
Abstract
Objectives
The role of vitamin D deficiency has been linked with recurrent upper respiratory tract infections, but its impact on the frequency of tonsillitis is not yet fully understood. The objective of this study is to determine the association between vitamin D deficiency and recurrent tonsillitis based on current literature.
Data Source
A systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. Data were collected from online medical databases (PubMed, MEDLINE, EMBASE, and Cochrane Collaboration Registry of Controlled Trials).
Review Methods
All studies addressing the association of vitamin D deficiency and recurrent tonsillitis prior to March 2019. The data were collected in different phases: screening review using search words and controlled vocabularies followed by detailed review of screened articles based on inclusion and exclusion criteria, then a full review that included screening the references of selected articles.
Results
Fifty-three studies were potentially eligible; of these, 4 publications met the inclusion criteria and were included in the quantitative synthesis. There was a statistically significant reduction of vitamin D levels in patients with recurrent tonsillitis as compared to healthy controls (mean difference, −10.71; 95% CI, −19.12 to −2.31; P = .01). The odds of vitamin D insufficiency were significantly higher in patients with recurrent tonsillitis as compared to the control group (odds ratio, 4.37; 95% CI, 2.78-6.88; P < .001).
Conclusion
Vitamin D deficiency was present in patients with recurrent tonsillitis and might be associated with an increase in the risk of recurrent tonsillitis. There is a need to explore these findings via clinical trials based on large populations.
Tonsillopharyngitis is considered one of the major causes of outpatient visits in the United States. 1 It is defined as an inflammation of the tonsils, characterized by signs of erythema and exudate with or without abscess formation. Recurrent tonsillitis is defined as, according to Paradise et al, 2 at least 7 episodes in a year, or a minimum of 5 episodes in a year for 2 consecutive years, or at least 3 episodes in a year for 3 consecutive years. It is commonly caused by viral infection, but group A β-hemolytic accounts for 5% to 17% of cases.3,4 It poses a major concern in terms of repeated antibiotic usage.
Although several theories explain the frequent attacks of tonsillitis, the exact etiology of this phenomenon is still unclear. The immune system, environmental factors, and maltreatment of the acute attack all play a role in the recurrent attack of disease. Moreover, it has been linked to being deprived of sunlight during the winter, which results in inadequate synthesis of vitamin D in the human body during that particular season. 5 Besides, incidents of upper respiratory tract infection (URTIs) are inversely related to sun exposure, as reported in some studies.6-8
Vitamin D in its hydroxylated form has an impact on the immune system. It has many effects on immune cells, including B and T lymphocytes. 9 It is considered an immunomodulator of both innate and adaptive immunity, as it is responsible for transforming T helper cells toward Th2 status. Moreover, 25-hydroxvitamin D plays a significant role in the induction of antimicrobial peptides (defensins and cathelicidin) when bacterial or viral pathogens are recognized by the immune cells.6,10-12
In addition, vitamin D receptor (VDR) is enormously expressed in different cells types, including immune and respiratory tract cells. 1,25-Hydroxy vitamin D ligates with these receptors to induce a wide spectrum of antimicrobial responses against bacterial and viral respiratory agents.13,14 Morphologically, there is an inverse relationship between vitamin D levels and the size of the tonsil. 15
Besides its effect on bone metabolism and calcium hemostasis, it is well established that there is a consistent association between low levels of 25-hydroxvitamin D and the risk of respiratory tract infection, as evident from both observational and experimental studies.16-20 Literature has linked recurrent URTIs with vitamin D deficiency. In 2011, Reid et al 15 reported that 78% of the pediatric age group who underwent tonsillectomies in Auckland, New Zealand, had 25(OH) vitamin D levels below 75 nmol/L. Another case-controlled study in Turkey elaborated that vitamin D insufficiency was significantly more prevalent in children with recurrent tonsillitis (18% vs 0% in the control group). 21 Low vitamin D levels have also been found in children with a history of recurrent tonsillar infections and allergic rhinitis. 22 Specifically, decreased vitamin D levels were associated with a higher risk of recurrent group A streptococcal tonsillopharyngitis in adults, as observed by Nseir et al. 23
Moreover, a systematic review of randomized controlled trials conclusively indicated that vitamin D supplementation provided a protective effect on acute respiratory tract infections. It also indicated that those with vitamin D levels >25 nmol/L experience a higher level of protection from acute URTIs. 24 However, only a few observational studies have explained the association of vitamin D and recurrent tonsillitis.5,21,23,25 Therefore, we conducted the current systematic review to determine potential associations between vitamin D levels and recurrent episodes of the disease.
Methods
Protocol and Registration
The protocol of the current study is registered at PROSPERO, International Prospective Register of Systematic Reviews (No. CRD42018090199). The study received exemption from the institutional review board.
