
Abstract
Objective
There is a debate regarding the durability of fat implants. Our experience and recent publications suggest fat implantation may deliver a long-lasting improvement. This study aims to present the long-term outcomes for vocal fold fat augmentation using strict harvesting, preparing, and implantation protocols.
Study Design
A prospective cohort conducted between 2014 and 2020 (recruitment 2014-2017).
Setting
An academic tertiary referral center.
Subjects and Methods
Twenty-two patients with glottic insufficiency were enrolled: 11 had unilateral vocal fold paralysis (UVFP), and 11 had atrophy or scar. Harvested fat was injected unilaterally or bilaterally into multiple sites. Six of these patients also had simultaneous microlaryngoscopic removal of other benign glottic lesions. Outcome measurements included video stroboscopy; Grade, Roughness, Breathiness, Asthenia, Strain (GRBAS) score; Voice Handicap Index (VHI); and acoustic analysis, performed preoperatively, 3, 12, 24, and 36 months after surgery.
Results
Ten augmentations were unilateral and 12 bilateral. Comparing the preoperative and 36-month postoperative periods, the mean VHI score improved from 73.45 (±22.78) to 44.88 (±28.93), P = .001, and the mean GRBAS decreased from 8.64 (±3.89) to 2.82 (±2.3), P = .001; 24 months postoperatively, the mean fundamental frequency decreased from 163.88 Hz (±41.61) to 150.44 Hz (±41.47), P = .012. Stroboscopic analysis revealed statistically significant improvement in mucosal wave propagation, phase closure, and phase symmetry. Best results were achieved in the UVFP subgroup. Computed tomography scans demonstrated long-term viability of the implanted adipose tissue.
Conclusion
Fat is an excellent source of autologous graft. With careful patient selection and proper surgical technique, fat is suitable for long-term correction of glottic insufficiency. Fat augmentation should be considered as a long-lasting or even permanent solution, rather than temporary.
Glottic insufficiency is defined as the inability to achieve glottic closure, resulting in voice and swallowing dysfunction. 1 Etiologies include unilateral vocal fold paralysis (UVFP), atrophy, and scar.2-5 Dysphonia may result from air leak and/or impaired vibration; symptoms and signs may include vocal fatigue, speech dyspnea, breathy voice, roughness, and strain. Generally, treatment aims for improved closure and vibration. These can be achieved by voice therapy, injection laryngoplasty, or laryngeal framework surgery. 6 Medialization or augmentation can improve glottic closure and reduce air leak. These procedures may also improve vibration, as long as the vibratory components of the vocal folds (VFs) are intact.
In medialization laryngoplasty (thyroplasty type I 7 ), the VF can be medialized with silicone, Gore-Tex, or titanium implants.8-13 It offers a long-term relief in UVFP. It is, however, limited in voice improvement in cases of VF scarring. 5
Medialization by injection augmentation can be achieved by synthetic and biologically derived materials or autologous grafts. Synthetic and biologically derived options include calcium-hydroxylapatite, hyaluronic acid, and collagen-based products14,15; all are absorbed over time, with a range of 2 to 12 months of glottic insufficiency relief. None of these materials can improve vibration in a scarred VF. Autologous materials include fat and fascia. Their advantages are availability and low cost. These materials may also improve vibration of scarred atrophic folds. 16 Fat transfer was introduced by Brandenburg et al 17 in 1987. In VF atrophy, fat augmentation may improve roughness, breathiness, amplitude, and mucosal wave excursion. 18 Fat transplant integrates and survives in the injection site. 19 Concern relates to the unpredictability of the graft’s final volume retention and outcome durability. 20 Because partial reabsorption of fat is inevitable, overinjection is recommended 17 ; yet, the durability of the correction remains unpredictable, despite all efforts and improved techniques. 20
There is a debate regarding the long-term effect of VF fat implantation. Traditionally, the duration of fat graft survival was expected to last no longer than 6 to 9 months.21,22 However, recent publications have suggested an impact that last at least 1 year, 23 and imaging studies have proved that approximately 30% of the injected fat may survive over 2 years.24,25
The dynamic properties of fat are closest to that of the VF mucosa. Therefore, its use may be favorable for phonatory improvement. 26 Another reported graft is autologous fascia, injected 27 or transplanted.28,29
In the past decade, we have performed fat injection under a strict protocol of harvesting, preparation, and injection. Encouraged by our favorable long-lasting results, we performed a prospective, long-term study to analyze the functional outcome of this procedure. We hypothesized that with proper patient selection and adequate surgical technique that will be described in detail, adipose graft can last years after injection and may provide a long-term solution for glottic insufficiency.
Methods
This prospective cohort study was approved by the institutional review board of Kaplan Medical Center, Israel. Adult patients with glottic insufficiency due to UVFP, atrophy, or scarring or sulcus were recruited between 2014 and 2017; patients were follow-up for 3 years (complete study period 2014-2020). Exclusion criteria included severe glottic fibrosis following radiation or stenosis, significant donor site (abdomen) scarring, or cachexia. Another exclusion criterion was a chance for spontaneous recovery of a paralyzed VF. Only patients with proven recurrent laryngeal nerve irreversible injury, complete recurrent laryngeal nerve section during surgery, or those who had longer than 1.5 years of follow-up after paralysis diagnosis, were included.
Study Protocol
Patients were first diagnosed by video stroboscopy. They were offered observation, voice therapy, fat augmentation, or thyroplasty. Patients who chose fat augmentation were offered to participate in the study. The study protocol included preoperative workup, surgical procedure, and long-term follow-up.
