
Abstract
Objective
To investigate the prevalence of eustachian tube dysfunction (ETD) in elderly adults in the United States and its association with other upper aerodigestive inflammatory processes.
Study Design
Cross-sectional study.
Setting
Population based.
Subjects and Methods
In total, 147,805 patients without malignancy were compared to 13,804 demographically matched patients with malignancy of the upper aerodigestive tract (UADT) by querying the Surveillance, Epidemiology, and End Results (SEER)–Medicare linked database for patients aged 66 to 99 years between 2003 and 2011. The prevalence of ETD and inflammatory diseases among these patients was compared. Association between ETD, other upper aerodigestive inflammatory processes, and UADT malignancies was evaluated.
Results
The prevalence of ETD was 5.44% among patients without malignancy and 9.08% in those with cancer (odds ratio [OR], 1.73; 95% CI, 1.63-1.84). Patients with ETD in the control population were more likely (OR, 95% CI) to be diagnosed with chronic rhinitis (5.00, 4.70-5.33), chronic sinusitis (4.20, 3.98-4.43), allergic rhinitis (4.27, 4.08-4.47), and gastroesophageal reflux disease (GERD) (2.42, 2.31-2.53). Patients with ETD and chronic rhinitis (1.43, 1.24-1.65), chronic sinusitis (1.57, 1.38-1.78), and acute otitis media (1.33, 1.08-1.65) were associated with higher rates of UADT malignancy.
Conclusion
Over 5% of patients older than 65 in the United States are diagnosed with ETD in the absence of UADT malignancy. Associations between ETD and chronic rhinitis, chronic sinusitis, allergic rhinitis, and GERD in the absence of UADT malignancy suggest that some patients may benefit from treatment of inflammatory disease as a cause of ETD.
Eustachian tube dysfunction (ETD) is a common presenting complaint in general otolaryngology practice, accounting for over 2 million visits per year.1,2 ETD has been extensively studied in children but is not well defined in older populations.3-7 In adults, ETD can occur in isolation or in association with a number of inflammatory disorders of the aerodigestive tract, 8 although these associations remain incompletely characterized, particularly in the elderly population. Recent studies have suggested associations between chronic inflammatory conditions of the head and neck such as chronic sinusitis and gastroesophageal reflux and the development of malignancy of the upper aerodigestive tract (UADT).9-13 There is a perceived assumption that ETD in an elderly population is largely associated with the presence of UADT malignancy or a result of the treatments for UADT malignancy, but there are little data directly comparing these populations.
We conducted a population-based study of patients with and without UADT malignancies using a national database, for the purpose of evaluating the association between inflammatory disease processes and ETD. Specific aims were to (1) define the prevalence of ETD and other common inflammatory processes among patients with UADT malignancies compared to a control cohort, (2) describe the association between ETD and UADT malignancies, and (3) perform subgroup analysis stratified by sex, race, and age with respect to ETD when controlling for inflammatory conditions. To our knowledge, this is the first study to investigate ETD in the US elderly population while specifically controlling for the presence of UADT malignancy.
Methods
The National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER)–Medicare linked database was queried for this study. SEER is a cancer surveillance system consisting of population-based tumor registries designed to track cancer incidence and survival in the United States. It gathers data regarding demographics, incidence, and treatment information in geographically defined areas. The SEER database represents approximately 28% of the population of the United States. Medicare is the primary insurer for 97% of people in the United States aged 65 years or older.
The SEER-Medicare linked database was analyzed for cases diagnosed from January 2003 to December 2011 for cases under the “Oral Cavity and Pharynx” and “Other Respiratory System” cancer sites from the Patient Entitlement and Diagnosis Summary File (PEDSF), Medicare Provider Analysis and Review (MEDPAR), Carrier Claims (NCH), and Outpatient (OUTPT) databases. MEDPAR contains information about Part A services, containing 1 record per Medicare hospitalization; NCH contains information about Part B services with bills for services from physicians and other providers that occurred in the office or hospital. The OUTPT database also contains information about Part B services but contains Medicare outpatient claims, including diagnosis, procedure codes, and demographic information. The PEDSF database contains records for each individual in the SEER database matched with the patient’s Medicare enrollment record. This study was approved by the institutional review board of Ochsner Clinic Foundation as required by SEER-Medicare data use policy.
Study Cohort
The study cohort was limited to Medicare beneficiaries who were continuously enrolling in Part A and B non–health maintenance organization Medicare coverage at least 12 months prior to diagnosis. UADT malignancy cases included patients ages 66 to 99 years diagnosed with malignancies of the larynx, hypopharynx, oropharynx, tonsil, nasopharynx, and paranasal sinuses using the International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3) topology codes C09.0 to C11.9, C13.0 to C13.9, and C30.0 to C32.9 with morphology codes 8000 to 8576, 8940 to 8941. Study controls were obtained from a 5% random sample of Medicare beneficiaries, including both the Summarized Denominator File (SUMDENOM) and 5% PEDSF file who were living in the same SEER areas during some time point of SEER coverage as those diagnosed with UADT malignancy.
