
Abstract
Objective
To (1) review concepts of medical hierarchy; (2) examine the role of medical hierarchy in medical education and resident training; (3) discuss potential negative impacts of dysfunctional hierarchy in medical and surgical training programs, focusing on otolaryngology; and (4) investigate solutions to these issues.
Data Sources
Ovid Medline, Embase, GoogleScholar, JSTOR, Google, and article reference lists.
Review Methods
A literature search was performed to identify articles relating to the objectives of the study using the aforementioned data sources, with subsequent exclusion of articles believed to be outside the scope of the current work. The search was limited to the past 5 years.
Conclusions
Two types of hierarchies exist: “functional” and “dysfunctional.” While functional medical hierarchies aim to optimize patient care through clinical instruction, dysfunctional hierarchies have been linked to negative impacts by creating learning environments that discourage the voicing of concerns, legitimize trainee mistreatment, and create moral distress through ethical dilemmas. Such an environment endangers patient safety, undermines physician empathy, hampers learning, lowers training satisfaction, and amplifies stress, fatigue, and burnout. On the other hand, functional hierarchies may improve resident education and well-being, as well as patient safety.
Implications for Practice
Otolaryngology–head and neck surgery programs ought to work toward creating healthy systems of hierarchy that emphasize collaboration and improvement of workplace climate for trainees and faculty. The goal should be to identify aspects of dysfunctional hierarchy in one’s own environment with the ambition of rebuilding a functional hierarchy where learning, personal health, and patient safety are optimized.
Keywords
Workplace hierarchies exist to achieve unified professional goals, and across professions, such as business and the military, a well-organized hierarchy is vital for efficient, safe operations. In medicine, trainees and students undoubtedly benefit from mentorship, role modeling, teaching, guidance, and the safety net that their faculty provide. A common theme among these “functional,” as opposed to “dysfunctional,” hierarchies 1 is that lower-ranked individuals are empowered to use their voice, share relevant information, and be treated as valued members of the group. 1
While hierarchies may be beneficial, many examples exist of rigid hierarchies resulting in catastrophes—from airplane accidents to surgery mishaps.2,3 Negative impacts of hierarchy have been documented in various medical professions,4-6 and they have the potential to create moral distress and ethical dilemmas; endanger patient safety; amplify stress, fatigue, and burnout; undermine empathy; hamper learning; lower training satisfaction; discourage use of “voice”; and legitimize trainee mistreatment.5,7,8 These, in turn, may influence trainee career choices, decrease patient care quality, and contribute to poor health and well-being.7,9 The negative impacts of hierarchy also affect attending physicians, in particular, junior faculty.10,11 Therefore, while well-structured hierarchy in medicine is commonplace,8,12 the consequences of hierarchy on trainee education have not been critically examined.
The 4 major goals of this article are to (1) clarify the concept of medical hierarchy; (2) examine the role of medical hierarchy in medical education and resident training; (3) discuss the potential negative impacts of dysfunctional hierarchies, with a critical focus on the field of otolaryngology; and (4) propose solutions to these issues facing otolaryngology trainee education.
Methods
A comprehensive review of the literature relating to hierarchy in otolaryngology and other residency programs was performed ( Figure 1 ). A systematic, computerized Medline, Embase, and Google Scholar database search of English journals and conference abstracts was conducted using the following terms: hierarchy, work environment, collaboration, workplace, culture, student, medical student, resident, residency, training, otolaryngology, otorhinolaryngology, OMFS, surgery, surgical subspecialty, moral distress, patient safety, ethics, shame, psychological safety, feedback, burnout, stress, fatigue, and quality of life. Medline and Embase were queried through Ovid. Search was limited to years 2014 through 2019 in line with state of the art review guidelines. The search revealed 1515 partially overlapping results, of which 773 were unique articles; 684 articles deemed to be outside the scope of the article were excluded. Exclusion criteria included basic science articles and articles that did not directly address work environment on medical trainee experiences. From this search, 84 articles and 5 conference abstracts were further analyzed, and an additional 14 articles were retrieved through review of reference lists for analysis. Articles and abstracts were grouped together based on themes: socialization and the “hidden curriculum” (5); psychological safety, voicing of concerns, or communication (7); patient safety (9); work environment and support (13); ethical dilemmas, moral distress, and empathy (9); harassment or discrimination (9); and well-being and burnout (37). Twenty works were primarily focused on the field of otolaryngology. Forty works from these search criteria that provided novel ideas were ultimately included. Redundant works that did not contribute novel findings were excluded.
