
Abstract
Objective
The location and size of the frontal sinus ostium are critical in determining surgical difficulty. The more anterior the ostium, the more difficult is the surgical access. We propose a novel computed tomography (CT) grading specific to the anatomical position of the frontal ostium.
Study Design
Observational study followed by a prospective part.
Settings
Tertiary rhinology practice
Subject and Methods
On a specified sagittal CT cut, a vertical line was drawn through the posterior edge of the frontal process of the maxilla (frontal buttress/beak) along its vertical axis (reference [R-] line). A second (S-) line was placed at the point of upturn of the skull base. Based on if the S-line was posterior or anterior to the R-line, the frontal ostium was graded positive and more easily accessible or negative and thereby more challenging, respectively. If both lines overlapped, then a neutral (0) grading existed.
Results
A total of 297 CTs (594 ostia) were analyzed. In total, 394 (65%) ostia were grade positive, 52 (8.75%) were grade negative, and 103 (17.3%) were grade neutral. Ninety frontal sinusotomies were then performed using this grading system: 48 were positive, 21 negative, and 21 neutral. The average time to complete a frontal sinusotomy was 9.96 minutes for grade positive compared to 11.4 minutes for neutral and 16.05 minutes for grade negative (P < .005).
Conclusion
This novel anatomical CT grading system is designed to be useful in planning and predicting the level of difficulty in endoscopic frontal sinus surgery.
Keywords
Endoscopic frontal sinus surgery is much more challenging than endoscopic surgery on the other paranasal sinuses.1,2 The wide range of anatomical variability within the frontal sinus and frontal recess region, regardless of the frontal cells that might occupy this space, are some of the important reasons behind this potentially challenging endoscopic surgical region. 3 Differing location, diameter, and position of the internal frontal ostium encompass the variability found in this region.
Increasing levels of difficulty translate into longer operating times and therefore a greater cost to the surgery. The more difficult frontal recess anatomy will demand the expertise of surgeons with superior skills, training, and angled instrumentation to achieve a successful outcome with minimal risk of orbital and intracranial complications. 4
The location and size of the internal frontal sinus ostium (the narrowest part of the frontal sinus outflow drainage pathway) are crucial in determining the level of difficulty that the operating surgeon will face during dissection and clearance of the frontal recess. The location and diameter of the frontal ostium are directly related to the position of the nasal process of the frontal bone anteriorly (also known as spina nasalis interna, frontal buttress or frontal beak) and the point of upturn (deflection point) of the anterior skull base.
The frontal process of the maxilla at the level of the lateral aspect of the lacrimal bone (medial lacrimal sac) just inferior to the frontal ostium is a constant landmark that forms part of the lateral frontal sinus outflow drainage pathway below the ostium. We hypothesize that creation of a preoperative computed tomography (CT) grading system using this anatomical axis on a sagittal CT cut as a reference will have great value in predicting endoscopic surgical difficulty level. It will form the basis for this anatomical CT surgical grading system.
The smaller the frontal sinus ostium diameter and the more anterior its location in relation to the frontal process of maxilla, the more difficult will be its surgical access, correlating with an increase in surgical time to clear the frontal recess drainage pathway.
Many factors contribute to anatomical variability of the frontal recess. These include presence and degree of pneumatization of various previously described anterior ethmoid cells as well as anatomical variations of the middle turbinate, uncinate, and nasal septum. However, the actual physical placement of the frontal sinus ostium in relation to the frontal process of the maxilla will always play a critical and independent part in the surgical difficulty level faced during endoscopic dissection of the frontal recess.
We therefore propose a new CT grading system for the frontal sinus that is specific to the anatomical position of the frontal sinus ostium on a specified sagittal plane. This frontal ostium grading (FOG) system is independent from all other variables relating to pneumatization patterns of the anterior ethmoid and frontal cells.5,6 The previously described frontal cells and their associated anatomical classification, when present, can affect surgical access to the frontal sinus but in more of an obstructive manner rather than affecting access.5,6 This new FOG system is proposed to be an additional tool to predict surgical difficulty. It is not meant to detract from the importance of other obstructive anatomical variations within the frontal recess that have been previously described.1,5,6
Objective
The objective of this study is to create and validate a novel FOG system based on preoperative CT imaging studies. The FOG system will allow for another layer of presurgical planning in preparation for frontal sinus surgery.
This new grading system is meant to be simple to use and effective in function. It is based simply on marking two vertical lines parallel to each other on a sagittal preoperative CT cut at the level of frontal sinus ostium. The ideal CT cut in the sagittal plane is almost always identified as the cut that transects the most medial aspect of the lacrimal sac. Using this sagittal slice, the first line, called the reference or R-line, is standardized and drawn along the vertical axis of the frontal process at the level of the maxilla/lacrimal bone; this relates to the most posterior projection of the frontal beak/buttress. The second line (S-line) is variable in position, depending on the patient, and is drawn at the point of upturn (deflection point) of the anterior skull base at the level of the frontal sinus ostium. It is drawn parallel to the R-line ( Figure 1 ).
