
Abstract
Objectives
Conventional reporting of posttympanoplasty hearing outcomes use a pure-tone averaged air-bone gap (ABG) largely representing a low-frequency sound conduction. Few studies report high-frequency conductive hearing outcomes. Herein, we evaluate high-frequency ABG in patients following temporalis fascia total drum replacement.
Study Design
Case series with chart review.
Setting
Tertiary care center.
Subjects and Methods
All patients who underwent type 1 tympanoplasty using a lateral graft total drum replacement technique between August 2016 and February 2019 were identified. Patients with pre- and postoperative audiograms were included. Low-frequency ABG was calculated as the mean ABG at 250, 500, and 1000 Hz. High-frequency ABG was calculated at 4 KHz. Pre- and postoperative ABGs were compared.
Results
Twenty-three patients were included, and the mean age at surgery was 44 years (range, 9-68 years). Perforation etiology was from trauma (n = 14) or chronic otitis media (n = 9). Preoperative mean low-frequency ABG was 27.8 ± 12.6 dB and mean high-frequency ABG was 21.5 ± 15.1 dB (P = .044). Postoperatively, the mean low-frequency ABG was significantly reduced by 15.5 ± 13.3 dB (P < .001) while the mean high-frequency ABG insignificantly changed (reduced by 2.6 ± 16.2 dB, P = .450).
Conclusion
In a series of patients undergoing temporalis fascia total drum replacement, low-frequency ABG improved; however, high-frequency conductive hearing loss persists. Conventional methods of reporting ABG may not identify persistent high-frequency ABG. These results merit further study across a range of tympanoplasty graft materials and surgical techniques.
Keywords
Tympanic membrane (TM) perforation is a common cause of conductive hearing loss in pediatric and adult populations. Large survey-based studies report prevalence rates of 0.45% in adults 1 and 1.2% to 4% in children.2,3 TM perforations most commonly result from otitis media or middle ear trauma, including foreign body perforation and barotrauma. 4 Clinically, patients with TM perforations experience hearing loss, otorrhea, and otalgia, and water precautions must be observed to avoid recurrent infections.
Type 1 tympanoplasty is a common surgical approach to reconstruct the TM in an effort to reestablish a protective barrier for the middle ear and restore the normal conductive hearing pathway. As the functional goal of tympanoplasty is to improve middle ear sound conduction, multifrequency audiometry is routinely used to clinically assess pre- and postoperative hearing. Despite collecting data from a wide spectrum of frequencies, the postoperative hearing outcomes that are routinely published are often condensed in a manner that makes them challenging to interpret. This is not only due to the use of a single pure-tone average (PTA) air-bone gap (ABG) meant to represent a range of frequencies, but it is also due to the wide variability in methods employed for calculating ABG. Several studies have used a low-frequency biased 3-tone average ABG at 500, 1000, and 2000 Hz,5-8 while others have reported a 4-tone average including either 3000 or 4000 Hz.9-15 In 1995, the Hearing Committee of the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) attempted to quell this variability by releasing a standardized format for reporting hearing outcomes, which recommended a 4-tone average ABG including 500, 1000, 2000, and 3000 Hz. 16 This was expanded upon in a 2012 update that introduced scattergrams relating 4-tone PTA thresholds to word recognition scores (WRSs). 17 Although reporting standards have helped to homogenize ABG data, there are still limitations in understanding frequency-specific outcomes since current guidelines remain biased toward low- and mid-frequency hearing. As a consequence, they may fail to communicate changes to high-frequency hearing, leaving little to be known about high-frequency hearing loss or gain following middle ear surgery.
In this study, we assess high-frequency conductive hearing outcomes in patients having undergone type 1 tympanoplasty using a total drum replacement technique. Frequency-specific changes in ABG are analyzed and compared to standard reporting techniques in an effort to (1) understand high-frequency conductive hearing outcomes after tympanoplasty and (2) analyze the sensitivity of standardized reporting methods for identifying postoperative high-frequency hearing loss.
Methods
Subjects
The charts of all patients who underwent type 1 tympanoplasty at a single tertiary care center from August 2016 to February 2019 were reviewed. Inclusion criteria were patients with either a subtotal or total TM perforation, reconstruction using a temporalis fascia lateral graft total drum replacement technique, and available pre- and postoperative audiograms. Exclusion criteria included patients without perforation closure, canal wall-down mastoidectomy, ossiculoplasty, and/or the use of cartilage grafting of the TM. Institutional review board (IRB) approval was obtained from the University of Massachusetts Medical School Human Subjects Committee: approval H00017444.