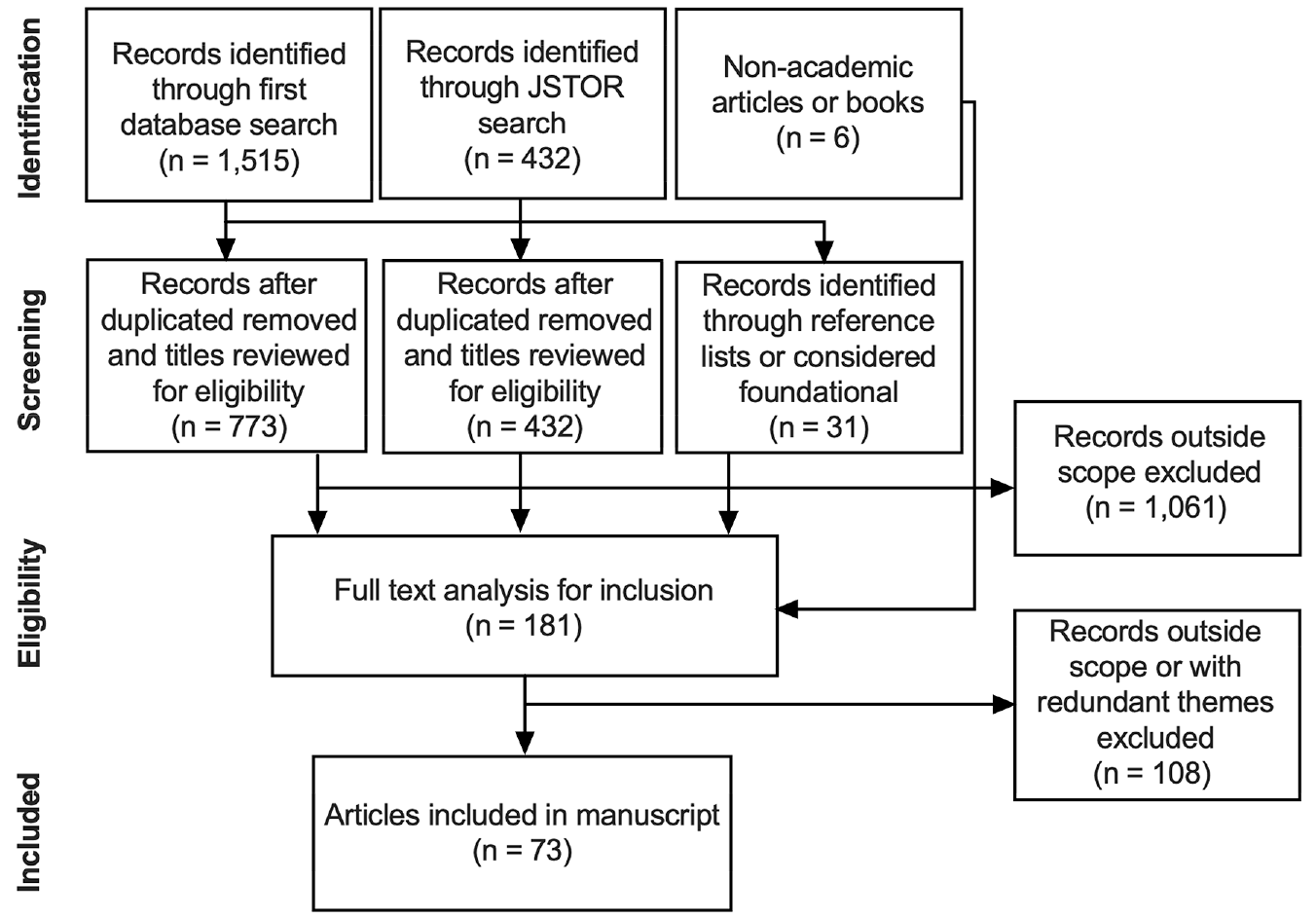
Modified Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram outlining search process and selection of manuscripts incorporated into the analysis.
