
Abstract
We describe the use of the medial sural artery musculocutaneous perforator (MSAP) flap at our institution. It is a relatively new flap, originally described in 2001 for lower extremity defects, that has become increasingly popular for head and neck reconstruction due to its versatility, thinness, pliability, long pedicle, and particularly favorable donor site. It has been described for reconstruction of oral defects, but there is little published on its use in pharyngeal reconstruction. We suggest that the MSAP is an ideal flap for addressing defects caused by pharyngoesophageal stenosis, pharyngeal fistulas, or laryngopharyngectomies. We review 5 cases at our institution from June 2016 to November 2017.
Keywords
The anterolateral thigh flap (ALT) and radial forearm fasciocutaneous flap (RFFF) have been the mainstay options for pharyngoesophageal reconstruction.1,2 However, the RFFF requires sacrifice of a major upper extremity artery and harbors a conspicuous donor site requiring skin grafting, and the ALT may be of limited use in patients with greater thigh adipose tissue, particularly when tubing is required.
Described in 2001 by Hallock 3 and soon after by Cavadas et al, 4 the medial sural artery musculocutaneous perforator (MSAP) is a fasciocutaneous flap based on a perforator deriving from the popliteal artery. The MSAP has proven to deliver thin, pliable tissue with limited donor site morbidity.
Method
We conducted a retrospective review of all MSAP flaps at our institution from July 2016 to November 2017. Five of 21 MSAP flaps were used for pharyngeal reconstruction ( Table 1 ). Follow-up ranged from 2 to 4 months. One MSAP flap was aborted due to inadequate perforator diameter and was therefore excluded. This study was approved by NYU School of Medicine Institutional Review Board.
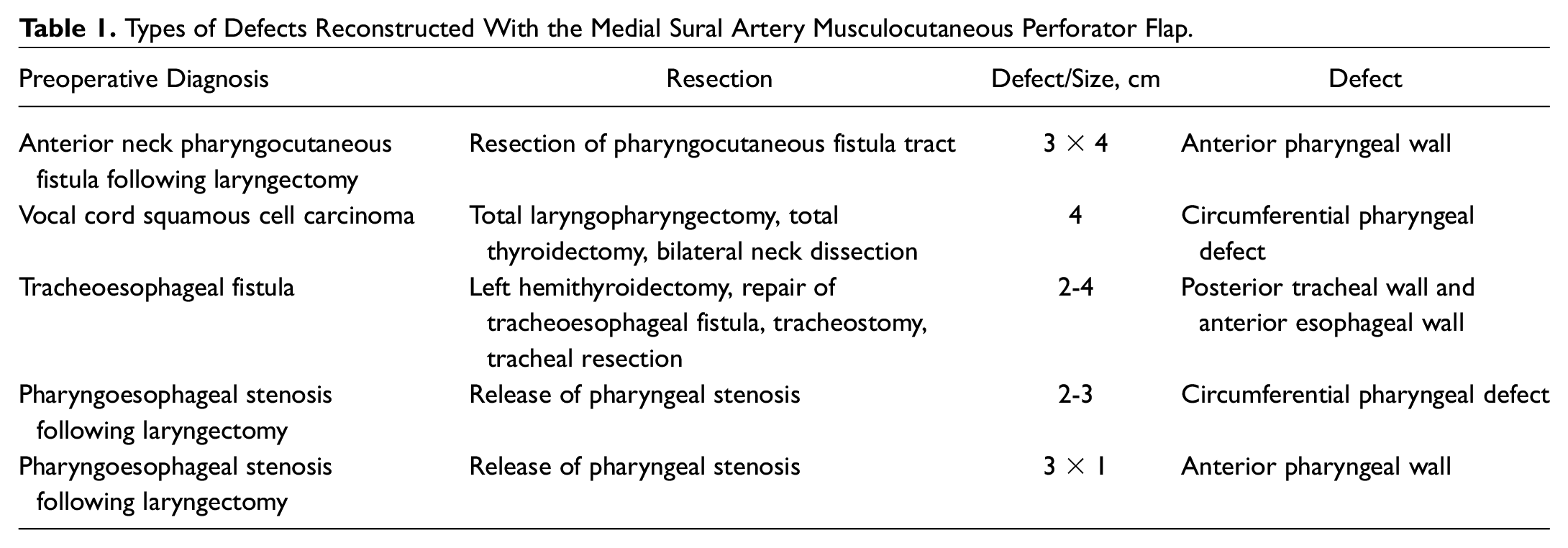
Types of Defects Reconstructed With the Medial Sural Artery Musculocutaneous Perforator Flap.
Patient demographics, preoperative diagnosis, history of radiation, surgery, chemotherapy, tobacco use, and comorbidities were recorded. Size and location of the defect, flap characteristics, and operative characteristics were measured. The primary outcome was flap success. Secondary outcomes included flap-related reoperation, flap failure (both partial and total), and other surgical complications (eg, fistula formation).