Surgical Technique
All type 1 tympanoplasties were performed using a lateral graft total drum replacement technique by a single surgeon with patients under general anesthesia. Specifically, a postauricular incision was made to harvest the temporalis fascia graft. Any native TM tissue was removed, including the fibrous tympanic annulus. A standard canaloplasty was performed, removing the anterior and inferior bony overhangs, to allow a 360-degree visualization of the bony tympanic annulus. Ossicular continuity and mobility were confirmed prior to placing the fascia graft lateral to the bony annulus but medial to the manubrium of the malleus. 18 The fascia graft and exposed bony ear canal wall were lined with split-thickness skin grafts before application of a rosebud dressing. 19 This consisted of silk strips soaked in mineral oil and packed with cotton impregnated with antibiotic solution.
Audiometric Evaluation
Standard pure-tone air and bone conduction threshold audiometry was performed on all patients before and following surgery. Pure-tone thresholds for air and bone conduction at 250, 500, 1000, 2000, 3000, and 4000 Hz were recorded. At each frequency, the ABG was calculated as the difference between the pure-tone air conduction and the pure-tone bone conduction.
Low-frequency air-bone gap was calculated as the mean ABG at 250, 500, and 1000 Hz. High-frequency air-bone gap was calculated at 4000 Hz.
In accordance with the recommended reporting methods by the AAO-HNS, 17 hearing results were also depicted in a scattergram format relating the average ABG pure-tone threshold to the WRSs. PTAs were calculated for both air conduction and bone conduction by averaging the patient’s thresholds at 500, 1000, 2000, and 3000 Hz. In cases where 3000 Hz was not measured, this value was calculated as an average of the 2000- and 4000-Hz thresholds. 17 The pure-tone average air-bone gap (PTA-ABG) was then calculated as the difference between the air conduction PTA and the bone conduction PTA. Patients without tested discrimination scores (due to non-English or Spanish primary language) were excluded. All audiometric data were collected from the pre- and postoperative audiograms that were performed closest to the date of surgery.
Statistical Analysis
All audiometric values are reported as the mean and standard deviation (SD). Student t test (2-tailed, paired) was used to compare measurements between low- and high-frequency ABG. Single-factor analysis of variance (ANOVA) was used to test for between-group differences when outcomes were stratified according to patient age and duration of perforation. Significance was set at P < .05 for all statistical tests. Kolmogorov-Smirnov normality test was used to confirm that all continuous variables planned for statistical significance testing were normally distributed.
Results
Twenty-nine patients were identified during the specified period. Of these, 6 were excluded for missing pre- or postoperative audiograms. Each of the remaining 23 patients ( Table 1 ) had a successful temporalis fascia total drum replacement for a total or subtotal TM perforation, as demonstrated in Figure 1 . Age of patients ranged from 9 to 68 years, with a mean age of 44 years. Ten patients (43%) were female and 15 (65%) were right ears. Perforation etiology was from trauma in 61% of patients (n = 14) or chronic otitis media in the remaining 39% (n = 9). Average time from surgery to postoperative audiogram was 6.7 months, with a range of 2.1 to 28.4 months.
Patient Demographics (N = 23).