At first, only articles specific to medical student or resident education were flagged for an in-depth review. Subsequently, in addition to the data sources previously mentioned, JSTOR was queried to select articles that investigated the psychological principles behind hierarchy and its impact on business, management, and biological sciences. The search terms used included hierarchy, learning, environment, training, resident, and hospital. From this search, an additional 432 academic articles were found, of which 47 were selected for further analysis. Articles were grouped as being not transferrable to medicine (23) or by the themes of hierarchy and team dynamics (12), impact on the follower (3), or theories of leadership (9). These themes have parallels related to resident education. Ten articles from this search were ultimately included.
For the “Background” and “Strategies for Change” section, business practices outside of academic literature were selectively searched for using Google. These search terms included union, business, Silicon Valley, technology, Facebook, Uber, Google, Apple, townhall, employee appreciation, business ladder, communication, burnout, professionalism, leadership, power, psychological safety, social status, resident union, and medical union. We believed the benefit of inclusion of nonacademic articles from Google searches outweighed the potential lack of future reproducibility inherent with its search algorithm. This is because results from these searches were not used as foundation for theory and core arguments in this manuscript. Five articles and 1 book from this search were included.
Finally, a further addition of 17 academic articles from outside the 5-year reference window, ranging from 1992 to 2013, were included as foundational works in the field. Foundational was defined as work for which current academic articles have been based, and without mentioning in this work, context for discussion would be incomplete. These include works that established the bases for academic theories or were seminal in their fields.
Discussion
Defining Hierarchy
Organizational Structure
Organizational structure defines how people in leadership positions interact with subordinates. One prototypical organization structure is a “hierarchical” structure, in which there are different levels of leadership that are ranked from employees to directors. 13 The reasons for hierarchical structures are readily apparent, in that centralization of power allows for delegated responsibility to ensure goals of the organization are met and to satisfy “stakeholders.” 14 In doing so, however, hierarchical structures sacrifice democracy, 15 and this trade-off may result in tension within the organization. Therefore, inherent in these organizational structures are differing roles and responsibilities of “followers” and “leaders,” and the interaction between these groups ultimately results in whether the organization will be “functional” or “dysfunctional.” 16 For this reason, before addressing organizational structure in medicine, an overview of theories in leadership and organization conduct is warranted.
Leadership Strategies within Hierarchical Systems
In recent years, there has been a trend toward describing and advocating for the adoption of new leadership styles. These “new genre” leadership theories, including ethical leadership, authentic leadership, and transformational leadership, focus on how leaders can more effectively interrelate with their followers.17-19 For example, ethical leadership involves leaders demonstrating “normatively appropriate conduct through actions and interpersonal relationships, and the promotion of such conduct to followers through two-way communication, reinforcement, and decision-making.” 20 In other words, a leader should demonstrate the norms of an organization through his or her words and actions. Utilization of these leadership styles improves intrateam and organizational-level performances, bolsters follower satisfaction, creates a climate of fairness, improves a follower’s career satisfaction, reduces staff turnover, and empowers ethical behavior.17,18,21,22 More specifically, through honesty and trustworthiness, ethical leaders have been shown to achieve a higher degree of moral authority and create an ethical work climate. 22 These leadership theories rely on hierarchy to promote the successful execution of organizational goals; however, active engagement and dialogue between the leader and follower are fundamental components to achieve these aims.
Power Distribution Within Hierarchical Systems
Hierarchical systems inherently have centralization of power, which is distributed and delegated to different degrees depending on the organization. When organizations increase centralization of power, it results in decreased personal autonomy. 15 In colloquial terms, “micromanaging” has been shown to reduce psychological empowerment. On the other hand, organizations that value “transparency, incentives for initiatives, [and] creation of opportunity” result in higher performance and citizenship of employees. 23 Another study reported that “guided autonomy,” in which upper-level managers provide increased autonomy for mid-level managers based on an organization’s core values and set of guiding principles, resulted in more targeted and specific interventions for local stakeholders compared to a system that provided less autonomy. 14 Finally, a study from Columbia Business School that examined deaths during mountain climbing found that when expeditioners were given the autonomy to voice concerns and not be punished, fewer deaths could occur. 16 These studies in the management literature support that provision of autonomy, under the correct conditions and set of guiding principles, allows for the creation and sustainment of a “functional hierarchy.”1,14
Hierarchy in Academic Medicine
Academic medicine is most typically a hierarchy, in which attending physicians manage the actions of fellows, residents, and medical students.7,24 Moreover, fellows supervise residents, and residents supervise medical students, and so forth. Typically, those higher up on the ladder have greater power, control, and voice. Indeed, well-organized and functional hierarchical systems under this model have the potential to benefit both residents and patients. Residents benefit from faculty and fellows who provide clinical and practice expertise, positive reinforcement, role modeling, and a safety net. Moreover, attending physicians regularly espouse ethical leadership characteristics by acting in a manner consistent with the norms of their professional field and organization. Finally, increasing autonomy is provided over the years of training, and active learning allows for personal improvement through continual feedback. Taken together, a functional hierarchy is beneficial for the trainee and the patient.
