
Abstract
Objective
For critically ill patients undergoing long-term mechanical ventilation, to determine whether early conversion from endotracheal intubation to tracheostomy reduces the incidence of laryngotracheal stenosis.
Data Sources
MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, and the Cumulative Index to Nursing and Allied Health Literature.
Review Methods
A systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and an assessment of bias were performed. Included studies reported outcomes of patients who were converted from endotracheal intubation to tracheostomy, compared early vs late tracheostomy, and reported the incidence of laryngotracheal stenosis and details of postoperative surveillance. Data were also collected for intensive care setting, method of tracheostomy, and timing of tracheostomy.
Results
Seven articles met inclusion criteria: 2 randomized trials, 2 quasi-randomized trials, 1 prospective cohort, and 2 retrospective cohorts. A total of 966 patients were included in this analysis (496 in the early tracheostomy group and 470 in the late tracheostomy group). The mean incidence of laryngotracheal stenosis was 8.9% (range, 0%-20.8%), with a mean incidence of 8.1% in early tracheostomy groups and 10.9% in late tracheostomy groups. In studies with the least risk of bias, there were no differences in the incidence of laryngotracheal stenosis in patients who underwent early vs late tracheostomy.
Conclusion
In critically ill patients undergoing long-term mechanical ventilation, early conversion to tracheostomy within 7 days of intubation does not significantly decrease the risk of laryngotracheal stenosis compared to later conversion as defined by the included studies.
Tracheostomy is a common procedure performed in 2% to 11% of patients requiring mechanical ventilation in the intensive care unit (ICU) and one of the most commonly performed procedures in critically ill patients.1-4 Long-term mechanical ventilation is the most common indication for tracheostomy in ICU patients. The performance of tracheostomy has multiple reported advantages over continued endotracheal intubation, including improved patient comfort, decreased airway resistance, easier and safer tracheal suction, improved patient communication, and improved oral feeding.3,5,6
Numerous randomized controlled trials (RCTs), systematic reviews, and meta-analyses have examined the timing of tracheostomy and have shown benefits of early tracheostomy in ICU patients requiring long-term mechanical ventilation. Reported advantages of early tracheostomy include improved mortality rates, decreased incidence of ventilator-associated pneumonia, decreased length of ICU stay, shorter duration of mechanical ventilation, and decreased median hospital cost. 5 Although the literature favors early tracheostomy for these outcomes, less is known concerning how laryngotracheal stenosis (LTS) should be factored into the clinical decision-making process for these patients. This outcome was excluded in trials such as the TracMan randomized trial. 7
Over time, endotracheal tubes cause pressure injury and necrosis at the posterior glottis and cuff site. Acute injury to the epithelium has been observed within hours of intubation8,9 and can lead to severe commissural and tracheal scarring. Earlier performance of elective tracheostomy, and thus removal of the endotracheal tube, may reduce the complications caused by the endotracheal tube.10,11 Published literature on the incidence of LTS and the utility of early tracheostomy to decrease this complication is conflicting, with reported rates of the incidence of LTS in patients undergoing long-term intubation ranging from zero patients developing laryngeal scarring or stenosis during follow-up in 1 study 12 to rates of nearly 20%. 13 Furthermore, the conclusions the authors have drawn in these studies about the risk reduction in patients who underwent early vs late tracheostomy vary from observing no significant difference 14 to finding a dose-dependent decrease in the incidence and severity of complications with early tracheostomy. 15
Performance of tracheostomy, whether an operative or percutaneous technique is used, introduces the patients to additional risks. These include both acute complications such as bleeding, infection, subcutaneous emphysema, pneumothorax, and chronic complications such as stenosis at the tracheostomy stoma and the cuff site.16,17 These potential complications of undergoing tracheostomy must be balanced against the risks of continued intubation. The goal of this systematic review was to investigate whether early tracheostomy reduces the risk of LTS in adults requiring long-term mechanical ventilation.
Methods
Data Sources and Search Strategy
A systematic search of MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) was performed. Electronic searches were performed using the keywords and phrases “early tracheostomy,”“early tracheotomy,”“tracheostomy timing,”“tracheotomy timing,” and “tracheal stenosis.” The reference lists of included articles were examined for additional articles meeting inclusion criteria. Institutional review board approval was not required since this analysis of data was obtained from published literature.