Variables
The entity of ETD in this study was defined collectively as coded diagnoses of ETD, otitis media with effusion (OME), or tympanic membrane retraction (TMR). Other upper aerodigestive inflammatory processes included rhinologic diagnoses (chronic rhinitis, chronic rhinosinusitis, and allergic rhinitis) and comorbid diagnosis (acute sinusitis, acute otitis media, upper respiratory tract infection, gastroesophageal reflux disease [GERD], and radiation therapy and related diagnoses). Table 1 lists the International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes for these conditions. Demographic variables used to examine the association of ETD with other upper aerodigestive inflammatory diseases were sex, race, age at diagnosis, and urban-rural location. Race was categorized as non-Hispanic whites (NHWs), non-Hispanic blacks (NHBs), or others, which include Asian/Pacific Islanders, Hispanics, American Indians, and Alaskan natives. Urban-rural location was defined based on state county level and categorized into metropolitan and nonmetropolitan areas.
Prevalence by Diagnosis Among Upper Aerodigestive Tract Cancer and Control Medicare Participants Aged 66 to 99 Years.

Abbreviations: ETD, eustachian tube dysfunction; GERD, gastroesophageal reflux disease; ICD-9, International Classification of Diseases, Ninth Revision; OME, otitis media with effusion; TMR, tympanic membrane retraction.
Statistical Analyses
Prevalence of ETD and other upper aerodigestive inflammatory conditions was estimated for UADT malignancy patients and control patients. Control patients were weighted 20 times when estimating the prevalence as these were derived from a 5% random sample of the entire source population. Logistic regression was used to assess the association between ETD and other upper aerodigestive inflammatory conditions among control patients and between UADT malignancies and inflammatory conditions. The associations between patients’ demographic factors and UADT malignancies by inflammatory condition were examined as well. Odds ratios were determined and reported for all associations and the phi coefficient computed to assess the effect size for each association. SAS version 9.4 (SAS Institute) was used to carry out all statistical analyses, and tests were conducted at the .05 significance level.
Results
A total of 13,805 patients in the United States aged 65 to 99 years were diagnosed with cancer of the UADT between 2003 and 2011 and compared to a control population of 147,884 patients. Prevalence data for ETD and other inflammatory conditions were calculated for both ( Table 1 ). The prevalence of ETD was 9.1% in the cancer population and 5.4% in the control group. The overall prevalence of ETD was 5.5% in the entire population. In the cancer population, the prevalence of chronic rhinitis (10.8%) and chronic sinusitis (15.7%) was higher than in the control population (4.9% and 8.9%, respectively).
Within the noncancer population, patients with ETD had greater odds (odds ratio [OR], 95% CI) of being diagnosed with chronic rhinitis (5.00, 4.69-5.32), chronic sinusitis (4.20, 3.98-4.43), allergic rhinitis (4.27, 4.09-4.48), and GERD (2.42, 2.31-2.53) ( Table 2 ).
Association Between ETD and Other Upper Aerodigestive Inflammatory Conditions Among 147,884 Patients in Control Population, Years 2003-2011.
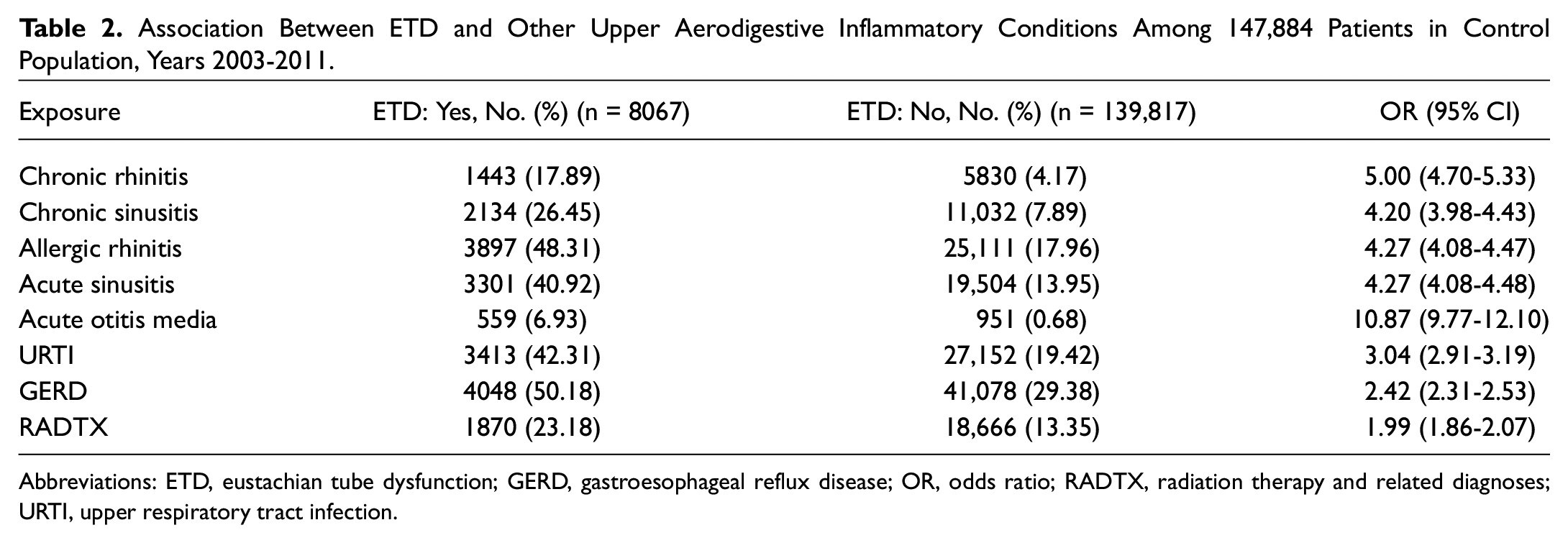
Abbreviations: ETD, eustachian tube dysfunction; GERD, gastroesophageal reflux disease; OR, odds ratio; RADTX, radiation therapy and related diagnoses; URTI, upper respiratory tract infection.