However, for each of these potential strengths of hierarchy, there are potentially weaknesses. For example, strict hierarchies may create a “do as you are told” framework in which individuals may feel compelled to carry out orders even if against one’s better judgment.21,25 This organizational structure may result in intimidation of some team members, which may ultimately influence their behavior. 26 The hierarchical structure may create a dilemma of deferred responsibility wherein those lower assume that the “higher-ups” are always correct. However, the “higher-ups” often expect subordinates to “speak up” if they catch a mistake. 27
It becomes apparent that when one area of hierarchical structure becomes detrimental, tension within the organization may result and decrease its ability to effectively achieve its missions. The remainder of the Discussion section will focus on problems that arise when hierarchy in medicine fails to be functional but rather becomes a detriment to the medical or surgical trainee. The goal is to elucidate characteristics of dysfunctional hierarchies to allow for individual programs to reflect and consider areas of potential improvement.
Areas Affected by Hierarchy
The Hidden Curriculum
The “hidden curriculum” refers to the socialization and acculturation of trainees into medicine and plays a large role in shaping trainee attitudes and behaviors.26,28 During this socialization, failure to conform to expectations can lead to personal jeopardy that has major implications for their future7,28 and teaches trainees to suppress their own concerns to prevent conflict with their seniors.7,29,30
The hierarchical structure of surgical teams also impresses standards for behavior on trainees. A study of behavior in the operating room (OR) revealed that most medical students perceived disruptive behavior, such as yelling, to be initiated by the attending surgeon and that such behavior led to apparent decreases in communication and increased mistakes. 26 Furthermore, medical students endorsed fear or stress as a result of such an environment. 26 Another study found that surgical residents often cited a desire to respect attendings’ management decisions as a reason for their delay in referral of patients to palliative care. 30
Voice, Psychological Safety, and Patient Safety
The concept of “psychological safety” includes the quality of feeling comfortable to speak openly without fear of retaliation. Rigid structuring in medicine has been directly implicated in limiting the voice of subordinates. 24 For example, in a study looking at surgical site infections, perceived ranking resulted in hesitation to speak up and challenge surgeons in part from fear of negative reactions. 31 Further studies suggest that one’s position within the hierarchy often determines the amount of voice one has. 32 Indeed, the 3 factors most associated with influencing the degree of voice in hospital staff are tenure, profession, and position—all of which are related to the hierarchy. 32
Hierarchy may also serve as a deterrence to meaningful communication and professional development. For instance, hierarchy in surgery programs acts as a barrier for residents to approach attendings for mentorship. 33 Furthermore, residents in programs perceived to have significant hierarchical culture are less likely to engage in high-quality feedback from faculty. 34 Since mentoring and feedback have both been shown to promote resident well-being,9,35,36 hindrance of these educational objectives amplifies rigid hierarchies’ negative impacts and further perpetuates them. Finally, hierarchical structure has been implicated as a hindrance to the creation of an inclusive workplace in health care organizations. 37
Moral Distress
The organizational structure of medicine leads to moral distress.7,8,29,38 Moral distress is the “experience of cognitive emotional dissonance that arises when one feels compelled to act contrary to one’s moral requirements.” 5 Often, a resident’s moral courage is outweighed by fear of repercussions from attendings. 28 This results in feelings of disempowerment, disenfranchisement, and hopelessness. 7 Many situations may create moral distress, such as negative role modeling, inaction by attending physicians, and witnessing substandard care or unethical behavior.5,8 The moral distress results from trainees witnessing these undesirable situations but being unable to address them due to their junior position. 7
Within pediatric surgery residency programs, a study found that 63% of residents experienced moral objection to a patient’s treatment plan but declined to express their opposition to the attending. 39 Moreover, 32% of the same cohort felt compelled to participate in staffs’ treatment plans despite their own objections. 39 In many of these instances, the residents reported feelings of guilt when proceeding with plans to which they disagreed. Indeed, 31% of residents felt reprisals could result from reporting unethical behavior of senior colleagues, and 58% of these residents felt that institutional-based policies for reporting unprofessional/unethical conduct fail to help. 39 The result of hierarchy in this study was a climate of fear.
