
Abstract
Objective
To compare measurements of the pediatric subglottis obtained by surgeon-performed ultrasound and endoscopy.
Study Design
Prospective observational comparison-of-methods study.
Setting
Tertiary care pediatric hospital.
Subjects and Methods
Thirty-one patients who underwent direct laryngoscopy from May 2017 to July 2018 were recruited. Transcervical ultrasound was used to visualize the vocal folds, subglottis, and cervical trachea. The anterior-posterior (AP) and transverse (TV) diameter of the subglottic space were measured endoscopically and via ultrasound by 2 independent evaluators. Measurements were compared for correlation, bias, and agreement. A clinically acceptable bias for subglottic diameter was assumed to be 0.5 mm or less.
Results
The median age of enrolled patients was 2.6 years (range, 4 months–13.3 years). Endoscopic subglottic AP and TV measurements ranged from 3.33 mm to 14.81 mm and from 4.44 mm to 11.65 mm, respectively, while ultrasonographic AP and TV measurements ranged from 4.57 mm to 9.85 mm and from 3.77 mm to 8.96 mm. Pearson coefficient showed strong a correlation for both endoscopic and ultrasound AP (R = 0.8081, P < .0001) and TV (R = 0.8796, P < .001) measurements of the subglottis. Bland-Altman plots revealed a bias (average discrepancy) for AP measurements of 0.22 mm and 0.11 mm for TV measurements.
Conclusion
Endoscopic and ultrasonography measurements of the pediatric subglottic airway were strongly correlated. The discrepancy between AP and TV measurements was less than 0.5 mm. Ultrasound of the subglottis may be an alternative to endoscopic assessment of the airway for measurement of the subglottic airway in children in select cases.
Keywords
The circumferential nature of the cricoid cartilage renders the subglottis the narrowest part of the pediatric airway. Stenoses, cysts, and vascular lesions can further narrow the subglottis and cause airway obstruction in children.1-5 Patients with these conditions may present with stridor or varying degrees of respiratory distress. In-office or bedside flexible nasolaryngoscopy is indicated in stable patients with symptoms of airway obstruction, but clear visualization of the subglottis beneath the vocal folds with this modality is often limited. 6
The subglottis is more accurately evaluated by direct laryngoscopy with bronchoscopy (DLB), although computed tomography (CT) evaluation of the airway is gaining favor. 4 The subglottis can be sized during DLB by noting the largest endotracheal tube that allows a leak with a peak airway pressure of 25 cm water. 7 While a child is spontaneously breathing, dynamic airway collapse can also be observed. CT can also gauge airway size and anatomy and additionally reveal the relationship of the airway to surrounding vascular structures. DLB requires general anesthesia with its associated risks; however, many CT protocols also require general anesthesia. In addition, CT exposes children to radiation, which raises concerns about future potential malignancies. 8
Transcervical ultrasound (TUS) has been used to confirm and assist endotracheal tube and tracheostomy tube placement.9,10 Ultrasonographic assessment of the subglottis circumvents the need for anesthesia or radiation exposure. Subglottic diameter assessed by ultrasound has been shown to correlate to sizing by magnetic resonance imaging (MRI) in adults. 11 It has also been shown to correlate with airway sizing using endotracheal tube leak tests in children. 7
Accurate measurement of the subglottis has many applications, from assessment of the region for pathology to choosing an appropriate endotracheal tube size. Previous studies have shown that radiologist-performed TUS showed agreement with videobronchoscopic assessments when using tissue-air interfaces to define the size of the subglottis. 12 Accurate measurement of the cricoid ring is possible with ultrasound, 11 and surgeon-performed ultrasonography may be of use in airway evaluation. This study seeks to evaluate the accuracy of surgeon-performed TUS in assessing the size of the pediatric subglottis when compared with subglottic measurements assessed with DLB.
Methods
This is a prospective observational comparison-of-methods study. The study was approved by the Baylor College of Medicine Institutional Review Board (H-40120). Thirty-one consecutive children undergoing DLB as a part of a combined aerodigestive evaluation with concurrent flexible bronchoscopy and esophagogastroduodenoscopy were recruited. Informed consent was obtained for all procedures. Exclusion criteria were patients with a tracheostomy, prior laryngotracheal reconstruction, surgical intervention on the subglottis, or severe sleep apnea.