Study Selection
The titles and abstracts of all articles found using the search strategy were screened for relevance, and the full texts of remaining articles were reviewed. Studies were included if they met the following inclusion criteria: published through March 2018, written in the English language, assessed critically ill patients treated in the ICU, compared outcomes between patients who were converted from endotracheal intubation to either early or late tracheostomy (as defined by each study’s protocol), and reported outcomes on the incidence of LTS. Two authors independently evaluated potential articles. Agreement was reached by consensus of the authors. Included study designs were randomized controlled trials and cohort trials; reviews, editorials, and case reports were excluded.
Data Extraction and Quality Assessment
Data from included studies were extracted onto a spreadsheet. Extracted data for each article included article title, authors’ names, study design, year of publication, number of enrolled patients, ICU setting, patient selection and randomization method, tracheostomy timing, tracheostomy method, length of follow-up, surveillance method, and laryngotracheal complications observed, including stenosis. Any disagreement regarding the data was resolved by discussion.
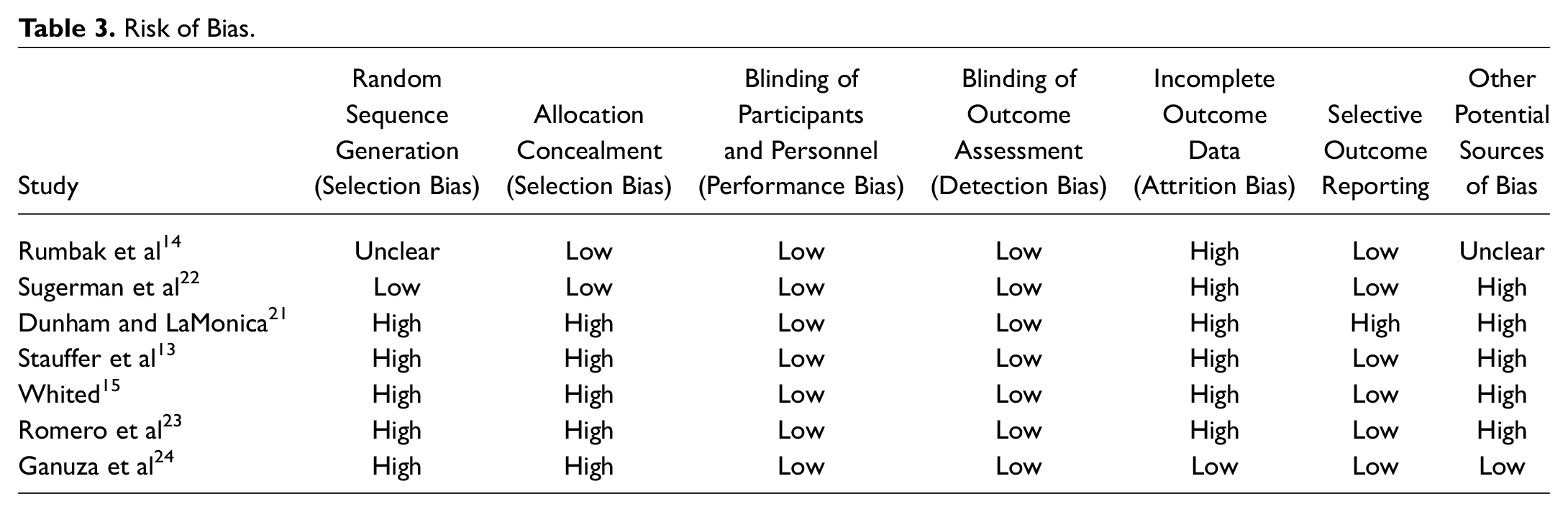
The assessment of the risk of bias in included studies was conducted in accordance with the Cochrane Collaboration’s tool for assessing the risk of bias. 18 Risk specifically relating to the outcomes relevant to the present analysis was appraised in the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential sources of bias. Results were summarized as “low risk of bias,”“unclear risk of bias,” or “high risk of bias” and plotted using RevMan 5.3. 19
Data Synthesis and Analysis
Extracted data from included articles were summarized in the included tables. Pooled effects were calculated using a random-effects model (DerSimonian-Laird method), and a forest plot was constructed. Analyses were performed in R version 3.3.3 (R Foundation for Statistical Computing, Vienna, Austria). Results were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol. 20
Results
The search strategy yielded a total of 2373 citations, including 1368 unduplicated articles. Seven studies, with a total of 1076 patients, were identified that met inclusion criteria. These included 4 randomized or quasi-randomized trials (501 patients) and 3 cohort trials (577 patients), including 1 prospective and 2 retrospective cohorts. The median number of patients per study was 152 (range, 74-225). The literature search selection process is shown in Figure 1 . The included articles examined various critical care settings, including medical,13-15 surgical,13,15 coronary care, 15 and trauma ICUs.21-24 Characteristics of these studies are listed in Table 1 .
