
Abstract
The novel coronavirus disease (COVID-19), caused by the SARS-CoV-2 virus, has quickly become a global pandemic since its initial outbreak in China in late 2019. Institutions are faced with the challenge of upholding the standard of care while maintaining safety for health care personnel and patients. Due to the common performance of aerosol-generating endoscopic procedures in the upper respiratory tract, otolaryngologists are at uniquely high risk for potential infection. When possible, alternative diagnostic and treatment strategies should be pursued. For patients suspected of having functional laryngeal abnormalities, transcervical laryngeal ultrasound provides a rapid and noninvasive evaluation of vocal fold motion to inform decisions about safety of feeding, airway, and progression of care.
Keywords
Since its emergence in Wuhan, China, in December 2019, the novel coronavirus has quickly escalated to a global pandemic of unprecedented scale. As of April 2, 2020, it has infected >1 million people and resulted in >50,000 deaths. 1 Health care institutions worldwide are faced with the challenge of modifying care to reduce risk of virus transmission to medical personnel and other patients.
Through recent publications and unofficial communications, we have learned that physicians in otolaryngology are among the highest-risk health care personnel during the COVID-19 crisis, likely due to performance of aerosol-generating procedures in the upper respiratory tract. 2 Colleagues in Wuhan have described successful techniques to minimize aerosolization during necessary laryngoscopies and endoscopies. These include ensuring that adequate topical anesthesia is delivered on pledgets or via gel instead of by spray, as well as using small-diameter scopes to decrease the likelihood of a patient coughing or sneezing during an examination. 2 Appropriate personal protective equipment includes a gown, gloves, N95 mask, and face shield. 3 Our group has taken the additional step of requiring that only 1 physician be present during such procedures (typically the attending physician). Though still required for airway concerns, malignancy, or pathology requiring immediate attention, endoscopic examinations are otherwise being deferred a minimum of 30 days to protect practitioners and conserve personal protective equipment.
Since the onset of the pandemic and resultant changes in clinical protocols, we have constantly sought to find balance between necessary care and the safety of patients and health care providers. Laryngoscopy has been a particular area of consideration, as it remains one of the most common requests made of otolaryngologists. Though the airway may not be at risk, there are many scenarios in which assessment of laryngeal function is necessary to inform the progression of inpatient care, most commonly for suspected vocal fold paralysis or paresis. These decisions can be critical to increasing bed and, particularly, intensive care unit availability. In addition, among the emergency and oncologic surgical procedures still taking place, there are patients who will require periprocedural evaluation of laryngeal function.
With this in mind, our institution has implemented a protocol to perform transcutaneous laryngeal ultrasound in place of flexible fiberoptic laryngoscopy when appropriate. Ultrasonography provides a rapid and noninvasive method to assess vocal fold function and can guide decisions about dietary safety and enteral feeding. Perhaps more important, in light of the increasing numbers of patients expected to require intubation during this illness, early identification of a vocal fold issue may help avoid an emergency reintubation. Patient groups in whom this technique is being successfully employed include postcardiac or thoracic surgery, recent intubation, prior or recent cerebrovascular event, or suspicion based on clinical signs of aspiration and voice change. Pre- or postoperative vocal fold evaluation for thyroid or laryngeal oncologic procedures and airway evaluation are also possible.