Search Strategy and Study Selection
We performed a comprehensive search of MEDLINE, PubMed, EMBASE, and the Cochrane Collaboration Registry of Controlled Trials for studies published from inception to February 2019 using a comprehensive search strategy (Appendix 1 in the online version of the article). We used terms related to vitamin D and tonsillitis in all the databases without any restrictions on publication type, language, date, age, sex, ethnic origin, baseline of vitamin D status, or any comorbidities. Afterward, reference lists of the identified studies were screened for potentially relevant studies. Relevant articles were retrieved, and abstracts were screened for eligibility according to the inclusion criteria. If a particular study met the inclusion criteria, a full text was assessed.
All eligible studies were screened by 2 of the authors independently (A.A.M. and A.A.A.). A discussion between all authors (A.A.M., A.A.A., T.A., H.M., F.Z.) was made if any disagreement had been raised. Manuscript preparation and review were performed by all authors.
Eligibility Criteria of Quantitative Analysis
According to predetermined criteria, studies were either included or excluded from the quantitative analysis.
i.
ii.
Study Measures
Serum 25-hydroxyvitamin D, also known as calcifediol or calcidiol, was considered the standard measure in our analysis. This parameter was reported in ng/mL, but in cases where mmol/L was given, we converted the value by multiplying by 0.4.
Data Extraction and Quality Assessment
