
Abstract
Objective
To describe the impact of vestibular dysfunction on gross motor development in children with hearing loss.
Data Sources
MEDLINE (PubMed), Embase (Elsevier), Web of Science (Clarivate), and the Cumulative Index of Nursing and Allied Health Literature (EBSCO).
Review Methods
A systematic review was reported in concordance with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses). Articles on children with hearing loss who underwent at least 1 instrumented measure of vestibular function and had gross motor milestones assessed were included. The Downs and Black checklist was used to assess risk of bias and methodological quality.
Results
Eleven articles were included in the systematic review. Three articles stratified quantitative results of gross motor milestone acquisition by severity of vestibular impairment. Over half of studies were case series published within the last 5 years. This systematic review showed that children with hearing loss and severe, bilateral vestibular dysfunction demonstrate delayed gross motor milestones. However, it was difficult to draw conclusions on whether milder forms of vestibular dysfunction significantly affect gross motor milestone acquisition in children with hearing loss. The reason is that most studies were of low to moderate quality, used different assessment methods, and contained results that were descriptive in nature.
Conclusions
This emerging area would benefit from future research, such as higher-quality studies to assess vestibular function and gross motor milestones. This would allow for better characterization of the impacts of vestibular impairment, especially milder forms, in children with hearing loss.
The vestibular system is critical for providing sensory input necessary to maintain gaze stabilization during head motion. It is also an essential component of the balance system. The impacts of vestibular dysfunction have been well described in the adult population. Specifically, individuals with vestibular dysfunction commonly report symptoms of vertigo, dizziness, unsteadiness, and falls.1-4 Less is known about congenital or early-onset vestibular dysfunction in children, yet there is a growing body of literature examining pediatric vestibular dysfunction. Recent epidemiologic studies have found a prevalence of vestibular dysfunction in the general pediatric population of 5% to 8%,5-7 although 1 study found a much lower prevalence at 0.4%. 8 This discrepancy could be due to the manner in which vestibular dysfunction was defined. The difference between these estimates highlights a challenge with our understanding of vestibular dysfunction in children: there are many complaints suggestive of possible vestibular dysfunction, such as dizziness or balance problems, but these symptoms are not specific to vestibular dysfunction.
The differences among the aforementioned studies suggest that we do not have a complete understanding of how vestibular dysfunction presents in children. Young children may not be able to adequately verbalize symptoms such as vertigo or disequilibrium. 9 Animal research has shown that early vestibular dysfunction can result in worse motor performance due to poor postural and movement control.10,11 In patients with congenital or early-onset vestibular dysfunction, the absence of adequate balance and postural control may impair gross motor development in early childhood. Several studies have used acquisition of commonly assessed gross motor milestones as a clinical proxy for vestibular dysfunction.12-14 Some studies examine the average ages at which head control, sitting, and independent walking are achieved, while others assess the proportion of children who acquire these developmental milestones at an expected versus delayed age. World Health Organization normative values for typically developing children are 6.0 ± 1.1 months (mean ± SD) for sitting and 12.1 ± 1.8 months for independent walking. 15 There is less consensus for the normal age of head control, although the American Association of Pediatrics says that failure to achieve head control by 4 months is abnormal. 16
While vestibular dysfunction in children may have various causes, hearing loss is a particularly associated symptom.17,18 It may be expected that congenital/early acquired sensorineural hearing loss would have high rates of co-occurring vestibular dysfunction given anatomic and embryologic connections, as well as closely related physiology. 19 Estimates of the prevalence of concomitant vestibular dysfunction among children with sensorineural hearing loss range from 15% to 85%.12,13,17,18,20 This wide range may be due to differences in defining what constitutes vestibular dysfunction, as discussed previously, or it could be due to variation in testing methods or interpretation of test results. Some etiologies of hearing loss may be associated with different rates of vestibular dysfunction or concomitant neurologic and/or visual problems predisposing to balance problems. Thus, discrepancies in estimates of concomitant vestibular dysfunction in children with hearing loss among studies may actually reflect differences in the representation of hearing loss etiologies across studies.
