
Abstract
Objective
There is little consensus regarding the efficacy and safety of treatment options for cricopharyngeal (CP) achalasia. The purpose of this scoping review is to assess the literature regarding the various treatments for this disease.
Data Sources
PubMed was searched for all articles addressing treatment of adult CP achalasia between January 1990 and June 2019.
Review Methods
In total, 351 peer-reviewed results were reviewed by 3 otolaryngologists for inclusion. After review of titles, abstracts, and full texts, 60 articles were selected.
Results
Among included studies, 55% were retrospective and 45% were prospective. Forty-five percent of studies were case series. CP achalasia etiologies included idiopathic (28%), cerebrovascular accident (CVA) (28%), neurologic disease (17%), head and neck radiation treatment (11%), Zenker’s diverticulum (10%), and myositis (5%). Most commonly employed treatments were botulinum toxin injection (40%), endoscopic CP myotomy (30%), dilation with either balloon or bougie (25%), and open CP myotomy (15%). A proportion of patients were treated with more than 1 approach. Most studies included both subjective and objective outcome measures. Complications were reported most often in patients with a history of head and neck radiation.
Conclusions
Small sample sizes and heterogeneity of causes and treatments of CP achalasia, as well as short duration of follow-up, make it challenging to assess the superiority of one treatment over another. There is a need for a prospective study that more directly compares outcomes of administration of botulinum toxin, dilation, and CP myotomy in patients with CP achalasia of similar etiologies.
The upper esophageal sphincter is the gateway to the esophagus. It is a 2- to 4-cm high-pressure zone that forms a barrier between the pharynx and esophagus. It is tonically contracted and opens briefly to allow the passage of the bolus into the esophagus during swallowing. This baseline closure at rest prevents reflux and aerophagia. The upper esophageal sphincter (UES) comprises mainly the cricopharyngeus muscle (CP). In practice, the UES and CP are interchangeable. The CP arises bilaterally from the lateral aspect of the cricoid cartilage and forms a posterior C-shaped band at the level of the junction of the pharynx and the esophagus. It is composed of small striated skeletal muscle fibers. The UES is opened by increased intraluminal pressure (by a bolus) or active distraction (by movement of the hyolaryngeal complex). During a swallow, vagal tone is inhibited and sphincter pressure falls about 200 ms prior to its opening. 1 This is followed by anterosuperior hyolaryngeal elevation and the generation of a pharyngeal constrictor and tongue base propulsive force, which drives the UES opening. As a bolus passes through the UES, the tension of the sphincter increases and allows for a greater force to be exerted by the UES behind the bolus, resulting in propulsion of the bolus and rapid closure of the UES.
During normal deglutition, the upper esophageal sphincter relaxes to allow passage of the bolus. An abnormality of the UES or CP, including failure to relax, stenosis, CP hypertrophy, the presence of a Zenker’s diverticulum, or achalasia, can cause a variety of symptoms from dysphagia to aspiration. 1 Bolus transit through the UES may be slowed by restricted opening, reduced pharyngeal driving forces, and impaired hyolaryngeal elevation. The most common causes of CP dysfunction are neurological disorders and the consequences, either directly or indirectly, of head and neck cancer. 2 Aging results in reduced CP compliance, strength, and muscle mass. Many neuromuscular diseases such as amyotrophic lateral sclerosis, polymyositis, myasthenia gravis, multiple sclerosis, Parkinson’s disease, and cerebrovascular accidents result in reduced muscle relaxation. 3 Dysfunction of CP opening can occur either in the timing of sphincter relaxation or in the ability of the sphincter to open widely enough to allow bolus passage. CP achalasia, failure of the CP to relax, may be idiopathic or result from gastroesophageal reflux disease, among other etiologies. 4
The causes of CP achalasia are as varied as the treatment options, which often depend upon the underlying etiology. Typically, surgical interventions are geared toward reducing sphincter tone or mechanically enhancing the UES opening through myotomy and/or dilation. 2 The current methods are best classified as endoscopic or open surgical procedures. Endoscopic procedures include the injection of botulinum toxin into the CP muscle, CP myotomy, and dilation. These may be done independently or in any combination. Dilation of the CP can be done using a balloon dilator or with rigid dilators such as the Savery dilators. Open surgical management involves accessing and dividing the CP muscle via a lateral cervical incision. With this much variety in approach, it is difficult to discern which method constitutes evidence-based medicine.