Preoperative Workup
Patients underwent video stroboscopy (Xion EndoStrob-DX, DIVAS Berlin, Germany) using a rigid (Hopkins strobo laryngoscope 70°, Karl Storz, Tuttlingen, Germany) or flexible distal-chip endoscope (Olympus ENF-V2 digital video rhinolaryngoscope, 3.2 mm, Center Valley, Pennsylvania). Video stroboscopic parameters and Grade, Roughness, Breathiness, Asthenia, Strain (GRBAS) scores were analyzed by two experienced laryngologists (Y.L. and H.S.H.). Stroboscopic parameters included mucosal wave propagation, phase closure, and phase symmetry, according to Poburka et al. 30 Mucosal wave propagation was defined as the magnitude in the percentage of lateral movement of the mucous membrane. Phase closure was defined on a scale from 1 to 5 (1 = open phase predominates, 3 = nearly equal, and 5 = closed phase predominates). Phase symmetry was defined as the degree of symmetry of vibration between the left and the right VFs in percentage. GRBAS scores were determined using the Hebrew language–validated version of the rainbow passage. 31 The Voice Handicap Index (VHI) was calculated using the Hebrew language–validated questionnaire. 32 Finally, acoustic analysis was performed using a computerized speech lab (CSL, Pentax Medical, Tokyo, Japan), which included fundamental frequency, vocal frequency range, jitter, shimmer, noise-to-harmonic ratio, and maximal phonation time.
Surgical Procedure
All procedures were performed under general anesthesia by the same surgeon (Y.L.). The donor site was the abdominal wall and rarely gluteal. Prophylactic intravenous antibiotics (cefalexin or clindamycin) were administered. The skin was prepared and draped, and a 2-mm stab was performed at the periumbilical or upper gluteal regions. An infiltration cannula (Col-Anes tumescent cannula 16ga-15 cm, Coleman, California) was inserted into the subcutaneal fat, and approximately 100 mL of tumescence solution (1000 mL ringer lactate, 1 mg adrenaline, 400 mg lidocaine) was infiltrated in a funnel-shaped motion to disintegrate the adipose tissue and to deliver local anesthesia and hemostasis. Fat harvesting began at least 10 minutes after infiltration.
A harvesting cannula (Col-Asp aspiration cannula, 23 cm) was introduced. Fat was aspirated into a 10-mL syringe by applying gentle manual negative pressure. Four to eight syringes, with a total of ~60 mL of aspirate, were aligned vertically for passive gravitational separation into 3 distinct layers of serum or water, adipose tissue, and free fatty acids. The separation process took about 10 minutes. The lower and upper layers were disposed, and the adipose tissue was spread over a Telfa nonadherent dressings sheet 3- × 4-inch (Covidien-Medtronic, Dublin, Ireland), for absorbance of residual serum, blood, and free fatty acids. Following this process, the fat aspirate would generally produce ~6 mL of homogenous yellowish paste. The graft was then loaded into a fat injection pistol (MCL55, Integra-MicroFrance, Plainsboro, New Jersey), and injected using a compatible 19-gauge needle (MCL55-1, Integra-MicroFrance). The total time from harvesting to implantation generally took 15 to 20 minutes.
To allow maximal survival of the graft, it was injected in repeated small doses through multiple injection points, as was previously suggested. 25 With this technique, the total surface area of the graft is larger than if it would have been injected in one bolus. Larger surface area allows for better nutritional support and oxygen delivery to the graft by the accepting tissue. Injection in one large bolus could lead to central graft bulk necrosis. Most injections were paraglottic, lateral or deep to the ligament, and posterolateral to the vocal process for optimal medialization; in selected cases, fat was also injected superficial to the ligament. Overinjection was the immediate desired outcome, taking into consideration partial resorption of the graft. An estimated amount of 2 to 3 mL of fat implant, were injected to each paraglottic space.
The decision to inject one VF or both was determined not only by the pathology but also by the relation of the VFs to each other. Bilateral scarring or atrophy was injected bilaterally as a rule. Unilateral paralysis was sometimes injected bilaterally, to overcome a large gap, or when the contralateral VF was atrophied. The decision regarding unilateral versus bilateral injection was taken preoperatively, based on stroboscopic findings and the relative contribution of each side to the glottic incompetence.
Patients were discharged 24 hours after surgery. A voice rest for 7 days was advised. No antibiotics or antireflux medications were prescribed routinely.
Postoperative Follow-up
All preoperative measures: video stroboscopy, GRBAS, VHI, and acoustic analysis were repeated at 3 months and 1, 2, and 3 years following surgery.
Statistical Analysis
Preoperative versus postoperative scores were compared using a paired Wilcoxon signed-rank test: patients’ scores were specifically compared with their own preoperative scores for each measure (ie, stroboscopic analysis, VHI, and GRBAS) and for each postoperative time point (3 months and 1, 2, and 3 years after surgery).
Continuous variables were tested for normality (Shapiro-Wilk test); for abnormal distribution, nonparametric tests were performed. Mann-Whitney U test was used to compare the groups for continuous variables (age and duration of surgery).
For all tests applied, a P value of .05 or less was considered significant. Statistical analyses were performed using SPSS version 20.0 (IBM, Armonk, New York).
Results
Twenty-two patients (16 males) were enrolled, with a mean age of 48.3 years (range, 15-75 years). Pathologies included 11 UVFP, 11 atrophy, 7 sulci, and 2 scars. Six cases of UVFP were injected before 1.5 years passed since paralysis was diagnosed: all were postsurgical cases with a complete recurrent laryngeal nerve section reported by the surgeon. The median time for injection in these 6 cases was 9 months after diagnosis (range, 3.6-10.8 months). All other cases were injected 1.7 to 16.7 years after paralysis was diagnosed ( Table 1 ). Six patients had other pathologies operated simultaneously: 3 tiny vascular lesions, 1 small cyst, 1 sulcus dissection, and 1 partial medial arytenoidectomy due to cartilage distortion. Ten patients had unilateral injections; 12 had bilateral injections. All patients were injected to the paraglottic space, deep to the ligament; 4 selected patients with either scar or sulcus were also injected superficially ( Table 1 ). The mean duration of surgery was 1:05 hours(range: 0:47-1:36). The mean follow-up was 3.8 years(range: 3.0-4.8). All 22 patients completed the preoperative workup; 21, 20, 17 and 18 patients complied with follow-up analyses in 3 months, 1, 2 and 3 years respectively. Table 1 summarizes the clinical and surgical data of all patients. Supplemental Figure S1 provides details on the adherence of each patient with each component of the protocol.