Much of the pediatric vestibular research in children with hearing loss to date has focused on assessment methodology,21,22 prevalence of vestibular dysfunction,23,24 methodology and effectiveness of vestibular rehabilitation,25,26 and the potential effect of cochlear implantation on vestibular function.27,28 More recently, researchers have examined the impacts of vestibular loss on quality of life and functional outcomes, such as reading ability 29 and motor control.30-32 These studies are critical to understanding how vestibular dysfunction manifests in children with hearing loss. This systematic review aims to describe the current understanding of the impacts of vestibular dysfunction on gross motor development in children with hearing loss.
Methods
Systematic Literature Search
We conducted a systematic review and reported the findings in concordance with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses). 33 We searched the following databases: MEDLINE (PubMed), Embase (Elsevier), Web of Science (Clarivate), and the Cumulative Index of Nursing and Allied Health Literature (EBSCO). The search was conducted by a professional medical librarian (J.W.) and included a mix of keywords and subject headings representing “hearing loss or impairment” and “function or dysfunction,” as well as equipment-based and bedside “vestibular testing” methods. No restrictions were placed by date or language. Results were filtered to include only pediatric studies. Editorials, letters, case reports, and comments were excluded, as were animal-only studies. Case reports were defined as articles describing a single patient. We included case series of >3 patients in this systematic review. Reproducible search strategies in PubMed can be found in the Supplemental Materials (Supplemental Table S1, available online), with similar search strategies being used in other databases. The search was executed in March 2020.
All citations were imported into the online screening platform Covidence (Cochrane) via EndNote (Clarivate). Duplicate citations were automatically identified and removed by Covidence. Two reviewers independently screened each reference by title and abstract, excluding irrelevant articles that did not align with the screening criteria. If studies did not have abstracts available, they were moved to full-text review. All discrepancies regarding eligibility were resolved through adjudication by a third reviewer. The full text of articles were assessed by 2 independent reviewers with a third reviewer to adjudicate discrepancies. Full texts meeting initial criteria of having instrumented and noninstrumented measures of vestibular function in children with hearing loss were identified. Articles were separated that included gross motor milestone measures as the noninstrumented measures, and those that had other types of noninstrumented measures were excluded from this analysis.
Inclusion/Exclusion Criteria
To be included in this systematic review, articles had to meet 3 inclusion criteria.
First, the patient population had to include children with hearing loss. We defined children to be individuals ≤21 years old. If patients >21 years old were included in an article, then the data had to be clearly separable by age. The inclusion criteria of the original article had to include hearing loss, or the article had to include audiologic testing results to examine patients for hearing loss. In articles involving participants with cochlear implants, evaluation of vestibular function had to be performed preimplantation.
Second, all children had to have at least 1 instrumented test of vestibular function. Possible vestibular tests included electronystagmography, videonystagmography, caloric tests, video head impulse test, vestibular evoked myogenic potential, subjective visual vertical, instrumented dynamic visual acuity, and/or rotary chair.
Last, children had to have gross motor milestones assessed through a questionnaire, parental report, or standardized measure such as the Peabody Developmental Motor Scales 2. 34
Articles were omitted if the patient population was limited exclusively to children with specific syndromes/diagnoses that had multiple sensory system involvement (eg, Usher syndrome) or with known concomitant neurologic problems. Articles were also excluded at the full-text stage if written in a language other than English and a translation could not be obtained.
Data Extraction and Risk-of-Bias Assessment
Extracted data included study characteristics, population, and results from each article. Study characteristics included design, country in which the study was conducted, and the overall stated goals of the study. Study population details included participant age, sex, number of participants, vestibular tests conducted, gross motor milestones measured, and further information about participants’ hearing loss. Hearing loss characteristics included type, laterality, severity, etiology, and method of measurement. Information about controls and inclusion of patients with cochlear implants was also extracted. If patients undergoing cochlear implantation were included, then vestibular assessment had to have occurred prior to cochlear implantation. Study results extracted included vestibular testing methods and results as well as information on acquisition of gross motor milestones. While not required by the PRISMA reporting standards, we opted to have 2 authors independently extract data and perform the risk-of-bias assessments, with a third author available if necessary to resolve conflicts. We chose to do so under the recommendation of our medical librarian to increase accuracy and lessen the likelihood of any errors.