To date, no analysis has been done to discern which of these treatments is most successful. To counsel patients regarding the best treatment for their CP achalasia, we must first have an understanding of the duration of results and the risk profile associated with each procedure. The goal of a scoping review is to review a body of literature to identify knowledge gaps. It does not aim to provide a critically appraised and synthesized answer to a particular question; rather, it provides a summary or assessment of available data pertaining to a particular question. Often, it is a helpful precursor to a systematic review and can be used to confirm the relevance of inclusion criteria and potential questions to be addressed. The purpose of this scoping review is to assess the available literature regarding treatments of CP achalasia and their associated outcomes and complications.
Methods
A scoping review was performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist for Scoping Reviews. 5 This investigation was granted a waiver by the Stanford University Institutional Review Board. The search was confined to manuscripts published from January 1990 through June 2019 that described the treatment of CP achalasia in adult patients. Peer-reviewed review articles, case reports, case series, and 1 clinical trial were included. All causes of CP achalasia were permitted; however, studies focusing on CP achalasia solely in patients following total laryngectomy were excluded. Due to the heterogeneity of the inclusion criteria in the reviewed manuscripts, those with total laryngectomy patients as a subset of the larger study population were included in this analysis. Papers were excluded if their full text could not be accessed, if they included pediatric patients, or if they were not written in English.
A research librarian at the Stanford School of Medicine Lane Library assisted in the development of the search approach and search terms. PubMed, Web of Science, Embase, and the Cochrane database were queried for peer-reviewed literature regarding treatment of CP achalasia. The following terms were used and modified, if necessary, for the search: cricopharyngeus, upper esophageal sphincter, dysphagia, achalasia, dilation, botulinum toxin, myotomy, and cricopharyngeal bar.
Three authors independently scanned the search hits based upon the title, abstract, and keywords. The titles and abstracts of the search results were screened for relevant articles to be included in the review, based on the inclusion and exclusion criteria. The full texts of the remaining articles were then acquired and read in their entirety. In cases where there was uncertainty regarding the relevance of a record based on its abstract, the full text was screened. Discrepancies about which articles to include were discussed among the 3 authors and subsequently resolved. The full text of each article was stored in EndNote reference management software, and key variable data were extracted. Microsoft Excel was used to tabulate and store extracted data. The references of articles were reviewed to find additional articles that met inclusion criteria. If the title in a reference list seemed relevant to our objectives, we reviewed the reference and deemed inclusion based on the above criteria.
The following data were collected from each included article: date of publication, study type (case report, case series, cohort, review, or clinical trial), study description (retrospective or prospective), level of evidence, patient population, intervention, outcome measures, superiority of one intervention over another, duration of symptom improvement, duration of follow-up, reported complications, and sources of bias within the article. It was quite common that studies employed more than 1 method of management of CP achalasia. In this case, each method was considered individually. Therefore, the percentages of each treatment may total more than 100%.
Results
The PubMed, Embase, Web of Science, and Cochrane database searches yielded 351 unique articles. Based upon review of titles, 193 of those articles fulfilled inclusion criteria. After abstract review, 64 articles were identified for full-text review. The full text of 3 articles could not be located. Sixty-one articles were reviewed. Two of the 61 reviewed articles were noted to be literature reviews that did not present any patient data ( Figure 1 ). The details of 59 of the included studies are summarized in Supplemental Table S1 (in the online version of the article). Most studies meeting inclusion criteria were retrospective (55%). The most common study type was a case series (45%) followed by cohort study (36%). The remaining studies were case reports (6.7%), systematic reviews (5%), and 1 literature review (1.7%).