Demographic, Clinical, and Surgical Details of the Study Cohort.
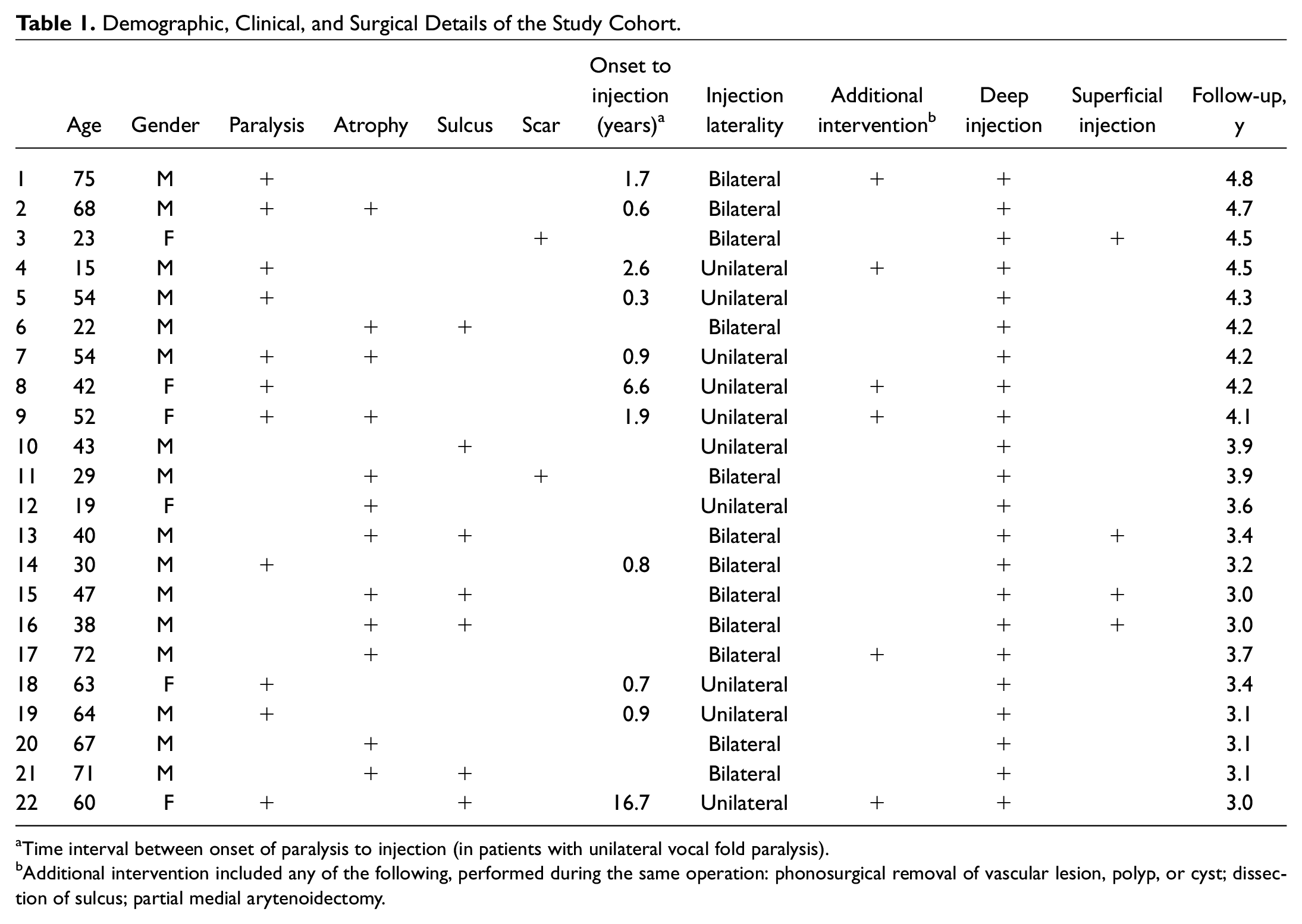
Time interval between onset of paralysis to injection (in patients with unilateral vocal fold paralysis).
Additional intervention included any of the following, performed during the same operation: phonosurgical removal of vascular lesion, polyp, or cyst; dissection of sulcus; partial medial arytenoidectomy.
The mean (±SD) preoperative GRBAS score improved from 8.64 (±3.89) to 3.43 (±3.43), 3.58 (±2.71), 2.50 (±2.11), and 2.82 (±2.3) at 3 months and 1, 2, and 3 years after surgery, respectively ( Figure 1A ). The mean (±SD) preoperative VHI score improved from 73.45 (±22.78) to 52.79 (±25.89), 51.17 (±25.42), 43.67 (±24.80), and 44.88 (±28.93) at 3 months and 1, 2, and 3 years after surgery, respectively ( Figure 1B ). The consistent improvement in VHI and GRBAS was statistically significant in each of the follow-up examinations as compared with the preoperative scores.
