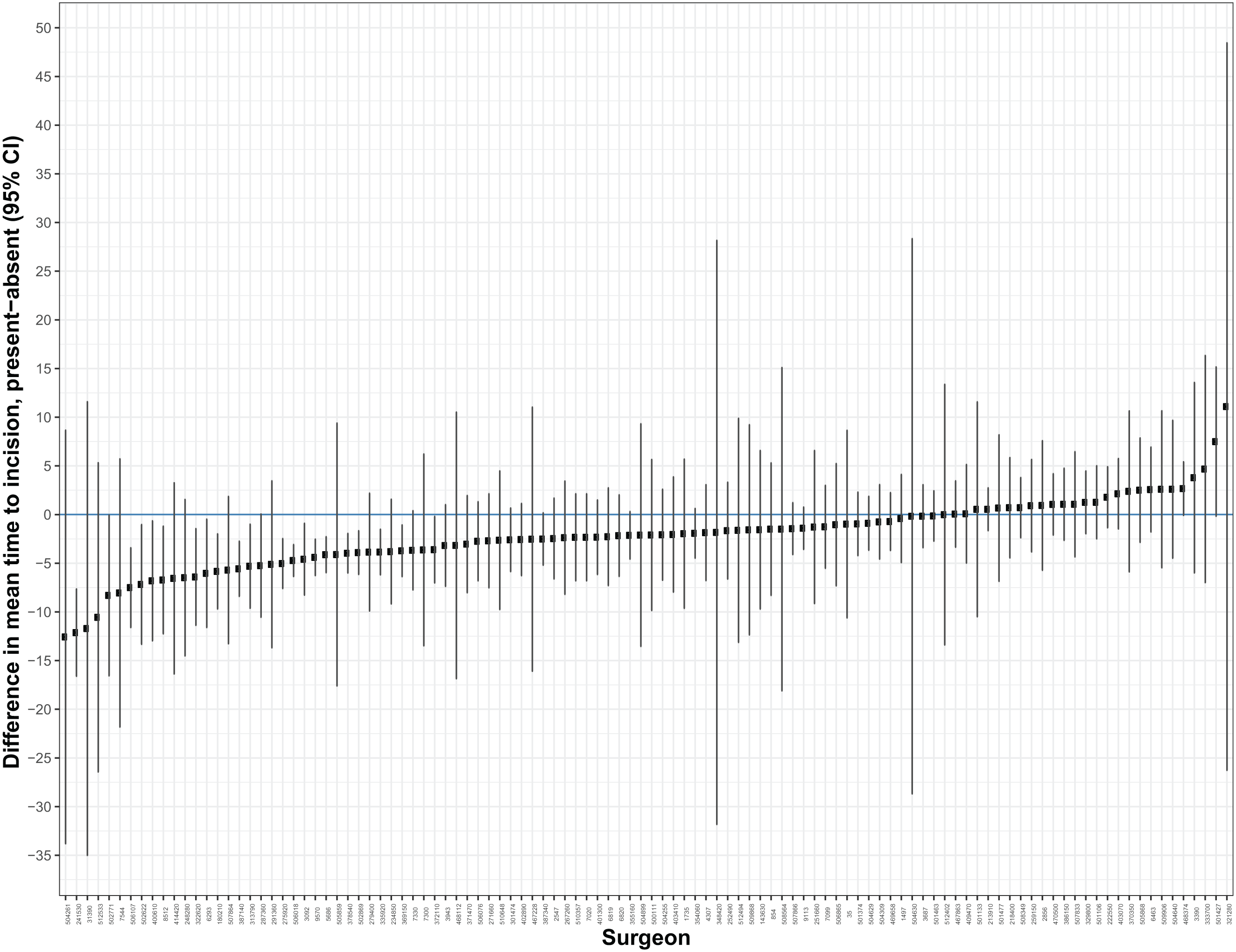
By surgeon: differences in mean time to incision when present vs absent. Each circle represents the difference in mean time to incision (present – absent) with 95% CIs.
Differences due to Complex Surgical Equipment or Complex Position
The difference in mean time to incision between cases with attending surgeon present versus absent was not significantly different when complex surgical equipment or positioning was used. If a case had complex equipment, the adjusted efficiency gain was 1.6 minutes, no different from the gain for cases without complex equipment (1.6 minutes; P = .353). If a case required complex positioning, the adjusted efficiency gain was 1.7 minutes, as compared with 1.8 minutes for cases without complex positioning (P = .710).
Differences due to Surgical Service Line
In the unadjusted analysis, attending surgeon presence at the preinduction briefing was associated with a faster time to incision in 11 of the 12 surgical services ( Figure 3 ). After adjustment, the efficiency gain was still observed in 9 of the 12 surgical service lines. The adjusted efficiency gain was highest in orthopedics (3.0 minutes), urology (2.1 minutes), and transplant surgery (2.0 minutes), followed by otolaryngology, neurosurgery, and general surgery (each 1.9 minutes). The effect was weakest in vascular surgery, which had a 1.6-minute decrease in efficiency with attending surgeon presence at the preinduction briefing. A test for an interaction between surgeon presence and service line trended toward a significant difference but did not meet it (P = .070).