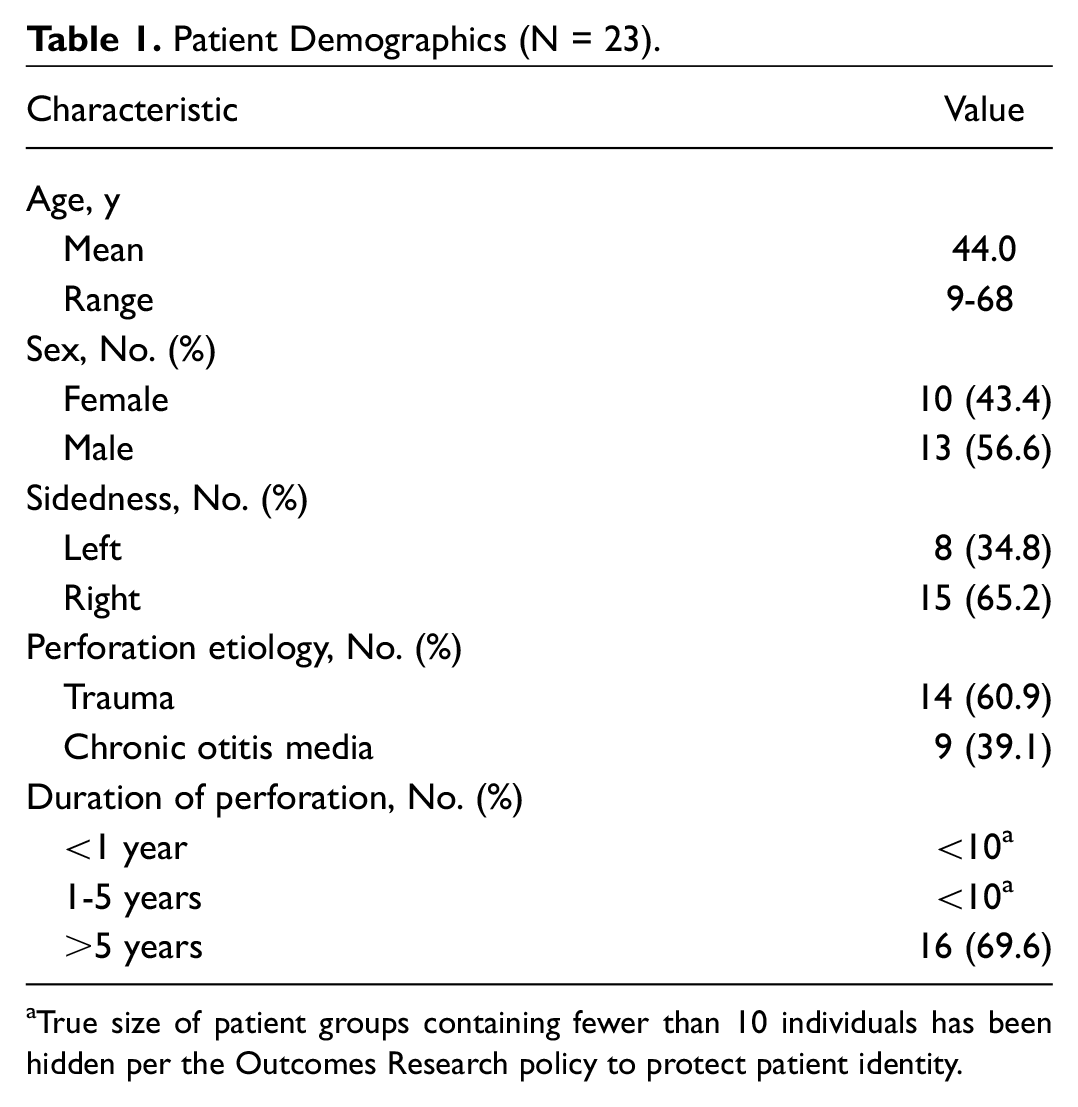
True size of patient groups containing fewer than 10 individuals has been hidden per the Outcomes Research policy to protect patient identity.
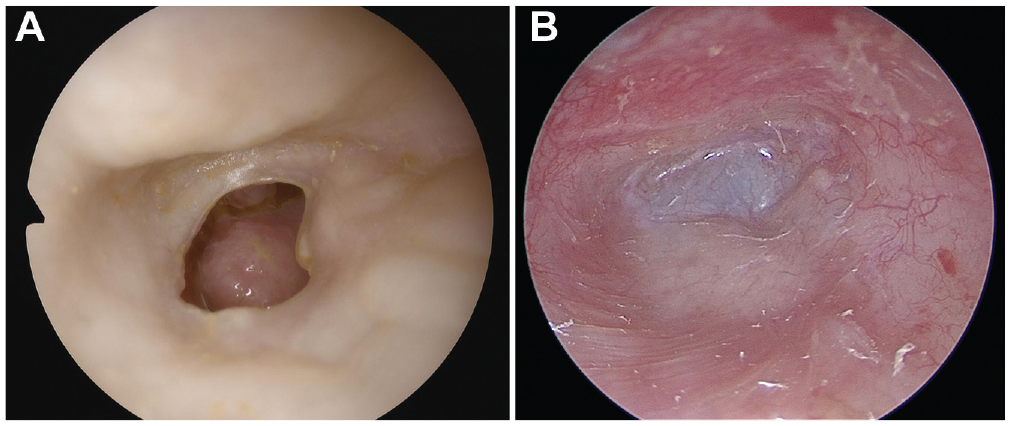
Representative endoscopic images demonstrating a preoperative subtotal tympanic membrane perforation (A) and postoperative repair (B) via type 1 tympanoplasty total drum replacement technique using temporalis fascia.
