
Abstract
Objective
To identify and seek consensus on issues and controversies related to ankyloglossia and upper lip tie in children by using established methodology for American Academy of Otolaryngology–Head and Neck Surgery clinical consensus statements.
Methods
An expert panel of pediatric otolaryngologists was assembled with nominated representatives of otolaryngology organizations. The target population was children aged 0 to 18 years, including breastfeeding infants. A modified Delphi method was used to distill expert opinion into clinical statements that met a standardized definition of consensus, per established methodology published by the American Academy of Otolaryngology–Head and Neck Surgery.
Results
After 3 iterative Delphi method surveys of 89 total statements, 41 met the predefined criteria for consensus, 17 were near consensus, and 28 did not reach consensus. The clinical statements were grouped into several categories for the purposes of presentation and discussion: ankyloglossia (general), buccal tie, ankyloglossia and sleep apnea, ankyloglossia and breastfeeding, frenotomy indications and informed consent, frenotomy procedure, ankyloglossia in older children, and maxillary labial frenulum.
Conclusion
This expert panel reached consensus on several statements that clarify the diagnosis, management, and treatment of ankyloglossia in children 0 to 18 years of age. Lack of consensus on other statements likely reflects knowledge gaps and lack of evidence regarding the diagnosis, management, and treatment of ankyloglossia. Expert panel consensus may provide helpful information for otolaryngologists treating patients with ankyloglossia.
Keywords
Introduction
Medical practitioners have long been concerned that a restrictive lingual frenulum could adversely affect a child’s health by interfering with the ability to breastfeed, speak, or perform mechanical/social skills, such as licking the lips or keeping the teeth clean. In 1679, a surgical textbook was published with woodcuts showing an infant’s frenulum being cut with scissors. 1 Midwives in the 18th century reportedly kept 1 fingernail long so that they could lyse the frenulum following birth to facilitate breastfeeding. 2
Over the past decade, there has been an exponential increase in the number of children diagnosed and treated with ankyloglossia in more affluent countries. A 2017 study by Walsh et al of pediatric inpatients in the United States demonstrated that between 2003 and 2012, there was a 4-fold increase in the number of newborns diagnosed with ankyloglossia and a 5-fold increase in the number of frenotomies. 3 Similarly, a 2017 study in Canada found “runaway” rates of frenotomy for infants in some territories. 4 In the Canterbury province of New Zealand, the frenotomy rate increased from a relative high of 7.5% to 11.3% in just 2 years (between 2013 and 2015). 5
Despite growing attention to ankyloglossia in recent years, the benefit of and indications for intervention are unclear and controversial, given the paucity of randomized controlled trials. 6 A Cochrane review of frenotomy in newborns concluded that it “reduced breastfeeding mothers’ nipple pain in the short term,” but the investigators did not find a consistent positive effect on infant breastfeeding. 7 A systematic review evaluating frenotomy for reasons other than breastfeeding found that “data are currently insufficient for assessing the effects of frenotomy on nonbreastfeeding outcomes that may be associated with ankyloglossia.” 8
Ideally, a clinical guideline would be developed to assist practitioners faced with infants and children with possible ankyloglossia; however, the quality and quantity of existing high-level evidence are insufficient for developing a multidisciplinary clinical practice guideline. Given this deficit, the American Academy of Otolaryngology—Head and Neck Surgery Foundation (AAO-HNSF) prioritized developing a clinical consensus statement (CCS) based on the views of expert panelists who actively treat patients with ankyloglossia and other oral ties. The objectives of the CCS are to identify areas of expert consensus—and nonconsensus—regarding the definitions of ankyloglossia, lip tie, and buccal tie; the indications for surgical intervention; perioperative management; and the expected outcomes.
Methods
This CCS was developed with an a priori protocol, 9 used by the AAO-HNSF to successfully develop multiple other consensus statements, with the following steps: (1) define the subject of a CCS as evaluation of the diagnosis, management, and treatment of ankyloglossia; (2) recruit the expert panel; (3) vet potential conflicts of interest among proposed panel members; (4) perform a systematic literature review; (5) determine the scope and population of interest for the CCS; (6) develop topic questions and consensus for statements for each topic question; (7) develop and implement modified Delphi method surveys; (8) revise the CCSs in an iterative fashion based on survey results; and (9) aggregate the data for analysis and presentation. The pertinent details of these steps are briefly described.
Determination of Ankyloglossia as the Topic of a CCS, Panel Recruitment, and Vetting
Ankyloglossia was proposed for a CCS by the American Society of Pediatric Otolaryngology. After deliberation, the AAO-HNSF Guidelines Taskforce approved and prioritized the suggestion; consensus panel leadership was selected; and administrative support was allocated. Panel membership was strategically developed to ensure appropriate representation of all relevant stakeholder groups and organizations within otolaryngology. The stakeholders were contacted regarding the consensus statement project and the requirements and desired qualifications for panel membership; each group then nominated its own representative content expert to participate.
The CCS development committee was made up of representatives from the American Society of Pediatric Otolaryngology; the Society of Ear, Nose, and Throat Advances in Children; the Triological Society; and appropriate committees within the AAO-HNSF, including the Board of Governors, the General and Sleep Clinical Advisory Committee, and the Pediatric Clinical Advisory Committee. The methodologists were nonvoting members of the development group.
All panel members are pediatric otolaryngologists in clinical practice who actively evaluate and treat children with ankyloglossia and other oral anomalies (including the performance of surgical procedures). All were required to agree in advance of appointment to participate in all verbal discussions (performed via teleconference) and votes. Once the panel was assembled, complete disclosure of potential conflicts of interest was reported and vetted within the group. Conflicts of interest were managed consistent with the Council of Medical Specialty Societies’Code for Interactions with Companies, 10 which requires that the chair and a majority of the participants do not have a direct conflict with the deliberations. The panel chair and assistant chair led the development of the clinical statements and the Delphi process with input from a senior consultant/methodologist from AAO-HNSF leadership and AAO-HNSF Guidelines Taskforce and with administrative support from an AAO-HNSF staff liaison.
Literature Review and Determination of the Scope of the Consensus Statement
Two systematic literature reviews were performed by an information specialist, using keywords identified by the development panel, to identify current evidence regarding the diagnosis, management, and treatment of ankyloglossia and oral ties.
The literature searches were conducted in December 2018 and March 2019 and restricted to year of publication from January 1, 2000, to December 31, 2018. Articles included all relevant publications in English from the following databases: PubMed, EMBASE, Cumulative Index to Nursing and Allied Health Literature, Cochrane Database of Systematic Reviews, Web of Science, Agency for Healthcare Research and Quality, ECRI National Guideline Clearinghouse, Canadian Medical Association Infobase, NHS Evidence ENT and Audiology, TRIP Database, Clinicaltrials.gov, Canadian Agency for Drugs and Technologies in Health, New Zealand Guidelines Group, Australian National Health and Medical Research Council, Guidelines International Network, and SCOPUS. The keyword strategy was as follows: (lingual frenum[mesh] OR ankyloglossia[mesh] OR ankyloglossia*[tiab] OR “tongue tie” OR “Tongue ties” OR tongue-tie OR tongue-ties OR Frenotom*[tiab] OR frenulotom*[tiab] OR frenulectom*[tiab] OR “lingual frenum” OR “lingual frenums” OR fraenectom*[tiab] OR frenulae[tiab])
The target audience of the CCS was defined as otolaryngologists treating patients with ankyloglossia in any clinical setting, including the operating room, ambulatory surgery center, physician’s office, and outpatient clinics. The target population was defined as children aged 0 to 18 years, including breastfeeding infants. Once the target population and scope of practice were determined, the panel used the results of the literature reviews, combined with its expert opinion and stakeholder needs, to identify and prioritize topics and questions for which knowledge gaps or uncertainty existed, which could most benefit from potential consensus from an expert panel. These areas were then used as the basis for the formulation of the initial statements, which were then evaluated through the Delphi survey method.