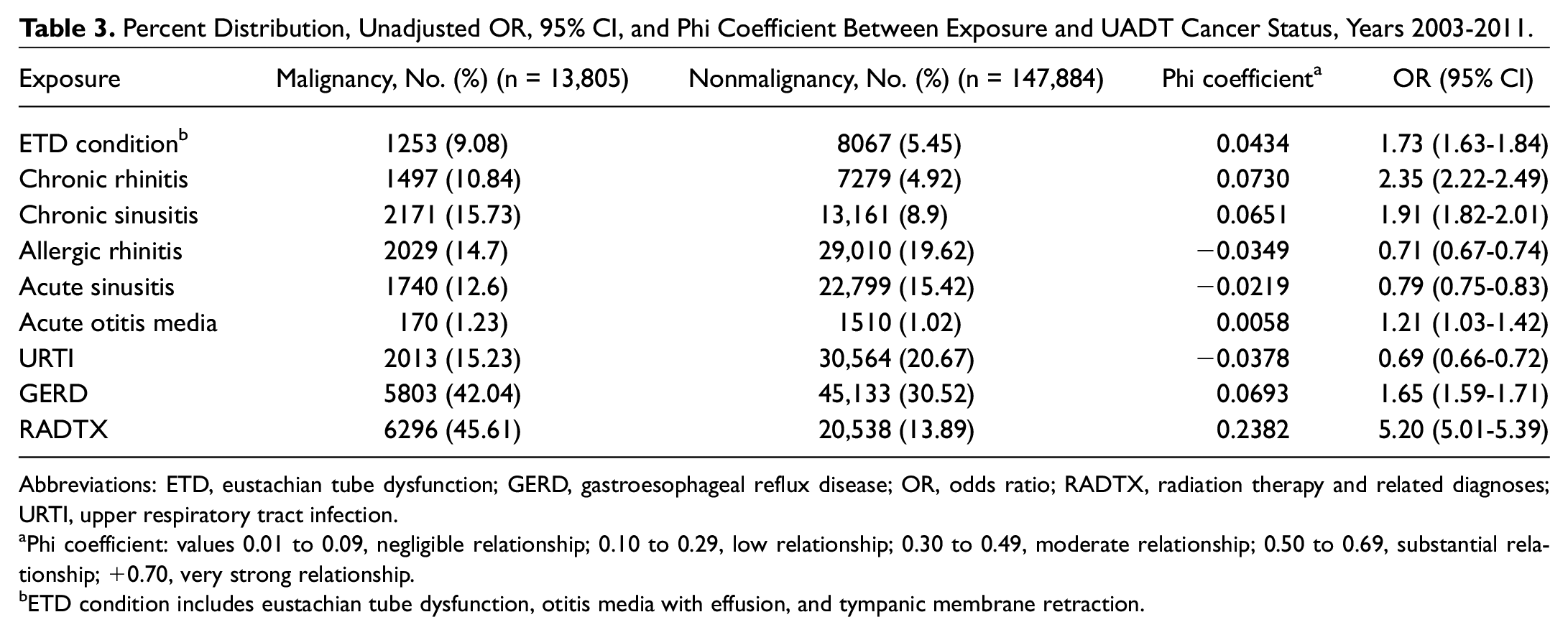
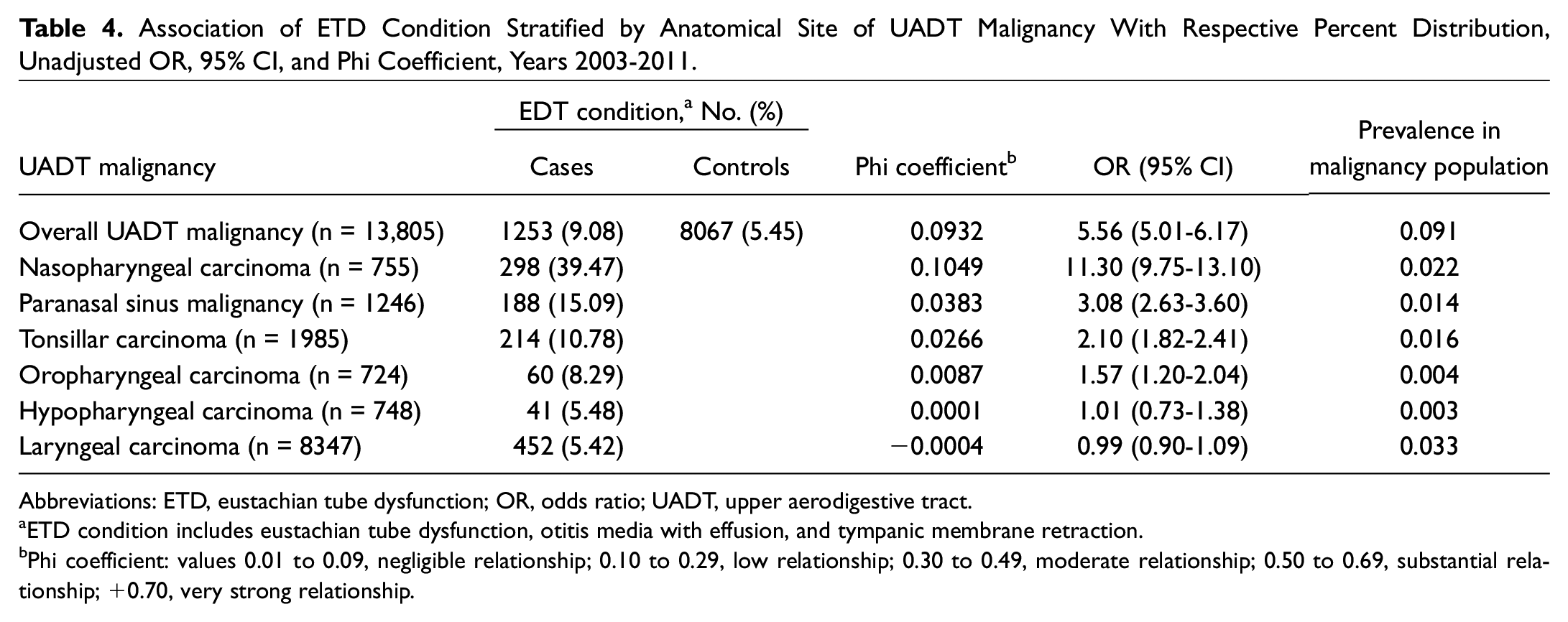
Patients with an UADT malignancy had greater odds of being diagnosed with ETD when compared to the control population (1.73, 1.63-1.84; Table 3 ). Similar associations were noted among the patients with rhinologic clinical diagnoses. Chronic rhinitis (2.35, 2.22-2.49) and chronic sinusitis (1.91, 1.82-2.01) demonstrated increased odds of diagnosis in the UADT malignancy population when compared to the control population. Patients with a malignancy of the nasopharynx (11.30, 9.75-13.10), paranasal sinuses (3.08, 2.63-3.60), tonsils (2.10, 1.82-2.41), and oropharynx (1.57, 1.20-2.04) demonstrated a stronger association with ETD diagnosis than hypopharyngeal (1.01, 0.73-1.38) and laryngeal carcinoma (0.99, 0.90-1.09; Table 4 ).
Percent Distribution, Unadjusted OR, 95% CI, and Phi Coefficient Between Exposure and UADT Cancer Status, Years 2003-2011.
Abbreviations: ETD, eustachian tube dysfunction; GERD, gastroesophageal reflux disease; OR, odds ratio; RADTX, radiation therapy and related diagnoses; URTI, upper respiratory tract infection.
Phi coefficient: values 0.01 to 0.09, negligible relationship; 0.10 to 0.29, low relationship; 0.30 to 0.49, moderate relationship; 0.50 to 0.69, substantial relationship; +0.70, very strong relationship.
ETD condition includes eustachian tube dysfunction, otitis media with effusion, and tympanic membrane retraction.
Association of ETD Condition Stratified by Anatomical Site of UADT Malignancy With Respective Percent Distribution, Unadjusted OR, 95% CI, and Phi Coefficient, Years 2003-2011.
Abbreviations: ETD, eustachian tube dysfunction; OR, odds ratio; UADT, upper aerodigestive tract.