Survey to Evaluate Attending Surgeon Perceptions of the Preinduction Briefing
The survey was administered to 94 attending surgeons across all departments, representing a subset who had performed at least 10 operations in the study period, and was completed by 64 surgeons (68%). When asked if attending surgeon presence at the preinduction briefing was a high priority to them, the majority of attending surgeons agreed or strongly agreed (n = 35, 55%), as opposed to 18 (28%) who disagreed or strongly disagreed ( Figure 5 ). When asked if attending surgeon presence was a high priority to other attending surgeons, only 18 surgeons (28%) agreed or strongly agreed. The majority (n = 26, 41%) were neutral, and 20 (31%) disagreed or strongly agreed. When asked if attending presence at the preinduction briefing was a core responsibility, 33 attending surgeons (52%) agreed or strongly agreed, 13 (20%) were neutral, and 18 (28%) disagreed or strongly disagreed.
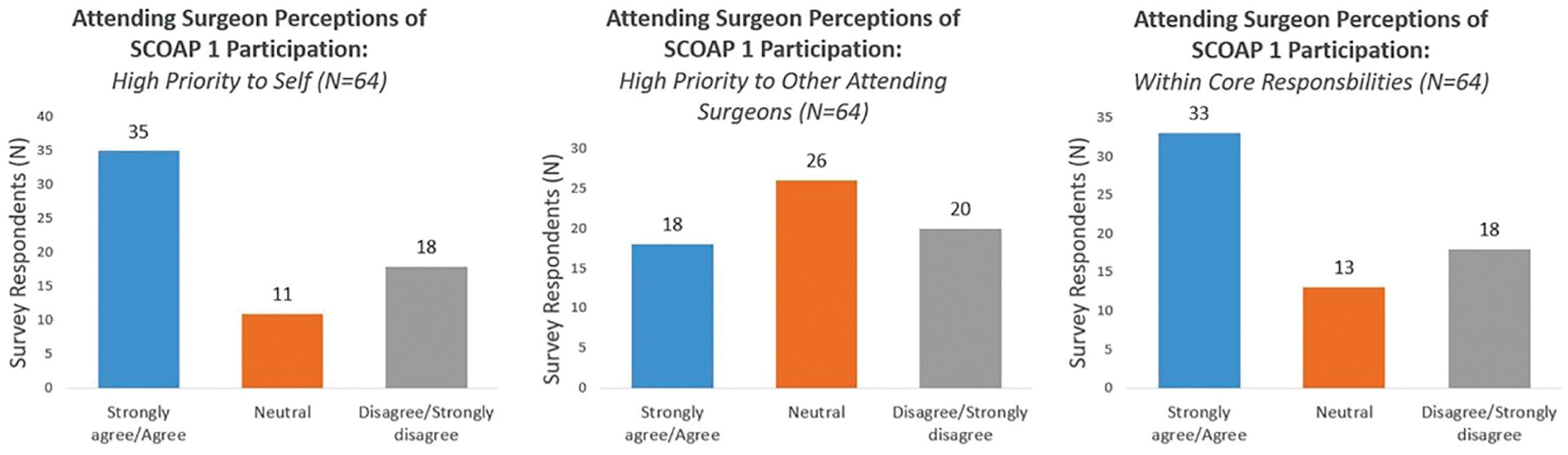
Survey: attending surgeon perceptions of the preinduction briefing. SCOAP, Surgical Comparison Outcomes Assessment Program.
Discussion
Our primary analysis demonstrates that, on average, there was an efficiency gain of 10 minutes (20% potential time savings) in time to incision when the attending surgeon was present as compared with when he or she was absent (analysis unadjusted for covariates). However, after adjusting for potential confounding factors, this association diminished to a <2-minute efficiency gain in time to incision ( Table 1 ). Although this difference was statistically significant, it was likely not operationally significant. The difference between the unadjusted and adjusted analysis was primarily attributed to differences among surgeons. We did not find a significant difference in the subgroups of complex surgical equipment and complex positioning, as demonstrated in Table 2 .
Secondary analysis was performed at the service line and surgeon levels. Analysis at the service line demonstrated that for 9 of 12 surgical departments, attending presence at the preinduction briefing was associated with an efficiency gain even after adjustment. There was not a statistically significant difference in the effect of attending surgeon presence at the preinduction briefing based on surgical specialty. Despite the lack of statistical significance, the results suggest that the efficiency gain may be more important in specialties with higher surgical case volumes per day, such as orthopedics and urology. In these service lines, these time savings may be more operationally important. Nevertheless, the efficiency gains are small. Furthermore, there is an opportunity cost in surgeon time for being present early in the case, which may outweigh any efficiency benefit of presence at the preinduction briefing.
