
Abstract
Efforts aimed at minimizing the spread of COVID-19 and “flattening the curve” may be affecting clinical care delivery for non-COVID-19 cases that include otolaryngologic and orbital conditions. We are witnessing changes in the manner that patients present, as well as modifications in clinical management strategies. An improved understanding of these phenomena and the contributing factors is essential for otolaryngologists to provide sound clinical care during this unprecedented pandemic.
Keywords
Since the World Health Organization declared a global pandemic on March 11, 2020, the novel coronavirus disease 2019 (COVID-19) has infected >3.5 million people, including >830,000 in the United States. 1 In response, hospital systems have implemented extraordinary measures to ensure safe patient care, conserve hospital resources, and limit spread of the virus. These efforts include expansion of COVID-19 testing, cancellation of elective surgery, closure of ambulatory facilities, implementation of telemedicine, and procurement of adequate personal protective equipment for health care workers. Likewise, much of the public health messaging has focused on measures necessary to “flatten the curve,” including social distancing and hand hygiene. Together, these efforts have shaped a new COVID-19 medical reality to which physicians have to adapt.
Lost amid a sea of COVID-19 coverage has been the significant impact that COVID-19-related measures have had on the care of patients without COVID-19. This “untold toll,” as referred to in a recent editorial in the New England Journal of Medicine, has affected all medical specialties. 2 Our treatment of patients at busy tertiary care hospitals in New York during the pandemic—those with urgent orbital conditions, in particular—has allowed us to better understand this phenomenon as it pertains to otolaryngology. Specifically, we highlight nuanced changes in the manner that patients are presenting, as well as modifications in clinical management strategies.
One of the greatest challenges that we now encounter is how to care for people “who are afraid to seek care.” 2 In line with recent evidence demonstrating fewer admissions for common emergencies such as heart attack and stroke during the pandemic,3,4 we have found that fewer patients are presenting to our emergency departments (EDs) with urgent otolaryngologic complaints. We believe that there are 2 explanations for this phenomenon. First, patients may be reluctant