ETD condition includes eustachian tube dysfunction, otitis media with effusion, and tympanic membrane retraction.
Phi coefficient: values 0.01 to 0.09, negligible relationship; 0.10 to 0.29, low relationship; 0.30 to 0.49, moderate relationship; 0.50 to 0.69, substantial relationship; +0.70, very strong relationship.
An association between male sex and diagnosis of malignancy across all inflammatory disorders was identified, accounting for 68% of the cancer population compared to 36% in the control ( Table 5 ). Non-Hispanic whites accounted for over 80% of patients in cancer and control groups. Non-Hispanic blacks demonstrated a slightly higher prevalence of malignancy in the setting of chronic rhinitis, chronic sinusitis, allergic rhinitis, and GERD. When compared to patients aged 66 to 69 years, patients older than 70 years diagnosed with all inflammatory conditions demonstrated an association with malignancy. Stratified analysis by age demonstrated the diagnosis of ETD, OME, and TMR had increased associations with UADT malignancy after adjusting for other demographics. The greatest association was noted between the ages of 75 and 79 years with an odds ratio of 9.09 (95% CI, 7.51-10.99).
Percent Distribution, Adjusted OR, 95% CI, and Phi Coefficient for Demographic and UADT Cancer Status for Each Exposure. a
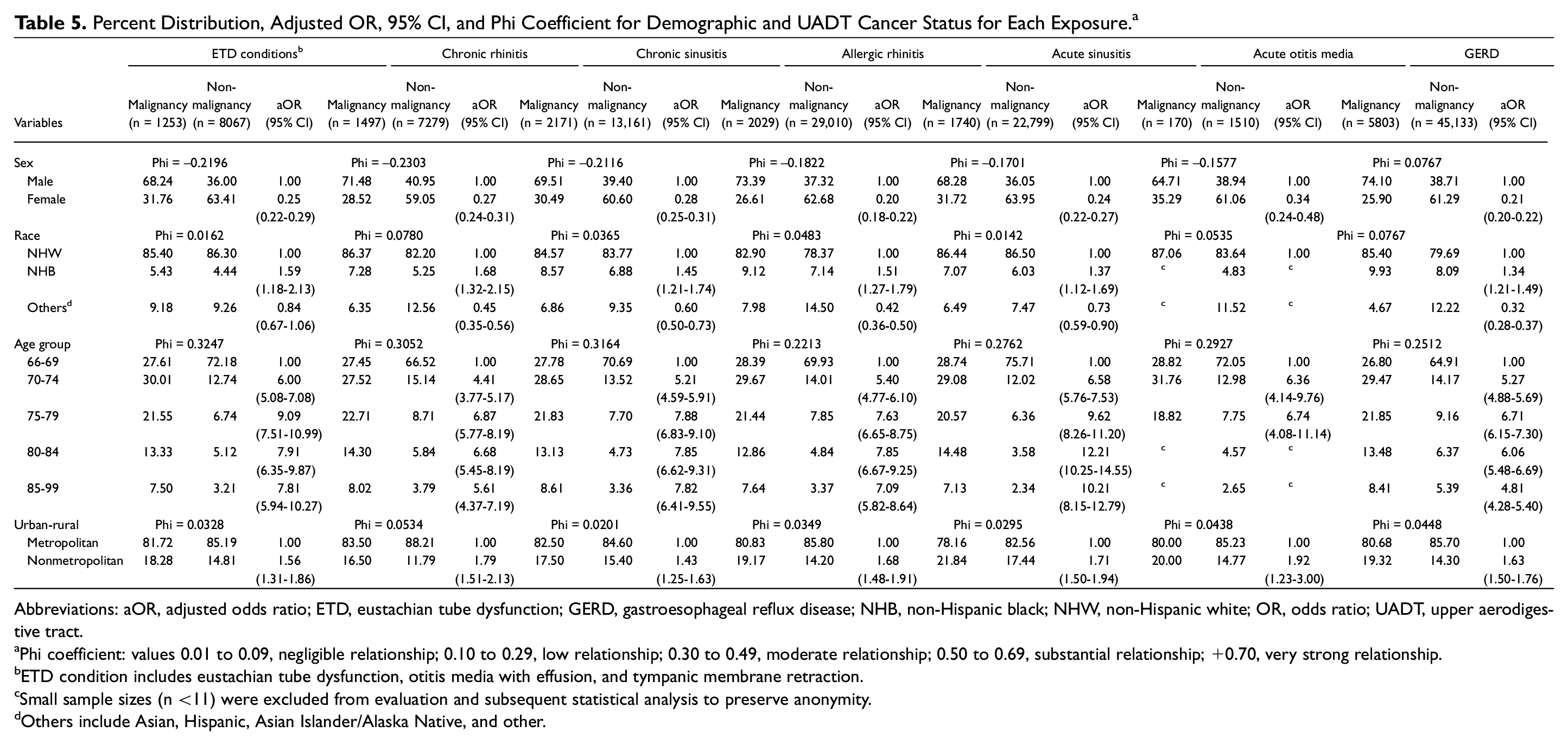
Abbreviations: aOR, adjusted odds ratio; ETD, eustachian tube dysfunction; GERD, gastroesophageal reflux disease; NHB, non-Hispanic black; NHW, non-Hispanic white; OR, odds ratio; UADT, upper aerodigestive tract.