Harvest Technique
The harvest technique is similar to those previously described.4,5 The patient was placed supine with hip abducted and knee flexed. Each flap was harvested from the patient’s nondominant lower extremity or based on patient preference. Perforators were identified preoperatively using doppler ultrasound. A line was drawn from the midline of the popliteal crease to the medial malleolus, and the perforators were identified along this line approximately 8 cm from the popliteal crease within a 2- to 3-cm radius. The anterior flap incision (medial) was made first, and the flap was raised in a plane just deep to the fascia enveloping the gastrocnemius muscle. If more than 1 perforator was identified, the more distal perforator was chosen to shift the skin paddle inferiorly and increase pedicle length. If a single perforator appeared clinically small or inaudible by doppler, a second perforator was incorporated into the flap, when available. Once the perforator was dissected to the pedicle, the pedicle was dissected to its take-off from the sural artery. After complete pedicle dissection, the posterior cut on the skin paddle was made ( Figure 1 ).
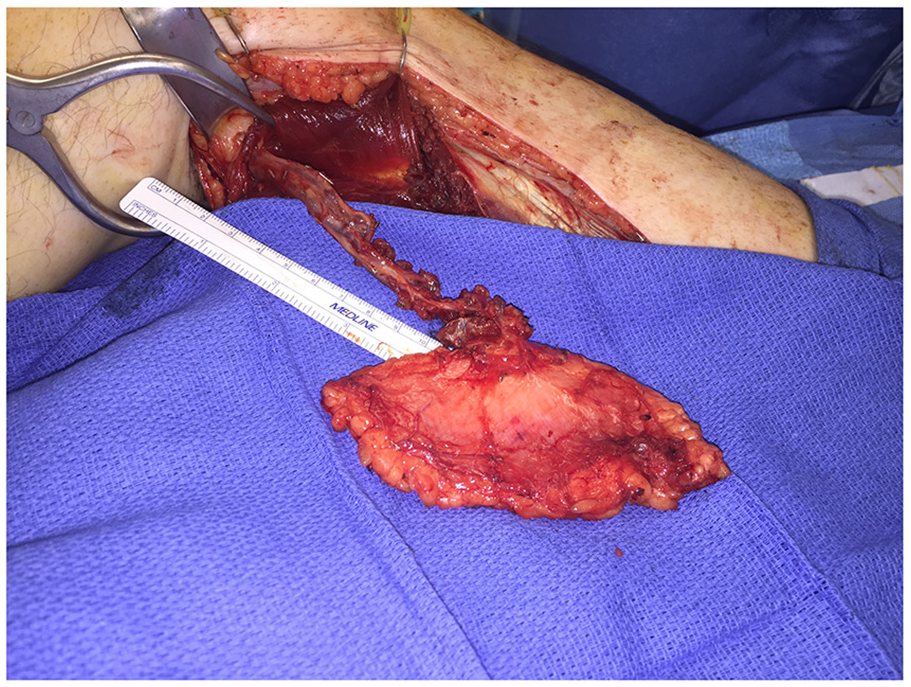
After careful dissection of the flap, this is how the flap appears right before ligation of perforator.
Flap Inset
The MSAP flap provides similar tissue to the RFFF with similar inset. The skin paddle is inset either as an anterior patch to augment the caliber of the pharynx or is tubed to circumferentially re-create the pharynx. In certain cases, the MSAP may be folded over onto itself, deepithelializing the outer half to provide a 2-layer closure of an anterior defect. The perforators can be quite fragile, requiring great care when handling the pedicle to prevent inadvertent damage ( Figure 2 ). No salivary bypass tubes were used in the procedure. Postoperatively, the flaps were monitored with implantable arterial and venous doppler devices.