Hearing Results
Pre- and postoperative ABGs were compared for all patients and are summarized in Table 2 . The preoperative mean low-frequency ABG (27.8 ± 12.6 dB) was significantly larger than the mean high-frequency ABG (21.5 ± 15.1 dB, P = .044). Postoperatively, the mean low-frequency ABG was significantly reduced by 15.5 ± 13.3 dB (P < .001) while the mean high-frequency ABG was not significantly changed (reduced by 2.6 ± 16.2 dB, P = .450).
Individual Patient Audiometric Outcomes.
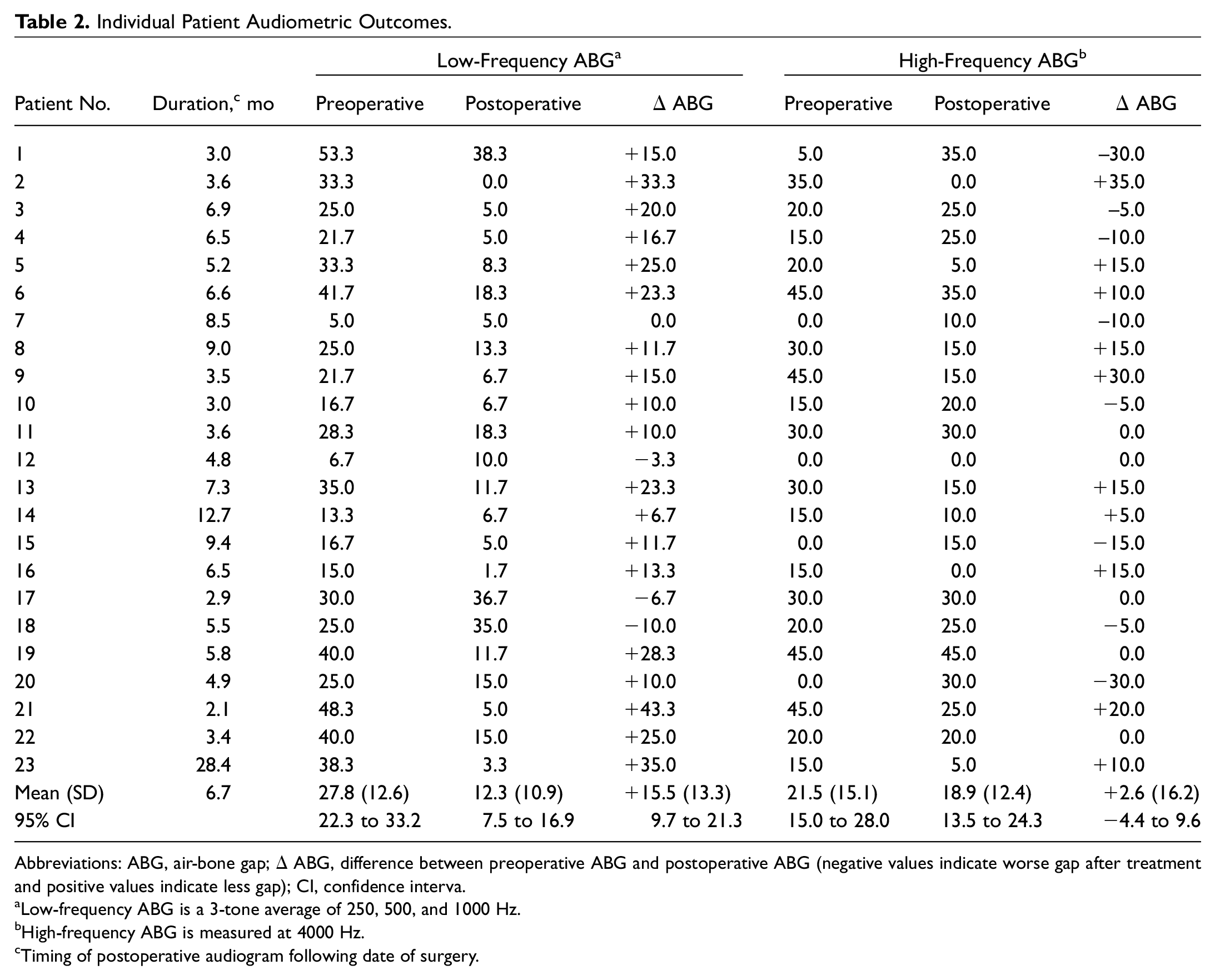
Abbreviations: ABG, air-bone gap; Δ ABG, difference between preoperative ABG and postoperative ABG (negative values indicate worse gap after treatment and positive values indicate less gap); CI, confidence interva.