Phi coefficient: values 0.01 to 0.09, negligible relationship; 0.10 to 0.29, low relationship; 0.30 to 0.49, moderate relationship; 0.50 to 0.69, substantial relationship; +0.70, very strong relationship.
ETD condition includes eustachian tube dysfunction, otitis media with effusion, and tympanic membrane retraction.
Small sample sizes (n <11) were excluded from evaluation and subsequent statistical analysis to preserve anonymity.
Others include Asian, Hispanic, Asian Islander/Alaska Native, and other.
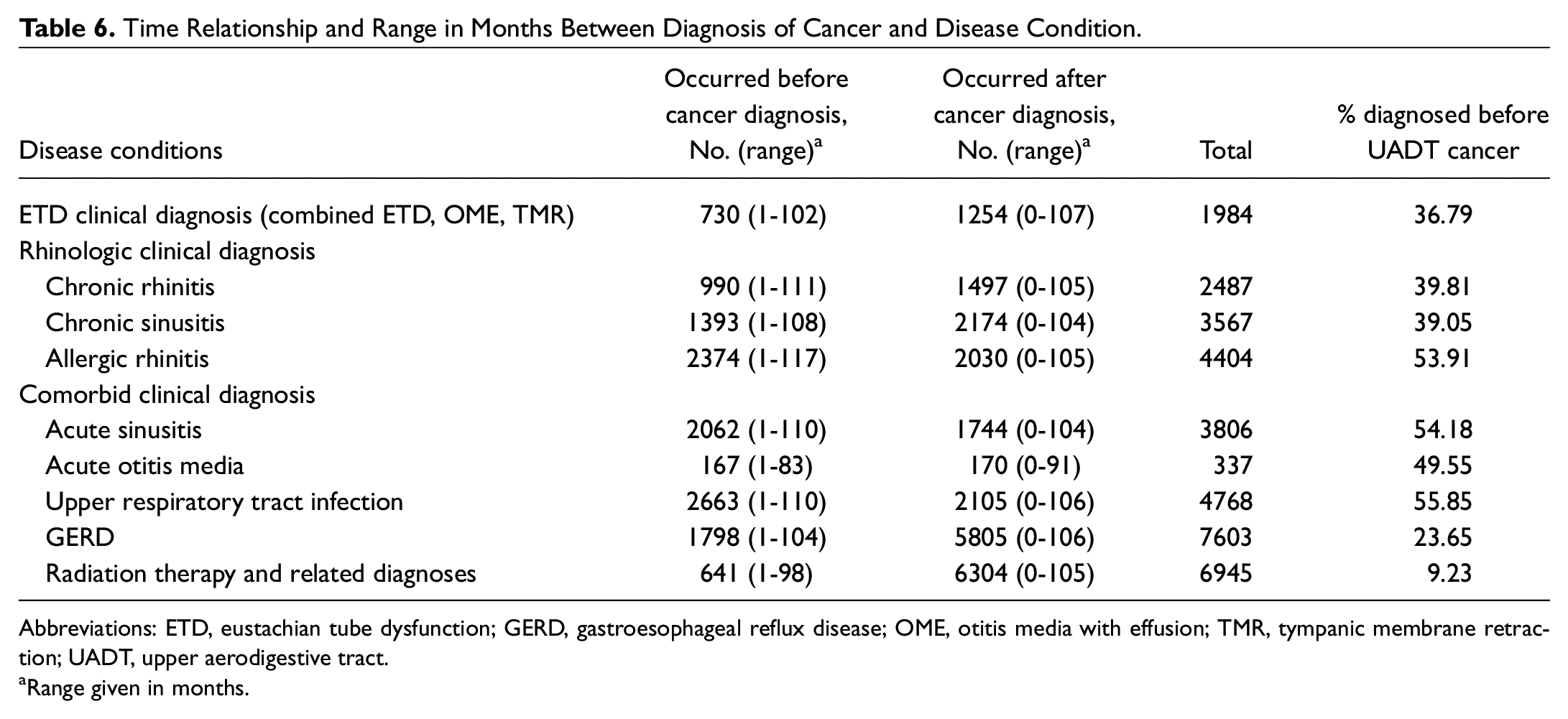
Patients with radiation exposure were more likely to have been diagnosed with a UADT malignancy (5.20, 5.01-5.39). Given that one of the mainstays of therapy for head and neck malignancy is radiotherapy and that multiple comorbid conditions can occur secondarily to radiation therapy, an analysis was performed demonstrating the temporal association between diagnosis of UADT malignancy and diagnosis of exposure disease conditions. Among patients with a UADT malignancy, 36.8% were diagnosed with ETD prior to cancer diagnosis ( Table 6 ). Similar results were calculated for chronic rhinitis, chronic sinusitis, and GERD. Among patients with allergic rhinitis, acute sinusitis, acute otitis media, and URTI, approximately half of the patients had disease prior to cancer diagnosis.