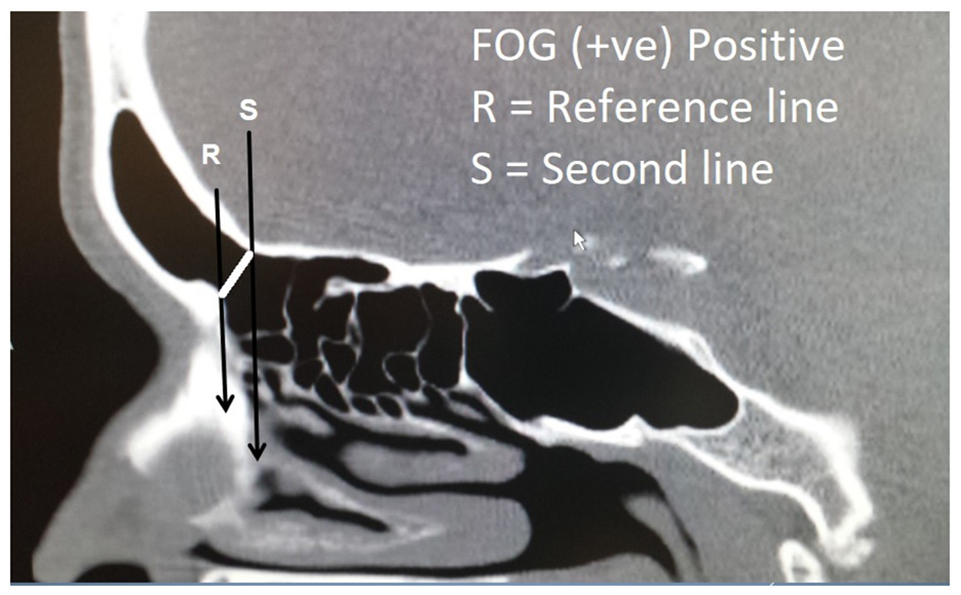
Frontal ostium grading (FOG) (positive) where the reference line (R) lies anterior to second (S) line.
If the R-line is anterior to the S-line, we term this frontal sinus grade as “positive” frontal ostium grade (FOG positive). A FOG positive grade is predicted to be a surgically easier dissection that should take a shorter time than a FOG negative grade ( Figure 1 ).
If the S-line and R-line overlap, then we classify such a frontal sinus as a FOG neutral (0) grade, predicted to be surgically more difficult than a FOG positive grade ( Figure 2 ).

Frontal ostium grading (FOG) (0) where the reference line (R) overlaps with the second (S) line.
If the R-line is posterior to the S-line, we would classify this as having a negative frontal ostium grade (FOG negative). A FOG negative grade is predicted to be surgically the most difficult FOG grade and will likely require a more experienced endoscopic surgeon with proper angled instrumentation for a successful outcome. The FOG negative ostium will predictably require the longest surgical time ( Figure 3 ).
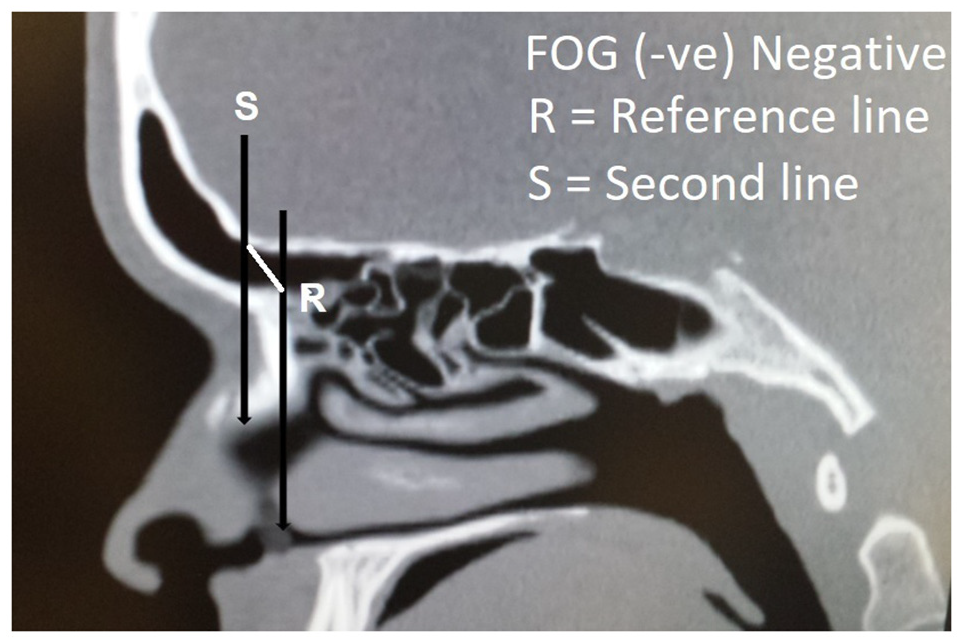
Frontal ostium grading (FOG) (negative) where the reference line (R) lies posterior to the second (S) line.