Delphi Survey Method Process and Administration
A modified Delphi survey method was utilized to assess consensus for the proposed statements, 9 with multiple anonymous surveys to minimize bias within the expert panel and facilitate consensus. 11
Web-based software (www.surveymonkey.com) was used to administer confidential surveys to panel members. A potential topic list of 37 questions was developed by the panel during the first call, and all panel members were invited to provide 1 draft statement for each of their top 5 ranked choices. The survey period was divided into 3 Delphi rounds. All answers were deidentified and remained confidential; however, names were collected to ensure proper follow-up, if needed.
Based on the outcomes of the top ranked topic list choices and resulting discussion, the panel chair and assistant chair developed the first Delphi survey, which consisted of 57 statements. Prior to dissemination to the panel, the Delphi surveys were reviewed by the methodologist for content and clarity. Questions in the survey were answered with a 9-point Likert scale (1 = strongly disagree, 3 = disagree, 5 = neutral, 7 = agree, 9 = strongly agree). The surveys were distributed, and responses were aggregated, distributed back to the panel, discussed via teleconference, and revised, if warranted. The purpose of the teleconference was to provide an opportunity to clarify any ambiguity, propose revisions, or drop any statements recommended by the panel.
The criteria for consensus were established a priori and are as follows 9 :
Consensus: statements achieving a mean score ≥7.00 and having no more than 1 outlier, defined as any rating ≥2 Likert points from the mean in either direction
Near consensus: statements achieving a mean score ≥6.50 and having no more than 2 outliers
No consensus: statements that did not meet the criteria of consensus or near consensus
Three iterations of the Delphi survey were performed. The panel extensively discussed (via teleconference) the results of each item after the first Delphi survey. Items that reached consensus were accepted, and items that did not meet consensus were discussed to determine if wording or specific language was pivotal in the item not reaching consensus. The second and third iterations of the survey were used to reassess items for which there was near consensus or for items for which there were suggestions for significant alterations in wording that could have affected survey results. All items reaching consensus were accepted, except for 4 statements that were removed due to redundancy. The factors leading to the remaining items not reaching consensus were not attributed to wording or other modifiable factors but rather a true lack of consensus.
The final version of the CCSs were grouped into specific topics: ankyloglossia (general); buccal tie, ankyloglossia, and sleep apnea; ankyloglossia and breastfeeding; frenotomy indications and informed consent; frenotomy procedure; ankyloglossia in older children; and maxillary labial frenulum (MLF). The items most likely to direct the practice of otolaryngologists were also grouped. The final manuscript was drafted with participation and final review from each panel member.
Results
The initial literature search yielded 202 articles, with 104 remaining after the titles and abstracts were screened for relevance. Additional exclusions at this stage included commentaries, letters to the editor, editorials, studies in animals, and research limited to adults. The remaining 104 articles were reviewed independently by the chair and assistant chair and classified per the Oxford Centre for Evidence-Based Medicine (CEBM) 2011 levels of evidence. 12 An additional 7 articles were included outside the literature searches on the basis of panel agreement of relevance and not being captured in the 2 literature searches. The CEBM evidence levels included 14 level 1 articles, 7 level 2 articles, 19 level 3 articles, 54 level 4 articles, and 17 level 5 articles.
A total of 89 clinical statements were developed for assessment throughout the 3 iterations of the Delphi survey. After removal of duplicative statements and combination of similar statements, 86 statements remained for assessment. All panelists completed all survey items. After 3 iterations of the Delphi survey, 41 statements (48%) met the standardized definition for consensus (
Tables 1
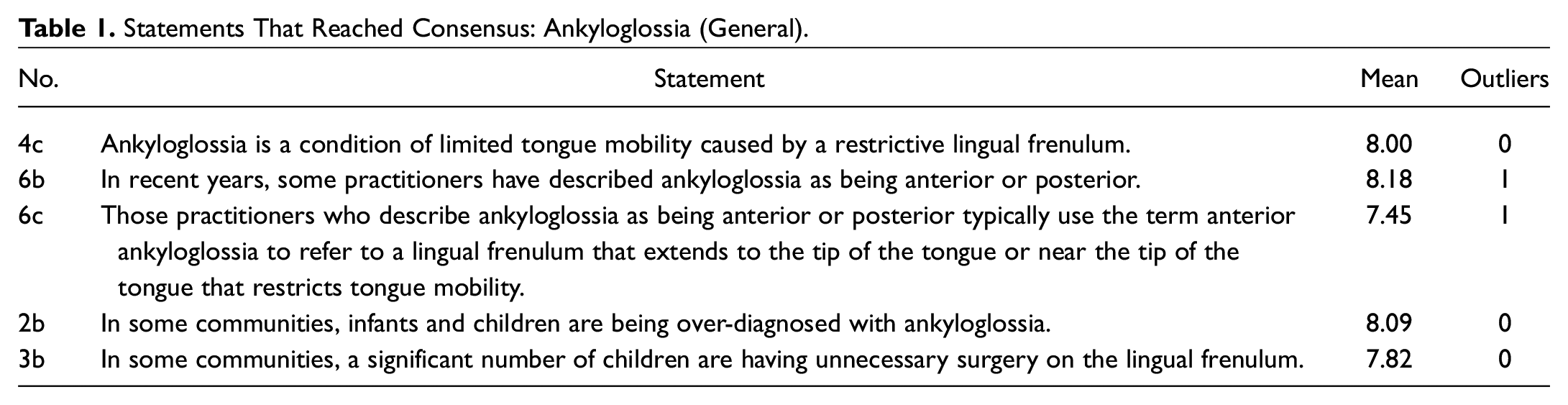
Statements That Reached Consensus: Ankyloglossia (General).
Statements That Reached Consensus: Buccal Tie/Ankyloglossia and Sleep Apnea.

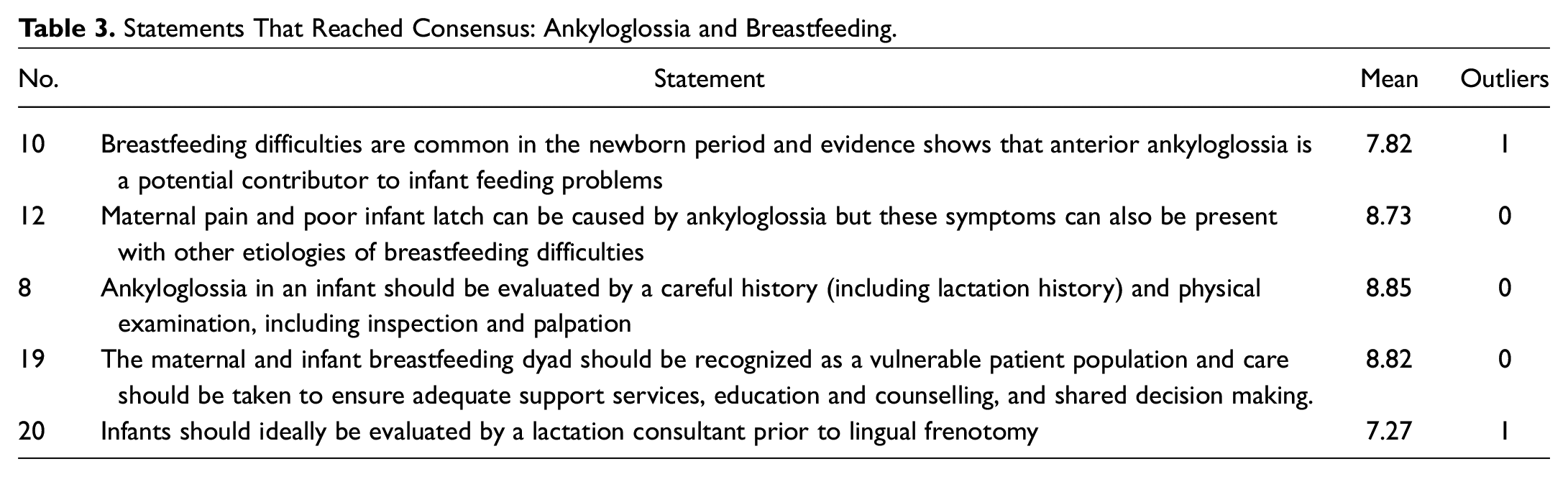
Statements That Reached Consensus: Ankyloglossia and Breastfeeding.