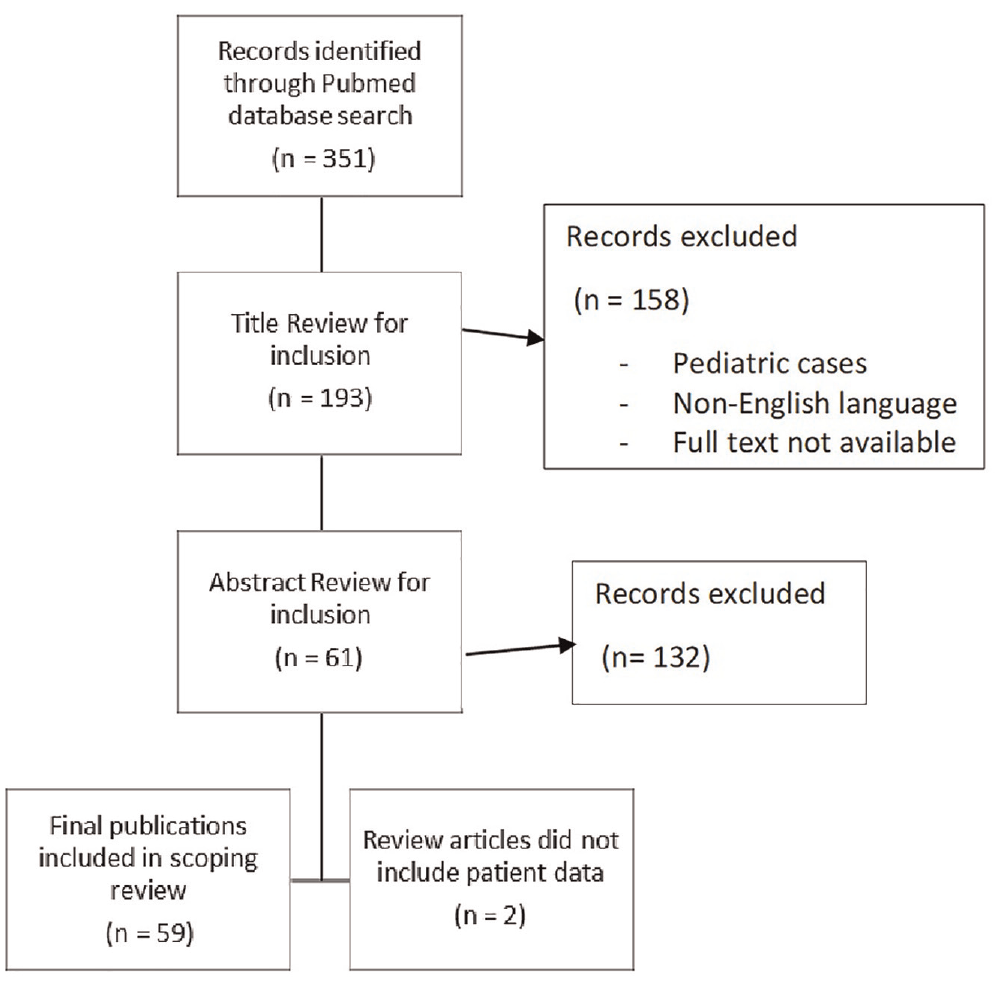
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram depicting the selection of articles to be included in this scoping review.
A detailed analysis of the quality of the studies included is beyond the scope of this review, as its aim is not to determine the efficacy of the various treatments. However, it is notable that the etiology of CP achalasia varied widely to include idiopathic (28%), cerebrovascular accident (CVA) (28%), neurologic disease (17%), head and neck radiation treatment (11%), Zenker’s diverticulum (10%), and myositis (5%). This heterogeneity further confounds the ability to directly compare treatment modalities, as the differing pathophysiology of disease may lend itself more appropriately or effectively to a certain intervention.