Subjects and Methods
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (University of British Columbia–Providence Health Research Ethics Board H16-02317) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
The first part of the study was an observational CT-based anatomical study. Preoperative CT sinus scans of all patients who underwent sinonasal surgery over a 3-year period were examined for appropriateness of inclusion into the study. Patients were included if they were booked for sinus surgery for benign condition with no previous evidence of frontal sinus surgery. Image-guided CT scans were obtained with axial cuts of 1.0 mm or less in thickness with sagittal and axial reformats, a standard for image guidance protocol at our center.
The FOG for each side was determined as explained above. We noticed that the best sagittal slice for this assessment is the sagittal plane that first transects the ipsilateral lacrimal sac. Using this sagittal CT cut, the first vertical line (reference or R-line) is drawn through the frontal process of the maxilla along its vertical axis. The correct position for placement of the R-line on the sagittal plane is the most prominent projection of the frontal beak (anterior buttress) on the same plane as the level of maxillary process of frontal bone, which also represents the most inferior point of the frontal ostium. The second or S-line is placed at the point of upturn (deflection point) of the anterior skull base, which is variable between sides, and can be found posterosuperior, superior, or anterosuperior to the (anterior buttress) frontal beak depending on the slope of the anterior skull base. The S-line is a vertical line drawn parallel to the R-line and represents the superior margin of the frontal sinus ostium. It is drawn at the point of upturn (or deflection) of the anterior skull base where it proceeds to become the posterior table of the frontal sinus. As noted, the frontal sinus ostium by definition, as described by Stammberger et al, 6 is the narrowest part of the frontal sinus drainage pathway. Therefore, a line drawn between where the R-line intersects the frontal beak and where the S-line intersects the skull base would by definition be the frontal ostium, or the narrowest part of the frontal sinus drainage pathway. The length of this third line would then become the frontal ostium diameter (FOD).
The FOD is another important factor that comes into play during dissection of the frontal recess. A larger diameter makes for easier surgical access to the frontal sinus and vice versa.
Measuring the FOD in millimeters is easily obtained from the same sagittal CT scan cut using the digital measuring tool that comes with CT software application. The FOD measurements, together with the FOG, will be used to create a newly proposed surgical difficulty level score for endoscopic frontal sinus surgery.
We propose 4 categories of frontal sinus surgical difficulty (I-IV) based on the above parameters. Difficulty level I includes patients with positive frontal ostium grades (FOG positive) and large ostium (≥7.5-mm FOD) diameters (greatest ease group), while level IV includes patients with negative frontal ostium grades (FOG negative) and small/narrow (<7.5-mm FOD) diameter (most difficult group) ( Table 1 ). The 7.5-mm value is based on the median FOD value calculated for all frontal sinuses combined (both right and left sides) and obtained from the total 594 CT assessments made in the first part of the study. Interestingly, this 7.5-mm median value was found to be very close to the average FOD of the same cohort (mean = 7.6 mm), indicating that our sample seemed to follow a normal distribution pattern with adequate size and quality ( Table 2 ).
Frontal Sinus Surgery Levels of Difficulty According to FOG and FOD Grade. a
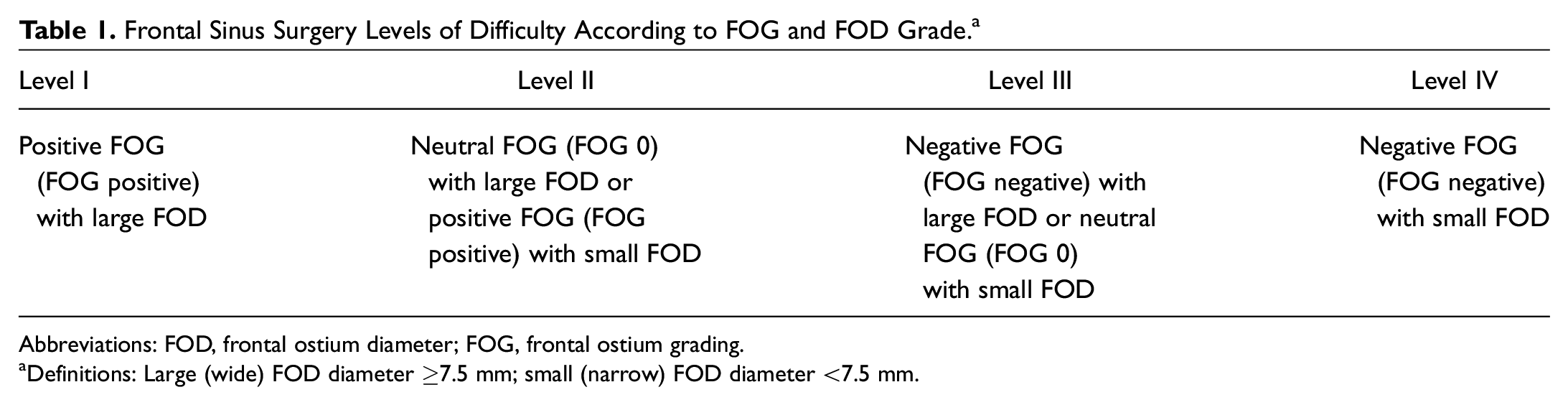
Abbreviations: FOD, frontal ostium diameter; FOG, frontal ostium grading.