The Downs and Black checklist was used to assess the risk of bias of the articles. 35 This is a 27-item checklist on methodological quality, with questions focusing on reporting, external validity, bias, confounding variables, and power. It can be used for randomized and nonrandomized studies. All studies were independently assessed by 2 reviewers, with conflicts subsequently resolved between themselves. Reproducible strategies for risk-of-bias assessment are presented in the Supplemental Materials (Supplemental Table S2, available online).
Results
Literature Search Results
The database search yielded 2377 studies. After duplicates were removed, 1458 articles were screened by title and abstract, and 109 full-text studies were reviewed for eligibility. A total of 11 studies were identified as meeting inclusion/exclusion criteria for data extraction. The PRISMA study inclusion chart is presented as Figure 1 .
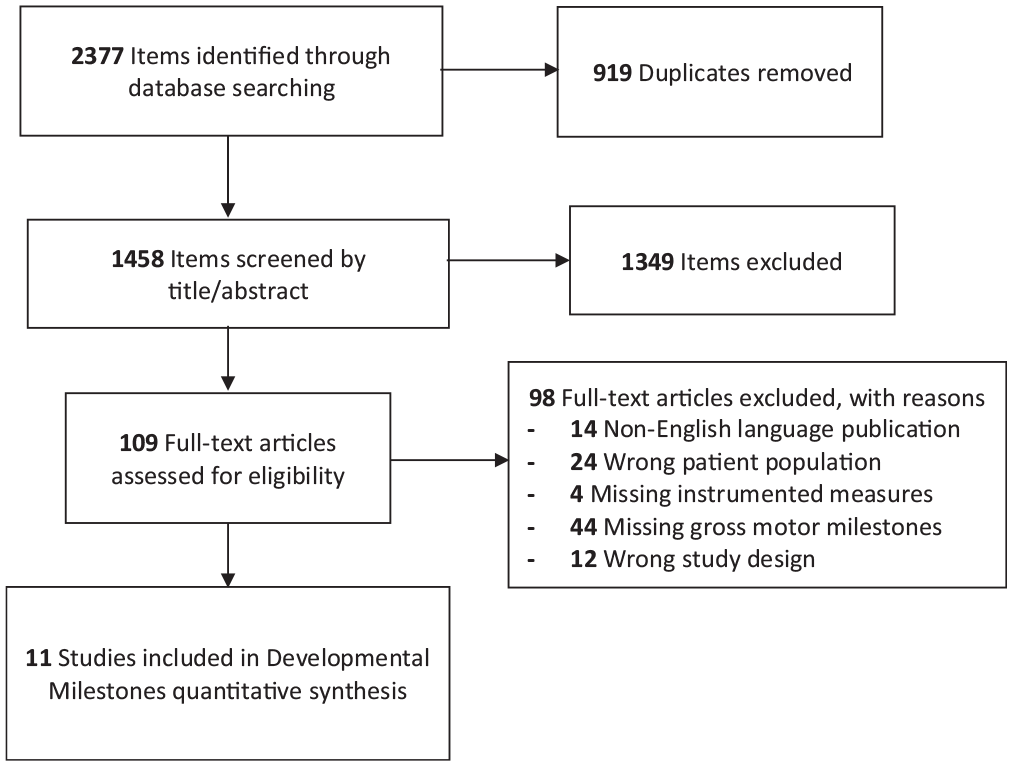
Article selection/study inclusion flowchart.
Study Characteristics
Of the 11 studies, 6 were published between 2015 and 2020 ( Table 1 ). All but 1 study were case series. The studies were conducted in 5 countries (Belgium,28,36 France, 37 Japan,13,30,31,38,39 United Kingdom, 40 and United States12,32), with several articles having overlapping groups of authors. For example, De Kegel and Maes were the second author on each other’s first author article, both with the same last author.28,36 Similarly, Kaga is an author of 4 studies, once as first author and thrice as last author.13,31,38,39
Study Characteristics of the 11 Articles Included in the Systematic Review.