Medical hierarchy also affects patient care by negatively affecting empathy. A recent systematic review found that moral distress experienced by residents during their training resulted in decreased empathy. 8 Decreased empathy has been linked directly to worse patient care and with higher rates of emotional exhaustion and depersonalization.8,40 Importantly, residents in technology-oriented specialties (TOSs), including surgery and otolaryngology, have been shown to have lower empathy scores compared to residents in people-oriented specialties (POSs), including internal medicine. 40
Trainee Harassment and Mistreatment
Hierarchy may further negatively affect trainees by perpetuating mistreatment. In surgical specialties, sexual harassment (SH) and gender discrimination are highly prevalent,41-44 with reported rates of up to 90% of female residents in cardiothoracic surgery having experienced SH. 41 SH is related to hierarchy in that persons in positions of “direct” leadership to trainees perpetrate SH at high rates of up to 71% in a study of cardiothoracic trainees and 31% of oral and maxillofacial surgery (OMFS) trainees.41,43 Furthermore, among those who experience SH, many do not feel comfortable reporting the offending actions to organizational leadership.41,43 Finally, SH further aggravates the negative effects of hierarchy by worsening ethical and moral distress. 42 Apart from SH, other forms of mistreatment including bullying, discrimination, and other forms of harassment in surgery are also prevalent at rates of 22.4%, 40.3%, and 31.2%, respectively, based on a recent meta-analysis.45,46
Mistreatment is not limited to residents. A survey of medical students found that “student abuse” was one of the 3 most commonly encountered professionalism dilemmas. 8 Most students report at least 1 incident of mistreatment by faculty (64%), residents (75.%), or both (68.9%). 47 The fact that students are more likely to be mistreated by residents, who are relatively near to them on the social ladder, highlights how the hierarchy may perpetuate a cycle of mistreatment. This mistreatment is associated with burnout, poor emotional and mental health outcomes, decreased confidence, lower career satisfaction, thoughts of regret, and decreased desire to pursue academic positions. 47
Autonomy, Burnout and Well-Being
As previously mentioned, the interaction and relationship between the leader, such as an attending physician, and the follower, such as a resident, is at the core of hierarchical organizations. While most of the implications of hierarchy occur within the work environment, the distribution of free time to a trainee within a residency training program is within the scope of this discussion. That is because demands of individual programs ultimately dictate the length of time residents spend inside the hospital (and therefore outside of it), as well as personal time for wellness while in and out of the hospital.
Rigid hierarchies reduce personal autonomy among those in the lower ranks, which directly affect control over one’s time. In residents, lacking control over work-life balance has been associated with burnout, increased sleepiness, distress, stress, depression, and other health complications.10,48-51 This may be in part related to chronic stress, which elevates cortisol and negatively affects physical and mental health, 49 performance in the OR, and trainee learning. 52
Organizational structure and support also affect residents. In a study involving general surgery residents, workplace climate and perceived organizational support significantly predicted job satisfaction and burnout. 35 Hierarchical structure has also been linked to poor emotional and mental health outcomes (eg, substance abuse, depression), decreased self-confidence, lower career satisfaction, thoughts of regret and dropping out, increased rates of surgical resident attrition, and decreased desire to pursue academic medicine.29,47,53 However, most resident “well-being” programs focus on coping mechanisms and resilience strategies as opposed to institutional correction of dysfunctional hierarchy. 35
Hierarchy in Otolaryngology–Head and Neck Surgery
Overall, there is a paucity of literature on the effects of hierarchy and training environment on otolaryngology residency. However, the existing literature suggests that hierarchy within otolaryngology–head and neck surgery (OTO-HNS) training programs may negatively affect patient safety, resident learning environment, and well-being.