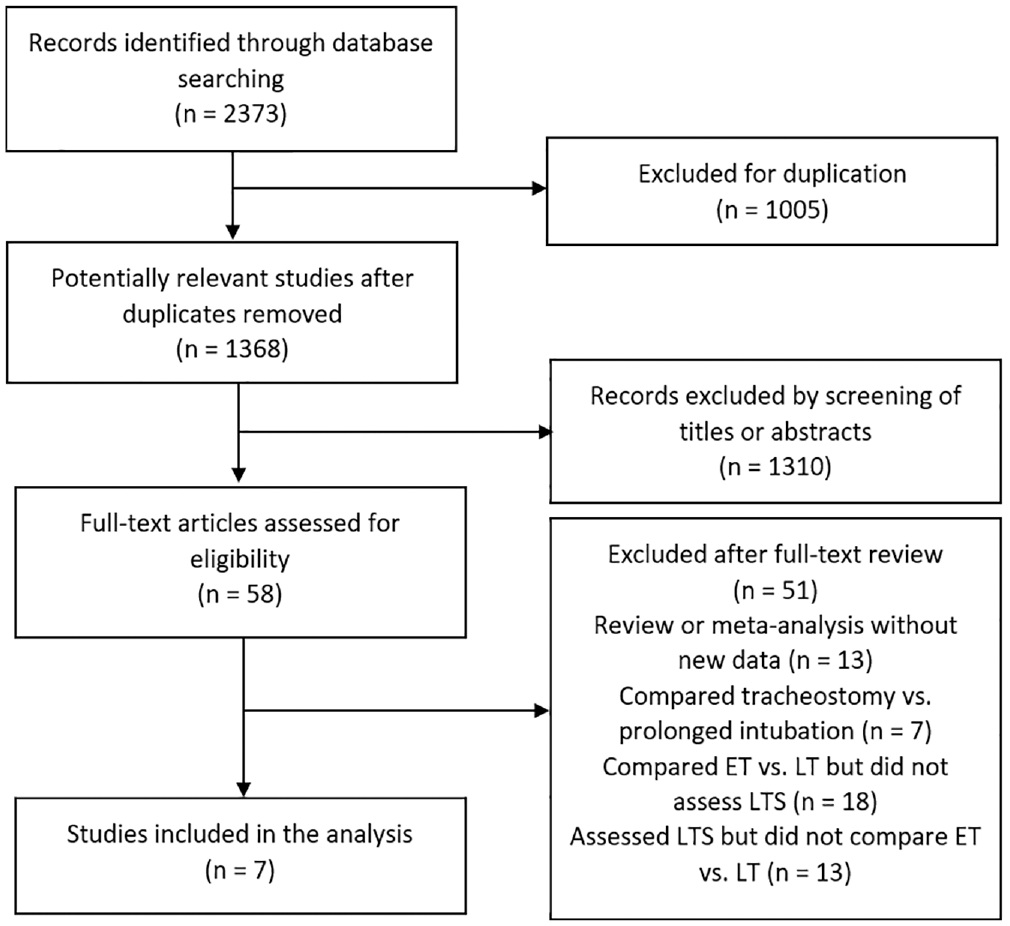
Flowchart of study selection. ET, early tracheostomy group; LT, late tracheostomy group; LTS, laryngotracheal stenosis.