Low-frequency ABG is a 3-tone average of 250, 500, and 1000 Hz.
High-frequency ABG is measured at 4000 Hz.
Timing of postoperative audiogram following date of surgery.
Ten patients (43%) experienced a reduction in high-frequency ABG while 8 other patients (35%) had a worsening of their high-frequency ABG; the remaining 5 (22%) experienced no change. In comparison, 19 patients (83%) experienced a reduction in low-frequency ABG, while only 3 (13%) had a worsening of their low-frequency ABG; the remaining 1 (4%) experienced no change. The magnitude of improvement was larger for low-frequency ABG compared to that for high-frequency ABG (P < .001). Postoperatively, the mean low-frequency ABG (12.3 ± 10.9 dB) was lower than the mean high-frequency ABG (18.9 ± 12.4 dB) (P = .008). No significant between-group differences were observed when outcomes were stratified according to patient age and duration of perforation. Representative audiograms from 2 patients are demonstrated in Figure 2 .
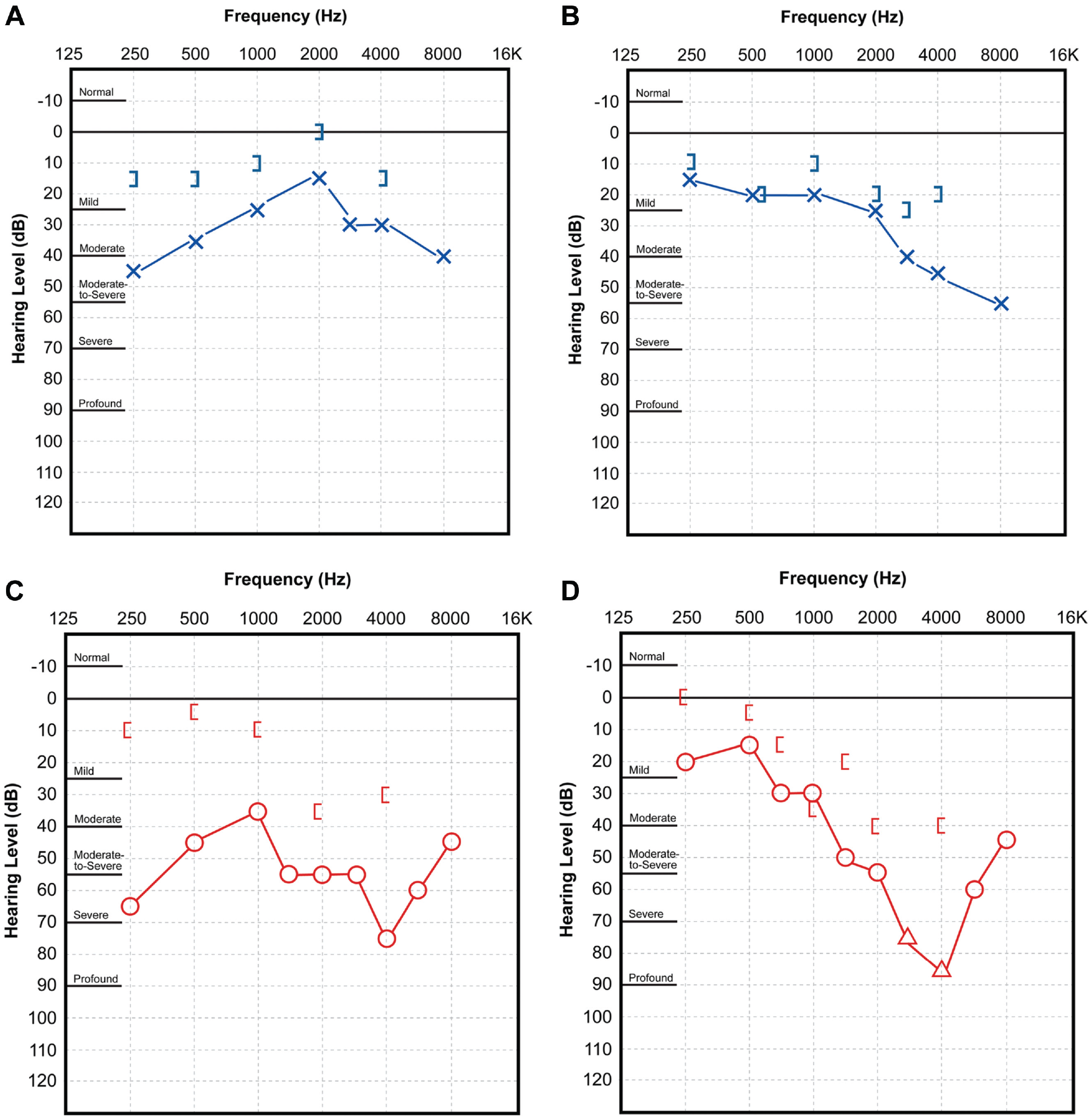
Representative audiograms demonstrating near closure of the low-frequency air-bone gaps (ABGs) but worsening high-frequency ABG (4000 Hz). Patient 4: Left ear preoperative (A) and postoperative (B). Patient 19: Right ear preoperative (C) and postoperative (D).