In 2 recent studies, one in OTO-HNS and the other in OMFS residents, at least half of the residents in each program reported experiencing personal shame, and even more had witnessed a fellow resident being shamed.54,55 Attending surgeons were responsible for these instances. Residents were shamed in response to lack of knowledge in most cases. However, less frequently, it was due to disagreements over patient care. While such instances resulted in moments for personal reflection in certain cases, 52.5% of residents endorsed loss of confidence, 54 feelings of depression and isolation, and decreased job performance after being shamed by their attendings. 55
The negative effects of hierarchy in otolaryngology may directly and indirectly negatively affect patient care. In a survey of surgical residents (including OTO-HNS residents), a lower degree of perceived power differential between resident and faculty was correlated with an increase in a sense of inclusivity and psychological safety. Increased perceived psychological safety, in turn, corresponded to an increase in resident willingness to report adverse events. 56 Another recent survey of OTO-HNS residents found that increased organizational support (ie, when hierarchy functions well and leadership supports residents) improves resident perception of their clinical learning environment. 9 Furthermore, those residents who perceived greater organizational support performed better on their yearly otolaryngology trainee examination. 9
Harassment is also prevalent in otolaryngology training programs. In a survey of OTO-HNS trainees in Australia and New Zealand, of those who responded, 17% experienced discrimination, 37% experienced bullying, 8% experienced sexual harassment, and 15% experienced any form of harassment. 57 Furthermore, a meta-analysis of burnout in medical and surgical residents found that OTO-HNS residents reported the highest depersonalization scores (53.3%) and second highest emotional exhaustion scores (47.3%), trailing only general surgery. Well-being and sleep deprivation are significantly worse in junior OTO-HNS residents when compared to more senior residents, 48 indicating a potential relationship with hierarchical ranking. In addition, burned-out OTO-HNS residents are less likely to pursue fellowship. 9
Organization structure also directly affects a resident’s access to wellness resources. A study of OTO-HNS program directors (PDs) found that 25% of programs are noncompliant with basic wellness requirements mandated by the Accreditation Council for Graduate Medical Education (ACGME), more than 40% of programs do not formally monitor resident burnout, and most do not have policies to address the ACGME requirement for protected time for medical/dental appointments. 36 Alarmingly, 1 PD in the study remarked that modern OTO-HNS trainees are just “soft.” 36 Such a comment highlights, without intervention, the cycle of mistreatment pervasive in medical hierarchy may continue to sustain itself.
Summary
Academic medicine’s hierarchical organizational structure, in its most functional form, provides for patient safety through the centralization of medical decision making and educates trainees through active learning, role modeling, positive reinforcement, and engagement. At its core, this hierarchy relies on the successful communication and execution of ideas between the more experienced physician and trainee. We have outlined ways in which reduction in autonomy, poor role modeling, restriction of voicing of concerns, creation of ethical dilemmas, perpetuation of harassment, and overburden of trainees create dysfunction and tension within hierarchies. These factors all ultimately relate to discrepancy or lack of transparency between organizational values, a leader’s actions, and the trainees’ expectations.
Strategies for Change
To truly improve trainee education and work environment, a paradigm shift in the relationship between trainees and leadership needs to take place. Such paradigm shifts often take years of concerted effort and may explain why programs have focused on addressing the downstream consequences of the training environment rather than the root cause. 35 Meaningful change requires first recognizing rigidity that reduces transparency or open dialogue between different levels within a hierarchy as a problem and, second, working to improve the trainee work environment while combating the downstream effects of rigid hierarchy. That is, if people receive “training in teamwork to improve their culture, but are forced to continue using an inefficient and risky work system, much of the benefit will ‘bleed away.’” 58
To create change within the “team culture,” programs should embrace the idea of a “just culture,” in which trainees are not punished for expressing concerns and viewpoints. 59 Such a culture has recently been proposed in the field of patient safety and quality improvement (PS/QI) to improve safety. 59 It has been noted that for an individual to feel comfortable enough to have a voice, several criteria, including safety (freedom from fear of retribution), opportunity (forum for making voice heard), and legitimacy (feeling as though one’s voice actually matters), must be met. 32 In systems where leaders display openness, use transformational behaviors, and encourage staff to use their voice, employees are naturally more inclined to bring forth concerns instead of staying quiet.32,60 Residency training programs that encourage trainees to “speak up” may result in lower rates of treatment errors and improve trainee moral development, health outcomes, decision making, organizational learning, management productivity, and quality improvement.32,38,60,61 Furthermore, systems should aim to decrease perceived power differences and barriers to help create an environment in which residents feel comfortable approaching faculty for mentorship. 33 Indeed, through ethical leadership that aligns institutional core values and leadership actions, leaders may actually gain increased moral authority and performance that strengthens functional hierarchy. 22
Institutions and leadership should also focus on innovating ways to increase organizational support for trainees and junior faculty.9,35 Trainees perform best when they perceive support from their institution and when there is increased psychologic safety. 56 This occurs when an organization provides resources and support that highlights the value of trainees’ contributions and well-beings.9,35 Finally, with regard to harassment, unwanted behaviors should be addressed at the time of occurrence. Effective ways to stop harassment include distraction and interruption. 62 In these techniques, the unwanted behavior is stopped or interrupted when the perpetrator is distracted by another task or a “time-out” is called. 62 Furthermore, openness by leadership to hear, investigate, and act on complaints is needed.