Characteristics of Included Studies. a
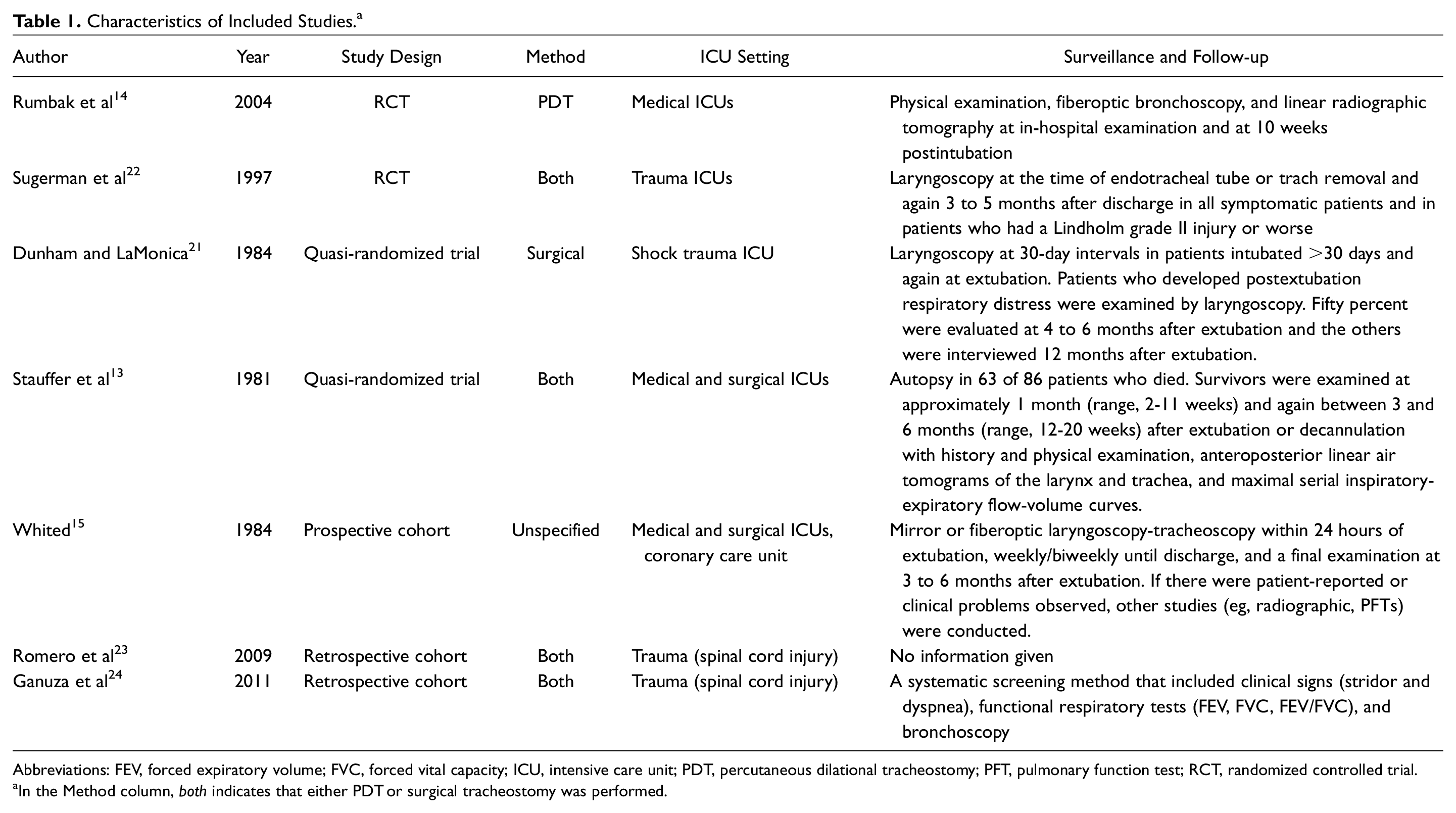
Abbreviations: FEV, forced expiratory volume; FVC, forced vital capacity; ICU, intensive care unit; PDT, percutaneous dilational tracheostomy; PFT, pulmonary function test; RCT, randomized controlled trial.
In the Method column, both indicates that either PDT or surgical tracheostomy was performed.
The definitions of early vs late tracheostomy varied across studies but comprised 2 nonoverlapping categories among the included studies. Early tracheostomy in the included studies included procedures performed from 1 to 7 days after intubation. The late tracheostomy groups included patients who underwent tracheostomies from day 8 after intubation up to day 24 after intubation. While this created a convenient demarcation between 2 groups, the division into “early” and “late” tracheostomy is inherently arbitrary, heterogenous, and nonbinary. Patients were allocated into either early or late tracheostomy groups using protocols that included randomization14,22 and quasi-randomization based on the patient’s hospital ID number,13,21 or else the decision to perform and the timing of tracheostomy was made by the treating physician.15,23,24 One study 15 included a middle period at 6 to 10 days of intubation between early and late tracheostomy. Patients in this middle group were excluded from the present analysis. The timing of conversion to tracheostomy and incidence of LTS in the included studies are listed in Table 2 . The treatment effect of early tracheostomy varied widely between studies ( Figure 2 ).
Timing of Tracheostomy and Cases of Laryngotracheal Stenosis.