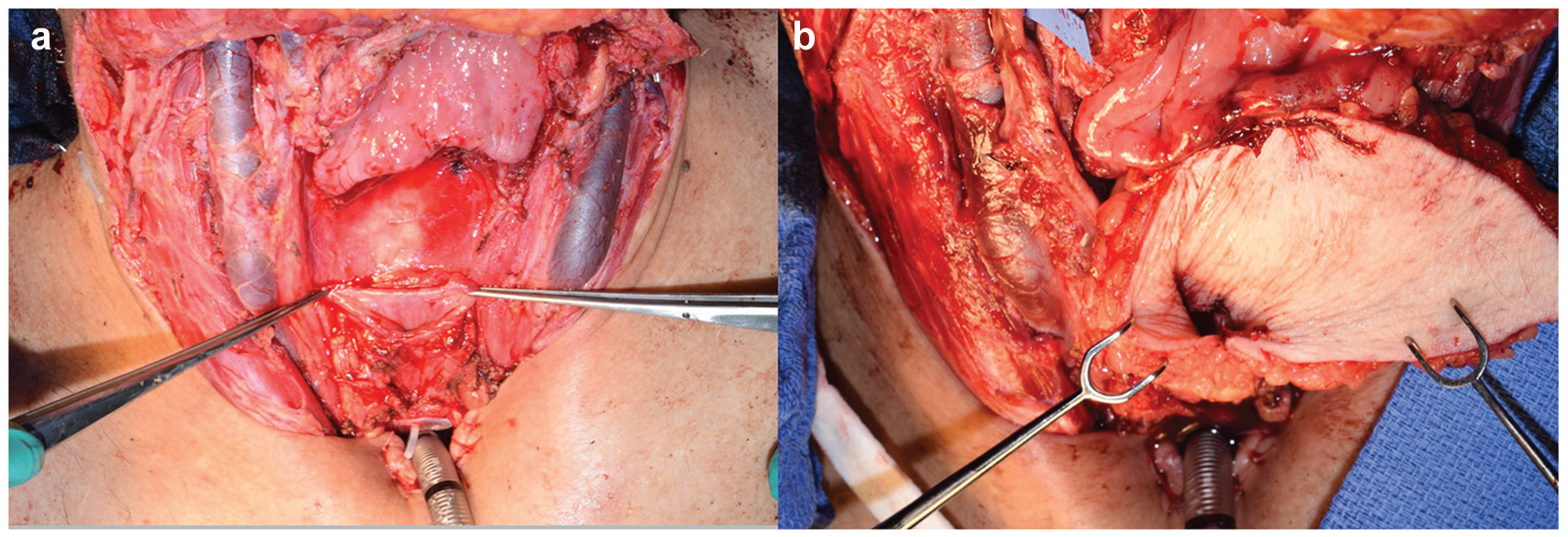
(a) Pharyngoesophageal defect during repair of stenosis. Repair of pharyngoesophageal stenosis prior to inset of medial sural artery musculocutaneous perforator (MSAP) flap. (b) Flap inset. MSAP tubularized inset for repair of pharyngoesophageal stenosis demonstrating the pliability of this flap.
Results
The MSAP flap was used in 5 patients for pharyngeal reconstruction. Average patient age was 57 years, and all were male. Four underwent either preoperative chemotherapy, radiation, or both. Two were used for anterior pharyngeal defects, 2 were tubed for circumferential reconstruction, and 1 reconstructed the anterior esophageal wall and posterior tracheal wall for a tracheoesophageal defect.
Flap skin paddle dimensions ranged from a length of 6 to 15 cm and a width of 4 to 8 cm. Average pedicle length was 10.8 cm (range, 10-12 cm). All donor sites were closed primarily. One takeback was performed for venous flap congestion with successful salvage on postoperative day 1. There were no partial or total flap failures or donor site complications ( Table 2 ).
Medial Sural Artery Musculocutaneous Perforator Flap Characteristics.

Four of 5 patients received MSAP flaps only, with local tissue rearrangement performed for external skin defects as necessary. One patient requiring reconstruction of a complex pharyngocutaneous fistula also underwent a right supraclavicular island perforator propeller fasciocutaneous flap in conjunction with a folded MSAP flap for anterior pharyngeal patching to assist with closure of the anterior neck external defect. The patient developed recurrent direct pharyngocutaneous fistulas at 2 and 4 months postoperatively. The patient underwent readvancement of the supraclavicular flap with full-thickness skin grafting followed by unilateral pectoralis major muscle flap and split-thickness skin grafting at 2 and 4 months, respectively. The patient died 2 weeks after the final procedure due to causes unrelated to the surgery.
Discussion
Pharyngeal reconstruction requires pliable tissue that can be manipulated to reconstruct complex 3-dimensional anatomy. The MSAP flap covers anterior pharynx defects, and its pliability allows folding for 2-layer closure while providing excellent contour. It has also demonstrated success in tubing for circumferential defects. Complete pedicle dissection to the source vessel (ie, popliteal artery) is necessary and allows for adequate vessel length and caliber. While in certain cases perforators may be small, with gentle handling during elevation, the entire flap can be based successfully on a single perforating vessel.
Lower extremity tissue laxity is favorable and facilitates primary donor site closure. In our experience, the MSAP donor site is less cosmetically concerning for patients than the RFFF, which risks tendon exposure, requires coverage with a skin graft, and is in a visible area of the forearm. 5
Conclusion
The MSAP flap is a highly versatile and reliable option in pharyngeal reconstruction due to its thin, pliable soft tissue and favorable donor site.
Author Contributions
Disclosures
Footnotes
This article was presented at the 2018 AAO-HNSF Annual Meeting & OTO Experience; October 6, 2018; Atlanta, Georgia.