Definitions: Large (wide) FOD diameter ≥7.5 mm; small (narrow) FOD diameter <7.5 mm.
Descriptive Summary of Right and Left FOD: Study Part 1.
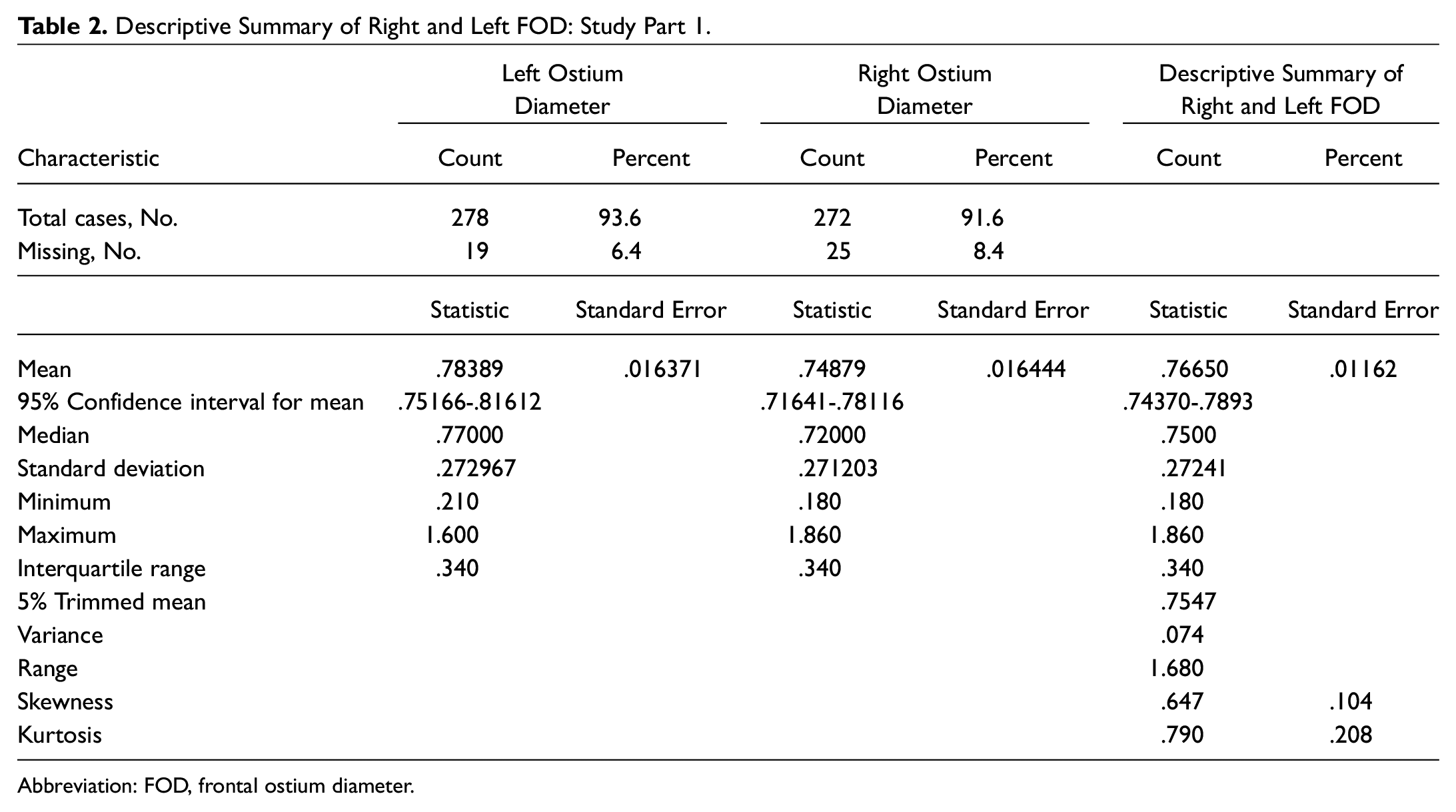
Abbreviation: FOD, frontal ostium diameter.
