
Abstract

Guidelines have been written during the coronavirus disease 2019 (COVID-19) pandemic to guide management of tracheostomy, particularly when and how to perform it. In the early absence of systematic data from the confounding clinical symptomatologies arising from this novel virus, these guidelines represent the consensus of experts based on opinion and historical experience. Nearly all, including 2 published in this journal, advise avoiding or delaying tracheostomy, because the risk of transmission of disease to surgeons, nurses, and ancillary staff is presumed high, as COVID-19 airway secretions are presumed to be unusually virulent.1,2
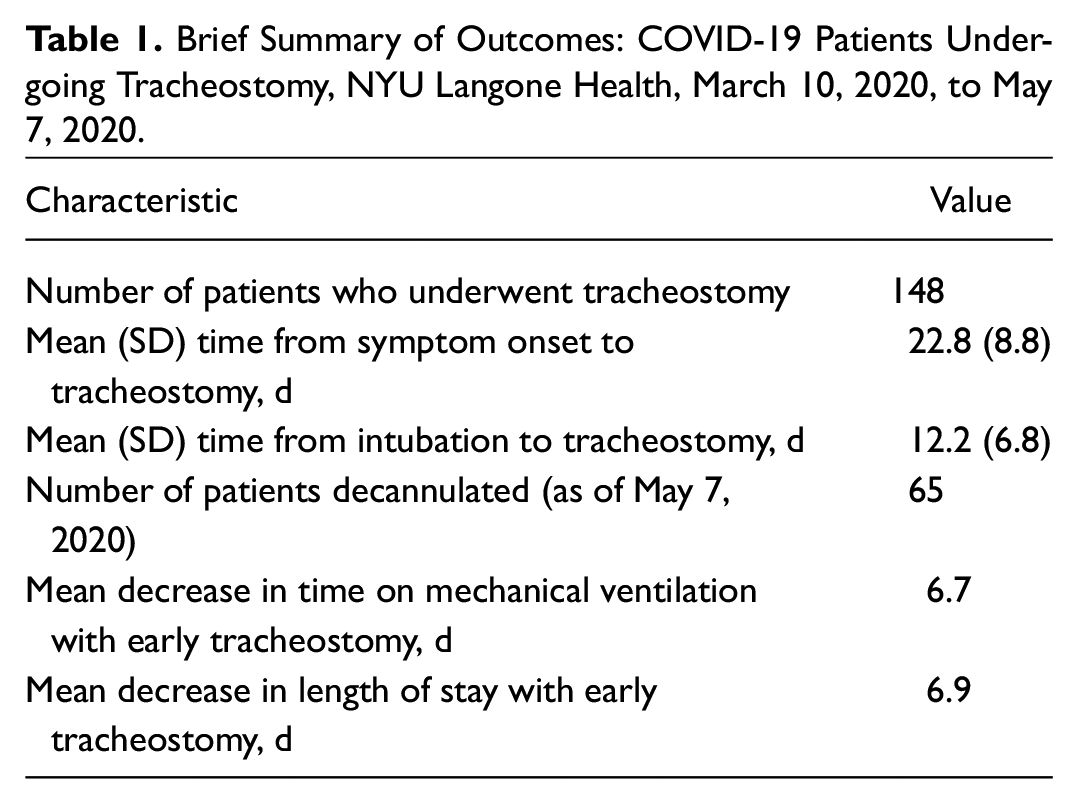
We respectfully disagree with recommendations to delay tracheostomy, or to make it a “rare event,” in the management of COVID-19 patients. We analyzed our data from the first 2 months of the pandemic in New York City, from 148 patients who underwent tracheostomy at this institution. These findings bear highlighting:
The mean (SD) time from endotracheal intubation to tracheostomy was 12.2 (6.8) days; the mean (SD) time from symptom onset to tracheostomy was 22.8 (8.8) days. Emerging evidence indicates that virulence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) peaks at 2 to 0 days prior to symptom onset and decreases thereafter. 3 Therefore, it is not clear that tracheostomy even in a “early” period following intubation is uniquely risky; by 12 days from intubation, or 22 days from symptom onset, infectivity of secretions is likely to be markedly diminished.
Early tracheostomy (within 10 days of intubation) decreased time to discontinuing mechanical ventilation by a mean of 6.7 days (P = .016) and decreased overall length of stay by mean of 6.9 days (P = .005) ( Table 1 ).
No surgeons were infected with COVID-19 as a direct result of performing tracheostomy.
Brief Summary of Outcomes: COVID-19 Patients Undergoing Tracheostomy, NYU Langone Health, March 10, 2020, to May 7, 2020.
Systematic reviews in this journal have suggested benefit to early tracheostomy in non-COVID-19, critically ill patients and that delaying tracheostomy increases the incidence of long-term airway stenosis.4,5 We continue to operate with the belief, and increasingly the data, that the virology and clinical course of COVID-19 do not indicate departure from standard best practices in the timing and management of tracheostomy. We submit that the discussion about appropriate timing of tracheostomy be informed and expanded by emerging findings about timelines of virulence and situated in the larger context of a patient’s symptom trajectory, with unwavering respect for the health and safety of our colleagues.