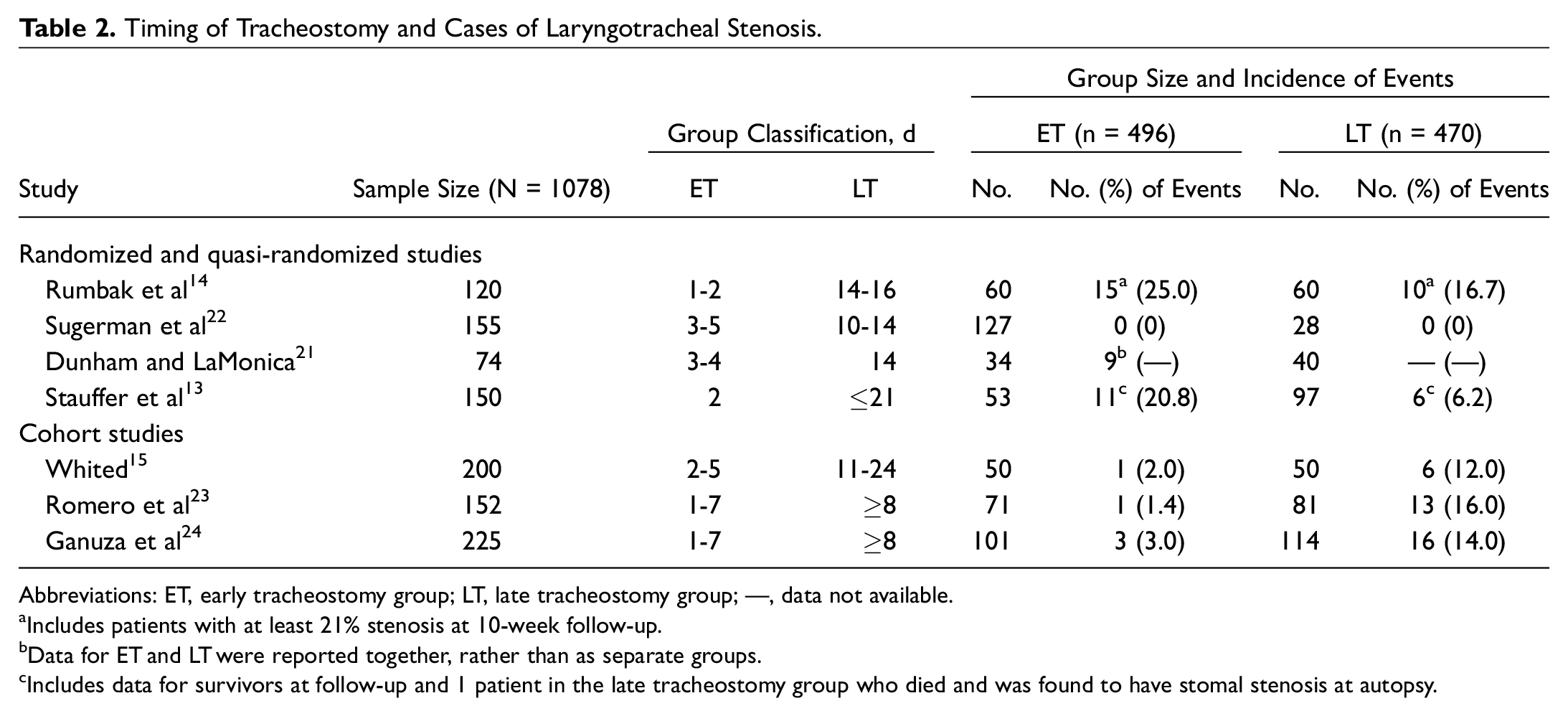
Abbreviations: ET, early tracheostomy group; LT, late tracheostomy group; —, data not available.
Includes patients with at least 21% stenosis at 10-week follow-up.
Data for ET and LT were reported together, rather than as separate groups.
Includes data for survivors at follow-up and 1 patient in the late tracheostomy group who died and was found to have stomal stenosis at autopsy.
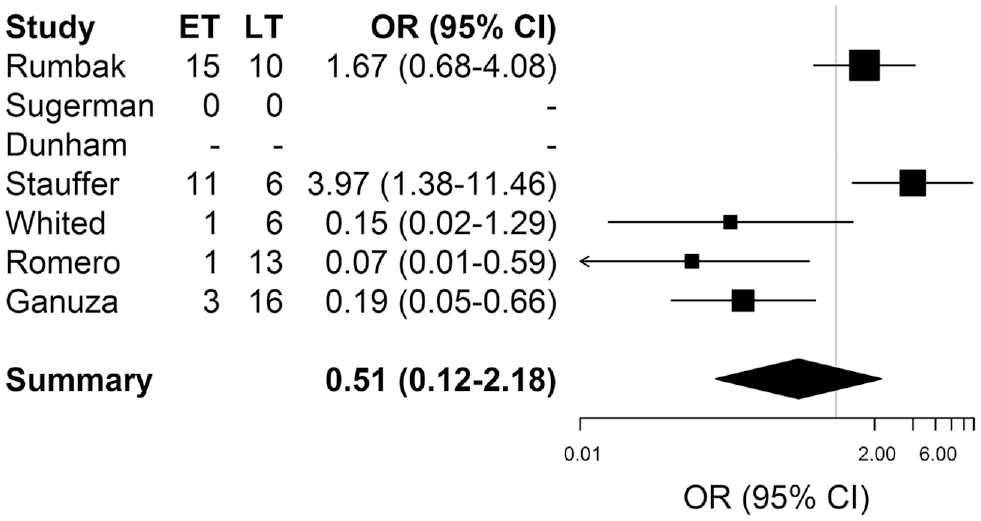
Forest plot. CI, confidence interval; ET, early tracheostomy group; LT, late tracheostomy group; OR, odds ratio.