to present to clinical care settings due to concern of COVID-19 exposure. Second, given the widespread closure of offices and ambulatory settings, patients may find it increasingly difficult to follow up or obtain proper clinical guidance from physicians. We have treated several patients with orbital pathologies who presented in a delayed fashion and, as a result, allowed nonurgent pathologies to become emergent. This includes a 34-year-old-woman who presented with a large multiloculated intraconal orbital abscess and fluid collection in the infratemporal fossa 4 days following extraction of a maxillary molar ( Figure 1 ). By the time that she presented to the ED, she had no light perception vision, and her intraocular pressure had increased to 54 mm Hg. Despite emergent canthotomy and cantholysis at bedside and surgical drainage in the operating room (OR), she did not regain vision.
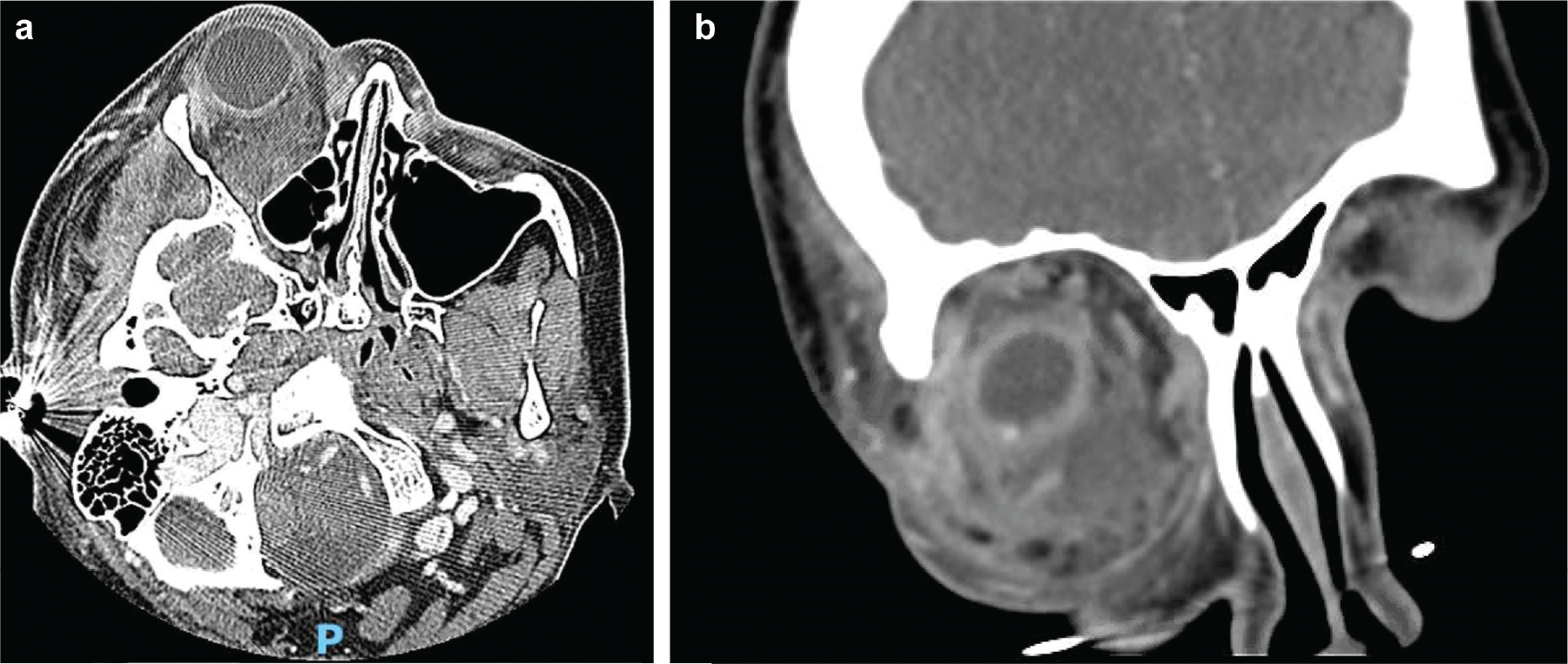
Computed tomography scan with intravenous contrast, including (a) axial and (b) coronal cuts, demonstrates fluid collection and phlegmon in the intra- and extraconal spaces of the right inferior orbit.
The potential for delayed presentation and advanced pathology belabors the need for hospitals to have a streamlined process by which patients can rapidly move from the ED to the OR. This process must include rapid, reliable COVID-19 testing and strict OR protocols designed to prevent viral transmission for patients with positive, negative, or undeterminable viral status. At our institution, we have employed variable personal protective equipment requirements for operative team members based on the result of the patient’s COVID-19 testing. Irrespective of test results, for all endonasal or orbital cases, the smallest possible surgical team is used, and transit in or out of the OR is prohibited during the entirety of the case.
We have also noticed distinct alterations in management strategies for certain otolaryngologic and orbital conditions during the pandemic—most notably, a shift toward medical management. This is undoubtedly due to concerns that certain operative procedures (ie, endonasal) presumably carry a high risk of viral particle aerosolization and viral spread.5,6 We have pursued medical treatment for several patients with orbital conditions that normally would be surgically managed. For a 47-year-old man who presented with a large subperiosteal abscess along the orbital roof secondary to a frontal sinus mucocele ( Figure 