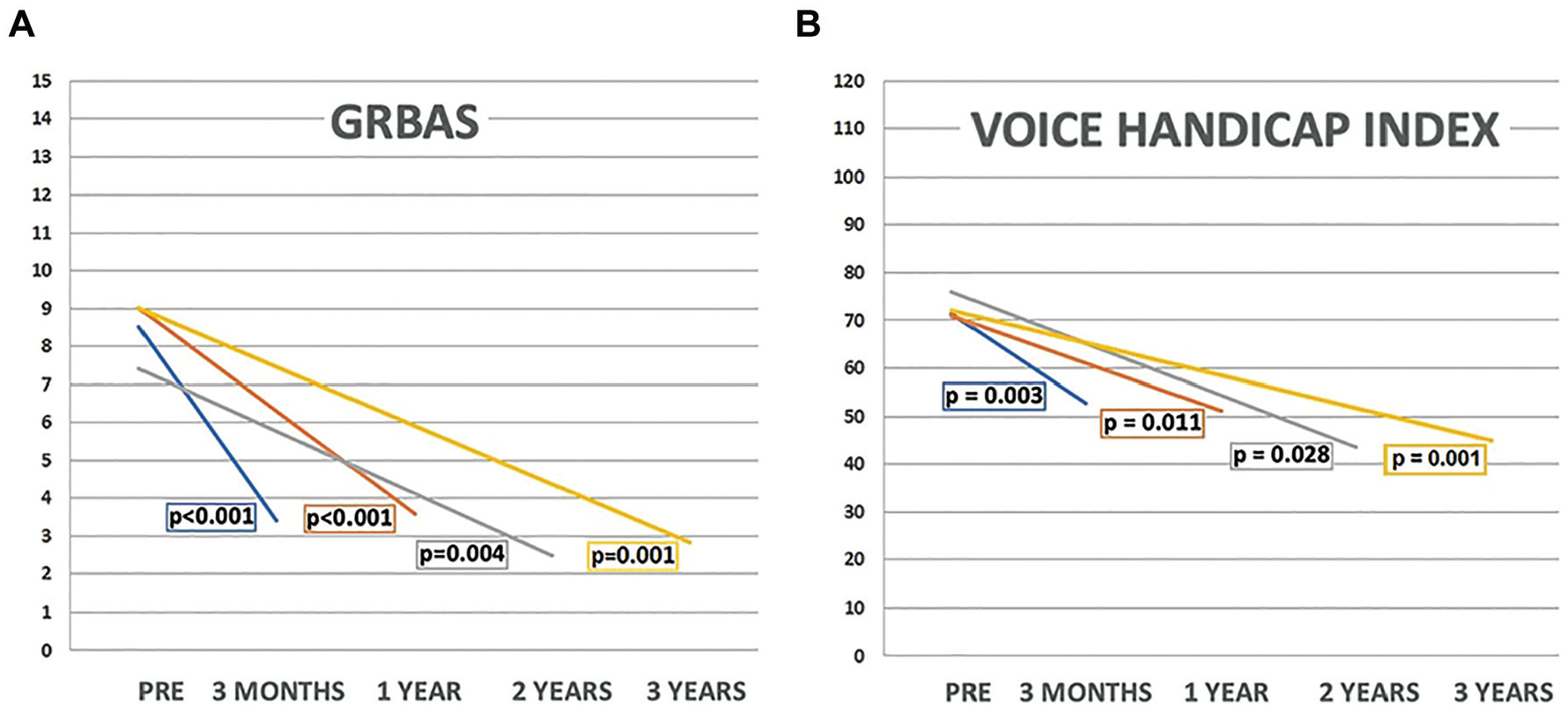
(A) Grade, Roughness, Breathiness, Asthenia, Strain (GRBAS) and (B) Voice Handicap Index (VHI) paired comparisons, between each time point after surgery and the preoperative score (paired Wilcoxon signed-rank test). Each line denotes the data only from subjects who followed up at the specified time point.
The mean fundamental frequency decreased from 163.88 Hz to 150.25, 151.55, 150.44, and 156.92 Hz at 3 months and 1, 2, and 3 years after surgery, respectively; statistically significant improvement was noticed for the 2-year follow-up measure (P = .012; Table 2 ). The preoperative mean (±SD) maximal phonation time was 11.02 (±4.93). It increased to 13.90 (±4.98), 13.30 (±5.46), 12.86 (±4.76), and 15.69 (±4.17) at 3 months and 1, 2, and 3 years postoperatively, respectively. The last 2 measures were statistically significant compared with preoperative measures ( Table 2 ). Measures of jitter, shimmer, and noise-to-harmonic ratio failed to demonstrate any consistent change. Stroboscopic analysis revealed statistically significant improvement in mucosal wave propagation, phase closure, and phase symmetry at 1, 2, and 3 years after surgery ( Table 2 ).
Acoustic and Stroboscopic Analysis.
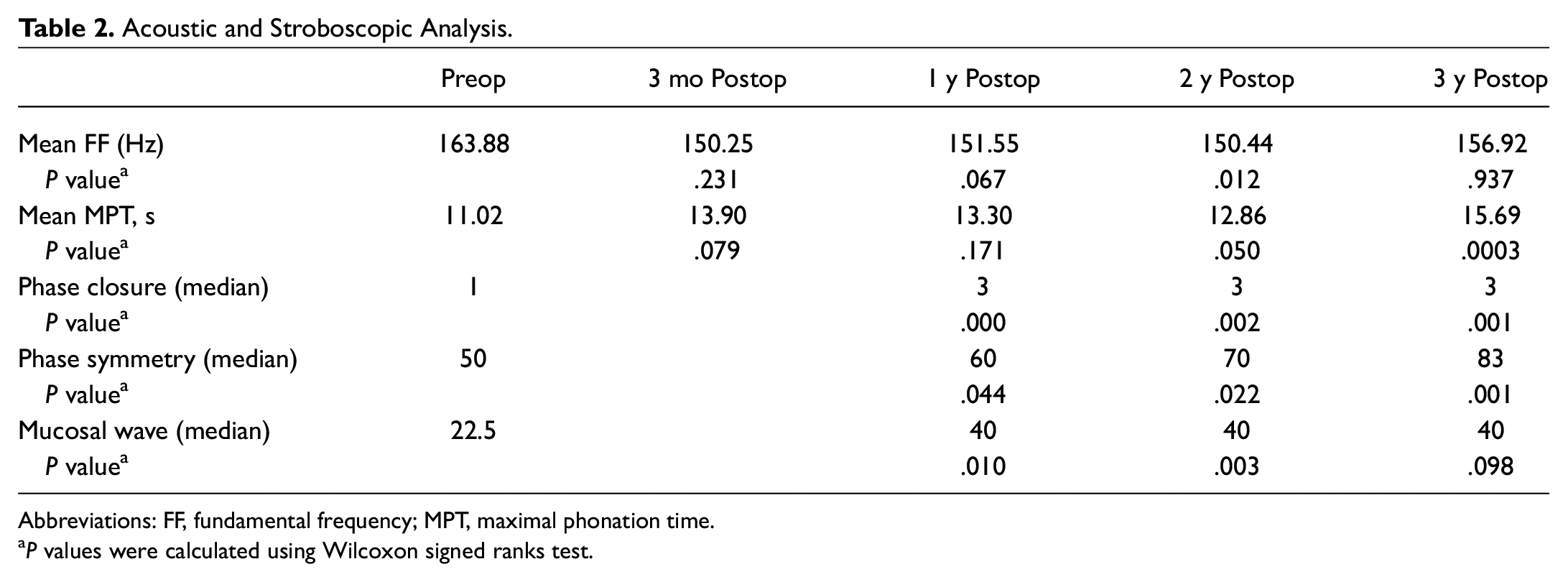
Abbreviations: FF, fundamental frequency; MPT, maximal phonation time.