The included articles were each assessed for their risk of bias in the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other potential sources of bias. 18 Results are shown in Table 3 and summarized in Figure 3 .
Risk of Bias.
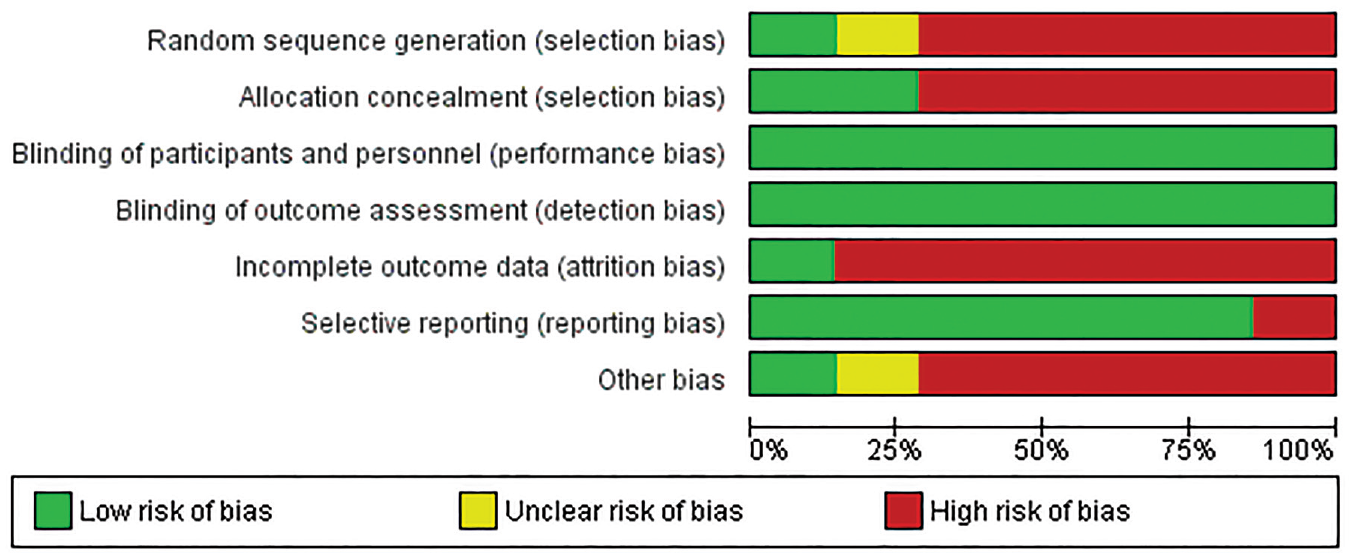
Summary of risk of bias.
Patients underwent either operative or percutaneous tracheostomy by study protocol or per the treating physician’s choice. Both techniques were used in 4 studies.13,22-24 The others used exclusively surgical tracheostomies 21 or percutaneous dilational tracheostomies, 14 or the method was unspecified. 15 Because of the nature of the intervention, patients and treating physicians were not blinded to the timing of tracheostomy performance.
Study methodology was associated with finding significant differences between treatment groups. Three of the randomized or quasi-randomized trials found no difference in the incidence of LTS between the early and late tracheostomy groups, and none of the 4 randomized or quasi-randomized trials found a significant benefit to early tracheostomy. All 3 of the cohort studies reported significantly higher incidences of LTS in the late tracheostomy groups compared to early tracheostomy groups.