When reported in accordance with the AAO-HNS guidelines, 17 preoperative PTA-ABG was 20 ± 11 dB. Postoperatively, the PTA-ABG significantly improved to 10 ± 8 dB (P < .001). The change in air-bone gap was 10 ± 12 dB. Results for the 21 patients with available word recognition scores are mapped into pre- and posttreatment scattergram plots shown in Figure 3 .
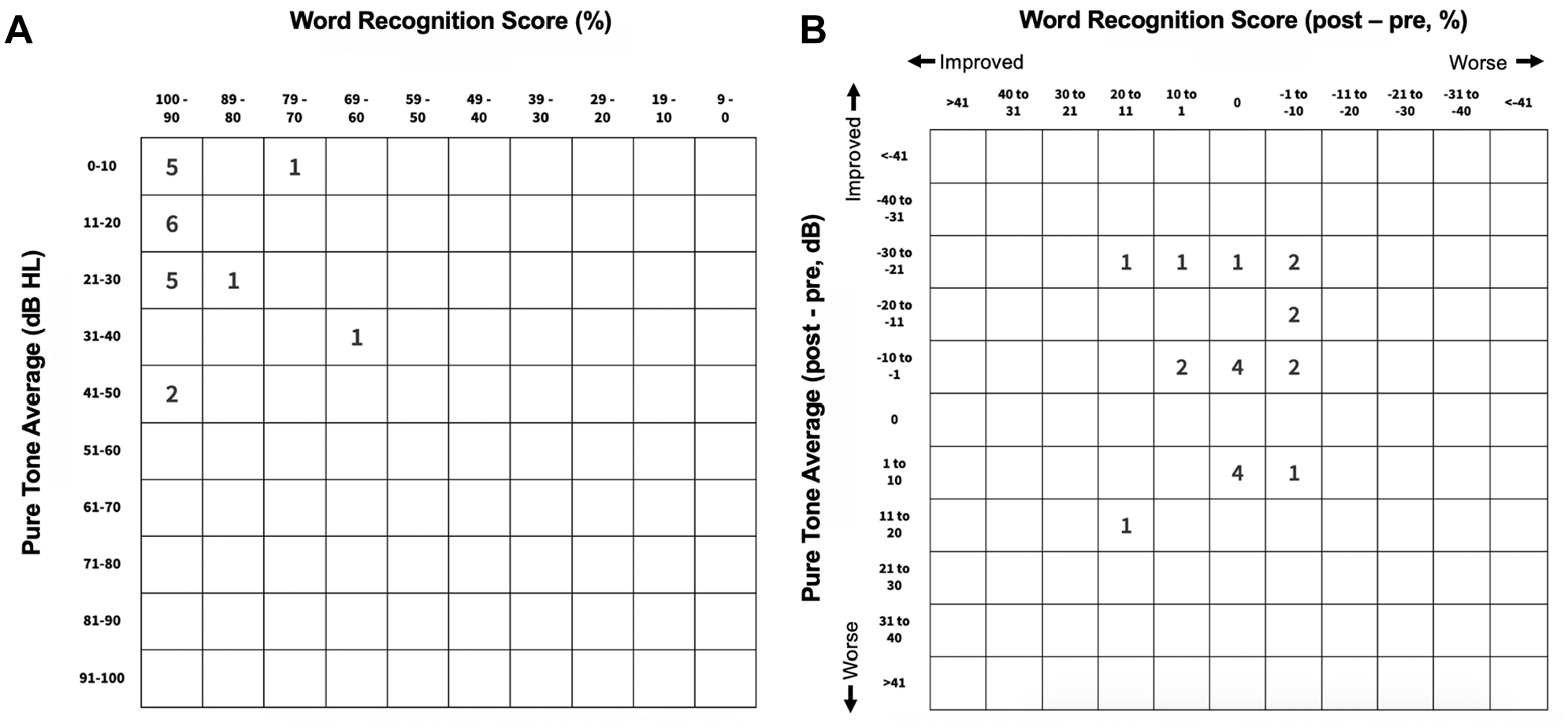
Scattergrams relating word recognition scores (WRSs) and 4-frequency pure-tone average air-bone gap (PTA-ABG) as per American Academy of Otolaryngology–Head and Neck Surgery recommendations. Scattergrams for pretreatment (A) and postoperative changes (B) include the 21 patients with available WRSs.