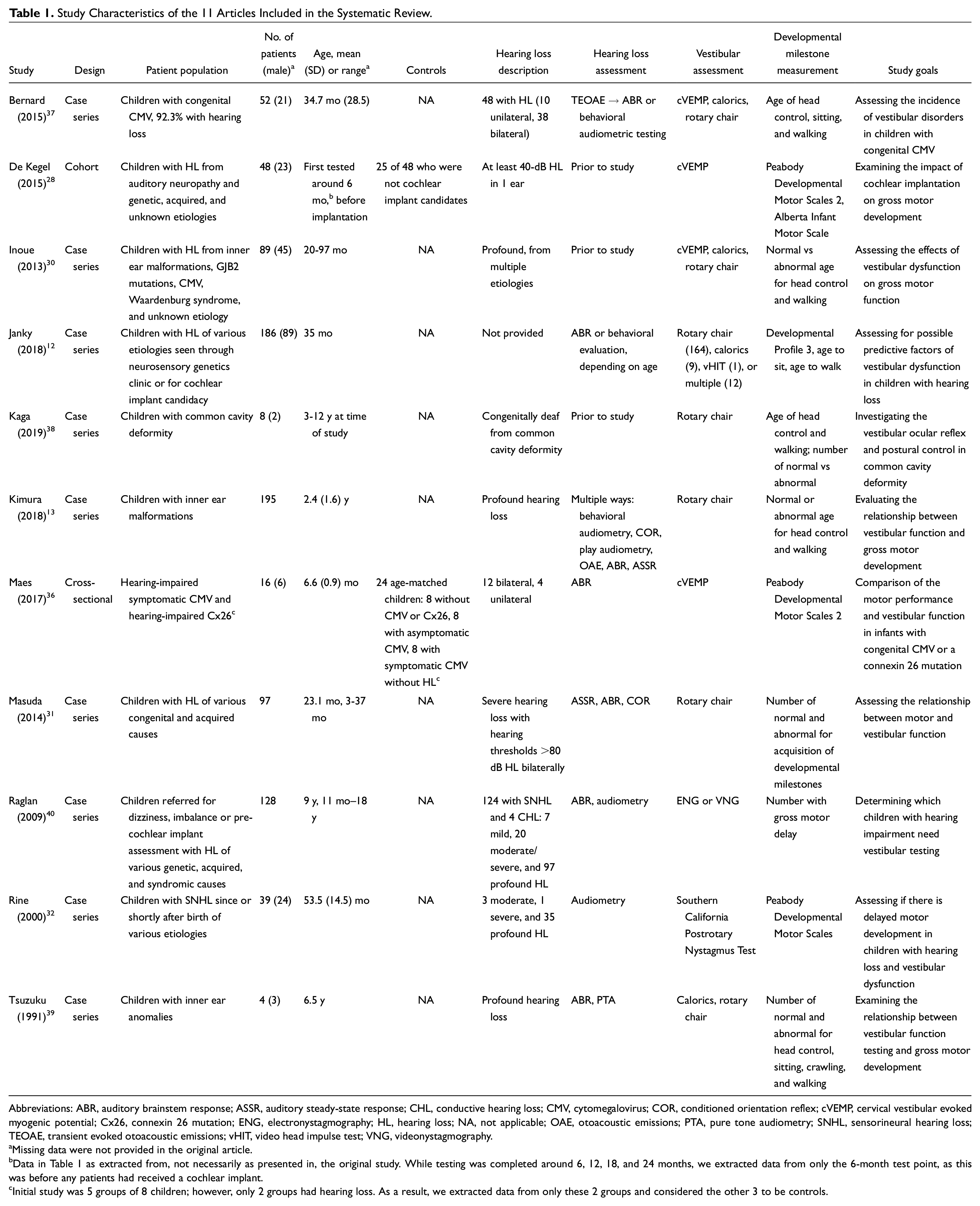
Abbreviations: ABR, auditory brainstem response; ASSR, auditory steady-state response; CHL, conductive hearing loss; CMV, cytomegalovirus; COR, conditioned orientation reflex; cVEMP, cervical vestibular evoked myogenic potential; Cx26, connexin 26 mutation; ENG, electronystagmography; HL, hearing loss; NA, not applicable; OAE, otoacoustic emissions; PTA, pure tone audiometry; SNHL, sensorineural hearing loss; TEOAE, transient evoked otoacoustic emissions; vHIT, video head impulse test; VNG, videonystagmography.