Measurement of the Subglottic Airway During DLB
DLB was performed using a tubeless spontaneous ventilation technique under general anesthesia. The larynx was exposed using an age-appropriate laryngoscope, and lidocaine was sprayed prior to evaluation of the subglottis. A 0° telescope (Karl Strorz SE & Co, KG, Tuttlingen, Germany) with a photorecording system was used to capture images of the subglottis. An endoscopic 90° blunt hook (Karl Strorz SE & Co, KG) of known length was placed in the subglottis to assist with estimation of subglottic dimensions. Two pediatric otolaryngologists performed independent measurements of all endoscopic images and were blinded to each other’s measurements. Measurements of the subglottis proceeded as follows: ratios of pixel lengths were used to calculate the anterior-posterior (AP) and transverse (TV) diameter. The number of pixels occupied by the reference hook was compared with pixel length, defined by a vertical line running from the AP limits of the subglottis and a horizontal line running from the TV limits of the subglottis using Adobe Photoshop (Adobe, San Jose, California). Calculated diameters in millimeters were recorded. An example is shown in Figure 1 . In this case, the known length of the reference probe was 5 mm. The number of pixels taken up by a vertical line running through the length of the probe was 75. The number of pixels taken up by the vertical line bounded by the limits of the subglottis was 93, whereas the pixels of the horizontal line was 99. The AP diameter for the example shown was 6.20 mm (93/75 × 5), while the TV diameter was 6.60 (99/75 × 5).
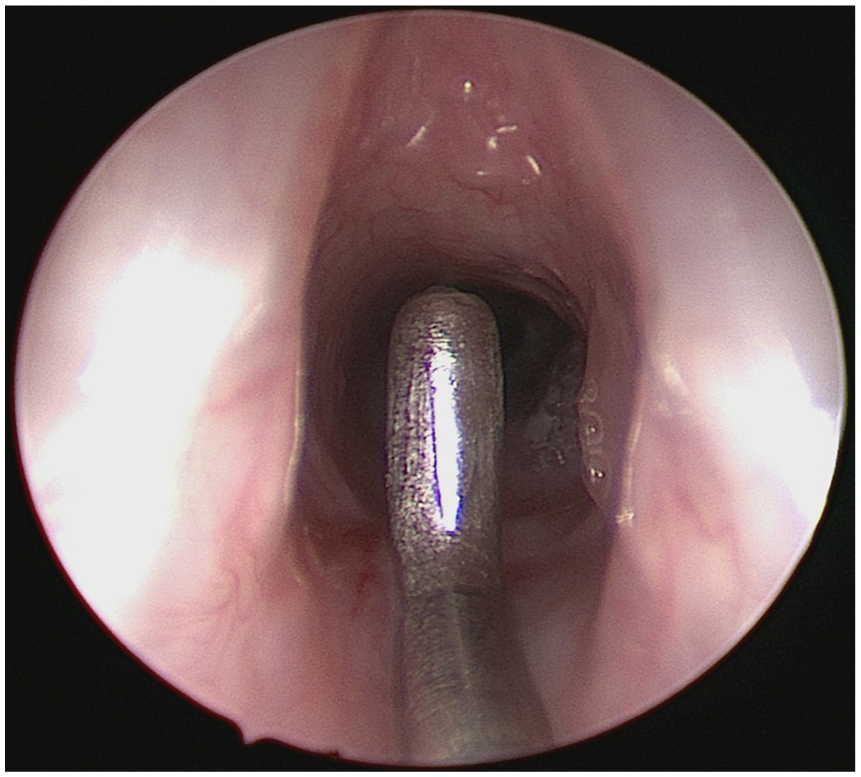
Endoscopy of the subglottic airway showing a right angle probe used to estimate subglottic diameter.
Transcervical ultrasound
Following the DLB, ultrasound was performed by the same surgeons who performed the DLB using a L38xp 10-5 MHz linear array with the Sonosite X-Porte system (Sonosite, Inc, Bothel, Washington). Serial images were taken from the sternal notch to the hyoid with the neck in the neutral position in the TV plane, with the right side of the patient oriented to the left side of the screen. Depth and gain of the ultrasound images were adjusted to resolve the airway landmarks. Images were saved and reviewed, and AP and TV measurements were made of the subglottic airway. Each surgeon performed independent measurements of all ultrasound images. When the laminae of cricoid were difficult to define, estimation of the subglottic space was made by defining the hyperechogecites formed by the air–soft-tissue boundaries between the airway and lamina. When neither the posterior laminae nor the posterior air–soft-tissue hyperechogenicity were identified, the position of the posterior laminae was estimated by drawing a TV line through the cricothyroid joint, as described in Or et al. 11
Statistical analysis
TV and AP measurements of the subglottis measured by DLB and ultrasound were compared by plotting the difference between the 2 measurements versus the average of the 2 measurements. Bland-Altman plots were graphed using Graphpad (Graphpad Software, San Diego, California). The bias or average discrepancy between the DLB and ultrasound measurements was calculated. The 95% confidence limits were also calculated. A clinically acceptable bias was set as <0.5 mm because of the size intervals used for endotracheal tubes. The correlation between values was noted using a Pearson correlation coefficient calculation with statistical significance attained with P < .05. A paired t test was performed to compare DLB and ultrasound measurements. Differences in measurements were deemed statistically significant with P < .05.