Interventions employed across studies included dilation with either balloon or rigid dilators (Savary or bougie), cricopharyngeal myotomy (open or endoscopic), and injection of botulinum toxin. Botulinum toxin injection was most common (40%), followed by endoscopic CP myotomy (30%), dilation with either balloon or bougie (25%) and open CP myotomy (15%). The administered dose of botulinum toxin ranged from 25 to 100 units. Within the reviewed studies, the duration of follow-up reported was too variable to assess the efficacy of differing doses of botulinum toxin for CP achalasia treatment. And in 6 patients, dysphagia worsened after botulinum toxin injection. 6 Dilation protocols also varied widely. Wei et al 7 employed a balloon dilation protocol involving dilation 7 times over a 4-week period, with the addition of botulinum toxin injection for a patient with cricopharyngeal achalasia following a cerebrovascular accident. In contrast, Murata et al 8 published a prospective case series treating cricopharyngeal achalasia in the setting of inclusion body myositis with intravenous immunoglobulin (IVIg) infusion followed by balloon dilation daily for 1 week. In prior work, it has been determined that endoscopic CP myotomy, in terms of swallowing outcomes, is equivalent to open CP myotomy. 9 Most studies employed a combination of treatments, and very few offered any comparison of treatment methods.
Comparison of outcomes is also challenging, as outcome measures were not standardized. Most studies employed at least 1 subjective and 1 objective measure of dysphagia. The most commonly used objective outcome measures were video fluoroscopic swallow study (VFSS) and fiberoptic endoscopic evaluation of swallow (FEES). VFSS results are reported on an 8-point penetration aspiration scale (PAS). FEES results, however, which were reported in over 25% of the included studies, have no uniform scoring system in the current literature. Results are, therefore, reported subjectively by the examiner and cannot be quantified easily or consistently. Symptomatic and subjective improvement was reported for the majority of studies. In addition, the ability to advance diet and remove feeding tubes was reported.
Twelve included papers made mention of complications. These were most commonly associated with balloon dilations in patients who had previously undergone radiation for head and neck cancer treatment. Abu-Ghanem et al 4 report a complication rate of 48% in those patients who have undergone endoscopic management via botulinum toxin injection, dilation, and myotomy for CP achalasia with a history of head and neck radiation. Complications include mediastinitis and subcutaneous emphysema. Complications reported in other series included microperforations, recurrent dysphagia, dental injuries, partial-thickness esophageal tears, laryngospasm, hematoma, and temporary unilateral vocal fold paralysis. Complications were also reported in poststroke patients in conjunction with botulinum toxin injection or balloon dilation of the CP. Only 1 hematoma was reported. This was in a poststroke population who underwent both balloon dilation and CP myotomy. 10
Studies included in this scoping review were plagued with bias. The most common sources of bias were the lack of a control group, lack of randomization of treatment modalities, and failure to mention patient attrition. In addition, the heterogeneity of the subjects with respect to underlying cause of CP achalasia, presence of systemic disease, and other laryngeal pathologies were notable sources of bias.
Discussion
The purpose of this scoping review is to assess the depth of the literature regarding treatment of CP achalasia. In general, the study methodologies, patient inclusions, treatment approaches, and outcome data were far too variable to allow a clear comparison of the currently available techniques.
The 3 most common treatments for CP achalasia are botulinum toxin injection, dilation, and myotomy. Esophageal dilation is perhaps the most traditional procedure discussed here. It may be performed with bougie or wire-guided dilators, such as Savary dilators, although most are done using the controlled radial expansion balloon dilators. A large published series of 46 patients dilated with 60 French esophageal dilators showed that two-thirds of patients experienced improvement in their swallow that lasted at least 2 years. 11 A large meta-analysis showed success rates ranging from 65% to 100% with recurrence seen in 0% to 50% of patients. 2 In general, CP dilations are typically temporary procedures for the radiation induced fibrotic UES and have a high incidence of symptomatic recurrence.
Botulinum toxin injection to the UES was originally described as an alternative to the more invasive CP myotomy. The toxin provides chemodenervation and temporarily weakens and relaxes the muscle to allow easier passage of the bolus. Although reported response rates range from 43% to 100%, 12 a recent Cochrane review determined that there was insufficient evidence for its use to inform clinical practice. 13 In our review, botulinum toxin was used most often in studies of patients with CP achalasia after a cerebrovascular event.