Missing data were not provided in the original article.
Data in Table 1 as extracted from, not necessarily as presented in, the original study. While testing was completed around 6, 12, 18, and 24 months, we extracted data from only the 6-month test point, as this was before any patients had received a cochlear implant.
Initial study was 5 groups of 8 children; however, only 2 groups had hearing loss. As a result, we extracted data from only these 2 groups and considered the other 3 to be controls.
The participant characteristics varied. Some studies focused on particular anatomic malformation (common cavity deformity, 38 inner ear anomalies 39 ), children with a particular disease (cytomegalovirus [CMV],36,37 connexin 26 mutation 36 ), those being seen prior to cochlear implant without regard for etiology,12,28,30,40 and/or children who were simply being followed for hearing loss.13,31,41 Sample sizes ranged from 4 participants 39 to 195 participants. 13 Only 2 studies included a control group.28,36 Four studies included patients who were candidates for cochlear implantation,12,30,37,40 and 3 included patients who underwent cochlear implantation.28,31,38 However, data were extracted only if gross motor milestones were assessed prior to cochlear implantation.
The majority of children had sensorineural hearing loss, although 1 study included 4 of 128 participants with conductive hearing loss. 40 In the Bernard et al study, 37 the focus was on patients with CMV, and 92.3% had hearing loss. Children with and without hearing loss were pooled; therefore, a small percentage of children without hearing loss were included in this study ( Table 1 ).
Hearing loss severity ranged from moderate to profound across the studies and was measured with a variety of conventional assessment methods, including otoacoustic emissions, evoked potentials (auditory brainstem response, auditory steady-state response), and behavioral audiometry (conditioned play or conventional). Vestibular testing ranged from a single test for all participants to a battery of tests. In some studies with a battery approach to testing, the test battery varied by age or other criteria, such as patient cooperation. 21 The most common testing measures were cervical vestibular evoked myogenic potential, rotary chair, and calorics. Most results were reported as the number of participants with normal or abnormal findings, with abnormal findings often being reported descriptively by laterality (left, right, or bilateral) or severity of dysfunction (eg, mild vs severe). Several studies had missing data (ie, they did not perform the battery of tests on all participants).
Common methods to describe gross motor milestones included age at development of head control, sitting, and independent walking; number of children with normal or abnormal ages for achieving head control, sitting, and walking; and scores on standardized measures of development, such as the Peabody Developmental Motor Scales 2. Reporting of the developmental milestones was variable: researchers presented results as mean and standard deviation, assigned participants into normal and abnormal groups based on age of gross motor milestone acquisition, reported scores on standardized scales of gross motor milestones, or detailed milestones only in subsets of the study sample. About half the studies had the explicit goal of determining the association between vestibular function and gross motor development ( Table 1 ).
Vestibular Function Testing and Acquisition of Developmental Milestones
A summary of vestibular function testing results and acquisition of gross motor milestones by article is presented in Table 2 . Most studies had a mix of participants with normal and abnormal vestibular function as well as normal and abnormal acquisition of gross motor milestones. Although few studies conducted direct correlational/association analyses, many suggested that there was some association between vestibular function and acquisition of gross motor milestones. In most cases, these conclusions were reached by comparing children with normal vestibular function and those with severe, bilateral dysfunction.
Study Vestibular Testing and Developmental Milestone Results.