Results
Of 31 patients recruited, 21 were male (67.7%) and 10 were female (32.3%). The median age of patients in the study was 2.63 years (range, 4 months–13.3 years; interquartile range, 1.31-4.76 years). The mean age of the patients in the study was 4.0 (SD = 3.39). There were no adverse events during the study.
Endoscopic Measurements
All 31 patients had endoscopic assessments that allowed for AP diameter calculations, whereas adequate TV diameter calculations could be obtained from 29 of 31 patients. The 2 patients without TV measurements had subcordal edema and lateral shelves in the subglottis that inhibited reviewers from having accurate measurements. The median of the reviewer-averaged endoscopic subglottic AP diameter was 6.06 mm (range, 3.33-14.81 mm; interquartile range, 5.53-7.14 mm) with a mean of 6.54 mm (SD = 2.04). The subglottic TV diameter was 5.73 mm (range, 4.44-11.65 mm; interquartile range, 4.75-7.91 mm) with a mean of 6.34 mm (SD = 2.19). An example of the endoscopic view of the subglottis with reference probe is shown in Figure 1 .
Ultrasound Measurements
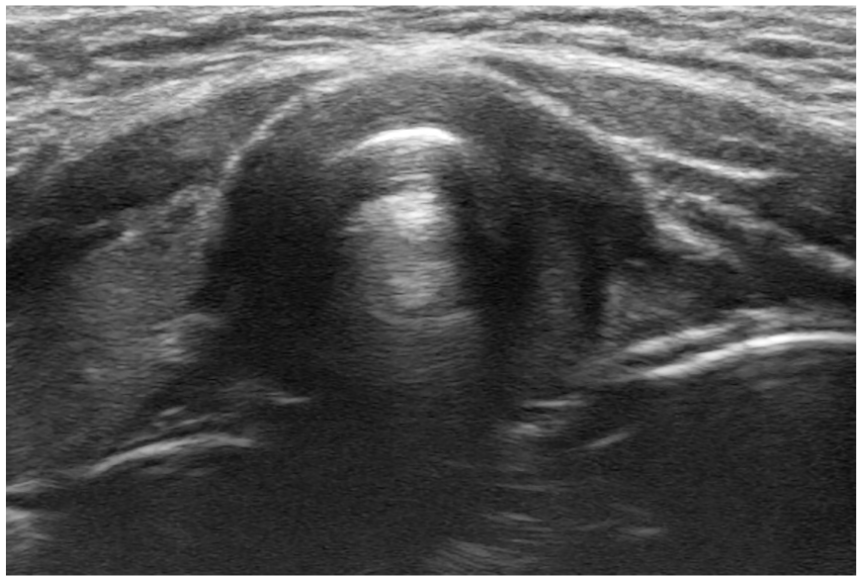
All 31 patients had ultrasounds in which the subglottis and/or cricoid ring was noted. The median of the reviewer-averaged ultrasound subglottic AP diameter was 6.18 mm (range, 4.57-9.85 mm; interquartile range, 5.15-7.09 mm) with a mean of 6.32 mm (SD = 1.38). The median TV measurement was 6.34 mm (range, 3.77-8.96 mm; interquartile range, 5.03-7.87 mm) with a mean of 6.46 mm (SD = 1.53). An example of the ultrasonographic view of subglottis with adequate resolution of the cricoid is shown in Figure 2 .