Methods of surveillance for LTS varied by study but usually involved both an in-hospital examination and a subsequent laryngoscopy after more than 2 months following extubation or decannulation. Surveillance methods also included radiologic evaluation,14,15 patient interviews, and autopsies in patients who died during the study period. 13 In 1 study, no information was given regarding the methods for surveillance of laryngotracheal pathology. 23 In another study of patients at the same hospital, however, the authors retrospectively analyzed data of prospectively collected data in patients who had been systematically screened using methods that included clinical signs, functional respiratory function tests, and bronchoscopy. 24 No information is given about whether the data collectors were blinded to the patients’ group allocation.
Loss to follow-up, patient mortality, and incomplete outcome reporting decreased the number of enrolled patients available for outcome assessment and increased the risk of bias in the included studies. Nearly half of the patients in Rumbak et al 14 died. In this study, there were more deaths in the delayed tracheostomy group (n = 37, 61.7%) compared to the early tracheostomy group (n = 19, 31.6%), producing a differential loss to follow-up. No information was reported regarding evaluation of LTS in these patients. Autopsies were performed on 63 of 86 (73.3%) patients who died in Stauffer et al 13 to evaluate for laryngeal and tracheal injuries both grossly and microscopically. Multiple centers that enrolled patients in Sugerman et al 22 did not submit data forms for analysis to the lead investigators, and many of the patients with head injuries were transferred to rehabilitation hospitals and were not examined with postextubation laryngoscopy.
Discussion
While endotracheal intubation provides a route for ventilatory assistance in critically ill patients, its use must be balanced against the risks of both short- and long-term complications compared to those of the alternative methods for providing respiratory support. LTS is a known complication of endotracheal intubation caused by pressure from the endotracheal tube and the inflated cuff. LTS has previously been found to be associated with the duration of intubation, the size of the endotracheal tube, high cuff pressure, traumatic intubation, and reintubation. Comorbid disease processes such as diabetes mellitus and airway infection are also associated with an increased risk of acquired LTS.25,26 Iatrogenic causes of LTS are associated with higher rates of tracheostomy dependence compared to traumatic or idiopathic causes. 27 Performance of early tracheostomy purports to reduce the sequelae of mechanical ventilation via an endotracheal tube, but there is controversy regarding the optimal timing of this procedure.
In the present analysis, our goal was to determine added risk of LTS in patients undergoing tracheostomy following longer periods of endotracheal intubation. This would allow LTS to be better factored into the clinical decision-making and informed consent processes. In studies with the lowest risk of selection bias due to their properly randomized designs, there was no significant difference in the incidence of LTS between early and late tracheostomy groups. One of the quasi-randomized studies found a higher rate of LTS in the early tracheostomy group among those who survived to follow-up, but there was no significant association between the duration of endotracheal intubation or tracheotomy and the overall amount of laryngotracheal injury found at autopsy in patients who died during the study. 13
In all 3 of the cohort studies, there was a moderate difference favoring a decreased incidence of LTS in patients undergoing early tracheostomy. The cohort studies are at greater risk of bias, especially confounding by indication. It is not clear, however, to what degree the results were affected by this bias, and differences may reflect an actual phenomenon. If the duration of endotracheal intubation were a consistent cause of LTS in the time frames studied, it would be expected to be reflected in the outcomes of the randomized trials. Furthermore, in the cohort studies, the patients in the late tracheostomy groups were not always converted to tracheostomy by day 14 of intubation, extending the time frame for late tracheostomy beyond what was accepted in the randomized trials and allowing for a greater risk of time-dependent effects of endotracheal intubation.
Treatment protocols that leave the decision about when a patient undergoes tracheostomy up to the treating physician may further bias outcome comparisons because physicians may be less likely to recommend surgery when patients are less ill and there is greater hope that the patients will able to extubate soon, or physicians may delay the conversion to tracheostomy in patients who are deemed not good candidates for surgery or who are not expected to survive long enough to benefit from the procedure. This may explain, in part, the consistent negative impact associated with late tracheostomy in the cohort studies. In the 2 studies on spinal cord trauma patients, patients in the late tracheostomy groups had higher Acute Physiology and Chronic Health Evaluation II scores, longer total time of mechanical ventilation, and longer total ICU days compared to the early tracheostomy group.23,24 In another study, 15 patients were rarely converted to tracheostomy before problems were observed or suspected. While these problems could have occurred due to the duration of endotracheal intubation itself causing pathology, these decisions select for patients at higher risk of LTS. Given these clinical differences in the patients who were selected for the late tracheostomy groups in these studies, it is possible that their higher acuity accounts, at least in part, for the increase in LTS reported in these cohorts.