The CP myotomy remains the gold-standard treatment for upper esophageal dysfunction. Comparisons between open and endoscopic techniques are exclusively retrospective. Dauer et al 14 examined outcomes of 14 patients who underwent laser CP myotomy compared with 8 patients who underwent open transcervical myotomy. The endoscopic group had shorter operative times and hospital stays, with fewer major complications. Both groups demonstrated measurable functional improvement. A larger retrospective review by Huntley et al 15 compared the outcomes of 38 open vs 41 endoscopic myotomies and found shorter surgical times and improved outcomes with respect to dysphagia in the endoscopic group. CP achalasia is a condition that is treated by different specialties, including gastroenterology and otolaryngology, via noninvasive and surgical methods. Therefore, it is understandable that a direct prospective comparison in a large group segregated by etiology of different possible treatment for CP dysfunction does not exist.
This scoping review highlights the lack of direct comparisons between the methods of treatment. There is a need for investigations that weigh the benefits of each of these interventions against one another and also in the context of the differing etiologies of CP dysfunction. This review included studies of patients with systemic neurogenic disease, cerebrovascular events, Zenker’s diverticulum, history of head and neck radiation, and idiopathic CP achalasia. These are fundamentally different pathophysiologies and require further study to that end. The CP muscle will be fibrotic in those patients with a history of radiation exposure, while that is not the case in those patients with systemic neurologic disease. Zenker’s diverticulum and CP achalasia are on the same spectrum of pathophysiologic disease process, both involving a tightening of the CP muscle. These studies used various approaches to CP myotomy: endoscopic and open. Appropriately, they did not employ botulinum toxin injection or dilation.
Management of cricopharyngeal achalasia is a challenging and sometimes dangerous undertaking. It carries with it risk of esophageal perforation, leak, subsequent mediastinitis, and even death. Therefore, 1 goal in reviewing this body of literature is to identify not only the most effective means of managing achalasia but also the safest. Upon review of this group of investigations, 12 (20%) studies reported complications, most commonly in patients who have a history of head and neck cancer treated with radiation. 4 The most commonly reported complication was perforation. Dysphagia that develops after the completion of radiation treatment results from inflammation and fibrosis of the CP muscle. Radiation therapy can, therefore, result in stricture or stenosis at the level of the CP. This is a unique challenge, as radiation-induced stricture/stenosis is often remarkably fibrotic and resistant to dilation. Due to increased friability and fibrosis of the tissues, as well as loss of surrounding fat that occurs after radiation exposure, complications like esophageal perforation, subcutaneous air, and mediastinitis are more common in this subset of patients.
The authors acknowledge the many limitations and sources of bias within this review. As mentioned previously, the notable heterogeneity in the etiology of CP achalasia, treatment combinations and protocols, outcome measures, duration of improvement, and overall follow-up hinder the ability to draw conclusions regarding the efficacy or safety of any given treatment. Selection bias may also arise from inclusion of studies written in English and published within the past 29 years, although we would expect older literature to primarily report outcomes for open CP myotomy. There is a need for prospective data comparing available treatment modalities for cricopharyngeal achalasia. To date, the literature regarding efficacy and safety of the 3 most common interventions is inconclusive. In the design of future studies, patients should be aggregated according to the underlying cause of achalasia, and outcomes and duration of follow-up should be standardized. A concerted randomized trial would be invaluable in furthering knowledge in the area of treatment for CP dysfunction as a whole or for individual etiological groups.
Supplemental Material
OTO931470_Supplemental_references – Supplemental material for Cricopharyngeal Achalasia: Management and Associated Outcomes—A Scoping Review
Supplemental material, OTO931470_Supplemental_references for Cricopharyngeal Achalasia: Management and Associated Outcomes—A Scoping Review by Karuna Dewan, Chloe Santa Maria and Julia Noel in Otolaryngology–Head and Neck Surgery
Supplemental Material
Table_1 – Supplemental material for Cricopharyngeal Achalasia: Management and Associated Outcomes—A Scoping Review
Supplemental material, Table_1 for Cricopharyngeal Achalasia: Management and Associated Outcomes—A Scoping Review by Karuna Dewan, Chloe Santa Maria and Julia Noel in Otolaryngology–Head and Neck Surgery
Footnotes
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.