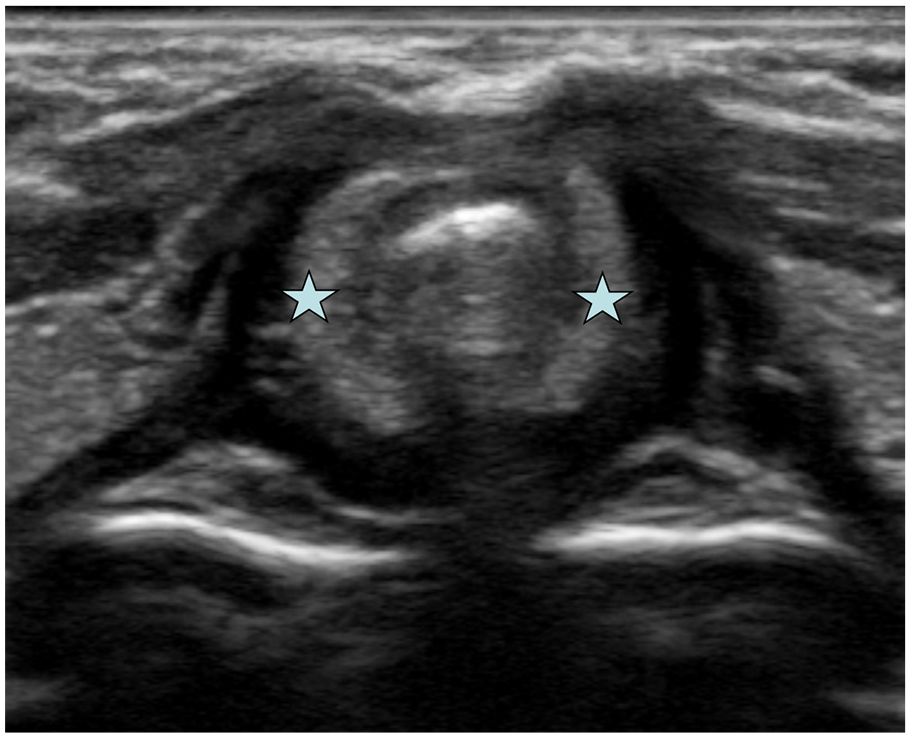
Transverse ultrasound of the subglottis at the level cricoid cartilage. The lateral aspects of the cricoid cartilage are indicated (★).
Comparison of Endoscopic and Ultrasonographic Views of the Subglottis
Calculation of the Pearson correlation coefficient between endoscopic and ultrasonographic measurements revealed a strong correlation for both AP (R = 0.8081, P < .0001) and TV (R = 0.8796, P < .001) measurements of the subglottis ( Figures 3 and 4 ). A comparison of the mean of all measurements showed no significant difference for AP DLB versus ultrasound (P = .33) and TV DLB versus ultrasound (P = .79) measurements. Unaveraged individual measurements were used to create Bland-Altman plots to compare measurements between the 2 modalities. The bias or average discrepancy for AP measurements was 0.22 mm and 0.11 mm for TV measurements. The 95% limits of agreement (LOA) for AP measurements was −2.664 to 3.102 mm, while the 95% LOA for TV measurements was −3.003 to 2.790 mm. As shown in Figures 5 and 6 , the difference between values did not seem to vary with average of values (ie, the difference between methods did not tend to get larger [or smaller] as the average increased). A subset analysis was done for patients younger than 3 years (n = 16) due to this age group’s susceptibility for recurrent croup. For AP measurements, bias in patients younger than 3 years was 0.05 mm (95% LOA −1.711 to 1.818), whereas TV measurements had a bias of 0.28 mm (95% LOA −2.221 to 1.652). There were subjects in whom the differences in DLB and ultrasound measurements were >3 mm. In these subjects, ultrasound images did not sufficiently resolve the cricoid ring, which appeared to prohibit accurate measurements of the subglottis ( Figure 7 ).