A systematic review and meta-analysis of 17 RCTs found no difference in major periprocedural and long-term complications between percutaneous dilatational tracheostomy and operative tracheostomy in critically ill patients. 28 In the 2 studies included here that specified that only 1 tracheostomy method was used, whether percutaneous 14 or surgical, 21 there was no significant difference in complications.
One notable finding among the different ICU settings of the included studies was the markedly increased incidence of major laryngotracheal pathology in patients with rigid posture due to head injury compared to patients without head injury or head injury with nonrigid posture (8/24 patients [33%] vs 3/50 [6%]). 21 Dunham and LaMonica 21 attributed this to repeated Valsalva maneuvers and tonic activity of the strap muscles during acute and chronic muscular rigidity. When patients with rigid posture vs those without were stratified between early and late tracheostomy, no significant difference in the incidence of LTS was found. This suggests that patients with rigid posture due to head injury have an increased risk of injury that may occur within the first few days of intubation. While it may be easier to predict the need for long-term ventilatory support in severely neurologically compromised patients, early tracheostomy in these patients is not associated with better outcomes. Early tracheostomy is associated with a decrease in the total days of mechanical ventilation in patients with severe head trauma but also with an increased risk of hospital death.29-31 Taken together, these results do not show a clear benefit to early tracheostomy in patients with severe head trauma.
While the true incidence of LTS is not clear, in a large, retrospective study of 1130 consecutive tracheostomies, 32 there were 21 cases of tracheal stenosis (1.9% incidence). Among the studies included in this review, the mean incidence of stenosis was much higher at 8.9% (range, 0%-20.8%). This increased incidence may reflect the greater risk of LTS in patients who undergo tracheostomy after a longer period of endotracheal intubation compared to patients for whom tracheostomy was performed for other reasons, including extensive maxillofacial trauma, upper airway obstruction, or as an adjunct to head and neck surgery. An increase in LTS, however, is also likely to be observed in a study with a defined protocol for surveillance of all the patients who undergo tracheostomy compared to a retrospective review of tracheostomies, which would likely miss stenosis in asymptomatic or mildly symptomatic patients. The surveillance of all patients who undergo tracheostomy in these studies suggests a meaningful risk of LTS even when tracheostomy is performed within 1 week of intubation.
Altogether, relatively few studies addressed the incidence of LTS in early vs late tracheostomy, and their methods were quite varied. The 7 included studies varied in their methods of patient selection, group allocation, ICU setting, and surveillance of laryngotracheal pathology. There was no one definition of “early” and “late” tracheostomy, limiting the comparability of results of some of these studies, although in the included studies, all patients in the early tracheostomy groups were scheduled to undergo tracheostomy within 7 days after the initiation of endotracheal intubation, and all patients in the late tracheostomy groups were assigned to undergo tracheostomy no earlier than day 8 of intubation. The heterogeneity of inclusion criteria, patient demographics, treatment techniques, and timing of tracheostomy prevent true meta-analysis of the included studies.
Based on the evidence available, there is a notable risk of LTS in patients undergoing long-term mechanical ventilation who are converted from endotracheal intubation to tracheostomy within 7 days of intubation. Although the included studies evaluated various end points in their late tracheostomy groups, there does not appear to be a significant decrease in the incidence of LTS in the early tracheostomy groups. While it is preferable to not subject patients to additional procedures such as tracheostomy, previous studies have found that physicians have a limited ability to predict which patients will require extended ventilatory support, 7 and common clinical scales have poor predictive value in identifying which patients will be able to undergo early extubation. 33 Thus, clinical decision making should rely on other factors to determine when is the best time to perform a tracheostomy in an intubated patient. Future investigation should examine ways to decrease the risk of laryngotracheal injury that can occur within the first few days of intubation and improve posttracheostomy screening to identify early cases of LTS, which are associated with better treatment outcomes compared to those that undergo later treatment. 34
This analysis is limited due to the small number of available studies meeting the inclusion criteria. Using the average incidence of LTS in the late tracheostomy groups as a baseline estimate (namely, 10.9%), designing a study with α = 0.05 and power = 0.8 would require a sample size of 826 individuals (with 413 in each group) to find a significant difference, if the proposed study anticipates half the incidence of LTS in the intervention group.
Conclusion
Endotracheal intubation and conversion to tracheostomy within 1 week carries a noteworthy risk of LTS. In studies with the least risk of selection bias due to their properly randomized design, there were no differences in the risk of LTS in patients who were intubated for long-term mechanical ventilation and underwent early tracheostomy compared to patients who underwent late tracheostomy. The timing of tracheostomy should be individualized, and early tracheostomy, as defined by the studies in this review, does not significantly decrease the risk of LTS.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.