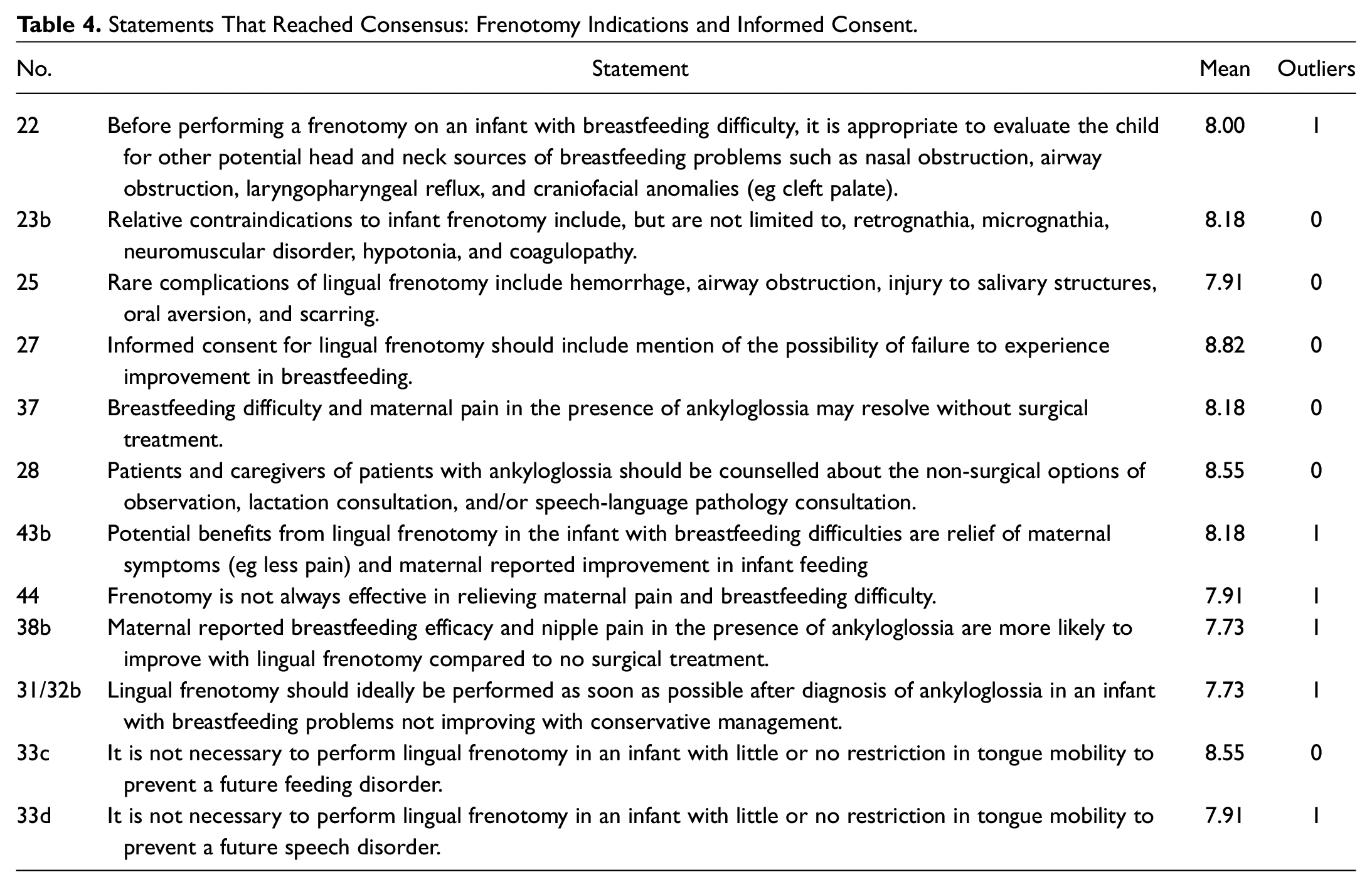
Statements That Reached Consensus: Frenotomy Indications and Informed Consent.
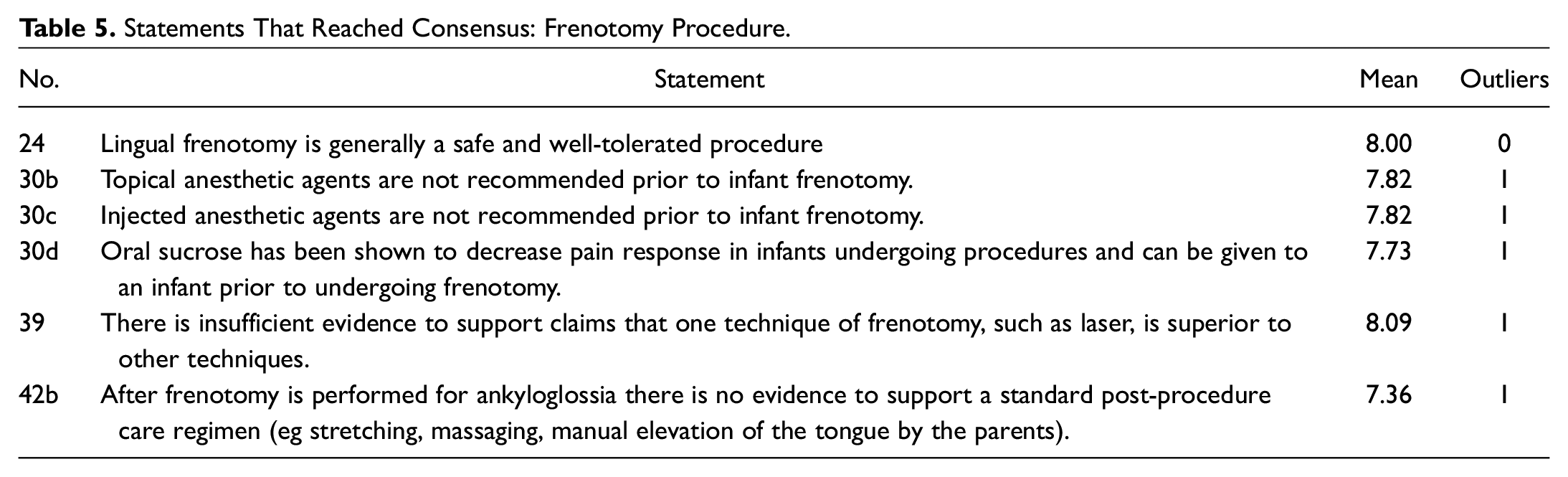
Statements That Reached Consensus: Frenotomy Procedure.