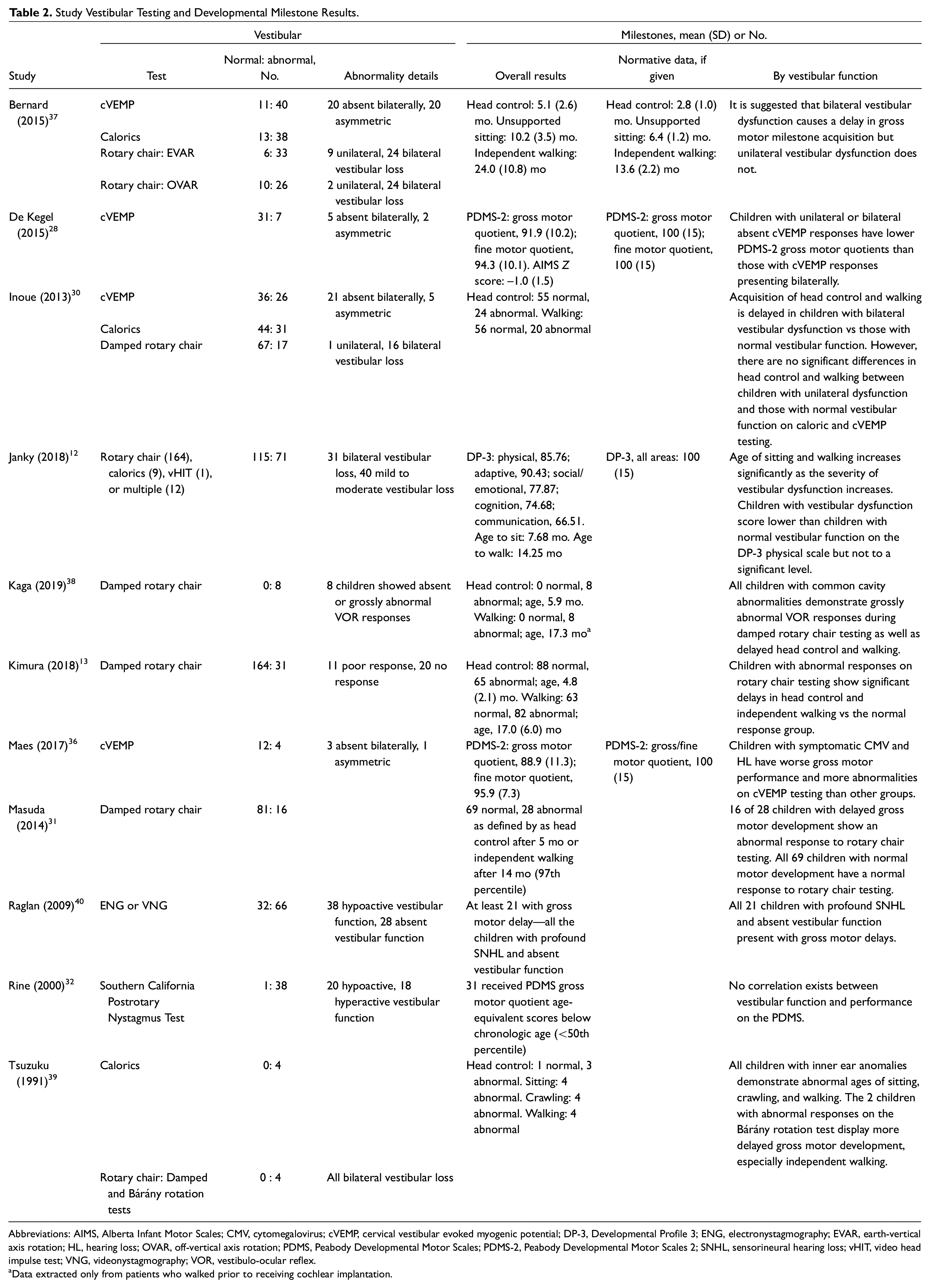
Abbreviations: AIMS, Alberta Infant Motor Scales; CMV, cytomegalovirus; cVEMP, cervical vestibular evoked myogenic potential; DP-3, Developmental Profile 3; ENG, electronystagmography; EVAR, earth-vertical axis rotation; HL, hearing loss; OVAR, off-vertical axis rotation; PDMS, Peabody Developmental Motor Scales; PDMS-2, Peabody Developmental Motor Scales 2; SNHL, sensorineural hearing loss; vHIT, video head impulse test; VNG, videonystagmography; VOR, vestibulo-ocular reflex.
Data extracted only from patients who walked prior to receiving cochlear implantation.
While many studies provided qualitative descriptions, 3 stratified quantitative gross motor milestone data by vestibular function testing results ( Table 3 ). In general, these studies showed delays in acquisition of head control,13,30 independent sitting, 12 and/or walking12,13,30 as vestibular function increased in severity. Children with normal vestibular testing results generally met milestones earlier than those with mild to moderate or unilateral dysfunction, and both those groups met milestones on average earlier than those with bilateral or severe vestibular dysfunction. Janky et al 12 also showed a decrease in the Developmental Profile 3–Physical subscore, a standardized checklist for parents assessing for physical developmental delays, as vestibular function worsened.