To further test the validity of this grading system, a prospective and more practical second part was conducted. Using the proposed FOG/FOD criteria and after obtaining ethics approval, 48 patients undergoing primary endoscopic sinus surgery were recruited over a 12-month period. The appropriate data were collected prospectively, including preoperative CT assessment for both FOG and FOD, as well as surgical time to complete the frontal sinusotomy, starting from when the anterior ethmoid artery was visualized until the frontal sinus was widely opened and the dissection completed. Possible confounding variables for quality control of the study included preoperative CT scan assessment for disease severity scoring per side using the Lund-Mackay CT scoring system, presence or absence of frontal recess cells, endoscopic visibility grade using Boezaart scores, mean blood pressure, and heart rate at the time of endoscopic frontal sinusotomy.
Results
For the first part of the study, 297 of 348 patients (85.3%) met the inclusion criteria. Reasons for exclusion were inadequate or unavailable CT imaging (31/297, 8.9%), benign sinonasal tumors (9/297, 2.6%), previous frontal sinus surgery (7/297, 2.0%), sinonasal malignancy (2/297, 0.6%), and frontal sinus mucoceles (2/297, 0.6%). CT scans for a total of 191 (64.3%) male and 106 (35.7%) female patients were found eligible and used for the study.
On the left side, 206 (69.4%) of the frontal ostium grades were positive. Forty (15.2%) were FOG neutral and 27 (9.1%) of ostia were found to be FOG negative. Nineteen patients (6.4%) had a hypoplastic frontal sinus on the left side ( Table 3 ).
Number of Participants with Left and Right FOG in Part 1 of the Study (Computed Tomography Review).
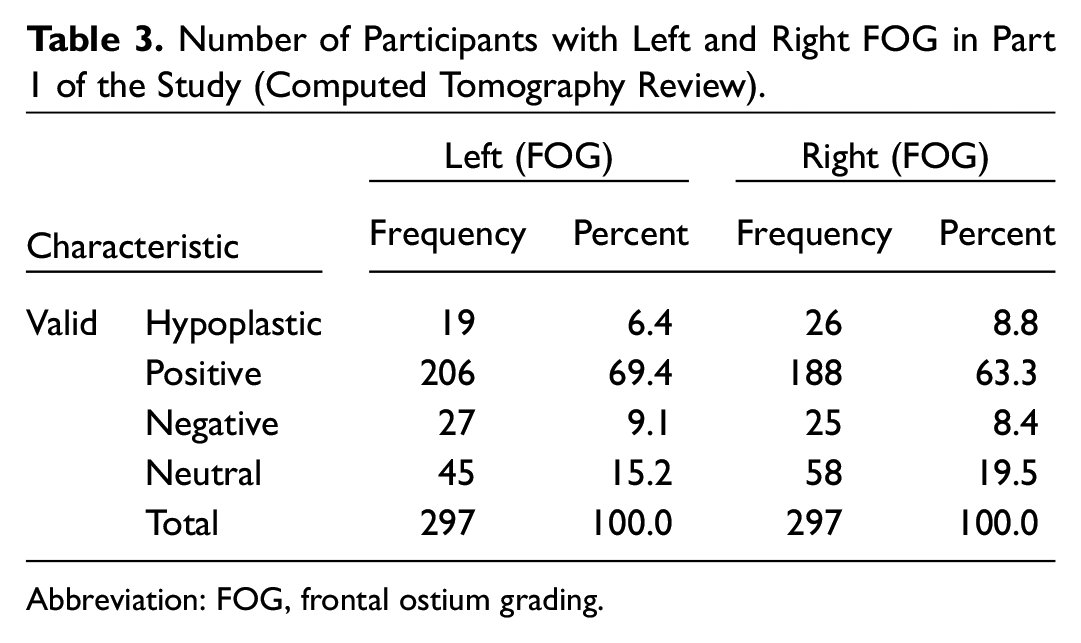
Abbreviation: FOG, frontal ostium grading.
Comparable results were found on the right side: FOG positive, 188 (63.0%); FOG neutral, 58 (19.5%); FOG negative, 25 (8.4%); and hypoplastic, 26 (9.0%) ( Table 3 ).
FOD was also calculated for all frontal sinuses (both right, left, and combined): the mean frontal ostium diameter for all frontal sinuses combined was 7.6 mm, and the median was 7.5 mm ( Table 2 ).
Using a nonparametric independent samples Kruskal-Wallis test, the results for the second part of the study showed that 48 sinusotomies were FOG positive, 21 FOG neutral, and 21 FOG negative. The average time to complete a frontal sinusotomy in both right and left sides combined was 9.96 minutes for the FOG positive ostia compared to 11.4 minutes in FOG neutral ostia and 16.05 minutes for the FOG negative ostia (P < .005) ( Table 4 ).
Comparison of Time of Surgery, Mean Arterial Blood Pressure, and Bleeding Score between Frontal Ostium Grading Positive, Negative, and Neutral for Right and Left Sides.