Time Relationship and Range in Months Between Diagnosis of Cancer and Disease Condition.
Abbreviations: ETD, eustachian tube dysfunction; GERD, gastroesophageal reflux disease; OME, otitis media with effusion; TMR, tympanic membrane retraction; UADT, upper aerodigestive tract.
Range given in months.
Discussion
This population-based study is the first to examine the prevalence of ETD in the US elderly population with various comorbid conditions with and without UADT malignancies. In the noncancer population, the prevalence of ETD was 5.4%, compared to 9.1% in patients diagnosed with a UADT malignancy. Patients with UADT cancer had greater odds of having ETD when compared to the noncancer population. The association between ETD, other chronic conditions, and UADT cancers varied by sex, race, and sex.
The increased prevalence of ETD in patients with UADT malignancy was an anticipated finding of this study. The occurrence of ETD as a symptom of nasopharyngeal carcinoma is well known, with a reported 40% of patients with that malignancy demonstrating middle ear effusion prior to radiotherapy. 14 The presence of unilateral otitis media is an indication for direct evaluation of the nasopharynx to rule out a neoplasm. 15 In our study, ETD was 1.73 (95% CI, 1.63-1.84) times more likely to be diagnosed in the UADT malignancy population when compared to a control population. When examining the UADT malignancy population by anatomical subsite, there was an anticipated association between proximity of neoplasm to the eustachian tube and presence of ETD. ETD was noted to be far more prevalent in the nasopharyngeal and paranasal sinus carcinoma populations with 39.47% and 15.09% affected, respectively. This association decreased in strength with laryngeal carcinoma demonstrating ETD in 5.42% of patients, approximating that of the general elderly population.
We found that a large portion of ETD patients with UADT malignancy had undergone previous radiotherapy. Although the data obtained from the SEER database do not fully account for the location to which radiation is administered, we found that only 9% of patients in our cohort had received radiation prior to their diagnosis of UADT malignancy. Radiation therapy is known to contribute to ETD, with inflammation and tubal obstruction worst at 6 months posttherapy and improving at 5 years after radiotherapy, with higher doses portending a worse prognosis for recovery.16,17 Our patient population demonstrated the prevalence of ETD at 36.8%, ranging from 1 to 102 months prior to their cancer diagnosis, compared to 4.0% in the general population. The association between ETD and radiation therapy also explains the noted association with ETD and various malignancies when stratified by anatomical subsite, as those malignancies closer to the eustachian tube are more likely directly affected by radiotherapy.
The perceived assumption is that most ETD in the US elderly population is related to the diagnosis and treatment of UADT malignancy. This was an expected and anticipated conclusion of our study that we feel is broadly accepted by the otolaryngology community. Where these results become important is in direct contrast with the control population. While there is a higher prevalence of ETD malignancy in the UADT cancer population, most elderly patients with ETD do not carry a diagnosis of UADT malignancy, and in fact, a large proportion have other comorbid inflammatory conditions that we feel have been incompletely characterized. The prevalence of ETD in the noncancer population has important clinical and epidemiological implications, particularly as new treatments are introduced for the management of ETD of benign origin.
In a previous population-based study examining the National Ambulatory Medical Care Survey data, authors determined 2.03 million adult visits per year for ETD and related diagnoses, compared to 2.63 million visits per year in children for similar diagnoses. Among the subgroup analysis of these populations, only 29.6% of adult visits were attributable to an elderly population. 1 A study of the British population identified that among a sample of 2708 patients who underwent otolaryngology and audiology evaluation, 4.1% of adults aged 18 to 80 years demonstrated chronic otitis media, with patients aged 61 to 80 years being twice as likely as those aged 18 to 40 years to have chronic otitis media. 18 This study demonstrated a similar prevalence of ETD in the adult population when compared to our study. A recent study of patients in a US population determined a prevalence of 4.6% based on tympanometry alone in the absence of symptoms. 19
When performing a subgroup analysis of our noncancer population, there was a 4- to 5-fold greater odds of having chronic rhinitis, chronic sinusitis, and allergic rhinitis in patients with ETD, which may contribute to a portion of the control population being diagnosed with ETD. In the United States, the prevalence of chronic sinusitis is estimated to range between 2% and 16%, with a global prevalence estimated to be between 7% and 27% with a broad variation based on country.20-22 Only 1 study stratifies significantly by age, demonstrating a prevalence of 4.7% in patients over age 60 years. 20 Multiple prospective studies have hypothesized that since the respiratory mucosa of the paranasal sinuses and nasal cavity also lines the eustachian tube, a process affecting one area may result in ETD.23,24 Prospective survey-based studies have demonstrated that in patients with known chronic sinusitis, a significant portion of patients will also report symptoms consistent with ETD when compared to the general population. 23 Another study demonstrated that the treatment of chronic sinusitis will result in significant reductions in symptomatic ETD that correspond with improvements in nasal symptoms. 24 This suggests the importance of treating underlying inflammatory conditions of the head and neck, which may in turn address coincident ETD.