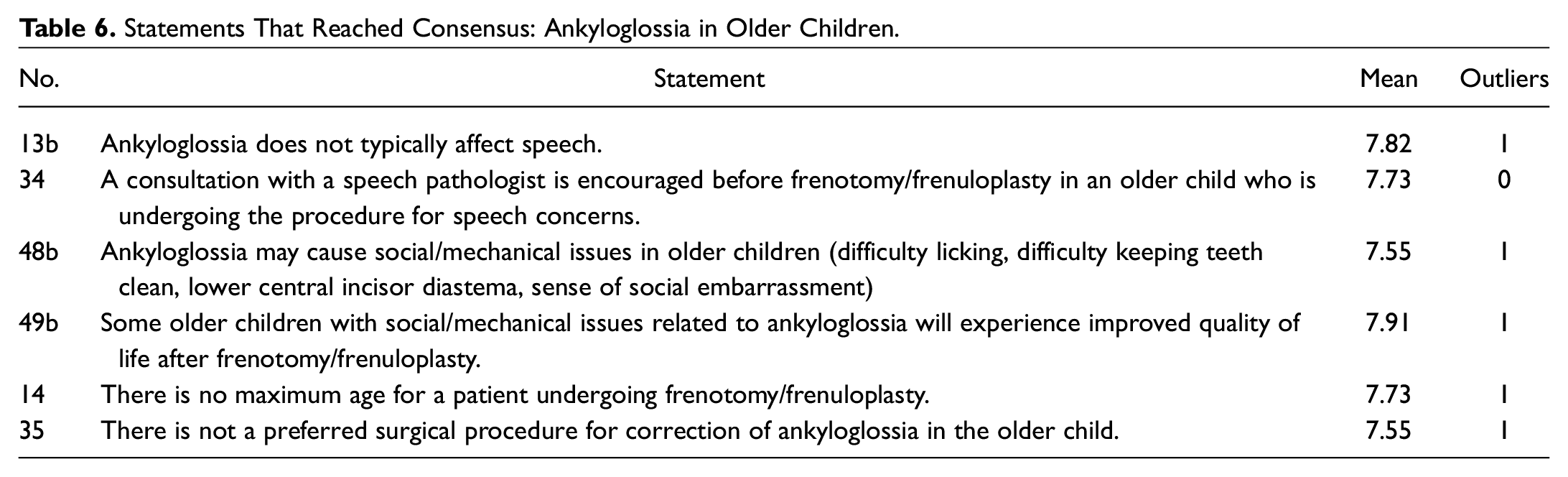
Statements That Reached Consensus: Ankyloglossia in Older Children.
Statements That Reached Consensus: Maxillary Labial Frenulum.

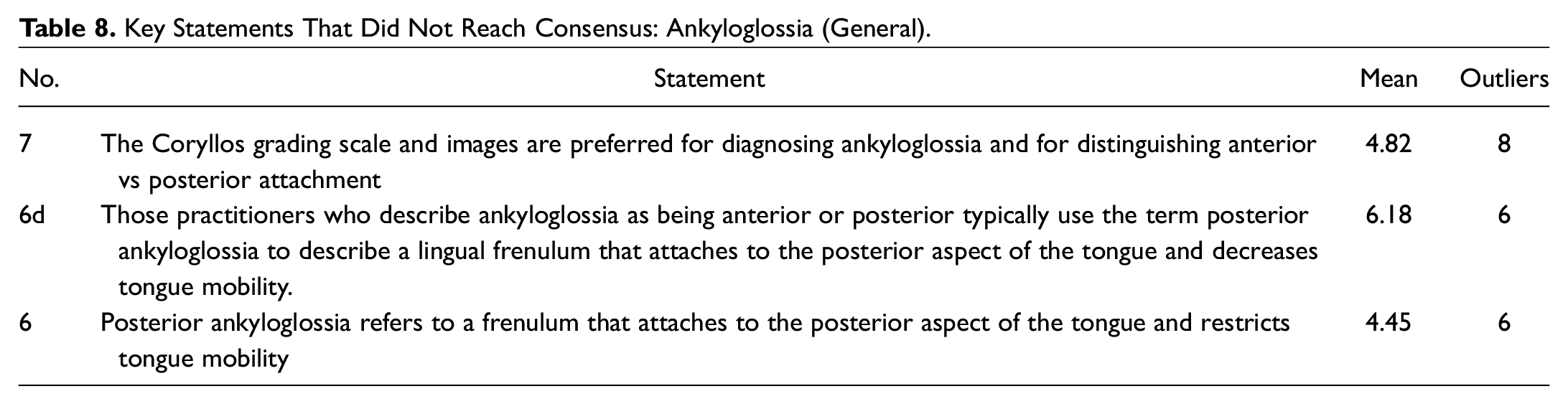
Key Statements That Did Not Reach Consensus: Ankyloglossia (General).
Key Statements That Did Not Reach Consensus: Ankyloglossia and Breastfeeding.

Key Statements That Did Not Reach Consensus: Infant Frenotomy. a
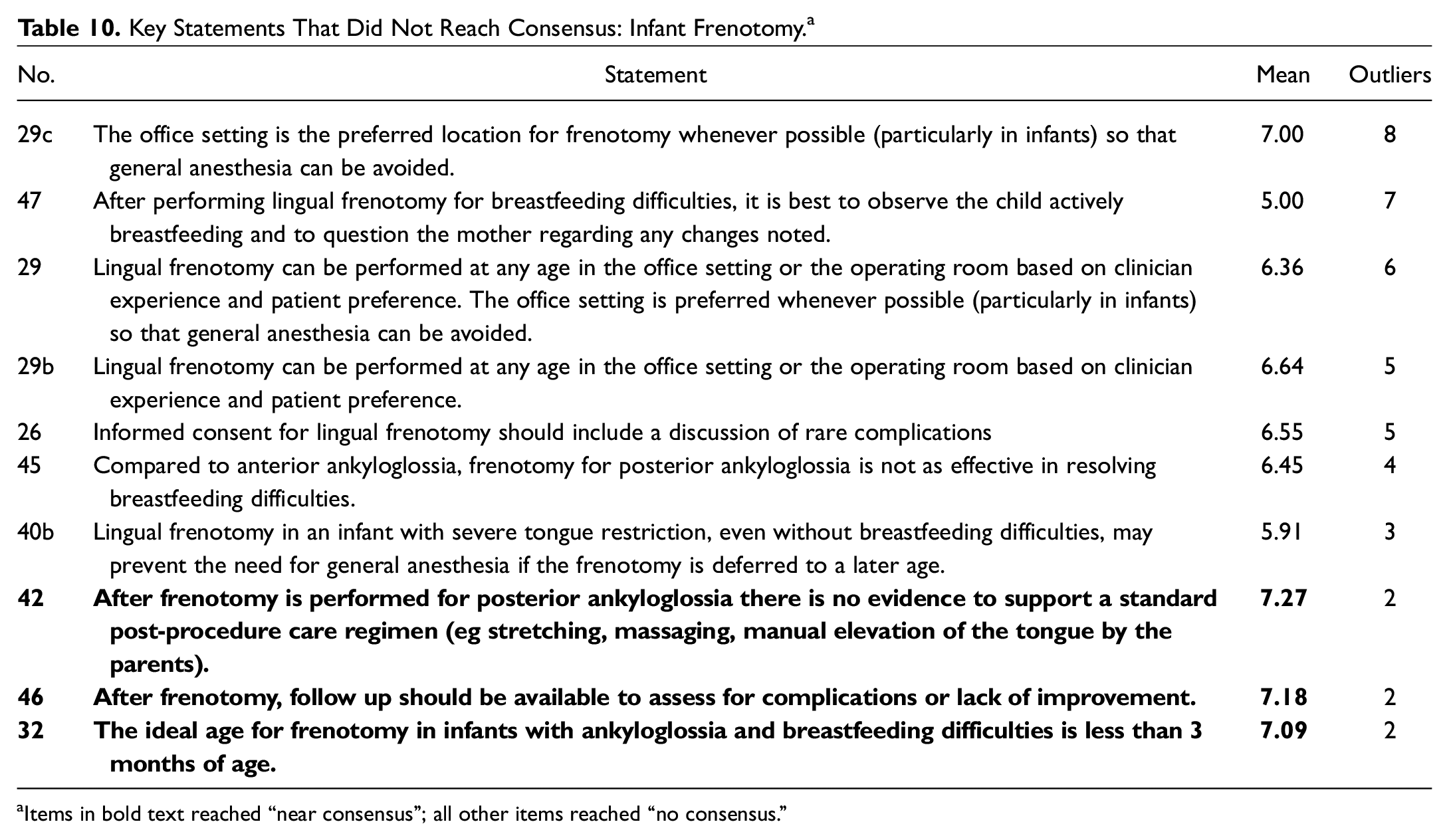
Items in bold text reached “near consensus”; all other items reached “no consensus.”