P values were calculated using Wilcoxon signed ranks test.
When comparing patients injected for UVFP with patients injected for other etiologies, both subgroups demonstrated significant improvements compared with the preoperative assessment. However, patients with UVFP had significantly better results in some of the measures (GRBAS, vocal frequency range, phase closure, and phase symmetry) as compared with the subgroup with other etiologies ( Table 3 ). Furthermore, the vocal frequency range specifically became worse in the other etiologies group.
Outcomes for Patients With Unilateral Vocal Fold Paralysis Versus Nonparalysis Patients. a
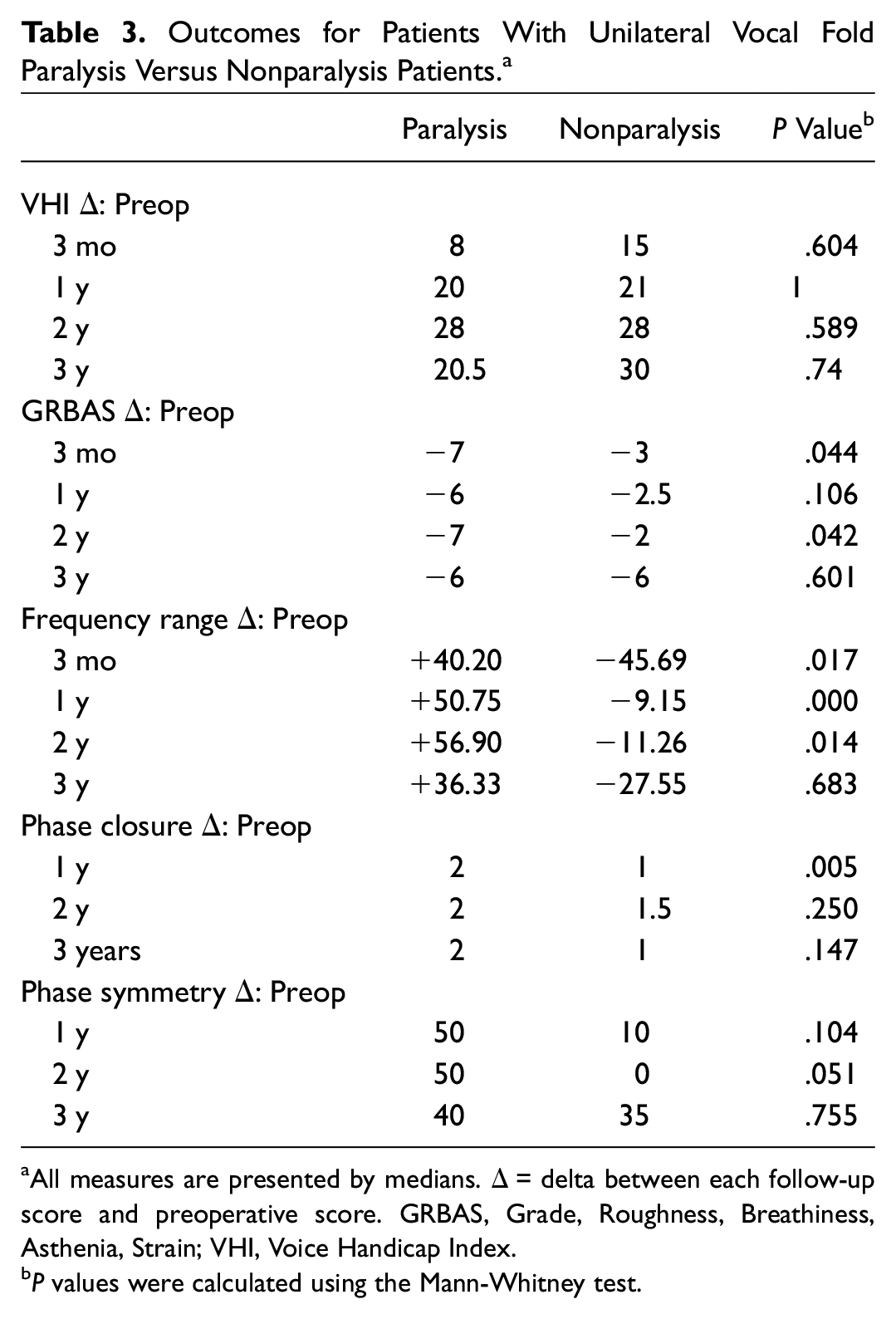
All measures are presented by medians. Δ = delta between each follow-up score and preoperative score. GRBAS, Grade, Roughness, Breathiness, Asthenia, Strain; VHI, Voice Handicap Index.
P values were calculated using the Mann-Whitney test.
No significant differences were noticed when comparing patients who had unilateral injections with patients who had bilateral injections or when comparing patients who had simultaneous phonosurgical procedure with patients who had not.
None of the patients required an additional or revision surgery during the follow-up period. Figures 2 and 3 present endoscopic images of long-term effect of bilateral fat-augmentation in a patient with VF atrophy and left VF augmentation in a patient with UVFP, respectively.