The strongest confounding variable was the primary surgeon. The decision to attend the preinduction briefing is unlikely to be random and may be dependent on multiple factors, such as a surgeon’s availability on the day, perceived case duration, perceived case setup and positioning time, patient disposition and expectation, level of trainee experience, and individual management preferences. This study was not designed to examine and distinguish among these mechanisms; however, future studies can build on this finding. Given that the surgeon is the most significant confounding variable, a surgeon-level analysis considers the outcome for each surgeon (a within-surgeon comparison). No study had examined the efficiency effects for each surgeon. When this was performed ( Figure 4 ), it became clear that for the majority of surgeons, presence at the preinduction briefing was associated with only a small reduction in time to incision.
Other important confounders were the anesthesiology team placing an arterial line preincision in the OR (–3.7-minute difference postadjustment), scheduled case duration (–3.2-minute difference postadjustment), patient disposition of intensive care unit/inpatient/outpatient (–2.7-minute difference postadjustment), and primary anesthesiologist (–2.3-minute difference postadjustment). Prior studies did not include these variables for adjustments. Given that our unadjusted findings are similar to those previously published, the reported efficiency gains of early surgeon presence in the OR may be overestimated in the literature.
To the best of our knowledge, our study is the largest performed in the literature, including >22,000 cases with 141 surgeons over 12 surgical service lines in a large academic medical center. Our study expands current work by considering multiple confounders and within-surgeon effects in a large cohort to evaluate the true relationship between presence at the preinduction briefing and time to incision. Notably, our findings demonstrate a smaller efficiency gain than that in previously published studies. Clark et al analyzed 227 endocrine cases prospectively and reported a 22-minute shorter time to incision for thyroidectomies, 27-minute shorter time for parathyroidectomies, and 44-minute shorter time for adrenalectomies based on early attending surgeon presence in the OR. However, without consideration of the surgeon, anesthesia, and patient variables as potential confounders, these results may be overestimated and accounted for by individual surgeon behavior rather than a true effect of early surgeon involvement. 9 Gottschalk et al found a significant but small 3- to 5-minute efficiency gain when the surgeon remained in the OR between cases; however, this study was also limited to a single specialty, by small sample size, and by lack of adjustment for potential confounders. 11
Our survey results ( Figure 5 ) demonstrate a slight tendency for surgeons to consider attendance at the preinduction briefing a high individual priority (55%) and core responsibility (52%). However, support is not uniform, as only 28% of surgeons thought that presence was a high priority to other attending surgeons. These underlying perceptions may contribute to the variability seen in attending surgeon’s decisions to be present or absent. While the slight efficiency gain may not justify the presence of the attending surgeon at the preinduction briefing, it is important to note that participation in the surgical checklist system may improve patient safety and clinical outcomes—irrespective of its effect on efficiency. 12
There are multiple limitations in our study. At our institution, we do not track the arrival time of the surgeon. Thus, we could not differentiate early involvement in the OR from the specific effect of the preinduction briefing checklist. In academic medical centers, attending surgeon presence at the preinduction briefing may be less important when an experienced postgraduate trainee is present in the OR. We did not evaluate the involvement of trainees in the study, and this represents an area of future exploration. Given the absence of validated instruments, we developed a survey to evaluate attending surgeon perceptions of the preinduction briefing. Our survey was designed to provide a cultural context for the preinduction briefing to better inform opportunities for intervention; future studies can expand on this work with more comprehensive assessments.
The major impetus for this study was to identify if attending surgeon presence at the preinduction briefing may be associated with improved case efficiency. Across 12 surgical service lines, the adjusted effect of surgeon presence at the preinduction briefing reduced the time to incision by only 1.8 minutes, likely operationally insignificant. Encouraging presence at the preinduction briefing does not appear to be a high-yield intervention to improve OR efficiency.
Conclusion
Cases for which the attending surgeon was present at the preinduction briefing had a statistically significant reduction in time to incision when compared with cases when the attending surgeon was absent. However, after adjusting for confounders, this efficiency gain decreased from 9.8 minutes to just 1.8 minutes. Thus, while the preinduction checklist is an important communication and patient safety tool, it does not appear that attending surgeon participation in the preinduction briefing checklist is associated with operationally significant gains in OR efficiency.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We acknowledge the contributions of T. Andrew Bowdle, MD, PhD, and Srdjan Jelacic, MD, who developed the Checklist Navigator software at the University of Washington. This checklist software enabled acquisition of the independent variable, surgical attending presence at the preinduction briefing.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the AAO-HNSF 2018 Annual Meeting & OTO Experience; October 7-10, 2018; Atlanta, Georgia.