Key Statements That Did Not Reach Consensus: Ankyloglossia in Older Children.

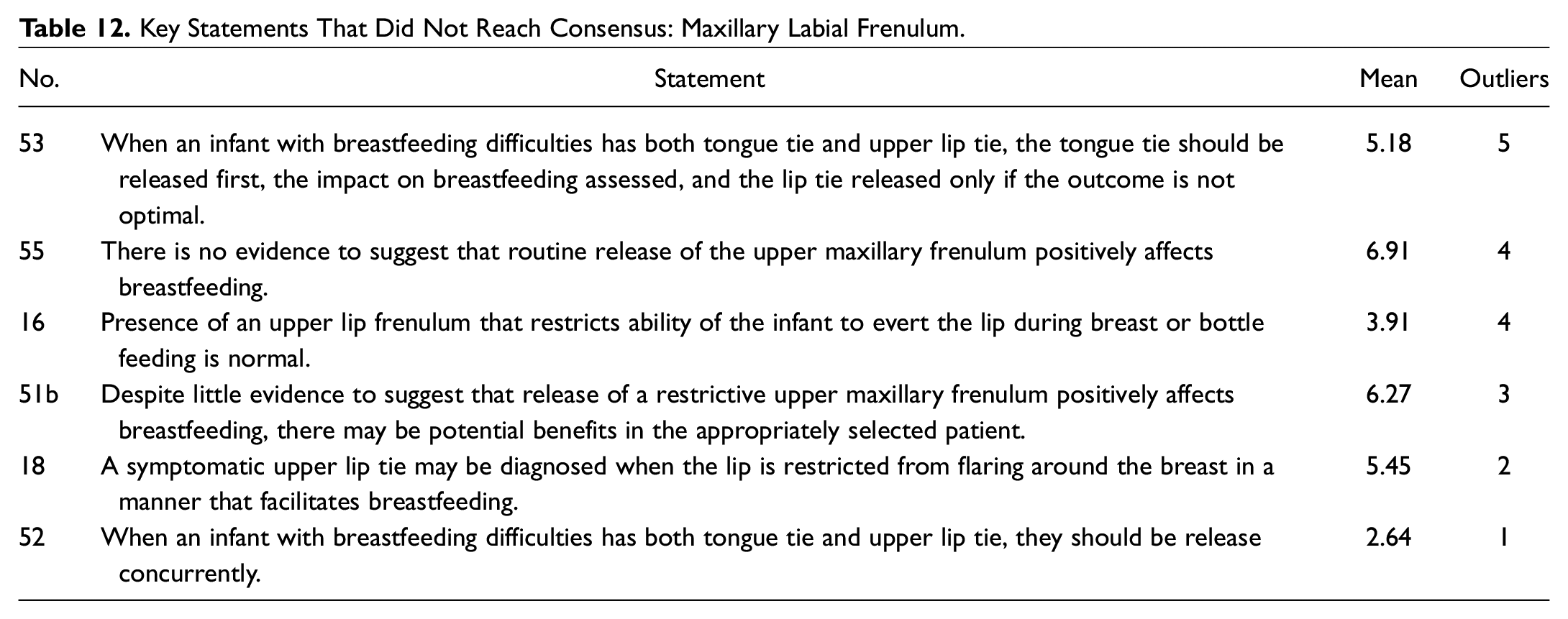
Key Statements That Did Not Reach Consensus: Maxillary Labial Frenulum.
Ankyloglossia and Oral Tie Action Statements for Clinicians. a
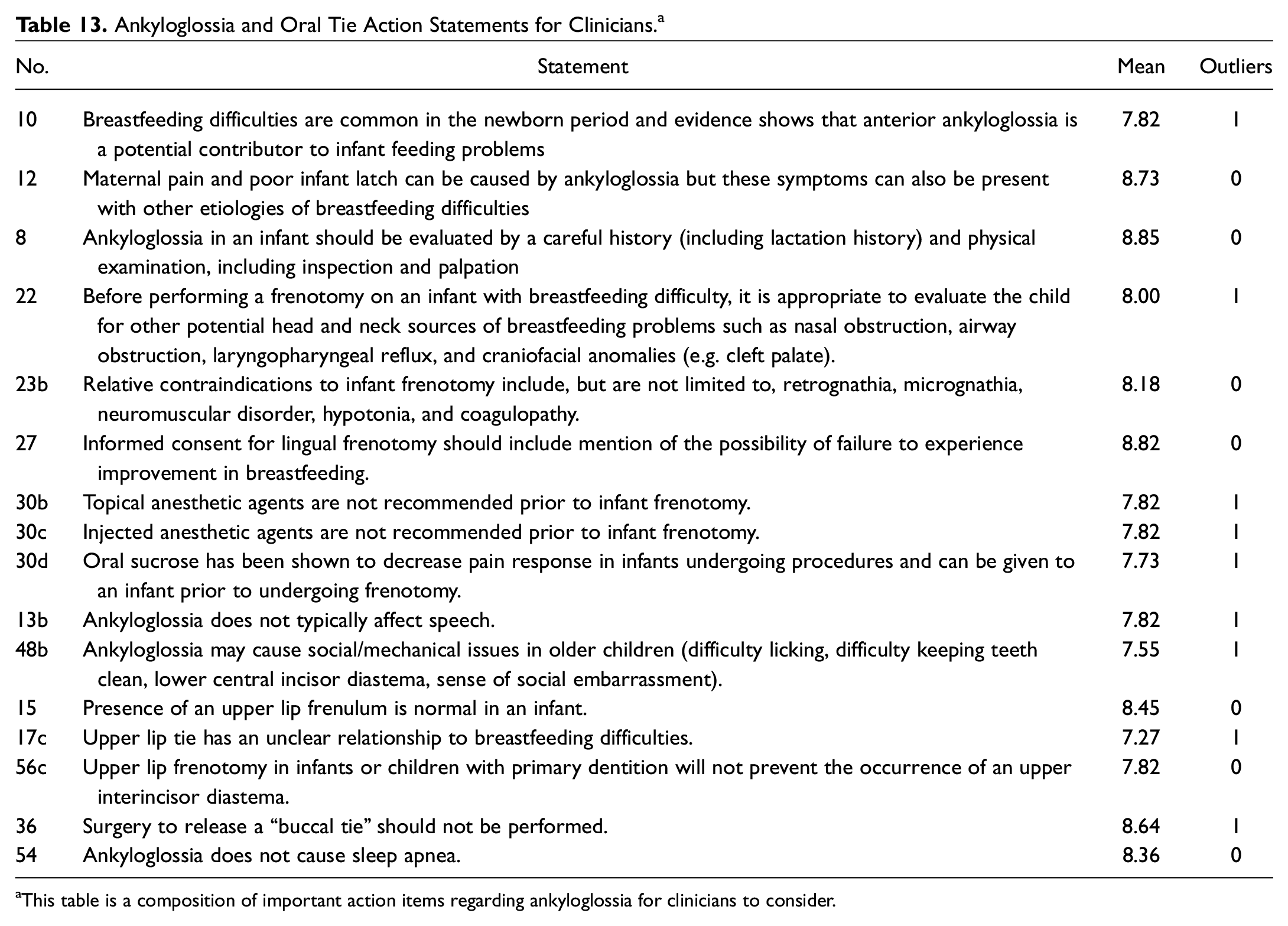
This table is a composition of important action items regarding ankyloglossia for clinicians to consider.