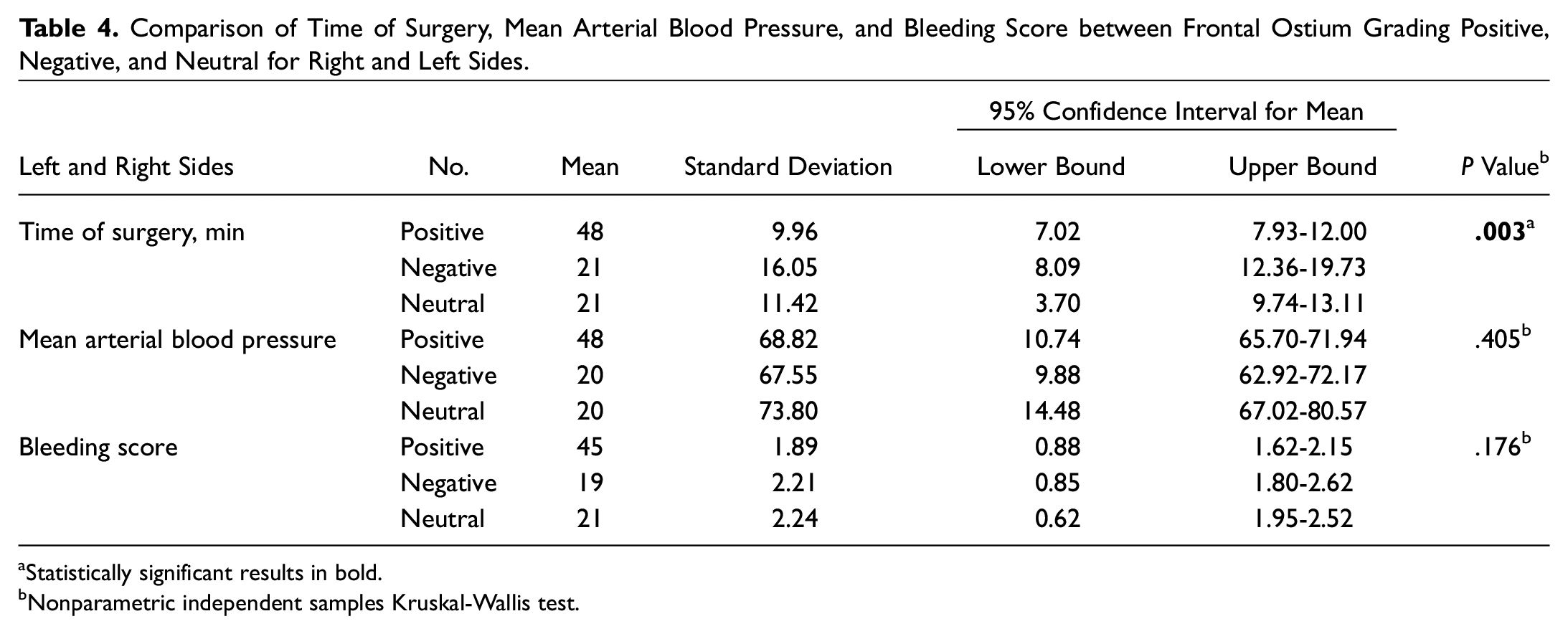
Statistically significant results in bold.
Nonparametric independent samples Kruskal-Wallis test.
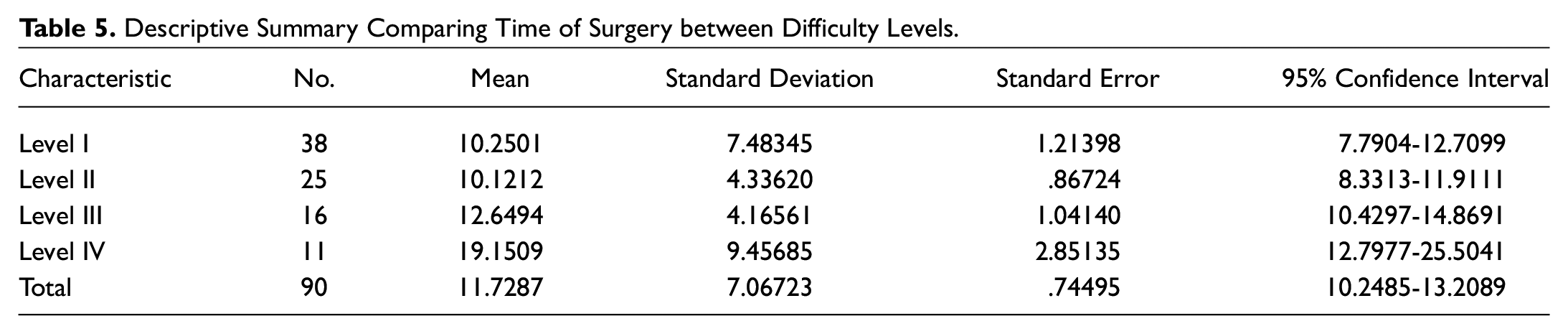
To test the validity of the proposed frontal sinus surgery difficulty level, we first applied an analysis of variance (ANOVA) test on the prospective 90 frontal sinusotomy data sample, which was grouped according to the proposed difficulty levels (level I-IV) based on the FOG and FOD. The ANOVA test results indicated that there was an overall significant difference in operative time between the 4 groups (P < .005) ( Table 5 ). This was then followed with pairwise comparison, testing the significance of surgery difficulty between each other and using frontal sinusotomy surgical time as the determinant measuring factor for surgical difficulty. Pairwise comparison test results showed significance between the means for each group at the .05 level ( Table 6 ).
