
Abstract
During the SARS-CoV-2 pandemic, patients in intensive care units who are undergoing long-term intubation may require tracheostomy. There is controversy about indication and health care professionals’ safety regarding the conventional or percutaneous technique. We performed a prospective analysis of a series of 27 consecutive patients with COVID-19 comparing both tracheostomy techniques, safety, and prognosis clinical markers. The results show that the techniques are equally safe, without cases of infection in surgeons. The Sequential Organ Failure Assessment score before surgery and the progression in ventilation support during the first 72 hours after tracheostomy are optimal prognostic markers for these patients.
Since the identification of a new type of pneumonia caused by a novel coronavirus in December 2019 in the city of Wuhan, the disease therefore known as COVID-19 has spread rapidly throughout the world to >180 countries. Spain has been one of the most hard-hit countries, with >213,000 cases diagnosed and 22,000 deaths as of April 23, 2020. 1
In hospitalized patients with severe COVID-19 and long-term endotracheal intubation, tracheostomy is usually considered. The decision about the type of tracheostomy—that is, percutaneous or conventional open tracheostomy—commonly relies on the responsible team. 2
Some controversy about these techniques currently exists in terms of appropriateness, time of procedure, or the aerosolization of the virus that can expose health care workers.3,4 Currently, open tracheostomy is the most common surgical procedure performed on patients who are infected, as it was during the SARS outbreak. 5
Material and Methods
We performed a prospective analysis (from March 1 to April 10, 2020) of a series of 27 consecutive patients with COVID-19 who needed a tracheostomy. Indications for tracheostomy were weaning failure, long-term mechanical ventilation, and inability to manage secretions. Those with a favorable neck anatomy were selected for a percutaneous tracheostomy, while patients with unfavorable anatomy were selected for conventional open tracheostomy.
Every tracheostomy was performed by 2 teams of experienced otolaryngologists, with full protective wearing, including N95 respirator, gown, cap, eye protection, and gloves. 6 The Tracoe Experc Dilation Set was used for every patient eligible for percutaneous tracheostomy. Every procedure was performed in the intensive care unit at the bedside.
We performed a logistic regression with multiple categorical and continuous predictors. We analyzed age, comorbidities, time of intubation, type of ventilation support, evolution, and Sequential Organ Failure Assessment (SOFA) score (range, 0-24 [best to worst]) as clinical markers of bad prognosis for in-hospital mortality ( Table 1 ). Improvement of ventilation support was also identified after the first 72 hours of tracheostomy. We considered an improvement of ventilation support when pressure support ventilation was achieved in patients with controlled mechanical ventilation.
Characteristics of the Analyzed Variables: Percutaneous vs Open Tracheostomy. a
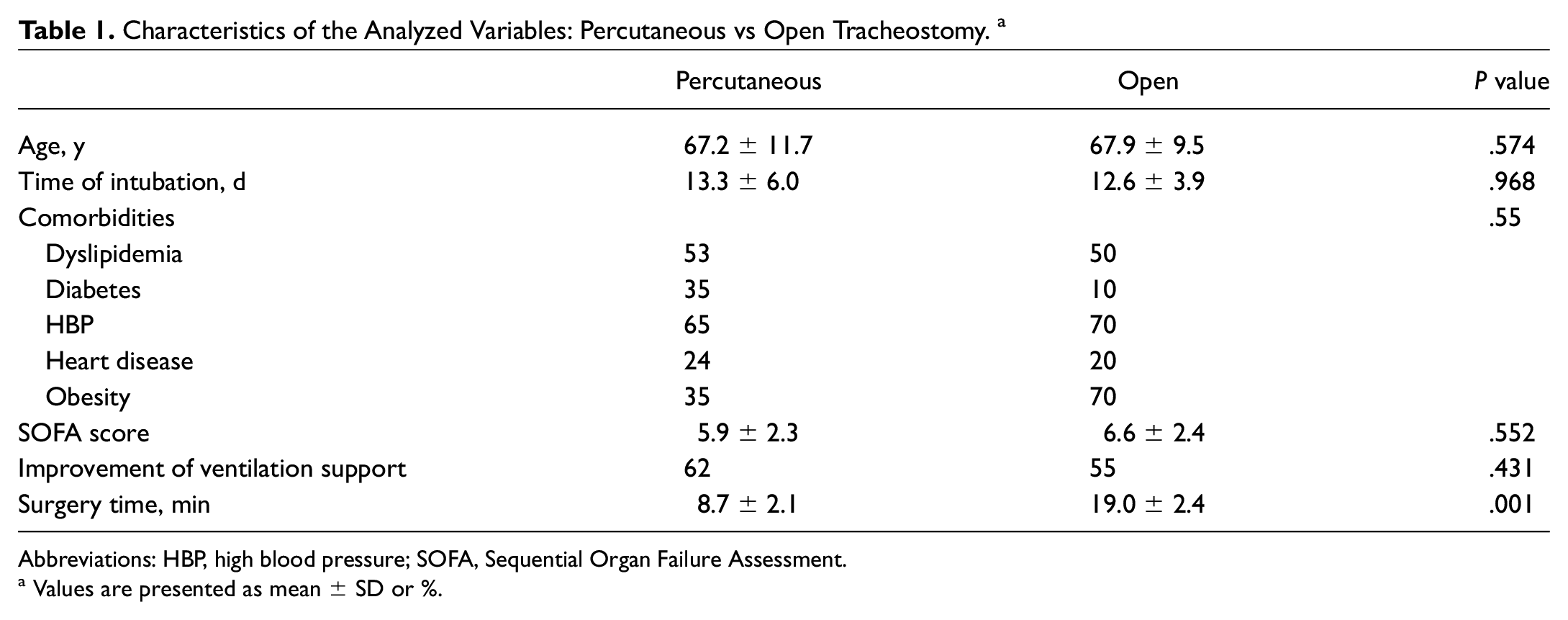
Abbreviations: HBP, high blood pressure; SOFA, Sequential Organ Failure Assessment.