Data extracted using a standardized data extraction tool were retrieved by the first author (A.A.M.) and checked by the second (A.A.A.). The senior author (F.Z.) oversaw the methodology of data extraction and analysis. The extracted data were study design, first author, year of publication, study setting, age of participants, total number of participants, serum vitamin D level, and vitamin D status. Detailed information regarding the outcomes of interest was tabulated for subsequent analysis. The Newcastle-Ottawa Scale (NOS) 26 and a customized version of NOS 27 were used to assess the quality and risk of bias of the case-controlled and cross-sectional studies, respectively.
Statistical and Meta-analyses
The heterogeneity was assessed by the I2 statistic and χ2 test; statistical significance of heterogeneity was defined as a P value >.05. We investigated the association between vitamin D levels and recurrent tonsillitis on the basis of events that occurred in each group and mean ± SD. Mean difference (MD) and odds ratio (OR) were the measure of estimates in our analysis, whereas the corresponding 95% CIs were the measure of the precision of the given estimate. Continuous variable (vitamin D level) was analyzed by MD with 95% CI based on the random-effect model. Vitamin D insufficiency/deficiency was defined as a vitamin D level below 30 ng/mL. The summary OR with 95% CI was used to evaluate the effect of vitamin D status (deficiency/insufficiency) on the risk of recurrent tonsillitis based on the fixed-effect model. The individual OR was obtained from each individual study, if being provided; otherwise, OR was calculated based on the occurrence of abnormal vitamin D status (deficiency/insufficiency) in the recurrent tonsillitis group vs the healthy group. A P value less than .05 was considered statistically significant for summary results. Statistical analysis was conducted using Review Manager (RevMan) version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration). Potential