Ultrasound assessment of vocal fold mobility has been described fairly extensively in the literature, particularly as it pertains to perioperative evaluation in thyroid and parathyroid surgery. When compared with the gold standard of fiberoptic laryngoscopy, the reported sensitivity and specificity of laryngeal ultrasound in detecting motion abnormalities range from 53.8% to 93.3% and 50.5% to 97.8%, respectively.4,5 Concordance with laryngoscopy findings ranges from 70% to upward of 95%.4,6 Adequate visualization can be affected by sex and age, with older men often being more difficult to image due to the shape and calcification of the thyroid cartilage. 7 Techniques such as viewing from a lateral or longitudinal approach or using a conductive gel pad can increase the likelihood of successful visualization.8,9
The basic laryngeal ultrasound technique is as follows: a high-frequency “small parts” transducer of 7.5 to 15 MHz is most commonly used, and the frequency is typically adjusted to the lowest end of the available range, while gain is increased as needed. Patients are typically supine with neck in extension, although the examination can even be performed in the seated patient. The transducer is applied to the skin with ample gel in the midline anterior to the vertical midpoint of the thyroid cartilage or inferior to it, by angling the transducer slightly superiorly. Some trial and error may be necessary to find the optimal imaging plane for any given patient. Vocal fold abduction and adduction are visualized during normal respiration and during breath-holding or Valsalva maneuver. When the patient is asked to stop breathing momentarily, the vocal folds adduct to the midline ( Figure 1 ). When the patient is told to resume respiration, vocal fold abduction is noted, confirming bilateral vocal fold mobility ( Figure 2 ). The true vocal folds are typically hypoechoic but may be distinguished by a fine hyperechoic line at their medial edges. The false vocal folds are hyperechoic and the arytenoid cartilages even more so. Even in the unconscious patient, it is possible to evaluate vocal fold mobility during passive breathing, with observation of small vocal fold movements with inspiration and expiration. Examination in the midline during phonation is more difficult and less successful, due to gross movement and simultaneous tilting of the thyroid cartilage upon the cricoid cartilage. However, if the vocal folds are not visible from a midline approach due to laryngeal calcification or poor laryngeal contact related to acute angulation of the thyroid alae, then each vocal fold can be assessed independently from a more lateral perspective. In this case, movement is observed during respiration or, better yet, during phonation, although symmetry cannot be directly compared.
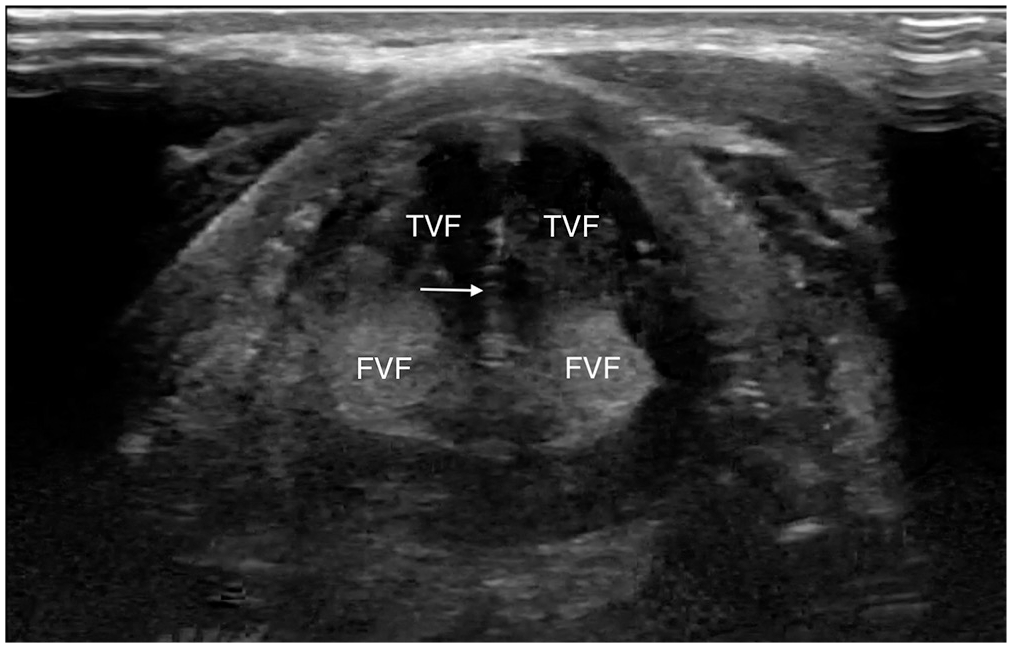
Transverse view of normal vocal folds during Valsalva (adduction). FVF, false vocal fold; TVF, true vocal fold. White arrow indicates hyperechoic medial margins of true vocal folds meeting in midline.