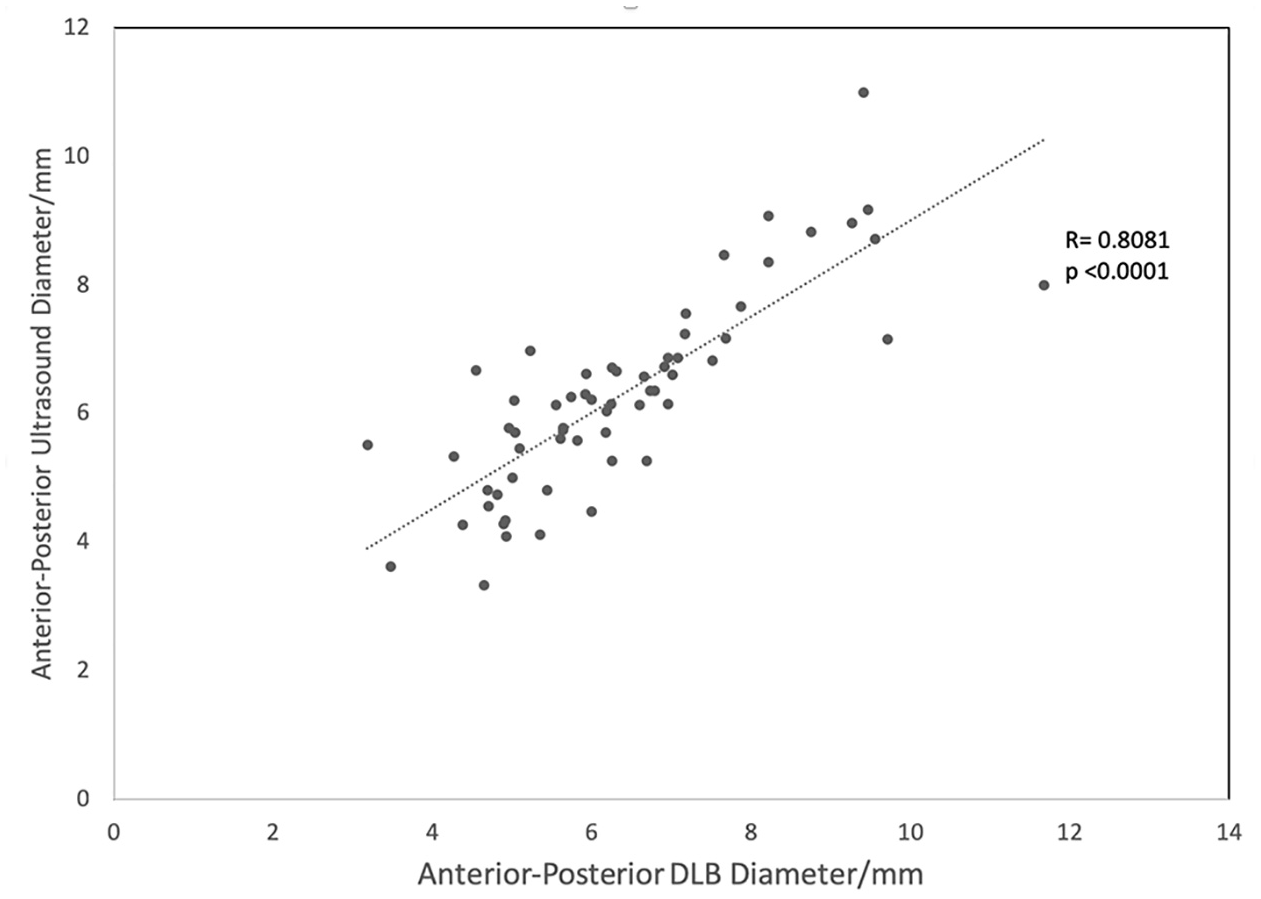
Plot of anterior-posterior direct laryngoscopy with bronchoscopy versus ultrasound subglottic diameter with trendline and R found by Pearson correlation shown.
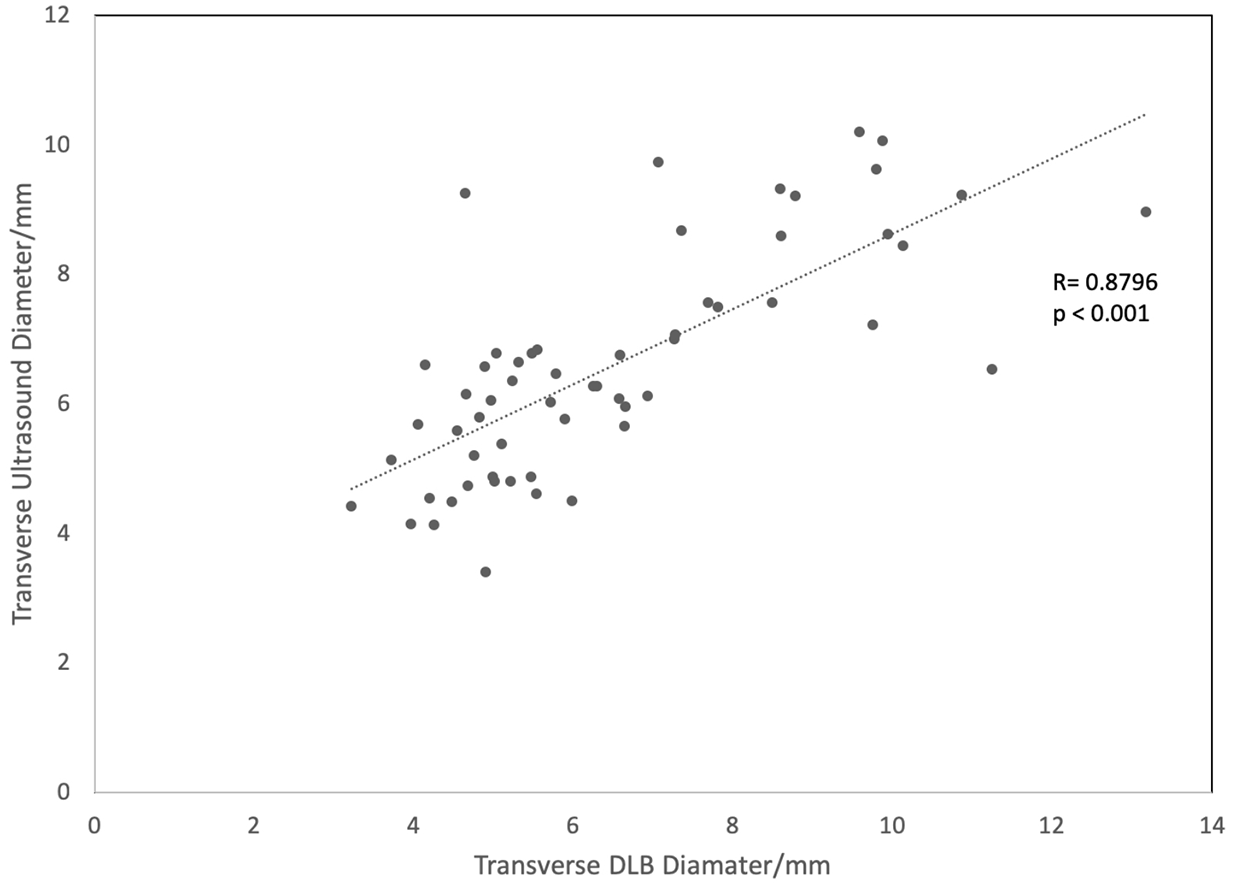
Plot of transverse direct laryngoscopy with bronchoscopy versus ultrasound subglottic diameter with trendline and R found by Pearson correlation shown.