risk of publication bias was assessed through visual inspection of funnel plot asymmetry and quantitively estimated by Egger’s test using comprehensive meta-analysis software v3 (Comprehensive Meta-Analysis Package, Version 3.3.070, 2014, Biostat).
Results
Identification and Selection of Studies
A total of 53 publications were identified, and after duplications were removed and title and abstract screened, 8 studies were subjected to a full-text screening. Among the relevant 8 articles, 6 studies fulfilled the criteria for inclusion. While 6 studies were included in this systematic review, a subset of 4 studies was selected in the final meta-analysis, after an in-depth review of the included studies ( Figure 1 ).5,21,23,25
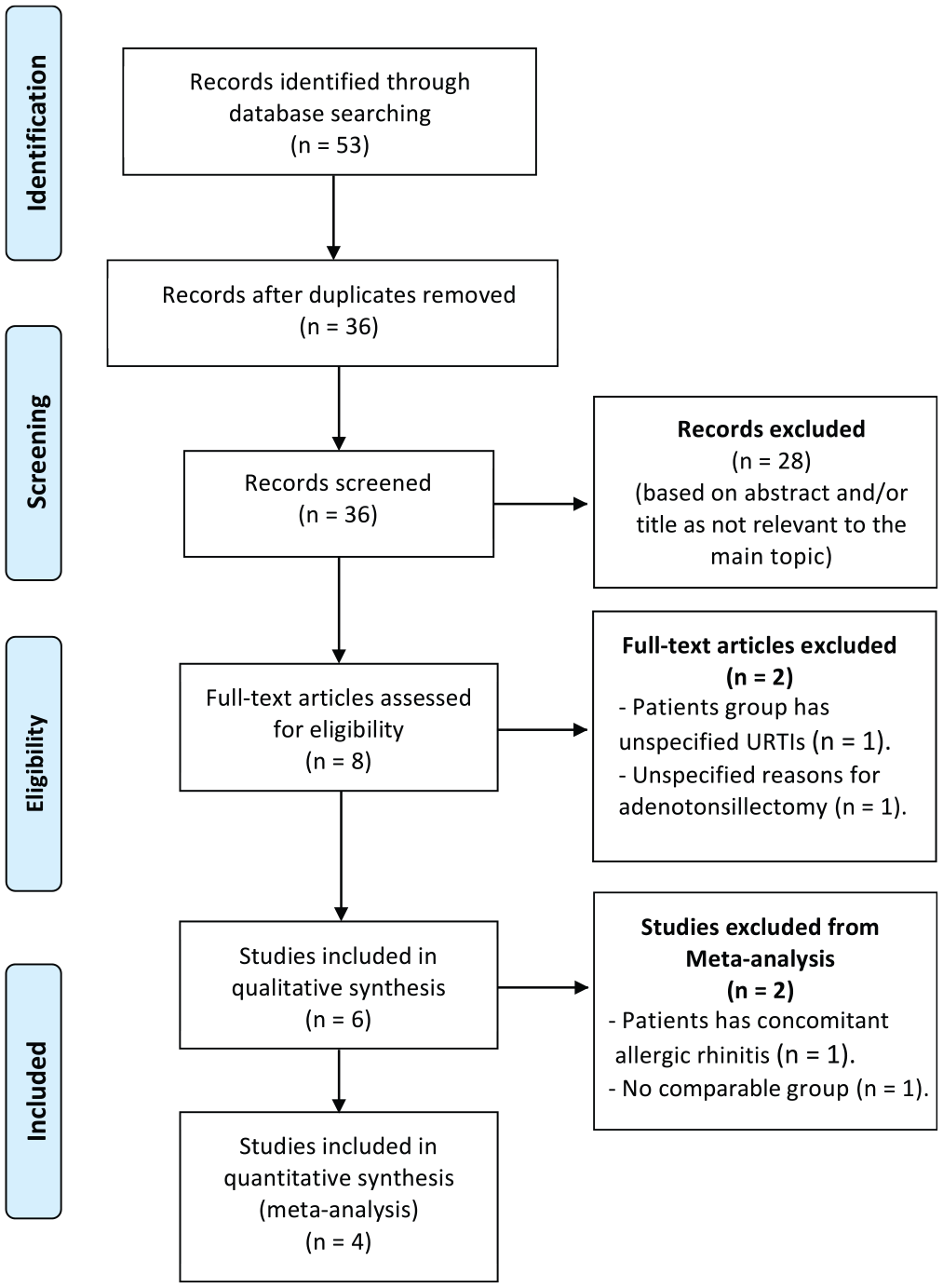
Flowchart depicting the method of study selection.
Study Characteristics and Quality
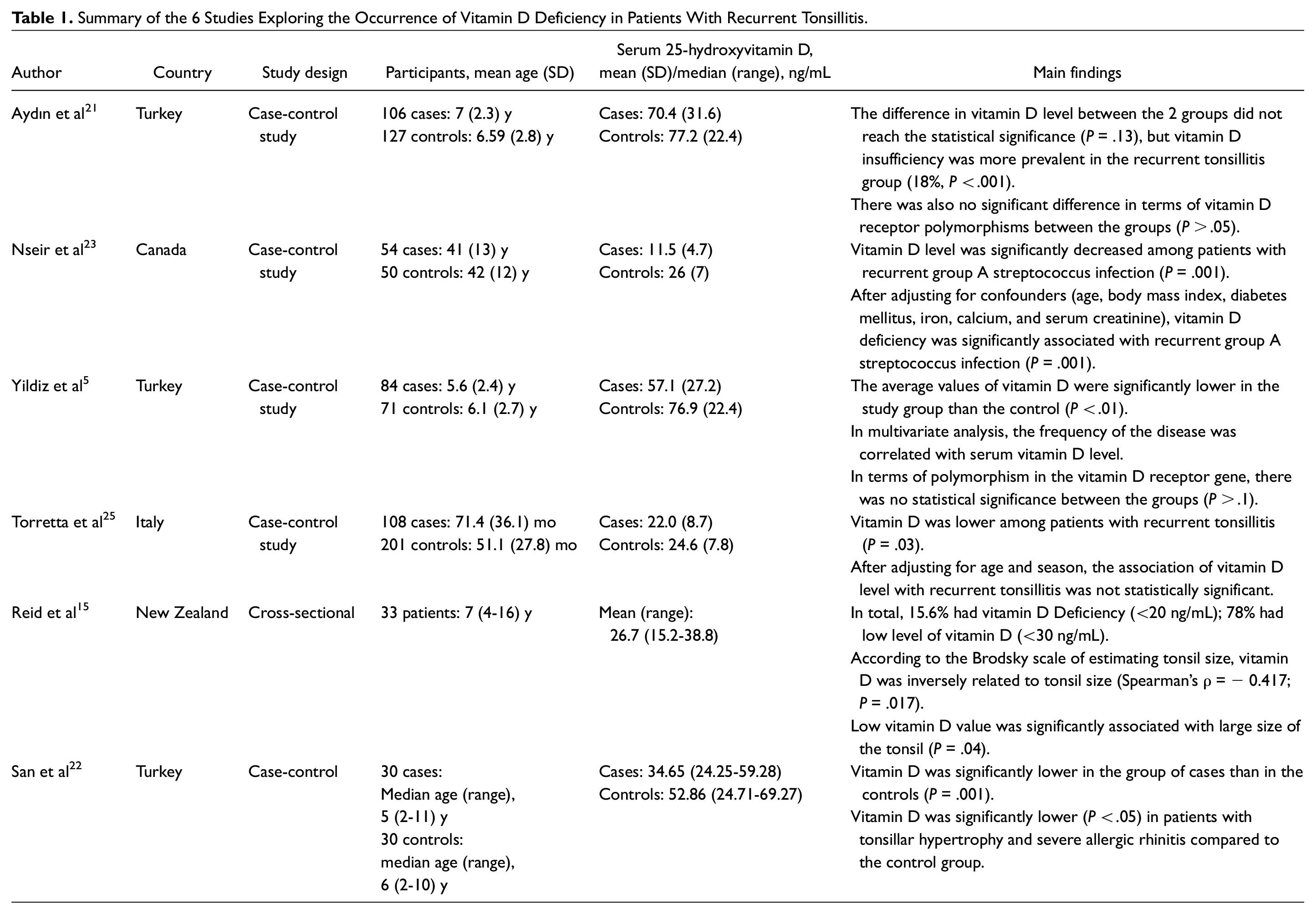
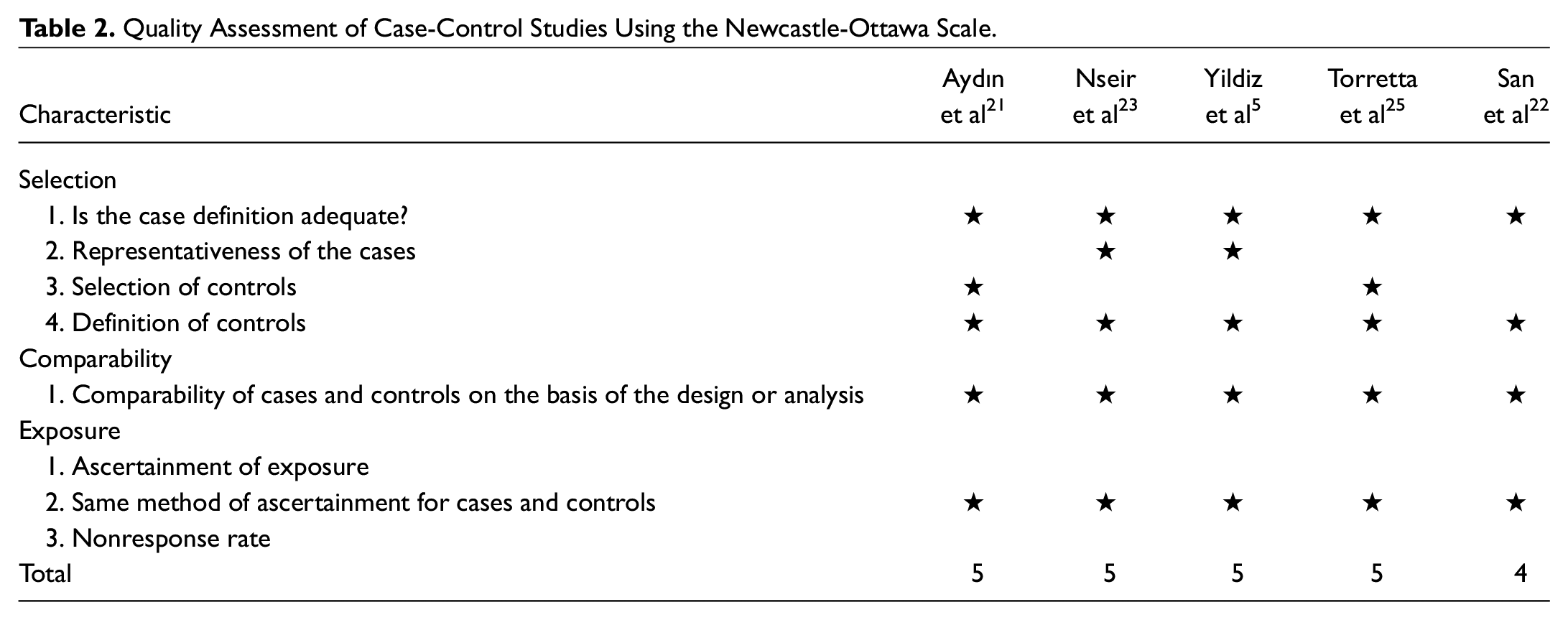
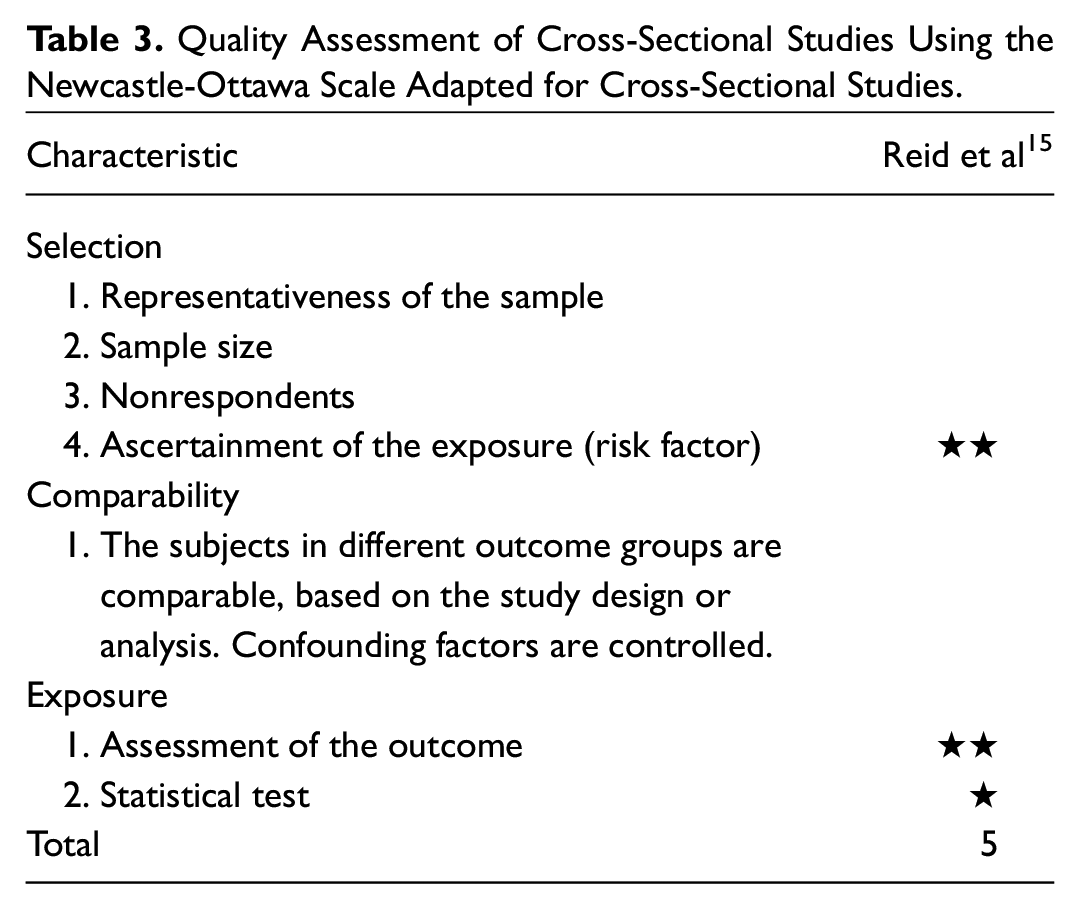
The 6 selected studies were conducted in different parts of the world; 3 were in Turkey, 1 was in Canada, 1 was in Italy, and 1 was in New Zealand. All 6 studies were written in English. All of them were observational studies and none were randomized controlled studies. Five of the studies were case-controlled, and one was a cross-sectional study design. Five of the 6 were conducted retrospectively, while only 1 was a longitudinal study. A total of 329 patients and 393 healthy individuals were included in the meta-analysis ( Table 1 ). With respect to study quality, all studies were graded as “intermediate quality” ( Tables 2 and 3 ).
Summary of the 6 Studies Exploring the Occurrence of Vitamin D Deficiency in Patients With Recurrent Tonsillitis.