Descriptive Summary Comparing Time of Surgery between Difficulty Levels.
Pairwise Comparison of Time of Surgery between Difficulty Levels Based on Frontal Ostium Grading and Frontal Ostium Diameter Grade.
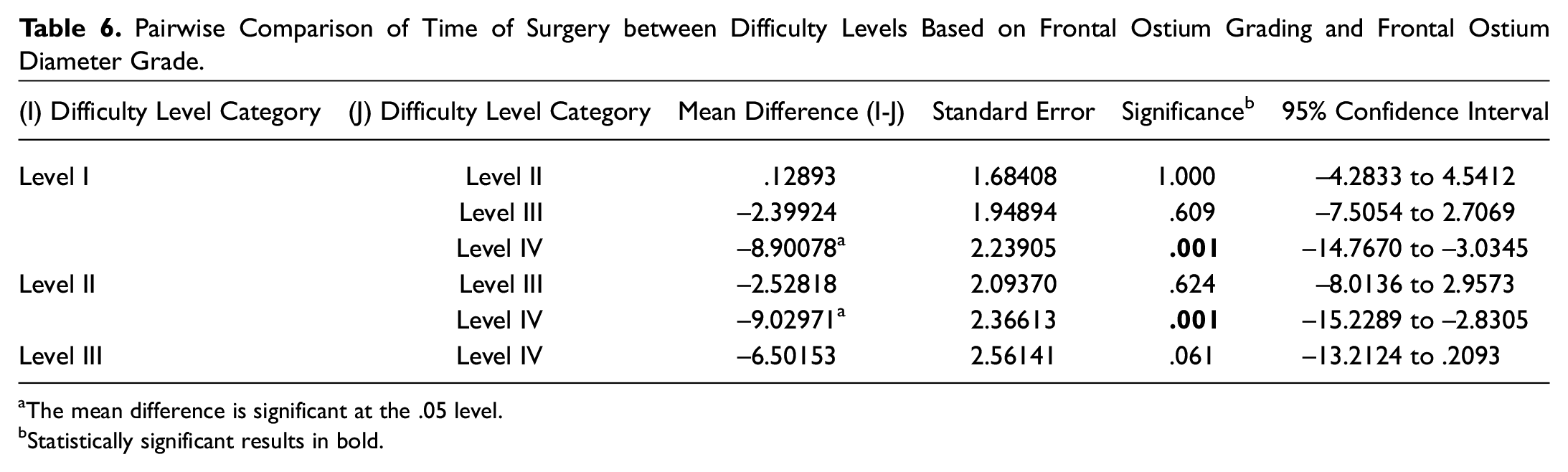
The mean difference is significant at the .05 level.
Statistically significant results in bold.
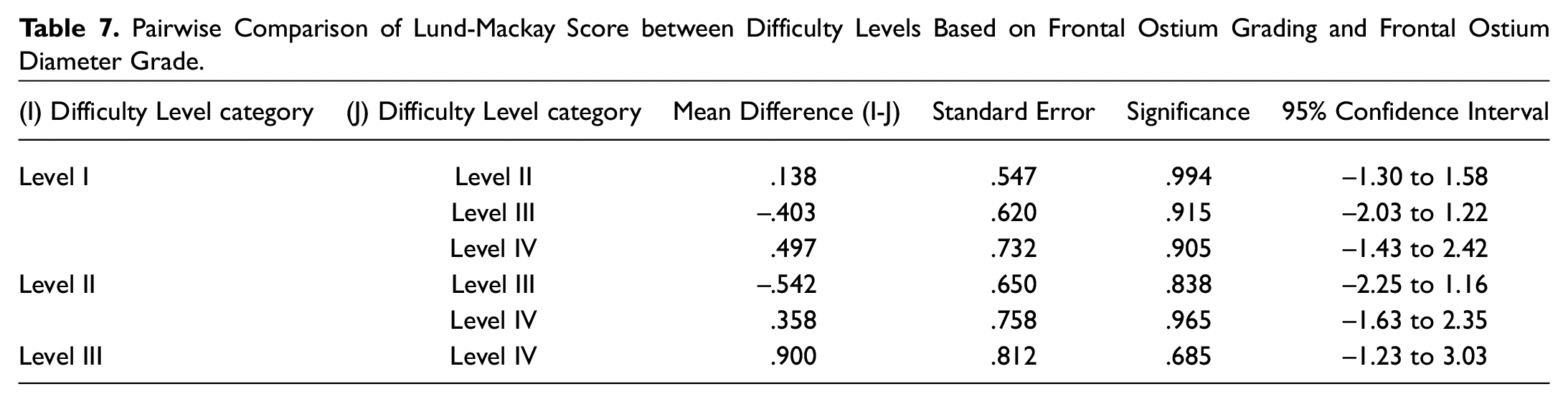
To further assess the quality of our prospective study with regard to confounding variables, a pairwise comparison study comparing Lund-Mackay scores among different FOG groups showed no significant difference in Lund-Mackay scores between FOG difficulty levels categories (P > 6; Table 7 ). To control for any possible effect of the presence or absence of frontal recess cells for the prospective study, a Pearson χ2 test was performed and results showed no significant difference between all the FOG difficulty groups with regard to effect of the presence or absence of frontal recess cells (P = .254).