2 ), for example, we modified our standard institutional practice and treated with intravenous antibiotics and steroids, with the anticipation that surgery could be deferred. This avoided the risks of surgery, including a potentially longer hospital course, insertion of drains into a sinus potentially harboring viral infection, as well as possible viral transmission during the procedure. 6 This patient did remarkably well, improved consistently on ophthalmologic examinations, and was discharged on hospital day 2. Although his underlying sinus pathology still must be surgically addressed, his treatment illustrates the option to medically temporize as a risk reduction strategy.
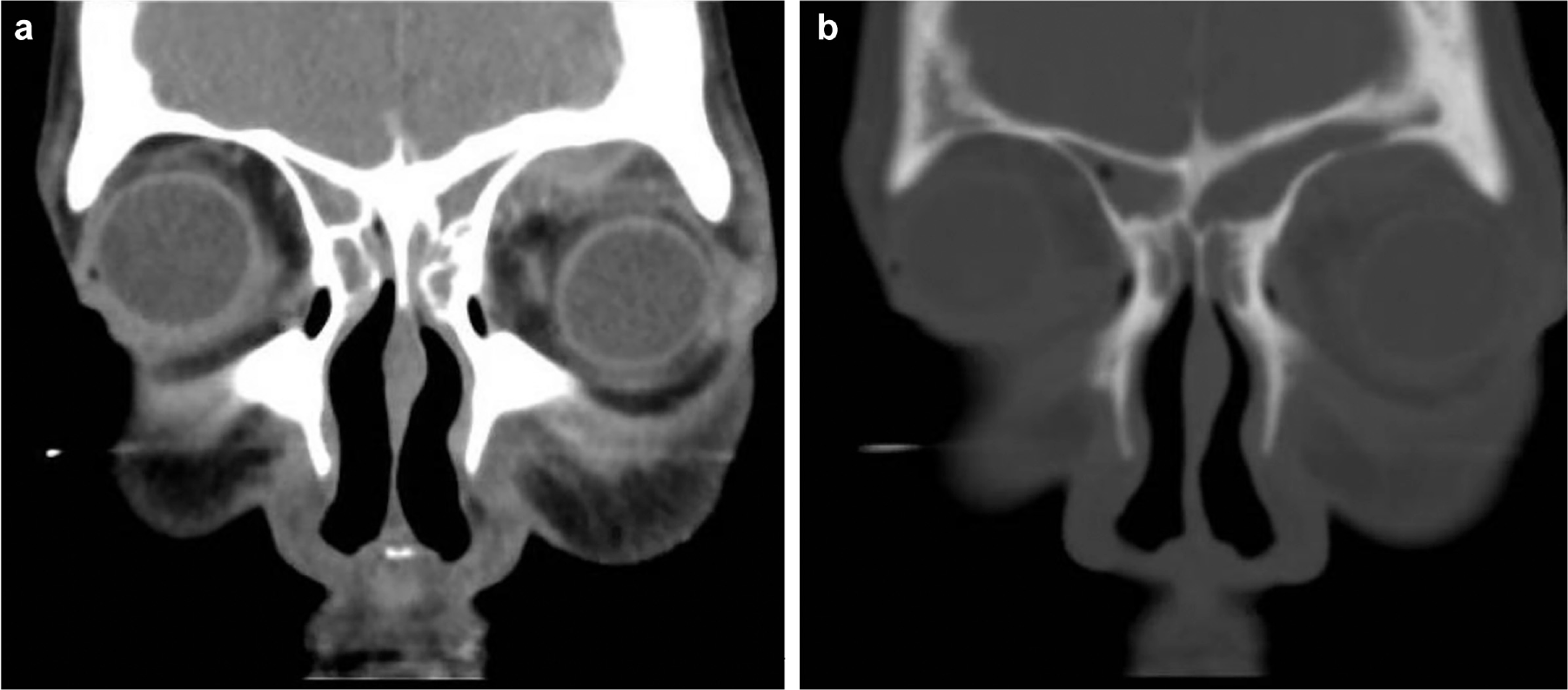
Computed tomography scan with intravenous contrast coronal cuts shows (a) left frontal sinus opacification with a subperiosteal abscess (1.3 × 1.6 × 0.5 cm) along the roof of the left orbit. (b) A small bone defect in the orbital roof can also be seen.
The unique circumstances surrounding COVID-19 may also motivate otolaryngologists to consider novel medical treatments as definitive therapies. In selected patients who have presented with Graves’ eye disease, for example, we have opted to forgo surgical decompression for medical treatment with teprotumumab, a human monoclonal antibody inhibitor of insulin-like growth factor receptor. 7 We recently decided against surgery for a 67-year-old woman with severe disease ( Figure 3 ) and new-onset compressive optic neuropathy due to her age, comorbidities, and months of preceding high-dose oral prednisone treatment. We felt that she was high risk for COVID-19-related morbidity and mortality if she contracted the virus either in the OR or during postoperative hospitalization. Teprotumumab was expeditiously started, and since her first infusion, her examination results have improved.
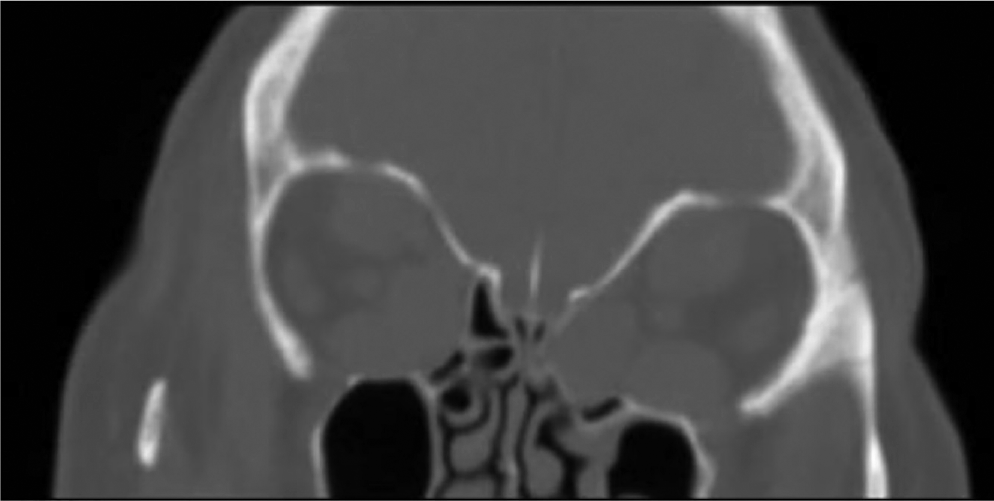
Computed tomography scan coronal cut illustrates diffuse enlargement of all extraocular musculature and bowing of the lamina papyracea bilaterally.
Moving forward, otolaryngologists must adapt to the evolving confines of the pandemic while not allowing vigilance for viral transmission to detract from the care of patients without COVID-19. This will ultimately require flexibility in regard to management strategies and recognition of the impacts that public health messaging have on patient presentation. To better understand this underappreciated phenomenon, objective study is needed.