Values are presented as mean ± SD or %.
COVID-19 in respiratory specimens was detected 1 week after the last tracheostomy conducted by each otolaryngologist—from nasal and pharyngeal swabs, by next-generation sequencing, or by real-time reverse transcription polymerase chain reaction (RT-PCR; Allplex 2019-nCoV Assay).
This project was approved by the institutional review board (Getafe Health Research Institute). Patient informed consent was obtained in every patient.
Results
Seventeen and 10 percutaneous and conventional tracheostomies were performed, respectively. We did not observe significant differences in the number of both techniques performed by either of the 2 otolaryngologist teams (χ2 = 1.67, P = .19).
Mean ± SD time of the procedure was significantly lower (P < .05) for the percutaneous tracheostomy (8.7 ± 2.1 minutes) than the conventional one (19.0 ± 2.4 minutes). Each surgeon had negative RT-PCR test result, so there were no significant differences between the techniques in terms of medical personnel safety. During the period of the study, no surgeon developed any symptom characteristic of COVID-19 infection.
The mean follow-up for the patients was 31 ± 11 days. Of the 27 patients, 11 (41%) died within 7 days after the tracheostomy. We did not observe any significant association (χ2 = 0.354, P = .55) between age, comorbidities, time of intubation, or surgical technique and the evolution of the patients. The clinical parameter that better predicted in-hospital mortality before the tracheostomy was the SOFA score, which was significantly higher (P = .001) in those patients who died (7.73 ± 0.52) than those who lived (4.75 ± 0.57; Figure 1 ). Likewise, all patients with an improvement in ventilation support after the first 72 hours of tracheostomy had less in-hospital mortality (χ2 = 7.34, P = .007; Figure 2 ).
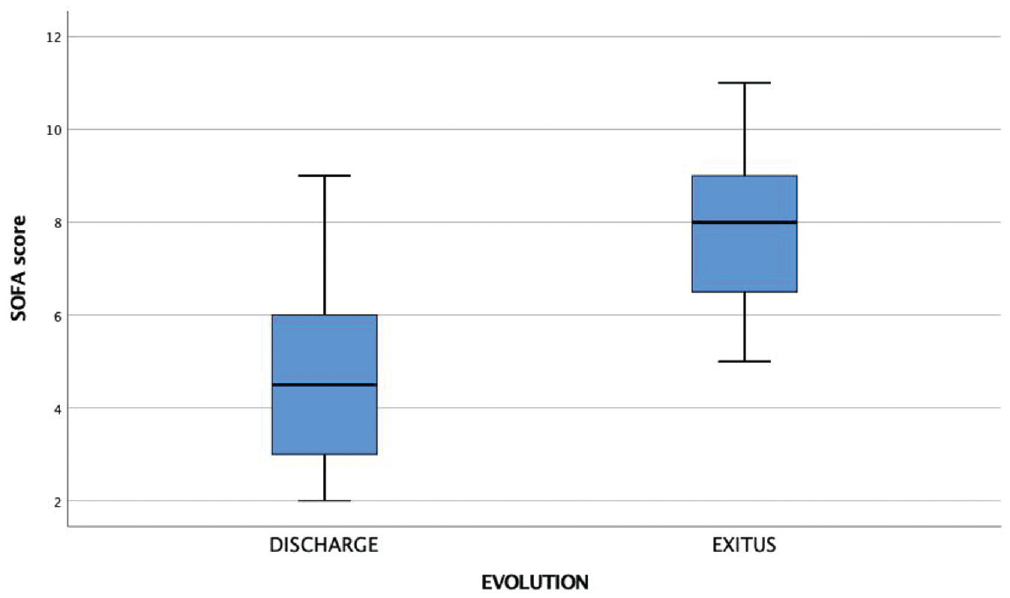
Box plot of SOFA score as a predictor of evolution. Patients who died 7 days after the tracheostomy had high SOFA scores as compared with patients who lived (P < .001). Values are presented as median, interquartile range, and 95% CI. SOFA, Sequential Organ Failure Assessment.