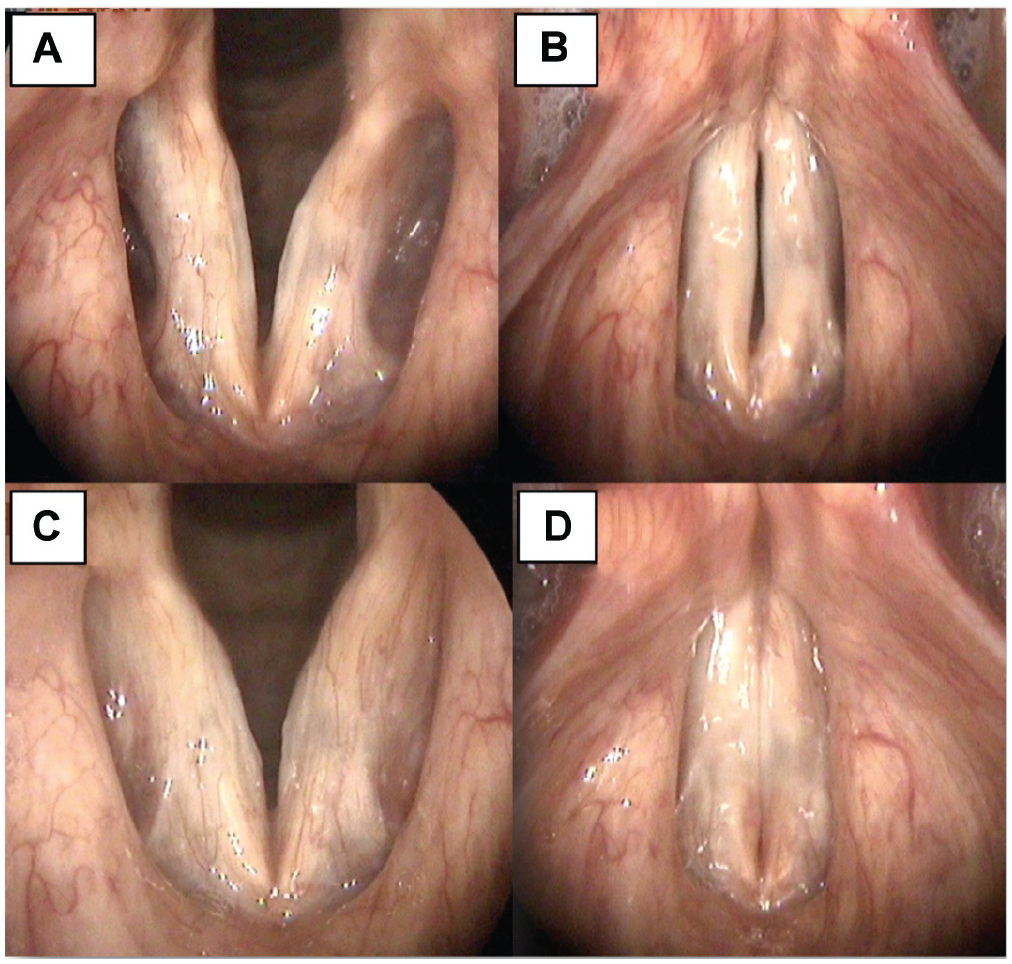
Age-related bilateral vocal fold atrophy, before and after bilateral fat augmentation. (A) Preoperative abduction, Note the deep ventricles. (B) Preoperative adduction with spindle or irregular glottal gap. (C) Two years after bilateral fat augmentation, abduction. (D) Two-year postoperative adduction.
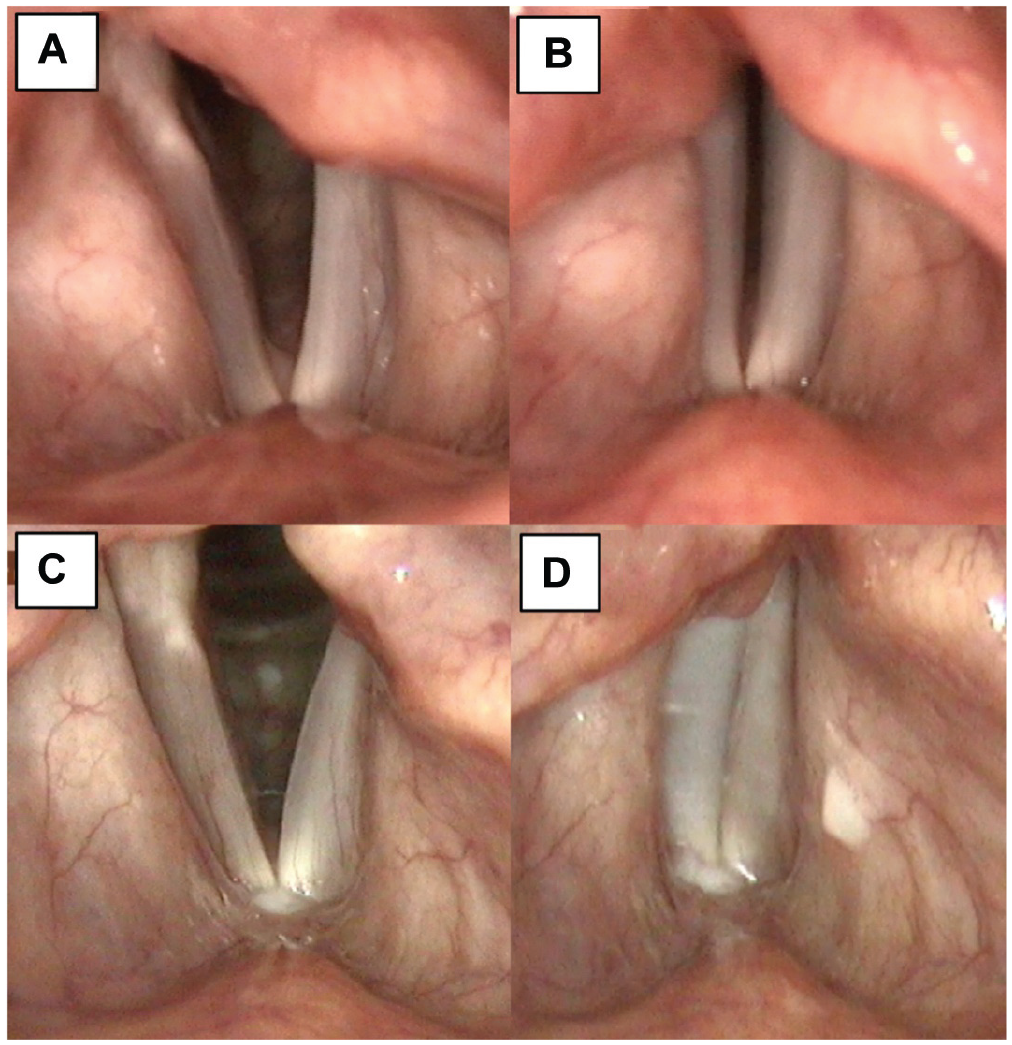
Left vocal fold paralysis, before and after unilateral fat augmentation. (A) Preoperative abduction. Note left vocal fold concavity (B) Preoperative adduction with incomplete glottal gap. (C) Three-year postoperative abduction, with convex left vocal fold. (D) Three-year postoperative adduction.