An additional item of interest is the association between ETD and GERD. We demonstrated that patients with ETD were 2.4 times more likely to be diagnosed with GERD than the general population. There are limited data evaluating the association between GERD and ETD in an adult population. A single adult study identified a significantly higher number of reflux events in the nasopharynx of patients with ETD and GERD, but this did not result in a significant change in pH when compared to a control population without ETD. 25 Animal models have demonstrated that inflammation secondary to exposure to pepsin and hydrochloric acid resulted in ETD secondary to impaired mucociliary clearance of middle ear contents.26,27 Additional study is necessary to better evaluate this association.
In 2019, the American Academy of Otolaryngology–Head and Neck Surgery released a clinical consensus statement regarding balloon dilation of the eustachian tube. 28 In this statement, they emphasized the need to treat possible comorbid allergic rhinitis, rhinosinusitis, and laryngopharyngeal reflux that may be contributing to patient symptomatology. This statement was based on a systematic analysis out of the United Kingdom that looked specifically at the etiology of otitis media with effusion in adults and specific pathological processes. 29 This study did not detail the prevalence or overall burden of these comorbid conditions in patients with ETD. The clinical consensus statement also details the need for nasal endoscopy to evaluate candidacy for ETD interventions rather than reliance on patient symptoms. An additional benefit of nasal endoscopy would be to aid in diagnosis of chronic rhinosinusitis, allergic rhinitis, or GERD that we have demonstrated are common comorbid inflammatory conditions.
The strengths of this study include its large sample size, population-based design, and use of validated cancer outcomes from the SEER cancer registries. Patients also were well matched for demographic information, geographic location, year of diagnosis, and comorbid diseases. As such, the results of this study are generalizable to the elderly population of the United States.
There are multiple limitations to this study. The data obtained from SEER-Medicare linked databases have inherent biases. The diagnosis of ETD is a clinical diagnosis without universally accepted diagnostic criteria. There is a single validated clinical assessment in the Eustachian Tube Dysfunction Questionnaire–7 (ETDQ-7), 30 but this has not been adopted on a national level as a requirement in the diagnosis of ETD. Resultantly, in a national database study, it is impossible to ascertain the diagnostic criteria applied to individual patients who have been included in the study. Laterality is not encoded in this database, and so unilateral vs bilateral ETD is not defined in this population. It is unknown if the initial symptoms of malignancy of the UADT were misdiagnosed as another sinonasal inflammatory disorder (ie, nasal congestion from neoplasm being diagnosed as chronic sinusitis or missed neoplasm in the setting of unilateral OME). In addition, it is difficult to determine the means by which many inflammatory disorders of the sinonasal tract were diagnosed. Diagnoses may have been made based on symptoms, invasive testing, or endoscopic examination, with interprovider variability. For ETD and all comorbid disorders, there was a noted tendency toward diagnosis of these disorders only after the diagnosis of a UADT cancer. This could be secondary to radiotherapy or cancer as independent risk factors for developing these disease processes but could also be secondary to surveillance bias that may have resulted in the diagnosis of more indolent processes or increased awareness of existing sinonasal complaints in patients who were recently diagnosed with a UADT cancer.
Other limitations of the SEER-Medicare database are well established. There are no data in this research study regarding the use of tobacco or alcohol, well-documented risk factors for UADT malignancy. Tobacco is an independent risk factor in the development of ETD, chronic rhinitis, and chronic sinusitis, as well as believed to be a factor in the development of head and neck cancers.31-33 Findings from this database are only capable of suggesting associations and correlations between inflammatory processes and the possible relationship to the development of UADT cancers. Causality cannot be established based on this study alone. Future study should include long-term prospective evaluation and possible head and neck screening recommendations.
Conclusion
Over 5% of patients older than 65 in the United States are diagnosed with ETD in the absence of UADT malignancy. Associations between ETD and chronic rhinitis, chronic sinusitis, allergic rhinitis, and GERD suggest that some of these patients may benefit from treatment of inflammatory disease as a contributor to ETD. Higher rates of ETD are present in the head and neck cancer population compared to the noncancer population.
Footnotes
There are no commercial or financial grant/assistance/disclosures declarations associated with this publication. The views expressed in this manuscript are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of the Air Force, Department of Defense, or the US government.