Discussion
This study is the first to our knowledge that investigates frequency-specific changes in conductive hearing for patients with total or subtotal perforations who underwent total replacement of the TM with a temporalis fascia graft. We found that surgery did not ameliorate conductive hearing loss at high frequencies despite perforation closure and a significant ABG improvement at low frequencies. If reported using traditional methods, 17 our findings would suggest that, on average, patients had improved hearing postoperatively, as demonstrated by the scattergram in Figure 3 . However, this method of reporting fails to recognize the large high-frequency conductive deficit seen in the majority of our patients, as demonstrated in Table 2 . Our results indicate that persistent high-frequency hearing loss may be “hidden” behind a low-frequency biased PTA calculation. As such, it is difficult to determine the prevalence of persistent high-frequency conductive deficits following middle ear surgery given the sparsity of previous studies that report frequency-specific outcomes.
Conversely, low-frequency hearing improvement after type 1 tympanoplasty using temporalis fascia is expected, and outcomes demonstrating consistent results have been widely reported. One retrospective study of 41 ears noted that the best audiometric outcomes were found in the lower frequencies between 250 and 1000 Hz; however, frequency-specific data were not described in detail. 15 Another retrospective review of 10 ears reported an improvement of the ABG across all frequencies (0.5-4 kHz), with the magnitude of ABG closure inversely related to the increase in frequency; however, the statistical significance was not made clear. 20 In both cases, low-frequency benefits were clearly demonstrated, but high-frequency outcomes were not addressed.
The clinical impact of high-frequency conductive hearing loss is multifold. High-frequency hearing loss impairs one’s ability to understand speech, which may result in poor word discrimination, particularly in the presence of background noise. 21 The ability to hear above 5 kHz has also been found to be important for sound localization and language comprehension, especially when there are multiple sources of speech. 22 Furthermore, a significant amount of environmental sound occurs at and above 4 kHz. For patients with high-frequency ABG after middle ear surgery, additional testing, such as speech understanding in noise, may demonstrate persistent hearing handicaps. 23 Additional rigorous assessment of hearing deficits following middle ear surgery is needed to improve operative technique and outcomes.
Identification of pre- and postoperative high-frequency ABGs is the first step toward understanding its etiology and developing methods for correction. Patient factors, surgical techniques, and the properties of reconstructive materials may all influence high-frequency conductive hearing outcomes. Due to the retrospective nature of this study, we are unable to conclusively explain the persistent high-frequency ABG observed. However, all patients included underwent complete replacement of their TM with a single graft material, in the setting of a normal and mobile ossicular system. As such, we believe the persistent high-frequency conductive hearing loss may relate to the structural properties of the reconstructed TM. Although not causally tested, we can use prior work in TM mechanical modeling24-27 to explore the functional effects of those properties thought to be most influential—notably, the conical shape of the drum, the strength of graft adhesion to the ossicular chain, the relative thickness and stiffness of the reconstructed TM, and the fibrous structure of the graft.
