
Abstract

Hypoglossal nerve stimulation was first approved in 2010 for obstructive sleep apnea (OSA) in continuous positive airway pressure (CPAP)–intolerant patients. The phase III multicenter Stimulation Therapy for Apnea Reduction (STAR) trial commenced in July 2010 and 126 patients were implanted over 12 months. 1 With the average battery life of the device of 9 to 11 years, patients initially implanted in the United States are beginning to encounter depleted batteries.
To our knowledge, this is the first published case of implant pulse generator (IPG) exchange for hypoglossal nerve stimulation for battery depletion. We identify several considerations for successful completion. This case report meets exemption criteria for the Mayo Clinic Institutional Review Board approval.
Case Report
A 75-year-old man with history of severe OSA presented for hypoglossal nerve stimulator battery depletion. He was previously CPAP intolerant with an apnea-hypopnea index (AHI) of 60.4/h on polysomnogram in April 2010. He underwent hypoglossal nerve stimulator implantation (Inspire Medical Systems) in May 2010. The patient continued to use the device with good benefit. At a routine follow-up in September 2019, the patient had been using the device daily and had noted an irregularity in the intensity of the activation vibration of the device. Device data downloaded showed battery life as “depleted.” IPG exchange was recommended, and he was referred to the otolaryngology department. Remaining battery reserves allowed continued device use until the day of the exchange.
Preoperative anteroposterior (AP) and lateral chest x-ray showed the sensing lead coursing superficial to the IPG. The patient was brought to the operating room and administered intravenous cefazolin. The upper chest was sterilely prepped and draped with an antimicrobial incise drape. The exchange was performed under local anesthesia via 1% lidocaine with 1:100,000 epinephrine injected around the medial aspect of the device, taking care to avoid the leads. A vertical incision was made along the medial edge of the IPG rather than using the prior incision scar from implantation. Dissection was carried down to the IPG with sharp incision of the scar capsule made along the medial border of the device. Anchoring sutures were cut, and the IPG was delivered through the incision. The IPG and leads were separated from the scar pocket. Using a wrench, the leads were released and the IPG removed. The cavity was irrigated with antibiotic solution. A 3-cm × 3-cm piece of scar capsule was removed using sharp dissection. The leads were secured into the new IPG, and it was inserted into the pocket and secured with the leads’ contact points at the medial aspect and the wires deep to the IPG with 2 silk anchoring sutures. The new IPG was interrogated and proper functioning was ensured. The wound was closed in a multilayer fashion. The patient tolerated the procedure without discomfort, and blood loss was minimal. Postoperatively, the patient continued to use the implant without disruption and experienced no complications.
Discussion
Hypoglossal nerve stimulation remains a relatively new therapy for OSA, and this is the first report of IPG exchange by an otolaryngologist. Although performed by cardiac and neurosurgical specialists, there are several important differences of the procedure, including laterality of the device, orientation of the IPG, and location and course of the lead wires. Experience with IPG exchange thus far is limited, and performing this procedure safely will continue to increase in relevance for otolaryngologists.
Preoperative chest x-ray proved to be valuable as the sensing lead was found to be superficial to the IPG, putting it at higher risk for damage during exchange ( Figure 1A ). Therefore, a vertical incision along the medial aspect of the pulse generator away from the leads was planned rather than using the prior incision ( Figure 1B ). The manufacturer’s recommendation of orientation of the device has also changed with a 90-degree rotation as the current standard ( Figure 2C ). This places the lead contacts at the medial aspect of the capsule, and the leads wires are then placed deep to the IPG. Future IPG exchanges with this orientation will be better suited for using the original horizontal incision. This highlights the importance of understanding when the device was placed, the orientation of the device, and the course of the leads to plan the best approach to maximize the likelihood of protecting the leads during battery exchange. General anesthesia vs local anesthesia was discussed with the patient, and a shared decision was made to undergo the procedure under local anesthesia.