Discussion
In this prospective series, we treated glottic insufficiency by fat injection and described the follow-up over a period of 3 to 4.5 years. VHI, GRBAS, and acoustic and stroboscopic analyses suggested the long-term beneficial outcome of fat augmentation. These findings confirmed our hypothesis that fat augmentation may offer a durable solution. To our knowledge, this is the first prospective study conducted on VF fat augmentation with a thorough workup and long-term follow-up. Similar to previous publications, 33 we did not encounter significant adverse effects, as fat augmentation is a benign surgery with very few complications.
Previous studies have demonstrated improvements in acoustic, aerodynamic, and perceptual measures after fat injection; however, they provided only short-term data.2,6,17,23,34 Long-term graft survival (up to 42 months) was illustrated using serial magnetic resonance imaging scans in 5 patients. 25 We believe the key for long-term success is preservation of adipose graft viability along the pathway of harvesting, preparation, and injection. Blood residue within the transplanted fat accelerates its degradation. 20 Therefore, we preceded the harvesting with atraumatic infiltration of tumescence solution (containing lidocaine and adrenaline) to disintegrate the adipose layer and to minimize intraoperative bleeding. Adipose graft can be harvested by either aspiration or resection and mincing. Havas and Priestley 1 described lipo aspiration with a low-suction apparatus and a collecting canister. Hsiung et al 2 described an incision in the lower abdomen, fat resection, mincing, and disposing nonadipose tissue. Comparing these 2 techniques, liposuction did not result in increased adipose cell damage. 20 Furthermore, Park et al 35 found that while liposuction initially causes more damage than resection, it may yield improved long-term viability. Liposuction is our preferred modality because of donor site consideration and easier graft processing. For isolation of vital fatty tissue, we favor gravitational passive separation, as it may be less traumatic than electrical centrifuge, although others advocate its use. 25 The Telfa sheath has an important complementary role, as it absorbs undesirable components in an atraumatic fashion.
We performed the entire procedure under general anesthesia with endotracheal intubation, with fat injected transorally. Hu et al 6 performed both abdominal harvesting and thyrohyoid membrane injection under local and topical anesthesia. Havas and Priestley 1 preferred general anesthesia with the avoidance of endotracheal intubation, alternating between laryngeal mask and jet ventilation. Theoretically, this technique may allow for more posterior augmentation, without the interference of the endotracheal tube. We prefer general anesthesia as it allows better control and injections of small fat droplets in multiple sites. We argue that this technique enlarges the graft’s surface area and promotes nutritional support, until a neovascular network is formed. For similar reasons, Cantarella et al 25 favored injection at multiple entry points; they also suggested a multilayered injection while withdrawing the needle.
Unlike synthetic implants, fat is a vascularized tissue consisting of adipocytes, preadipocytes, endothelial cells, and stem cells. 35 The success of implantation may partially derive from survival and differentiation of stem cells within the transplanted aspirate. 15 The atraumatic harvesting, preparation, and injection is essential also for stem cell preservation.
Fat graft resorption is a major drawback of this technique. Canine studies showed fat volume absorption of up to 82%. 36 Hill et al 37 demonstrated acute inflammation and necrosis 48 hours after injection in canines. Neovascularization is necessary for necrosis prevention. Nishiyama et al 28 studied the micro environment of the implant and found vascular endothelial growth factor–positive cells in the connective tissue surrounding the graft on days 7 and 30. Nevertheless, it was reported that 30% to 40% of patients will eventually require an additional intervention following fat injection. 38 In all of our cases, we overinjected about 50% more than needed to achieve closure. This may also explain why none of our cases required a repeated intervention.
For a demonstrative purpose, one of the participants in our cohort underwent computed tomography (CT) of the neck 1.5 years after injection because of posterior neck pain (unrelated to this study). The long-term integration of adipose graft in the larynx of this patient is demonstrated by her CT images on Figure 4 .