Discussion
Ankyloglossia (General)
As there is increasing awareness, diagnosis, and treatment of ankyloglossia globally, there is a need for common definitions.3,4,6,13-16 With regard to defining ankyloglossia, this panel mirrors the disagreements and uncertainty of the medical community. The panel achieved clear consensus in describing ankyloglossia as a “condition of limited tongue mobility caused by a restrictive lingual frenulum” ( Table 1 ). The panel also acknowledged that, in recent years, practitioners have been using the terms “anterior” and “posterior” ankyloglossia and that those practitioners who use the term “anterior” ankyloglossia are referring to a lingual frenulum that extends to the tip of the tongue or near the tip of the tongue and restricts tongue mobility ( Figure 1A ). But some panelists do not use this term and equate “ankyloglossia” with “anterior ankyloglossia.” When the definition of posterior ankyloglossia was considered, the panel was unable to achieve consensus.17-22 Some in the group use the term to mean a frenulum that inserts into the posterior portion of the tongue, whereas others think of it as a submucosal tethering of the tongue ( Figure 1B ). Still others feel that it does not exist as an anatomic entity and that the term “posterior ankyloglossia” should be abandoned.17-24 Figure 1 shows an example of anterior versus possible posterior ankyloglossia.
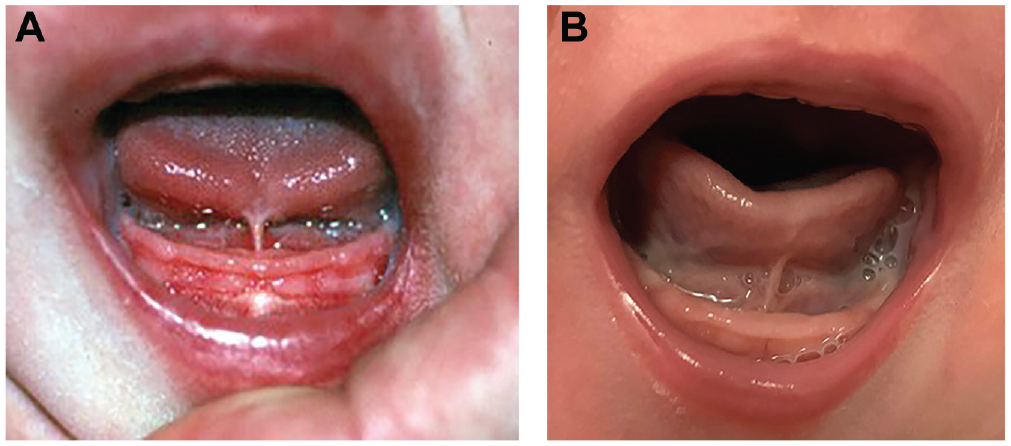
(A) An example of “anterior” ankyloglossia with the lingual frenulum attaching at the tongue tip, limiting tongue mobility. (B) Posterior attachment of lingual frenulum. Consensus was not reached regarding the definition of “posterior” ankyloglossia. Some in the consensus group would describe this figure as an example of posterior ankyloglossia if there are objective findings of restricted tongue mobility caused by the lingual frenulum.
As a result of definition disagreement and the lack of validated grading tools, the group was unable to recommend a preferred ankyloglossia grading system. Some grading systems, such as the Coryllos classification, focus on the type of frenulum but do not address functionality or criteria for ankyloglossia. Other systems, such as the Hazelbacker Assessment Tool for Lingual Frenulum Function or Bristol Tongue Assessment Tool, attempt to include functionality and ankyloglossia scoring.22,24-28 The panel’s consensus regarding ankyloglossia as a “condition of limited tongue mobility caused by a restrictive lingual frenulum” emphasizes the importance of demonstrating tongue mobility restriction and isolating that restriction to the lingual frenulum. Therefore, a diagnosis of ankyloglossia without limited tongue mobility and/or without a restrictive lingual frenulum should be reconsidered.
The reported incidence of ankyloglossia ranges from 2.8% to 10.7%,29,30 with a noted increase in recent years due in part to a widening definition of ankyloglossia. Traditionally, the terms “ankyloglossia” and “tongue-tie” referred to a frenulum that extended close or to the tongue tip, limiting movement of the tongue. Over the last decade—with the more expansive description of tongue-tie including anterior and posterior tongue-tie and with a broader range of attributed symptoms, as well as a lack of standardized diagnostic criteria—many more children are being diagnosed with ankyloglossia.3-5,14,31 The panel reached consensus that, in some communities, infants and children are being overdiagnosed with ankyloglossia and having unnecessary surgery ( Table 1 ). Additional potential factors that have led to more children being diagnosed with ankyloglossia include (1) an increased focus on the benefits of breastfeeding; (2) an increased awareness that ankyloglossia can negatively affect breastfeeding; (3) an increase in the number of lactation consultants who identify infants with possible ankyloglossia; (4) an increase in social media and websites related to tongue-tie, and (5) an increase in the number of medical practitioners, particularly dentists, who treat ankyloglossia.3-5
Buccal Tie
The term “buccal tie” has been used to describe a perceived tightness in the maxillary and/or mandibular buccal frenula. The buccal frena are small connective tissue folds between the buccal mucosa and the maxillary or mandibular gingiva typically located between the canines and premolars. They correspond to the lateral border of the lower portion of the incisivus labii superioris fibers of the orbicularis oris muscle or the anterior border of the buccinator muscle. 32 As such, the buccal frenulum augments the role of the buccinator in keeping the bolus between the teeth and in a medial position during the oral preparatory phase of swallowing. The importance of this function is underscored by evidence that manual cheek support enhances suction during breastfeeding. 33 Therefore, it is illogical that division or resection of the buccal frenulum would be useful in facilitating breastfeeding in infants. Furthermore, there are no existing criteria used to determine whether the buccal frenulum is restrictive. The panel reached a consensus recommendation against release of buccal frenula ( Table 2 ).
Ankyloglossia and Sleep Apnea
The notion that a short lingual frenulum may result in orofacial changes associated with obstructive sleep apnea (OSA) is being advocated by some in health care, particularly dentists. The presumption is that a short frenulum tethers the tongue to the floor of mouth, resulting in a narrow palatal arch and abnormal maxillary growth. While a narrow palatal arch has been shown to contribute to OSA,34,35 only a single small retrospective study has been cited as evidence of a direct association between ankyloglossia and OSA. 36 It should also be noted that anterior tethering of the tongue serves, to some degree, to prevent posterior collapse of the tongue and that if the frenulum is released, it could lead to worsening OSA.37,38 The panel reached consensus that there is no evidence that ankyloglossia causes sleep apnea ( Table 2 ).
Ankyloglossia and Breastfeeding
There was strong consensus among members of the panel that the maternal and infant breastfeeding dyad should be recognized as a vulnerable patient population and that care should be taken to ensure adequate support services, education and counseling, and shared decision making ( Table 3 ). This statement has implications in treatment choices, timing, obtaining consent, and outcome expectations, particularly in the current setting of poorly defined indications and diagnostic criteria.