On the leadership side, didactic programs designed to address the realities of the negative effects of hierarchy should be created and aimed at faculty. 5 With knowledge of how medical hierarchy affects their trainees’ lives, faculty may reflect on their personal role in helping make improvements. In addition, institutions should provide residents with an outlet to advocate for change. Just as institutions provide attending clinicians with opportunities to influence institutional culture through seats on committees and access to department chairs, 5 this same principle can be applied to residents by electing residents to the ethics committees, creating open forums to express concerns, or making department chairs routinely available to discuss issues.39,47
To cultivate this new culture, one may examine industries that have successfully restructured the archetypical hierarchy, such as the technology industry. For instance, at Facebook, Mark Zuckerberg regularly holds townhall-style meetings during which any employee, regardless of their position, has the opportunity to ask questions, voice suggestions, and showcase innovative ideas.63,64 In fact, these weekly sessions are common in Silicon Valley—Google, Twitter, and Uber all employ this tactic.63,64 Interestingly, despite having over 16,000 employees, information revealed about new projects, company secrets, and personal thoughts rarely ends up in the media.63,64 This speaks to the culture of trust that is fostered within a hierarchy that bolsters camaraderie, confidence, and legitimacy in the workforce.
Finally, organizations should promote the individual and personal lives of its trainees where possible, since residents who are physically and mentally well improve patient care. This can be seen in a psychology study in which doctors, primed with candy to stimulate happiness, came to a correct diagnosis nearly twice as fast as the control group and were 2.5 times less likely to “anchor” with the wrong diagnosis. 65 The ACGME has acknowledged the importance of the work environment on resident training and has created the Clinical Learning Environment Review (CLER) to “assess the role of quality and safety in residents’ learning environments.” 28 Several proposed interventions to increase trainee morale and minimize burnout include faculty mentorship programs, healthy food options during meetings, physical wellness programs, empathy training programs, professionalism forums, mistreatment programs, and mindfulness activities.36,48,66-68
Implications for Practice
Our literature review highlights the ways in which dysfunction within hierarchy can undermine institutional values and trainee education. 7 These effects include creating moral distress, restricting voice, reducing trainee autonomy, perpetuating mistreatment, and worsening burnout. * Attention should be directed to these issues because the entire specialty of OTO-HNS suffers as a result of their effects: burned-out and dissatisfied residents are less likely to pursue fellowship and academic medicine, have decreased career satisfaction, and are more likely to leave medicine entirely. 72 More so, lifestyle factors have been cited as drivers for medical students when choosing careers. 73 If OTO-HNS fails to address poor well-being in the specialty, this may affect the future caliber of potential residents.
OTO-HNS is in a unique position to revolutionize the future of faculty and resident learning environments for several reasons. First, to date, not much research has been done on this topic. Only 1 study in the OTO-HNS literature examines the role of the work environment on resident learning and well-being. 9 Second, more could be done to optimize resident work environments in OTO-HNS programs. 36 Third, since most academic OTO-HNS departments are relatively small, it may be easier to implement changes to program cultures than in larger specialties.
In conclusion, OTO-HNS programs would benefit from creating healthy systems of hierarchy that emphasize collaboration and improvement of the workplace climate for trainees and faculty. Programs should aim to focus on ethical leadership and increase available resources to promote organization-wide support for trainees.9,35 Programs should cultivate environments in which residents and junior faculty feel safe to use their voice and engage with leadership. The goal should be to create a supportive, collegial learning environment to facilitate a functional hierarchy. Yet, we acknowledge that implementing such shifts in practice will be challenging and run counter to some currently established cultural norms. It would be prudent for our field as a whole to look for ways to implement changes and to monitor for the resultant impact on quantifiable outcomes, such as patient care measures and trainee satisfaction and performance, to ensure these changes are inspiring positive change.