Quality Assessment of Case-Control Studies Using the Newcastle-Ottawa Scale.
Quality Assessment of Cross-Sectional Studies Using the Newcastle-Ottawa Scale Adapted for Cross-Sectional Studies.
Study Findings
All reviewed studies reported that patients with recurrent tonsillitis had lower vitamin D levels when compared with the control group.5,15,21-23,25 Yildiz et al 5 found that the level of vitamin D was negatively associated with the frequency of tonsillitis. In summary, the pooled MD indicated that there was a significant reduction in vitamin D levels among patients with recurrent tonsillitis when compared to the control groups, under a random-effect statistical model (MD, −10.71; 95% CI, −19.12 to −2.31; P = .01; Figure 2 ). However, a significant heterogeneity across the studies was shown in this analysis (heterogeneity measures: I2 = 96%, P < .001).

Forest plot illustrating the association of vitamin D deficiency with recurrent tonsillitis.
The included studies investigated the vitamin D status (vitamin D deficiency/insufficiency) in both case and control groups. Aydın et al 21 and Nseir et al 23 indicated that the vitamin D deficiency/insufficiency was more prevalent in patients with recurrent tonsillitis as compared with the healthy group, whereas Yildiz et al 5 and Torretta et al 25 suggested that recurrent tonsillitis was not significantly associated with vitamin D deficiency/insufficiency status, as compared to controls. However, the summary ORs revealed that serum vitamin D status had a significant effect on recurrent tonsillitis (OR, 4.37; 95% CI, 2.78-6.88; P < .001; fixed-effect model; Figure 3 ). Nevertheless, a substantial heterogeneity was detected across the included studies (heterogeneity measures: I2 = 92%, P < .001).