Clarifying indications and diagnostic criteria is essential for limiting overtreatment while ensuring that infants who would benefit from frenotomy are treated in a timely manner. In addition, the long-term effects on breastfeeding rates for infants who undergo frenotomy are not clear. In the province of Canterbury, New Zealand, the introduction of a standardized clinical pathway for infants with ankyloglossia aimed at supporting breastfeeding and avoiding unnecessary surgery resulted in a marked decrease in the frenotomy rate (11.3% in 2015 to 3.5% in 2017), without negatively affecting the rate of breastfeeding. 5 More recently, a study conducted in Boston demonstrated similar dramatic reductions in frenotomy rates. 39
Ankyloglossia is one of several factors that can contribute to breastfeeding problems. The panel reached consensus that pain and poor latch can be caused by ankyloglossia, but these symptoms can be present with other etiologies.40,41 As tongue-tie can be identified on a simple oral examination, it is often targeted by providers and/or parents as the primary causative factor for breastfeeding difficulties. Thus, the panel also found consensus that before a frenotomy is performed on an infant with breastfeeding difficulty, it is appropriate to evaluate the child for other potential head and neck sources of breastfeeding problems ( Table 3 ). It is also clear that not all infants with ankyloglossia have breastfeeding problems. 42 Ankyloglossia does not by itself indicate that surgical release must be performed, because many infants can still adequately feed without any surgical intervention.39,43 The evaluating provider should fully assess the clinical situation to include the degree of maternal/infant breastfeeding impairment and the physical examination and then devise a management plan that incorporates all of this information as well as the desires and preferences of the family (shared decision-making). As shown by the control groups in the available randomized clinical trials, many infants with varying degrees of ankyloglossia feed well despite no surgical intervention.44-46
For those infants with breastfeeding challenges, the most commonly associated symptoms of ankyloglossia in the newborn include nipple pain with nursing, irritation of the nipple skin, and shallow/poor latch.29,30,47,48 The evaluation of an infant referred for ankyloglossia should not be limited to a cursory assessment of only the lingual frenulum. It is important to obtain the lactation history, including previous breastfeeding experience (experienced mothers will often state that the latch feels different with the tongue-tied baby), the frequency and length of breastfeeding sessions, whether formula supplementation or pumping is being used, and whether lactation support has been utilized. 21 Maternal factors that should be considered include common discomfort during the first few weeks of breastfeeding, maternal nipple anatomy, poor positioning/support at breast, maternal milk supply, and breast infection. 41 Infant factors that should be considered include prematurity, abnormal palatal, mandibular or maxillary development, neurologic disorders, cardiovascular disorders, and upper airway obstruction leading to difficulty feeding. The physical examination should include a close inspection of the tongue, mandible, maxilla, and palate, as well as assessment for signs of airway obstruction. Providers should also palpate the frenulum. While otolaryngologists have expertise in the anatomy and function of the head and neck, the majority of otolaryngologists have a cursory knowledge of breastfeeding methods and problems. Given that 70% to 90% of mother-infant dyads who are experiencing difficulty with breastfeeding have been found to have suboptimal positioning at the breast,40,41 excellent lactation services are essential for successful breastfeeding.
Lactation consultants may not always be able to diagnose ankyloglossia, but they should be able to (1) identify those infants who have not had breastfeeding success from normal interventions and may be affected by ankyloglossia or another medical condition and (2) refer the parents to an appropriate provider. All providers should be adept at assessing the individual needs and preferences of the mother-infant dyad and tailor interventions such that a shared plan is developed. After lingual frenotomy, the lactation consultant can support the dyad in ensuring a good latch has been established postprocedure.
Frenotomy Indications and Informed Consent
The panel reached consensus that before a frenotomy is performed on an infant with breastfeeding difficulty, it is appropriate to evaluate the child for other potential head and neck sources of breastfeeding problems23,43,49-51 ( Table 4 ). Even in the context of ankyloglossia, the following situations can certainly contribute to neonatal difficulty at breastfeeding: nasal obstruction (eg, choanal atresia, piriform aperture stenosis), airway obstruction (eg, laryngomalacia, bilateral vocal fold paralysis), laryngopharyngeal reflux, and craniofacial abnormalities (eg, retrognathia, cleft palate). Failure to diagnose and treat these other disorders can cause increased patient morbidity and worse outcomes after lingual frenotomy.
The panel agreed that relative contraindications to infant frenotomy include, but are not limited to, retrognathia, micrognathia, neuromuscular disorder, hypotonia, and coagulopathy ( Table 4 ). In patients with retrognathia, micrognathia, neuromuscular disorders, and hypotonia, performing a lingual frenotomy can worsen glossoptosis and lead to airway obstruction and concomitant dysphagia.37,38 Furthermore, in patients with neuromuscular disorders and hypotonia, the feeding difficulty may be multifactorial and related to these underlying issues, increasing the chance that the lingual frenotomy will not be successful and improve feeding.
If an infant has been diagnosed with ankyloglossia and there are breastfeeding problems—particularly maternal pain associated with the latch, which is not improving with conservative management (eg, positioning, nipple shields)—then a lingual frenotomy should be performed as soon as possible to decrease the likelihood that the mother will abandon breastfeeding. 52 Once a mother has stopped breastfeeding, she will rarely restart, even if she has maintained her milk supply with pumping. The consensus group could not agree on a specific patient age where infant frenotomy would be most helpful but generally agreed with published studies advocating for early frenotomy, including infants who are <1 month of age52-54 ( Table 10 ).
The panel reached consensus on the statement that rare complications of lingual frenotomy include hemorrhage, airway obstruction, injury to salivary structures, oral aversion, and scarring ( Table 4 ). Although they are rare, all of these complications have been reported in the literature, and many have been seen by the panelists.37,43,55-58
The panel agreed that informed consent for lingual frenotomy should include mention of the possibility of failure to experience improvement in breastfeeding ( Table 4 ). While much evidence in the literature supports the idea that lingual frenotomy can lead to improvement in breastfeeding,43,44,46,50,51,54,59-72 it is also important to recognize that not all infant-mother dyads experience breastfeeding improvement after the procedure.5,45,51,62
The panel also reached consensus that patients and caregivers of patients with ankyloglossia should be counseled about nonsurgical options, including observation, lactation consultation, and/or speech-language pathology consultation ( Table 4 ). It is important for caregivers to understand that there are treatment options and not all patients with ankyloglossia must undergo a lingual frenotomy. Breastfeeding difficulty can often improve with time or nonsurgical intervention by a lactation consultant or speech pathologist who specializes in breastfeeding issues.49,73
The panel members all noted a recent significant clinical increase in referrals and parent requests for lingual frenotomy to prevent future feeding or speech disorders. Several studies support the panel’s consensus that in infants with little or no tongue mobility restriction, frenotomy does not prevent future feeding or speech disorders.8,74-76
Frenotomy Procedure
The panel reached strong consensus that lingual frenotomy is generally a safe and well-tolerated procedure ( Table 5 ). This statement is well supported by the literature.7,19,77-79
The panel agreed that there is insufficient evidence to support a specific technique ( Table 5 ). The panel was aware that some providers are routinely using lasers as their tool of choice for frenotomy, but the panel felt that there was insufficient and conflicting evidence to support its use as being superior to other techniques.80-82 This is critical in that different techniques may have cost implications for the patients. Additionally, terms such as “frenotomy,”“frenuloplasty,” and “frenectomy” have often been inappropriately used interchangeably. Frenotomy, or frenulotomy, is the usual procedure performed in infants: a simple incision of the lingual frenulum. The term “frenuloplasty” refers to an incision of the lingual frenulum with a rearrangement of the tissue (eg, horizontal to vertical, z-plasty). “Frenectomy” is the term used to describe removal of the lingual frenulum. This term has also been used with regard to the upper frenulum, where tissue is removed from the midline of the maxilla. They are distinct techniques that also have billing code implications. The studies available for specific techniques were of low quality with high risk of bias.
The panel reached consensus that there is no evidence to support a standard postprocedure care regimen, including massage or stretching ( Table 5 ). There are few data regarding ankyloglossia recurrence, the frequency of postprocedure oral aversion, and outcomes for frenotomy as a whole, so the panel was unable to support a statement that a postoperative regimen was beneficial.