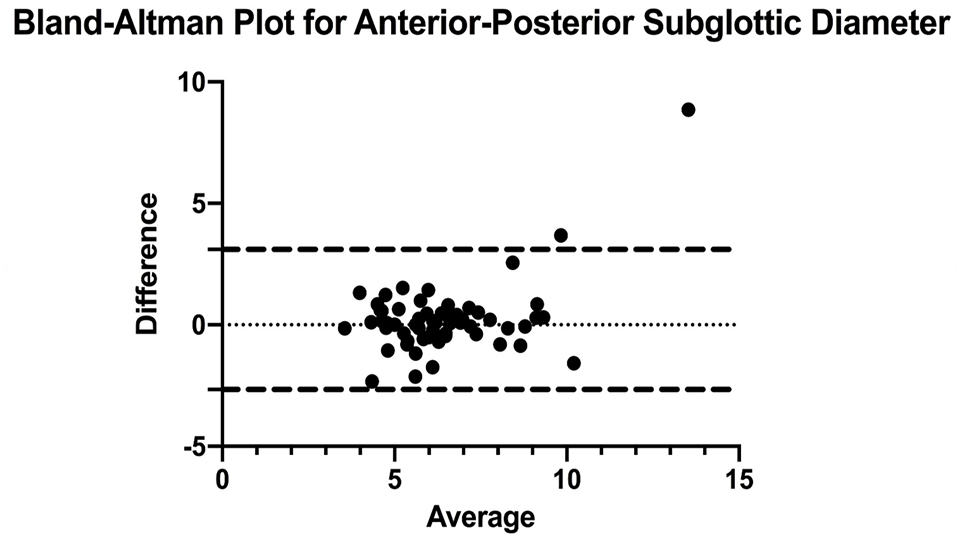
Blant-Altman plot showing differences in measurements versus average between anterior-posterior subglottic diameter assessed by direct laryngoscopy and bronchoscopy versus transcervical ultrasound. The 95% limits of agreement are indicated by the dashed lines.