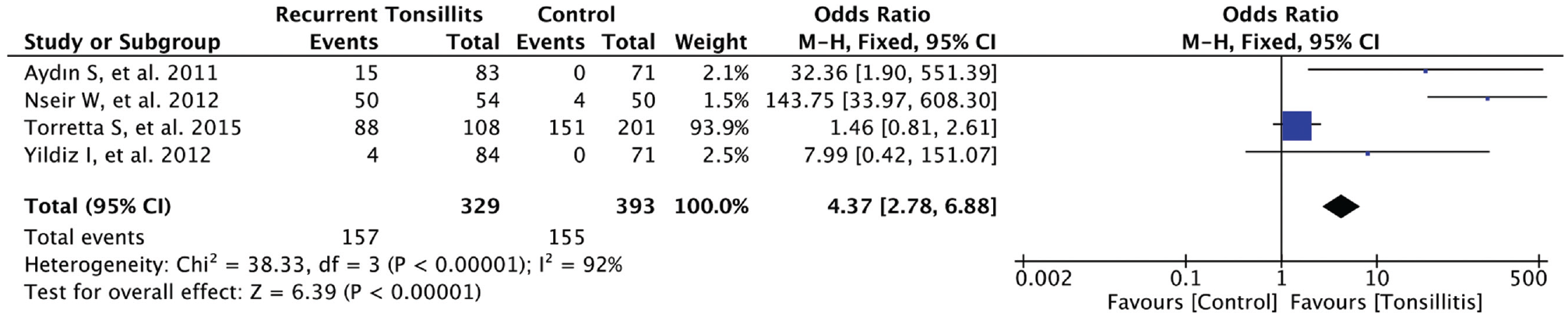
Forest plot demonstrating the prevalence of vitamin D deficiency/insufficiency in recurrent tonsillitis patients.
In addition, a case-controlled study investigated the occurrence of low vitamin D levels in patients with recurrent tonsillitis concomitant with allergic rhinitis. They revealed that the vitamin D values were lower in this particular group of patients (median, 34.65 pg/mL) compared to healthy controls (median, 52.86 pg/mL; P = .001). 22
With regard to the gross morphology of the tonsil, 1 study revealed a negative correlation between vitamin D and tonsil size (Spearman’s ρ = −0.417; P = .017). 15 Another also found that patients with tonsillar hypertrophy concomitant with severe symptoms of allergic rhinitis experienced low levels of vitamin D (P < .05). 22
Although in some disease polymorphisms, characteristics of the vitamin D receptor gene have been described, the included studies failed to prove an association between the group of recurrent tonsillitis and the healthy control with respect to vitamin D receptor gene polymorphisms.5,21
Evaluation of potential risk of publication bias, as per funnel plot illustration, demonstrated symmetrical distribution of published studies indicating no obvious risk of publication bias for the association between low level of vitamin D and recurrent tonsillitis ( Figure 4 ). Furthermore, the statistical analysis by Egger’s test revealed no significant finding of the publication bias in the meta-analysis (P > .658).
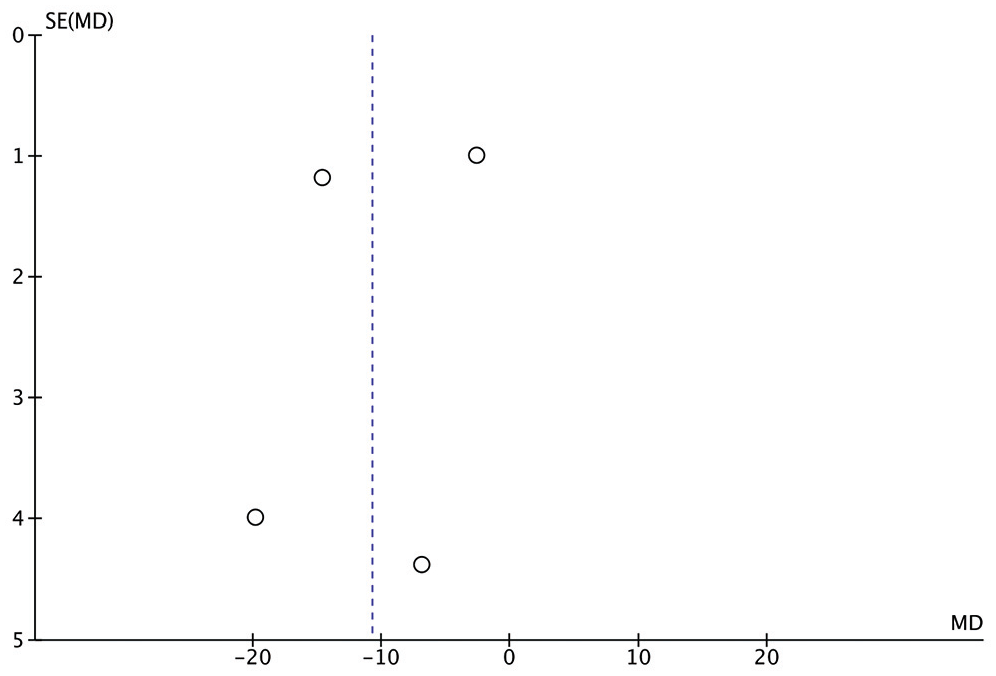
This funnel plot demonstrates symmetrical distribution of published studies indicating no obvious risk of publication bias for the association between low level of vitamin D and recurrent tonsillitis. MD, mean difference.