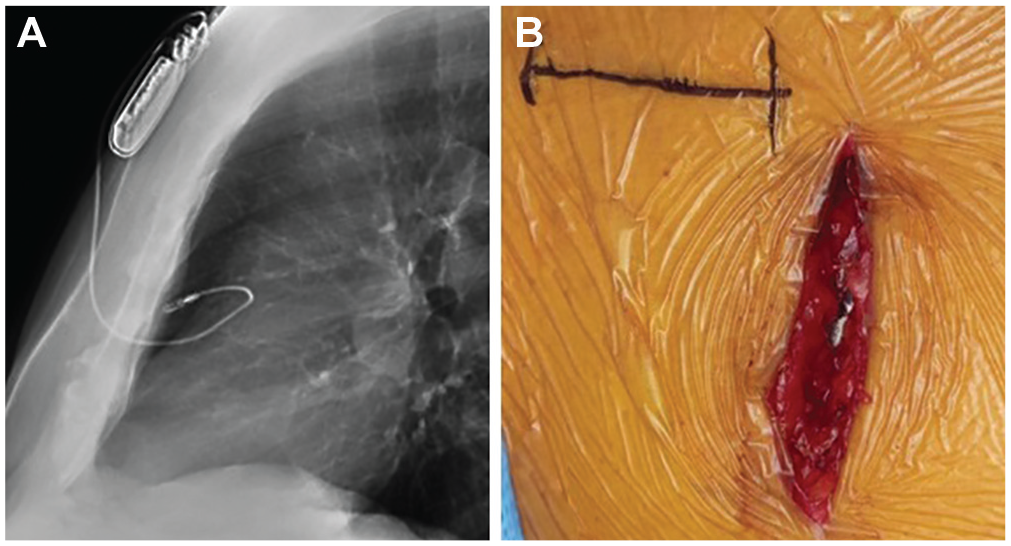
(A) Preoperative lateral chest x-ray shows sensing lead coursing superficial to the implant pulse generator. (B) Vertical incision for exchanged vs prior incision scar (outlined with marking pen).
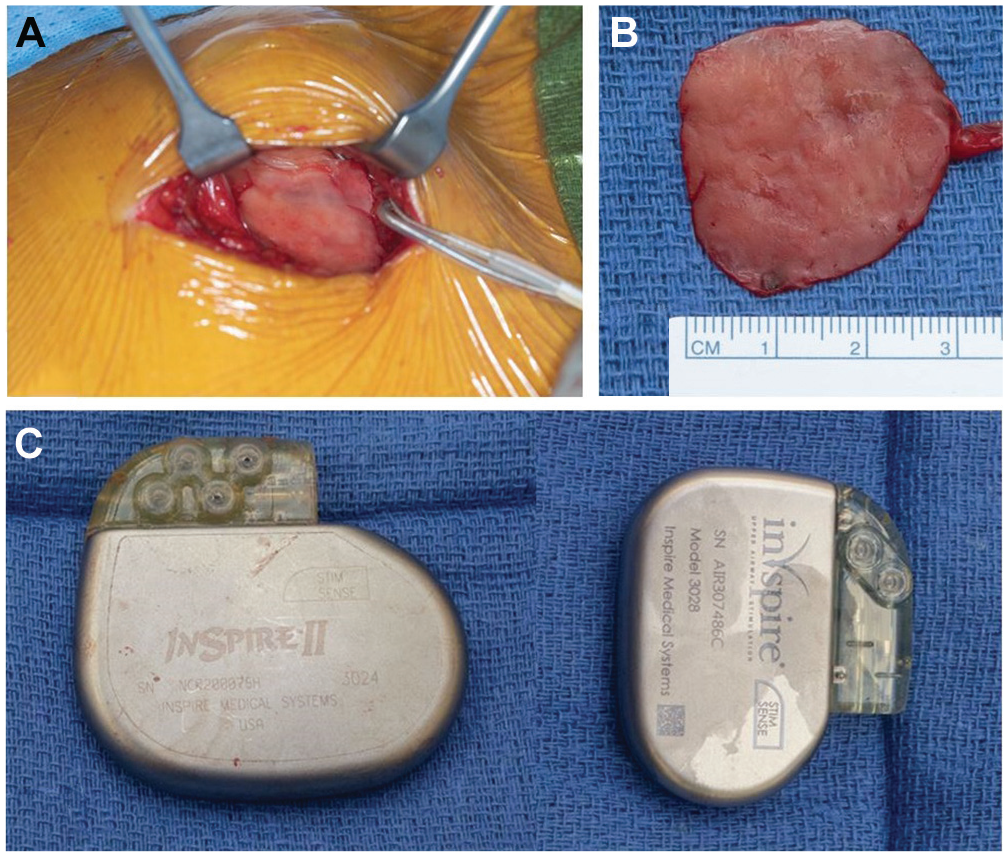
(A) Implant pulse generator pocket and scar capsule. (B) Scar excised from deep aspect of capsule. (C) Comparison prior size and orientation of the old model (left) and new model (right).
A limited capsulotomy was performed in this case (
In conclusion, implantable pulse generator exchange for battery depletion can be safely accomplished under local anesthesia. The principles outlined herein may reduce the risk of inadvertent damage to implant leads and postoperative seroma. Greater experience and further studies will help develop and refine best practices for this procedure.
Footnotes
Author Contributions
Disclosures
This article is associated with a scientific poster submission for the AAO-HNSF 2020 Annual Meeting & OTO Experience; September 13-16, 2020.