Several factors influenced the panel in not reaching consensus on the utility of frenotomy for posterior ankyloglossia ( Table 10 ). The panel was unable to reach consensus on a definition of posterior ankyloglossia, highlighting the controversy in the diagnostic criteria and its existence as a clinical entity ( Table 1 ). Additionally, there is little evidence to demonstrate the efficacy of frenotomy in these patients, as the few studies available have a high risk of bias.19,23,49,50
The panel did not support a preferred location in which to perform a frenotomy (clinic or operating room depending on age or patient/provider preference; Table 10 ). Many studies have found in-office frenotomy without general anesthesia to be a safe and effective treatment for infants with ankyloglossia.19,29,44-46,59,61,78,79 While it was generally acknowledged that older children would likely need general anesthesia, the consensus group could not agree on the exact circumstances that would lead to a recommendation for the procedures to be performed in the operating room as opposed to the clinic. In general, it is best to avoid general anesthesia in an infant if possible. 79
The panel reached consensus that topical anesthetic agents are not recommended prior to infant frenotomy ( Table 5 ). Two small randomized studies found no advantage to the application of topical anesthetics.83,84 One safety concern is that topical benzocaine increases the risk of methemoglobinemia. In 2018, the Food and Drug Administration issued a warning that oral drug products containing benzocaine should not be used to treat infants and children <2 years old. 85 Injecting local anesthetic agents is not recommended prior to infant lingual frenotomy when performed in the office.
The panel reached consensus that oral sucrose has been shown to decrease pain response in infants undergoing procedures and can be given to an infant prior to undergoing frenotomy ( Table 5 ). Sucrose is used commonly for other painful procedures during infancy, but its efficacy is debated, with some studies showing equal effectiveness with massage or breast milk. 86 Sucrose is unlikely to work in children >1 year of age, 87 and a minimally effective dose is not known. 88 Similarly, optimal timing before procedure is not known, 89 though 1 study suggests 2 minutes. 90
Ankyloglossia in Older Children
Much of the published literature regarding ankyloglossia has focused on infants; there is a paucity of literature regarding the indications and outcomes for frenuloplasty in older children and adolescents. 8 While breastfeeding difficulty is often the primary concern in infants with ankyloglossia, older children with ankyloglossia may present with concerns regarding speech, dentition, mechanical limitations, and social implications.
The consensus group concluded that ankyloglossia does not typically affect speech 91 ( Table 6 ). Even sounds that require the greatest amount of tongue elevation, /l/ and /r/, and protrusion, /th/, can usually be produced in the presence of significant tongue tip restriction. A few studies suggested an association between ankyloglossia and articulation difficulties, but they were of low quality.76,92,93 Studies on the impact of frenuloplasty on speech problems have also yielded conflicting results.74,76,92-95 Overall, studies evaluating speech outcomes in patients with ankyloglossia have suffered from the lack of control groups, randomization, and blinding; small sample sizes; and the use of nonvalidated subjective assessments. Another major limitation in many of the studies involves failure to adequately describe and standardize the utilization of speech therapy in subjects.8,96,97 As the true incidence of speech difficulties is unknown and there is no method to predict which children with ankyloglossia will require treatment, the consensus group agreed that consultation with a speech pathologist is encouraged prior to frenotomy/frenuloplasty for speech concerns.
The panel agreed that ankyloglossia may cause social/mechanical issues in older children (difficulty licking, difficulty keeping teeth clean, lower central incisor diastema, sense of social embarrassment; Table 6 ). There have been a few smaller studies but no randomized trials in children to determine whether frenuloplasty leads to definitive improvement in these types of mechanical and social issues.93,95,98 On the basis of our experience and the available literature, the panel concluded that some older children will have improved quality of life after frenotomy/frenuloplasty. There is no maximum age by which this procedure should be performed.
Data supporting the superiority of a specific frenuloplasty technique are lacking. As such, the panel agreed that there is not a preferred procedure for the correction of ankyloglossia in an older child ( Table 6 ). There have been no randomized studies to compare outcomes between cold techniques and laser for frenuloplasty. 99 A small randomized study 92 compared outcomes for 4-flap z-frenuloplasty and traditional horizontal-to-vertical frenuloplasty in children with ankyloglossia. While both procedures resulted in improvements in articulation and fluency, the 4-flap z-frenuloplasty group had improved articulation and superior tongue protrusion scores.
Maxillary Labial Frenulum
The MLF attaches the central portion of the upper lip to the maxillary alveolus between the central maxillary incisors. It consists of squamous epithelium; loose connective tissue; dense, irregular, collagenous connective tissue; and, in some cases, muscle fibers from the incisivus labii superioris portion of the orbicularis oris muscle.32,100,101 The MLF serves to provide stability for the upper lip.
Many cross-sectional studies demonstrated that the MLF is almost universally present as a normal, albeit variable, structure. 102 It is this variability that has led some clinicians to postulate that certain MLF presentations may be associated with either feeding difficulties in the newborn or later development of diastema. Unfortunately, investigators have yet to determine which, if any, classification schemes and presentations correlate with clinical symptoms, 103 and those in common use appear to demonstrate poor intra- and interrater reliability. 104
Regarding feeding issues, while several studies purport to establish the effectiveness of the MLF release for infant feeding difficulties,23,50,105 the studies are hampered by unclear definitions of lip tie, the absence of control groups, small patient cohorts, the presence of confounding variables, and short surgical follow-up. A recent systematic review identified no randomized controlled trials on the subject and concluded that the level of evidence for routine MLF release in infants with breastfeeding difficulties was poor. 103 The Australian Collaboration for Infant Oral Research has challenged the notion that “tie” of the lip even exists and suggested that the term be retired. 100 While several members of our panel concluded that there “is little evidence” to support MLF release when lip tie is suspected, others felt that the available studies and their personal experience suggest that some babies with poor lip eversion during breastfeeding may benefit from the procedure. The panel agreed that, in some communities, lip tie is being overdiagnosed ( Table 7 ).
The literature is replete with studies of the association between MLF presentation and interincisor diastema. 106 Despite this fact, no definitive relationship between the two has been established. 106 In addition, studies suggest that despite short-term improvement in diastema obtained through MLF release, controls improve equally with age, presumably due to eruption of the canine teeth.102,106 Additionally, some authors have postulated that scarring resulting from MLF release in childhood may actually make diastema more likely in the permanent dentition. 100 The panel, like the Australian Collaboration for Infant Oral Research, therefore reached consensus that MLF release is not indicated for prevention of diastema in the permanent dentition ( Table 7 ).
Strengths and Limitations
The strength of this study is the methodology of the consensus statement process. It is rigorous and follows an explicit, tested protocol to minimize conflicts of interest, minimize bias, and ensure consistency. Limitations of the study include the relatively small group of experts, all of whom are practicing pediatric otolaryngologists, and the lack of input from other professionals who evaluate children with ankyloglossia, including lactation consultants, pediatricians, and speech-language practitioners. In addition, there is a lack of CEBM level 1 studies to inform the panelists’ opinions, and the majority of studies available have high levels of bias. Additional high-quality studies regarding ankyloglossia and other oral tie diagnosis and treatment are needed to further inform the practice of otolaryngologists and relevant medical specialists in the future.
Conclusions
This CCS was developed by pediatric otolaryngologists with the intention to promote appropriate, evidence-based care of the infant and child with possible ankyloglossia and/or upper lip tie. A series of clinical statements were developed by an expert panel using an objective survey method. While members of the consensus group all evaluate and treat children with ankyloglossia, the group found some marked differences in opinion regarding controversial topics, such as the definition (and even the existence) of posterior ankyloglossia and lip tie. While the group was able to come to consensus that frenotomy in infants with ankyloglossia can lead to an improvement in breastfeeding, not all infants with ankyloglossia need to have a frenotomy, and there are other more common causes of breastfeeding difficulties. A frenulum procedure is also an option in older children with speech articulation and/or other mechanical social issues, but the evidence is limited and of relatively poor quality. Similarly, the level of evidence surrounding intervention for the maxillary frenulum and possible upper lip tie is poor. Further study is needed to refine patient selection and outcome assessments in these areas. The application of these statements is expected to result in an improved understanding of the controversies surrounding ankyloglossia in children and lead to more family-centered care.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We gratefully acknowledge the support of Sarah Towner Wright, MLS, for conducting the literature searches.
The following organizations have endorsed this clinical consensus statement: American Society of Pediatric Otolaryngology (ASPO), Society of Ear, Nose, and Throat Advances in Children (SENTAC), and Triological Society.