Discussion
Given the important role of vitamin D in innate immunity through the production of antimicrobial peptides (AMPs) that have been implicated in the destruction of invading microorganisms, 6 it is thought that vitamin D levels may be altered in patients with chronic tonsillar disease, which involves a complex interaction between innate and acquired immunity as well as bacterial load. In addition, vitamin D has been implicated in adaptive immune response through the influencing of autoreactive T cells and antigen processing cells. 28
The current systematic review including a meta-analysis of observation-based studies provided up-to-date scientific evidence of the risk of recurrent tonsillitis among patients with low vitamin D levels. A total of 4 studies conducted in different parts of the world recruiting adults and pediatric patients were included in the current meta-analysis. Serum 25-hydroxyvitamin D levels were retrieved from each individual study. In addition, the numbers of patients with vitamin D insufficiency or deficiency status, in both cases and control groups, were reported. Due to inconsistent reporting of vitamin D status (deficiency vs insufficiency) across the 4 studies, we chose to combine vitamin D insufficiency and deficiency in 1 particular group, namely, vitamin D insufficiency/deficiency, in the which vitamin D levels of 30 ng/mL were the cutoff value.
The present systematic review demonstrated that there was a significant reduction of vitamin D levels in patients with recurrent tonsillitis, supported by the second meta-analysis where there was an increase in risk of recurrent tonsillitis in patients with insufficient vitamin D. Inconsistent with the 3 other studies, findings by Aydın et al 21 showed no significant association of vitamin D levels with recurrent tonsillitis. It is worth noting that this study was conducted over a year, which may eliminate the eventual seasonal effect. However, they pointed out that vitamin D insufficiency was significantly higher among the patient group, as shown in the second meta-analysis. This variation across the different studies might be attributable to multiple factors, such as the difference in working groups, individual or racial factors, or the employed methods of vitamin D measurement.
Nseir et al 23 found that, after adjusting for confounders, vitamin D deficiency was associated with recurrent episodes of tonsillitis caused by group A streptococcus infection. In the first forest plot meta-analysis, findings by Nseir et al 23 were greatly deviated to left and showed the greatest MD and OR. This might be due to the selected population being adults with a mean age of just above 40 years, given the fact that vitamin D deficiency is more prevalent in adult than child populations. 29 Alternatively, this may be ascribed to the study population only including bacterial (group A streptococcus) tonsillitis cases. However, more evidence is required to establish an eventual particular association with bacterial vs viral tonsillitis.
Reid et al 15 reported that 15.6% of patients who underwent tonsillectomy had a deficient level of vitamin D (<20 ng/mL), and 78% of the same population had a level of vitamin D below 30 ng/mL, the level that was associated with a high incidence of URTIs. In addition, Torretta et al 25 demonstrated that vitamin D levels were decreased among patients with recurrent tonsillitis. However, adjustment of age and seasons yielded insignificant results.
Low vitamin D levels below 70 nmol/L (28 ng/mL) were also associated with a 50% increase in the risk of URTIs, as confirmed by polymerase chain reaction (PCR). 18 In addition, Ginde et al 30 found that the mean serum level of vitamin D in children undergoing tonsillectomy due to recurrent episodes of tonsillitis was less than 75 nmol/L. The same study showed that serum levels of vitamin D of <10 ng/mL, 10 to 30 ng/mL, and ≥30 ng/mL among different study groups had significantly different URTI rates of 24%, 20%, and 17%, respectively. Indeed, such findings indicate a remarkable reduction in the frequency of tonsillopharyngitis in association with increased vitamin D levels. 30 This is possibly because there is a growing body of evidence that 1,25(OH)D causes a remarkable increase in the production of cathelicidin peptides, 12 which are involved in several protective mechanisms against URTIs.31,32 In fact, the antiviral peptides induced by vitamin D might have a potent effect for fighting against adenovirus, herpes simplex type 1, and chickenpox. 33
In general, the incidence of URTIs, including tonsillitis, increases with young age and the reduction of vitamin D levels.18,34 Furthermore, the lack of adequate response to vitamin D might be a major player in the etiopathogenesis of chronic inflammation, particularly in neonates. This is because the anti-inflammatory response in neonatal neutrophils might be decreased, as reported by the prolonged neutrophil activity and decreased expression of vitamin D receptors in this age category. 35 Consistent with this observation, 1,25-vitamin D3 might cause reduction of lipopolysaccharide-induced expression of the inflammatory protein 1β and vascular endothelial growth factor exclusively in the neutrophils of adults rather than neonates. 35 Hence, in neonates, the decreased responsiveness to vitamin D may augment the burden of vitamin D deficiency and partially explain the increased liability to chronic inflammation, such as recurrent episodes of tonsillitis.