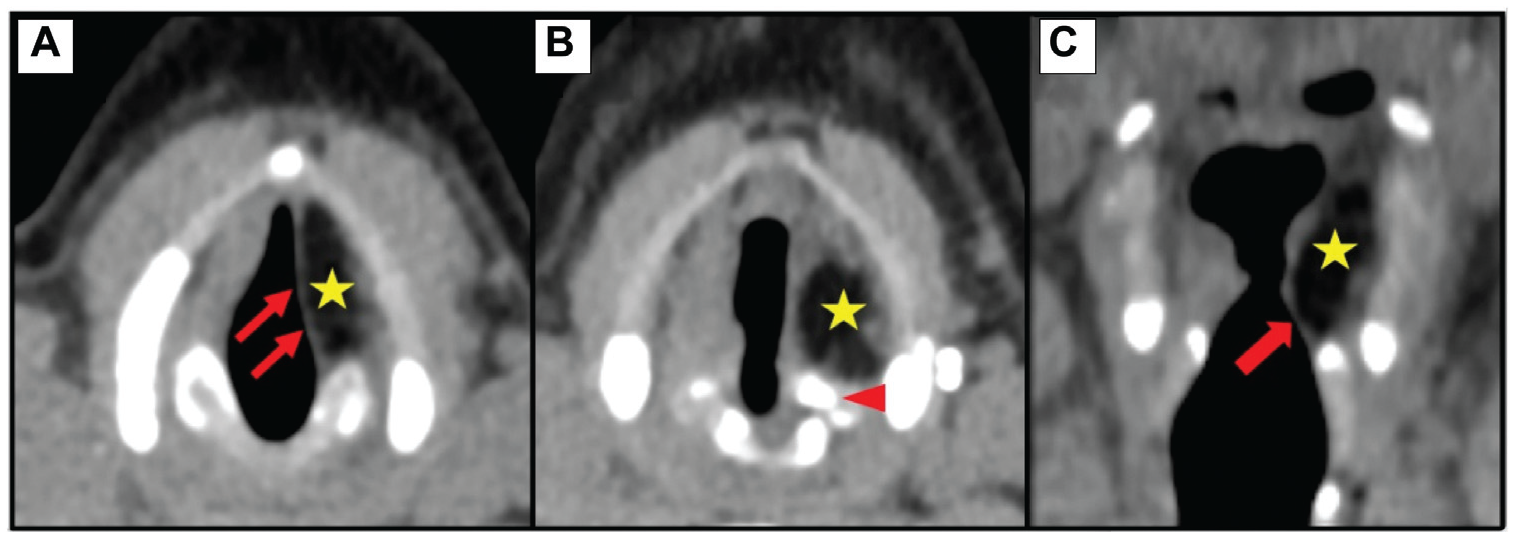
Computed tomography 1.5 years after left fat augmentation for paralysis. Adipose graft (star). (A, B) Axial, medialized vocal fold (arrows), repositioned arytenoid (arrowhead). (C) Coronal, conus elasticus angle on the left (arrow) is comparable with the right.
In our study, fat augmentation for UVFP delivered more substantial improvement in comparison with other etiologies. Specifically, for vocal frequency range, augmentation for UVFP resulted in an extended range, whereas augmentation for scar or atrophy resulted in the narrowing of the vocal range. Medialization in UVFP with relative preservation of normal VF vibratory layers probably allows for much better vocal function. In UVFP, when glottic insufficiency is corrected, compensatory mechanisms such as activation of the cricothyroid muscle are unnecessary, allowing for a wider range of frequencies. On the other hand, when insufficiency is associated with scarring, restoration of glottal closure may trade breathiness with further limited vibration. This may explain the reduced frequency range in this subgroup of patients; nevertheless, these patients did improve in other measures.
In our study, cases of UVFP or atrophy were injected into the paraglottic space, deep to the ligament and posterolateral to the vocal process for optimal medialization. 25 In selected scarred or sulcus cases, we also injected into the superficial subepithelial plane. As demonstrated by Chan and Titze, 39 fat bears viscous properties similar to those of the human lamina propria and therefore may serve as a substitute for vibratory tissue; yet, in our study, injection to the superficial layers of the VF failed to provide beneficial predictive outcomes. This phenomenon was described previously. Gray et al 40 discussed transoral fat implantation into the superficial layers for vibratory restoration and described migration of the implant to the superior aspect of the VF with subsequent symptoms relapse. They therefore developed the minithyrotomy technique, aiming for placement of fat graft in the inferior medial aspect of the VF.
Our study has several limitations. The population was relatively small with heterogenic etiologies for glottic insufficiency. Not all 22 patients completely complied with the study protocol: 21, 20, 17, and 18 patients completed the 3-month, 1-year, 2-year, and 3-year follow-up measures, respectively. Importantly, patients who failed to arrive to early follow-up appointments did later adhere to future follow-ups and vice versa (Supplement Figure S1). To overcome this difficulty, patients’ scores were specifically compared with their own preoperative scores for each measure and for each postoperative time point. Thus, we were able to demonstrate statistically significant, long-term differences compared with the preoperative findings.
Our study presents the favorable outcome of fat injection. Nevertheless, the physiological potential of this treatment is not fully understood. Injecting a tissue graft into a remote area in the body initiates a cascade of effects that should be further investigated. Fat implantation promotes vascular proliferation and involves an exchange of agents with the surrounding tissue; these processes influence the tissue’s bulkiness, stiffness, and vibratory capabilities, which may either benefit or impair normal function. Further studies are required to understand the effects of fat on the accepting tissue and ways to further improve it, for instance using the stem cells within the graft to improve the vibratory function of scarred VFs.
Conclusions
With proper patient selection and a strict technique of harvesting, preparation, and injection, fat augmentation is suitable for long-term relief of glottic insufficiency. Fat injection may achieve gap closure and with intact vibratory layers may also result in improved vibration. The best outcomes are achieved in patients with UVFP. Unlike other injectable materials, fat augmentation should be considered a durable, long-term treatment option for glottic insufficiency.
Supplemental Material
Supplement_figure_1_-revised – Supplemental material for Vocal Fold Fat Augmentation for Atrophy, Scarring, and Unilateral Paralysis: Long-term Functional Outcomes
Supplemental material, Supplement_figure_1_-revised for Vocal Fold Fat Augmentation for Atrophy, Scarring, and Unilateral Paralysis: Long-term Functional Outcomes by Yonatan Lahav, Liron Malka-Yosef, Yael Shapira-Galitz, Oded Cohen, Doron Halperin and Hagit Shoffel-Havakuk in Otolaryngology–Head and Neck Surgery
Footnotes
This article was presented as a podium presentation at the ABEA annual meeting at COSM; April 30–May 3, 2019; Austin, Texas.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.