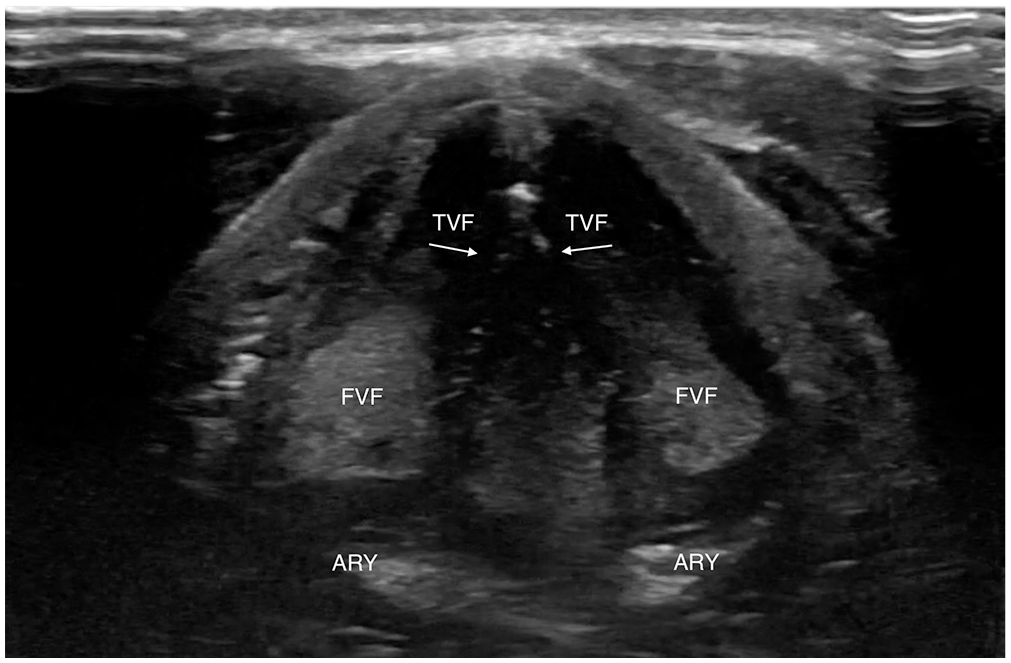
Transverse view of normal vocal folds during relaxation (abduction). ARY, arytenoid; FVF, false vocal fold; TVF, true vocal fold. White arrows indicate hyperechoic medial margins of true vocal folds.
Another advantage of laryngeal ultrasonography is the widespread availability and use of ultrasound technology. Relevant to the current crisis, physicians and health care providers in internal and emergency medicine, anesthesia, and critical care have extensive experience using ultrasound for diagnostic purposes and to guide interventional procedures. Even if unfamiliar with laryngeal evaluation, those with basic ultrasound knowledge are able to correctly identify vocal fold immobility without specialized training. 10 This also allows institutions without available otolaryngologists to perform rudimentary laryngeal evaluations. Furthermore, the need for handling and processing of an endoscope potentially contaminated with respiratory secretions, which are known to contain high viral loads, is eliminated.11,12
Ultimately, the findings on ultrasound must be considered in the context of the patient’s history and symptoms. In cases where ultrasound is not technically adequate or suspicion for pathology remains high despite an unremarkable scan, laryngoscopy should be discussed in line with institutional guidelines. In our experience, laryngoscopy is deferred unless intervention would decrease risk of aspiration and/or improve pulmonary toilet in a patient who may be at risk for reintubation.
With each patient encounter, we weigh difficult decisions about disease transmission and upholding the standard of care. Our position as otolaryngologists is unique, as procedures that were once routine now put us at high risk and must be carefully considered or avoided. As the COVID-19 crisis evolves, there is increasing uncertainty about the duration of impact on the health care system and a resultant need to find safer alternatives to treat our patients.