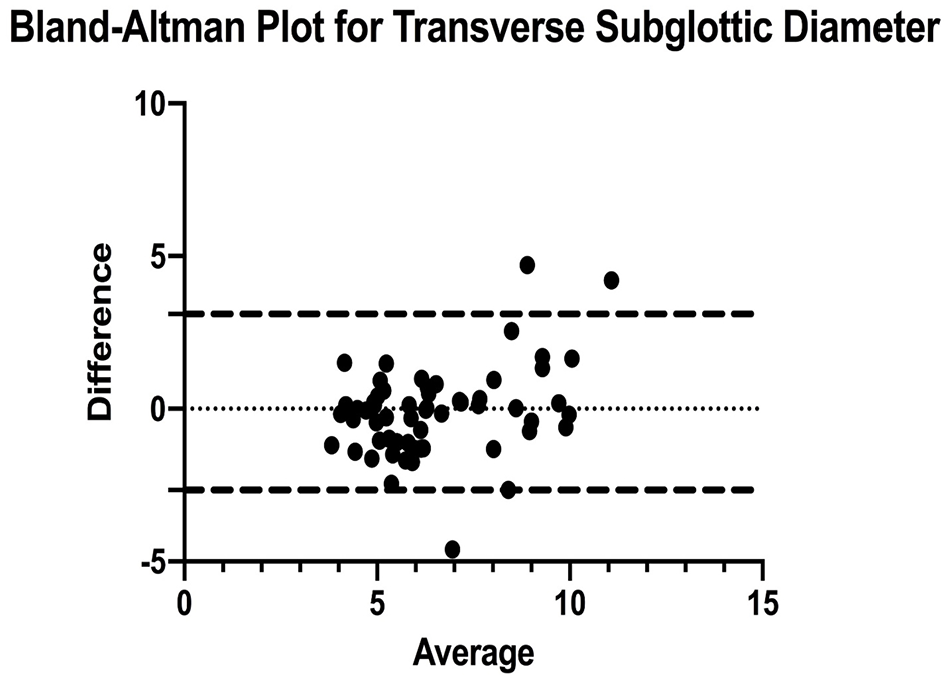
Blant-Altman plot showing differences in measurements versus average between transveres subglottic diameter assessed by direct laryngoscopy and bronchoscopy versus transcervical ultrasound. The 95% limits of agreement are indicated by the dashed lines.
Ultrasound at the level of the subglottis showing poorly defined boundaries of cricoids.
Discussion
We present a comparison-of-methods study using Bland-Altman plots to examine the differences in subglottic diameter evaluated by DLB and surgeon-performed ultrasound. This is the first study to document surgeon-performed ultrasound for subglottic measurement. The study shows average discrepancy between the 2 methods is <0.5 mm with a strong correlation, although the 95% confidence intervals for all subjects were greater than 1 mm. These results are similar to a study by Husein et al, in which the authors compared TV and oblique subglottic diameters found by videobronchoscopy and ultrasound. 12 Our study revealed a smaller 95% LOA confidence interval overall and documents the difference in AP diameter by the 2 methods. It should be noted that the referenced study precedes our work by more than 15 years. The resolution of ultrasonography continues to improve, and its applications in point-of-care evaluations are ever increasing. 13
Previous studies documenting subglottic measurements typically involve the use of an ultrasound technologist or radiologist to perform ultrasonography.9,10,12,14–16 Surgeons performed all ultrasounds in the study. Our data with the widest confidence intervals were associated with subject images, in which the limits of the cricoid were not easily seen. As surgeons attempt ultrasonography of the subglottis, gain, depth, and transducer types should be chosen that allow for adequate resolution of the cricoid. The study by Or et al, 11 which was a comparison-of-methods study between MRI and 3-dimensional (3D) ultrasonography for subglottic measurements in adults, had one of the lowest average discrepancies and smallest 95% confidence intervals (CIs) in the literature. This could be attributed to the ease with which 3D ultrasonography could resolve the cricoid, allowing for more accurate assessments. Future studies should investigate the use of 3D ultrasonography in the pediatric airway.
Subglottic stenosis, swelling, cysts, and vascular lesions are pathologies to consider in pediatric patients in whom subglottic obstruction is suspected. Ambulatory patients with hemangiomas, postextubation patients with subglottic swelling, and emergency department patients with croup often require evaluation of the subglottic airway to guide the practitioner. Patients younger than 3 years are particular susceptible to croup. We had a wide range of ages in the study (4 months–13 years), but 16 of 31 (52%) patients were younger than 3 and had a bias of <0.5 mm. The bias did not appear to vary greatly with age and appeared to be a function of adequately resolving the cricoid on ultrasound.