Pairwise Comparison of Lund-Mackay Score between Difficulty Levels Based on Frontal Ostium Grading and Frontal Ostium Diameter Grade.
Discussion
It is clinically difficult (if not impossible) to define and agree on a dividing value for a FOD that acts as the value that divides between a wide and narrow FOD, as this is has never been described in the literature. For this reason, the median FOD value of 7.5 mm for all measured frontal ostium diameters was used to establish 2 equal distributions of data for analysis. From a statistical perspective, using the median cut-point allowed the data to be equally distributed to minimize bias in the analysis. This 7.5-mm value is proposed as the ideal one to classify patients into the 2 categories of wide and narrow FOD diameters. Interestingly, the FOD median value of 7.5 mm was found to be very close to the mean value of 7.6 mm for the same cohort, indicating a good representative sampling that would follow a normal distribution.
In the second part of a planned prospective study, we were able to correlate the surgical time in each category with its FOG grade and FOD counterpart. As expected, statistical analysis of our results showed that the more anteriorly placed the frontal sinus ostium and the narrower the diameter of the frontal sinus ostium, the longer it took to perform the endoscopic frontal sinusotomy.
Taking both the FOG and FOD into account, we propose 4 levels of surgical difficulty when performing an endoscopic frontal sinus surgery ( Table 1 ):
Difficulty level I: Patients with FOG positive and a wide FOD ostia
Difficulty level II: Patients with FOG positive/FOD narrow or FOG neutral/wide FOD ostia
Difficulty level III: Patients with FOG neutral/FOD narrow or FOG negative and wide FOD ostia
Difficulty level IV: Patients with FOG negative and narrow FOD combination
Hosemann et al 4 described how anatomical variability of the dimension of the spina nasalis interna (nasal process of the frontal bone) can affect endonasal frontal sinus surgery, where a larger anteroposterior spina nasalis makes endonasal frontal sinus surgery more difficult and may require the use of a drill. They highlighted the importance of looking at sagittal CT reformat cuts to assess this region prior to endonasal frontal sinus surgery. Hilger et al 7 reviewed 10 sagittal reconstructed thin CT cuts and described the different variations of the angle between the frontal sinus and the ethmoid infundibulum, which, according to the authors, appeared to depend on the anterior projection of the frontal sinus and give an indication of the optimal endoscopic angle needed for visualization of the frontal ostium. A more angled endoscope would be necessary to visualize the frontal sinus ostium when the “front-nasal-angle” is smaller. We are not aware of any anatomical sagittal CT study specific to grading the position of the frontal sinus ostium, in relation to the maxillary process of the frontal bone, for grading the difficulty of endoscopic frontal sinus surgery. The CT grading system presented here is the first of its kind for grading the frontal ostium based on its location and diameter within the frontal recess, regardless of the numerous obstructive cells that have been previously classified multiple times.
In our opinion, a structured grading system that is able to predict difficulty level in endoscopic frontal sinus surgery can be very useful for planning the surgery. It can ensure that adequate skill, time, and equipment are present and available so that the operation can be performed successfully and with minimal morbidity.
Conclusion
We introduce a novel CT grading system that is independent of the various described cells within the frontal recess. It is expected to help in successfully predicting surgical difficulty level, thereby allowing adequate preoperative preparation, including planning for surgical time, surgical expertise, and equipment preparation. Furthermore, we feel that such a grading system will help reduce surgical complication rates.
Footnotes
Acknowledgements
We thank Rochelle Galleto, Waleed Aboarja, Jennifer Payandeh, and Sara Derikvand for their help in ethics submission, data collection, and manuscript preparation.