Polymorphism characteristics in the vitamin D receptor gene have been described in some diseases. 36 The presence of vitamin D receptors in immune cell types, such as the natural killer cells and B and T lymphocytes, has been also demonstrated.9,37 The existence of such receptors in those cells and the regulatory functions exerted by them due to stimulation of vitamin D receptors emphasize the relationship between vitamin D and the immune response, especially in the upper respiratory tract. 6 Furthermore, genetic polymorphism in vitamin D receptors in immune cells that results in modulation of their functions has been indicated. 38 However, both the studies by Yildiz et al 5 and Aydın et al 21 showed insignificant differences between the patients with recurrent tonsillitis and the healthy controls in regards to vitamin D receptor polymorphisms. Nonetheless, it seems that annual frequency of tonsillitis increases in patients with Ff polymorphism in the FokI receptors. 5
Tonsillar hypertrophy can be a result of recurrent infection. The relationship between tonsil size and vitamin D levels has been shown in Reid et al, 15 who demonstrated a significantly negative Spearman’s rank correlation coefficient between the operating surgeon’s classification of tonsil size and 25(OH) vitamin D levels (P = .017). San et al 22 revealed that vitamin D was significantly lower in patients with tonsillar hypertrophy and severe allergic rhinitis when compared to the control group. In fact, lack of vitamin D receptors could be associated with hypertrophy of subcutaneous lymph nodes as a result of dendritic cell accumulation in mice. 39 Moreover, low levels of 1,25(OH)D might contribute to decreasing the inhibition of dendritic cell differentiation, leading to adenotonsillar hypertrophy. 15
The aforementioned findings on the correlation between vitamin D levels and the incidence of recurrent tonsillitis have reinforced researchers’ need to investigate whether vitamin D supplementation would have a favorable impact on the incidence of URTI. Although some studies revealed that vitamin D supplementation reduced the incidence of seasonal influenza A 40 and acute respiratory infection, 41 including tonsillitis, other studies showed no effect of supplementation on the prevention of symptomatic URTIs.42,43 One meta-analysis of randomized controlled trials showed that patients with deficient levels of vitamin D (<25 nmol/L) experienced beneficial protection against acute respiratory infections. 24 There are no studies to date investigating the effect of vitamin administration on the occurrence of recurrent tonsillitis specifically.
The results of this systematic review should be cautiously interpreted due to the presence of some limitations. First, the low number of included studies might interfere with concluding sufficient remarks of a high statistical power. Second, the included studies showed a significant heterogeneity, which can potentially affect the relevant decision-making process, that is remarkable for systematic reviews. Such heterogeneity might be attributed to variations in the baseline characteristics of the participants, such as their age, sex, and ethnicity, as well as their numbers. The difference in timing of vitamin D level measurement and lack of a unified definition of the number of tonsillitis episodes to consider the patients as a “recurrent” case may be added as an additional limiting factor. Another limitation to be mentioned is that some factors led to reducing the quality of the included studies, such as a lack of case representativeness and a relatively inadequate selection of controls. Finally, despite no detected risk of publication bias in the meta-analysis, the authors were unable to exclude publication bias; this was due to the low statistical power that is owed to the limited sample size (ie, low number of studies).
Conclusion
In conclusion, the current evidence indicates that vitamin D levels could be related to the incidence of recurrent tonsillopharyngitis in children and adults, and bacterial pathogens tend to cause a higher reduction in vitamin D. In addition, this fact could be confirmed by the protective effect of vitamin D against upper respiratory tract infections. As such, future studies should focus on larger populations, with consideration to seasonal variation and standardized measurement of tonsil size. In addition, prospective studies investigating the effects of vitamin D supplementation on the incidence of recurrent tonsillitis are warranted. Finally, vitamin D screening should be encouraged for patients with recurrent tonsillitis, particularly at present where the prevalence of vitamin D deficiency is considerably high.
Supplemental Material
Appendix_1 – Supplemental material for The Association Between Vitamin D Deficiency and Recurrent Tonsillitis: A Systematic Review and Meta-analysis
Supplemental material, Appendix_1 for The Association Between Vitamin D Deficiency and Recurrent Tonsillitis: A Systematic Review and Meta-analysis by Ahmad A. Mirza, Abdulrahman A. Alharbi, Hani Marzouki, Talal Al-Khatib and Faisal Zawawi in Otolaryngology–Head and Neck Surgery
Footnotes
The study was presented as a poster at the 122nd Annual Triological Society Meeting at Combined Otolaryngology Spring Meeting (COSM); May 3-4, 2019; Austin, Texas.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.