Although flexible laryngoscopy can be used to evaluate the subglottis as a point-of-care modality, the subglottis is often not easily seen. Safety concerns arise in patients who are in distress and in awake patients when a scope is advanced through the vocal cords.6,17,18 Imaging of the subglottic airway may be a safe alternative. CT of the airway is increasingly being used to image the subglottis, trachea, and bronchi.4,5 We must be cognizant of the radiation risk, especially in the area of the thyroid, which lies in the radiation field of the subglottic imaging. The utility of MRI in the assessment of the airway in children is also apparent, but the need for sedation is a disadvantage.
Otolaryngologists and anesthesiologists typically communicate airway sizes by the largest endotracheal tube size that allows a leak with a peak airway pressure of 25 cm water. Subglottic size measured by ultrasound has been previously shown to be predictive in choosing an appropriately sized endotracheal tube in children.7,14,15 Our study did not compare appropriate endotracheal tube size and subglottic diameter. The interval nature of endotracheal tube size is not appropriate for a comparison-of-methods study, in which continuous variables are favorable. Practitioners must be comfortable using subglottic diameters obtained by cross-sectional imaging for clinical use prior to using them. 19 This study also does not advocate for the use of ultrasound in lieu of DLB in the evaluation of the subglottis, when indicated, and the clinical utility of TUS has not been fully elucidated.
Future studies should establish normal subglottic measurements by age for clinical use with lower limits that could predict pathologic states. Clinical applications of interest include the use of TUS in patients with croup and postextubation stridor. In our study, ultrasound was performed using a 10-5 MHz linear array. The optimal transducer type, gain, and depth settings needed to create reproducible high-resolution images of the cricoid in airway imaging is not known. Our study also used TV scanning for measurements, whereas Or et al 11 used a sagittal view for AP measurements of the subglottic diameter. While it is not clear which method would provide more reproducible results, it is clear that a standardized protocol of obtaining subglottic images is needed.
Our study showed low average discrepancy (<0.5 mm), but the 95% CI was >1 mm. Bias and 95% CI varied between the AP and TV measurements in all age groups, but not systematically. The wide CI and variance between measurements may be due to several factors. Our DLB and ultrasound measurements may have been taken at different superior-inferior levels of the cricoid. There could also be errors in DLB measurements due to distortion of the image and inaccuracies in the estimation of probe length. Variable shadowing effects could have distorted both the lateral and posterior aspects of the cricoid, which also may lead to wide CIs. As with any comparison-of-methods study, practitioners have to decide whether the CI matters clinically, just as we accept differences in the various methods to assess core body temperature. 20 Development of normal values for subglottic sizes assessed by each modality studied (DLB, TUS, CT, and MRI) may be helpful to resolve discrepancies.
TUS could be developed as a point-of-care modality for the evaluation of the subglottis. Learning curves are apparent for the use of ultrasound in endotracheal tube placement 21 and may need to be established when measuring the subglottic space. The study was performed in anesthetized patients. Surgeon-performed TUS of the subglottis may be used in ambulatory, emergency care, or inpatient settings, especially as the portability of ultrasound machines improves. However, tolerability and the ability of adequate images to be obtained in awake patients should be investigated. We advocate that practitioners attempt to adjust ultrasound settings to gain adequate resolution of the cricoid, then capture serial images for later measurement. Ultrasonography of the subglottis in awake young children may be challenging, but we have highlighted safeguards and pitfalls of the technique in anesthetized subjects that may improve success in ambulatory patients. Protocols for TUS of the subglottis can also be developed for more formal assessments performed by ultrasound technologists and radiologists, but surgeons should be encouraged to develop point-of-care protocols as well.
Conclusion
AP and TV dimensions of the subglottis measured by surgeon-performed transcervical ultrasound show strong correlation with measurements obtained by direct laryngoscopy and bronchoscopy. Our study was the first of its nature to compare AP diameter assessed by these modalities. The average discrepancy between modalities was <0.5 mm. Our work highlights the application of ultrasound in measuring subglottic size, and with further study we hope that its clinical utility will be be developed.
Footnotes
Acknowledgements
We would like to thank the Texas Children’s Hospital Aerodigestive Program for allowing patients to participate in this study.
This article was presented at the 2019 AAO-HNSF Annual Meeting & OTO EXPO; September 15-18, 2019; New Orleans, Louisiana.