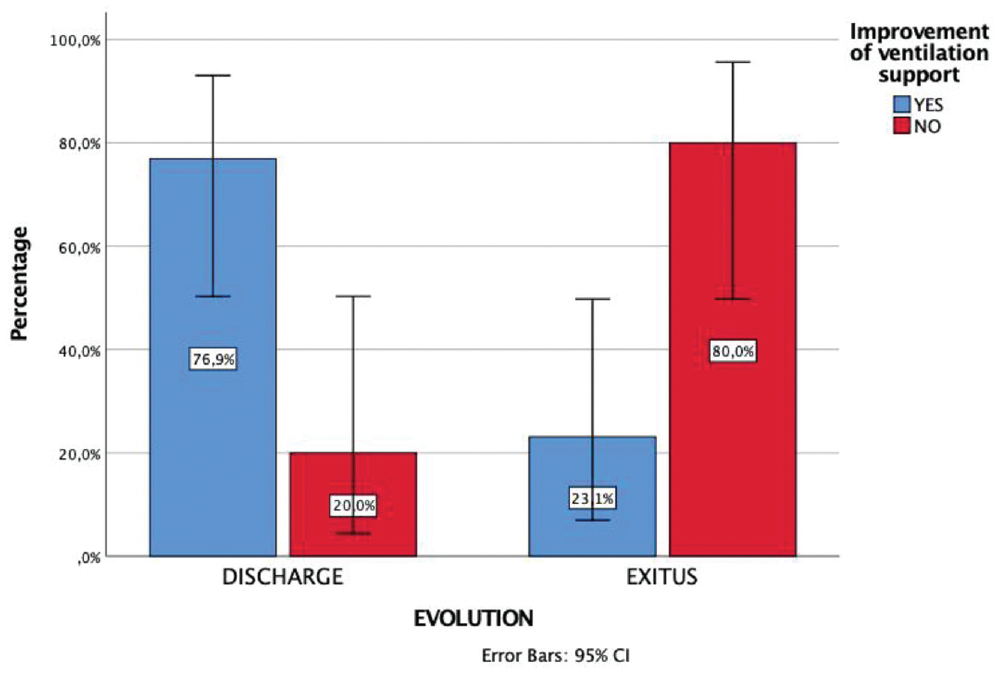
Box plot of the percentage of discharge and exitus in our population depending on the improvement of ventilation support. Most patients who lived had improved ventilation support in the 72 hours following the tracheostomy (P < .007). Values are presented as median, interquartile range, and 95% CI.
Discussion
We wish to highlight several important considerations arising from our results.
We found no differences in terms of medical personnel safety. Each otolaryngologist performing a tracheostomy, either open or percutaneous, had a negative RT-PCR result after the completion of the study, indicating that no contagion was produced. If every surgeon takes the necessary precaution measures, we cannot make bigger safety attributions to either technique.
Although both techniques were performed by experienced specialists in similar conditions at bedside in the intensive care unit, the mean time of the procedure was significantly lower when the tracheostomies were performed percutaneously. Those results are probably biased, mainly due to a more favorable anatomy previously identified for each surgical team. In our opinion, a reduction in the surgical time may be a great advantage, especially in this complex clinical scenario produced by the pandemic. Therefore, we consider the percutaneous tracheostomy a suitable technique when indicated. While the level of evidence from this small study is low, it represents the first systematic comparison of percutaneous versus open tracheostomy in the COVID-19 population to our knowledge.
We provide early tracheostomy for our patients instead of waiting >3 weeks as other authors propose. An earlier tracheostomy for patients with COVID-19 has potential advantages, such as better management of secretions, easier suctioning (in-line suction), improved patient comfort, weaning of heavy sedation, reduced duration of mechanical ventilator support requirement, and diminished stay in the intensive care unit. 7
In percutaneous and open tracheostomies, we follow the recommendations from the Critical Care and Acute Care Surgery Committees of the American Association for the Surgery of Trauma with minor modifications. 7 In percutaneous tracheostomy, we avoided the use of a bronchoscopy, with no observed complications. In open tracheostomy, we use electrocautery except for the skin incision and once the airway had been opened. We consider that the time saved on the procedure outweighs the risk of possible aerosolization of the virus in soft tissues.
Unfortunately, 41% of our population died within 7 days of the tracheostomy. These data far exceed the mortality rate usually found in percutaneous or conventional tracheostomies under normal conditions.8,9 With a small population and with binary outcome procedures, some statistical power is lost. However, our results suggest that the clinical condition is the key to understand such a high rate. The SOFA score, as a prior tracheostomy prognostic marker, was a good predictor for in-hospital mortality in patients with COVID-19 in our study, as also stated in a recent study. 10 In addition, the evolution of ventilation support might help clinicians determine a patient’s prognosis after the tracheostomy is made. Despite the results, more studies are needed to verify these facts due to the small sample size.