The normal human TM is a thin, conically shaped multilayered structure containing a unique arrangement of radial and circumferential collagen fibers that facilitate the efficient conversion of sound waves from the external auditory canal into mechanical motion of the middle ear structures.24,28 Important to the conduction of high-frequency sound waves, especially above 3 kHz, is a network of radial fibers composed of type II collagen that densely converges at the manubrium and umbo to provide structural rigidity that complements the elastic type III collagen circular fibers within the TM periphery.24,25,27,29 Mechanically, this unique network contributes to the highly organized displacement pattern demonstrated by the normal TM when subjected to high-frequency sound waves.26,30
In comparison, the temporalis fascia graft is a more basic network of linearly oriented collagen fibers that contribute to a thicker but less rigid membranous structure.24,31 Despite retaining a conical shape on postoperative visual inspection, the cone’s depth can theoretically vary following tympanoplasty, thereby affecting sound conduction. Fay and colleagues 27 demonstrated the functional consequences of altered conical depth using TM models to show losses of greater than 20 dB at high frequencies for shallow eardrums, whereas low-frequency thresholds were unchanged. Furthermore, the reconstructed TM may be more loosely coupled to the manubrium and umbo, relative to the native TM. Although literature exploring the impact of coupling strength could not be found, any alteration can theoretically impair sound conduction at certain frequencies.
More thoroughly demonstrated by TM models, however, is the propensity of stiffer graft materials to exhibit improved high-frequency but worsened low-frequency sound conduction.25,27 As such, although beneficial at low frequencies, the flaccid nature of the fascia graft presumably impairs high-frequency sound conduction. We believe it is unlikely that anterior tympanomeatal angle (ATA) blunting is responsible for the persistent high-frequency deficits seen, since TM thickening secondary to ATA blunting should only impair low-frequency hearing. 32 Finally, it has been suggested that the thick, linear, type I collagen fibers that form the architecture of the temporalis fascia graft lack the elastic properties shown to be important for efficient high-frequency sound conduction in healthy TM models.24,33 Even years after surgery, these grafts fail to remodel into the native TM fibrous architecture. 31 Collectively, a functional consequence of the numerous structural shortfalls outlined in this discussion is a reconstructed TM that demonstrates asymmetric and irregular rather than highly organized displacement patterns when subjected to high-frequency sound waves. 26
An alternative explanation for persistent high-frequency hearing deficits following tympanoplasty relates to the claim that intraoperative ossicular manipulation and/or bony drilling induces postoperative sensorineural hearing loss (SNHL).34-36 At frequencies higher than 4 kHz, we cannot address this claim because of limitations in measuring ABG; however, we have clear evidence demonstrating the presence of a worsened or persistent ABG at 4 kHz and thus reason to believe that postoperative hearing losses above 4 kHz contain a conductive component.
This study is limited by the small sample size and retrospective nature of the review. In addition, this study did not compare grafts made of temporalis fascia with those made of other autologous or nonautologous materials, but this was intentional as our goal was to permit conclusions about a single reconstructive material. Future studies could compare frequency-specific audiometric outcomes between a variety of graft materials (eg, fascia, cartilage, nonautologous materials). Furthermore, future investigations into the shape and thickness of the reconstructed TM would allow us to better delineate the contribution of postoperative structure to hearing function. Finally, this investigation could be extended to patients who underwent ossicular manipulation to determine if different forms of ossiculoplasty could augment the capabilities of TM grafts. For now, however, it is clear that the standard of care approach to type 1 tympanoplasty provides far from optimal hearing outcomes, and this reiterates the importance of developing grafting techniques and materials that better mimic the microanatomical and mechanical properties of the native human TM, which have been shown to be critical for high-frequency sound transmission. 24
In summary, changes in conductive hearing following type 1 tympanoplasty via a temporalis fascia total drum replacement are frequency dependent. This is only identified when independently analyzing audiometric outcomes at high frequencies. We found a significant difference in both the magnitude of ABG closure and the postoperative ABG values at low frequencies relative to high frequencies, with substantially more patients experiencing improvements between 250 and 1000 Hz than at 4000 Hz. Current reporting standards for conductive hearing outcomes do not identify postoperative high-frequency hearing loss.
Conclusion
In a small series of patients undergoing type 1 tympanoplasty using a lateral graft total drum replacement technique, low-frequency ABG improved; however, high-frequency conductive hearing loss persists. Current reporting standards appear inadequate for the identification of persistent high-frequency ABGs.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank Cheryl Fikucki, AuD, Kristen Bates, and Cheryl Rice, APRN, for their assistance with collection of audiometric data, clinical images, and perioperative patient care.
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the AAO-HNSF 2019 Annual Meeting & OTO Experience; September 15-18, 2019; New Orleans, Louisiana.