Quantitative Gross Motor Milestones by Vestibular Function Results. a
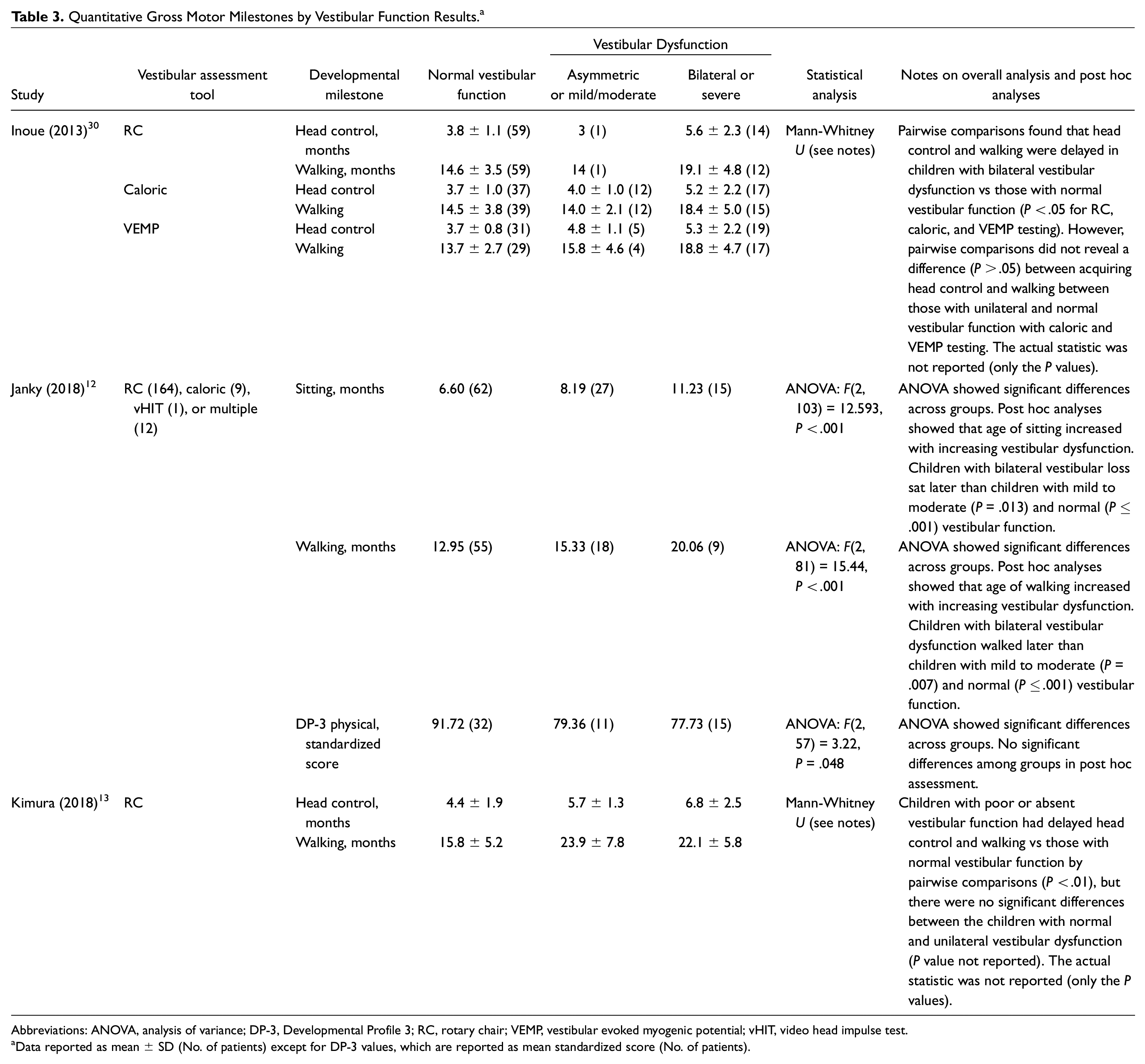
Abbreviations: ANOVA, analysis of variance; DP-3, Developmental Profile 3; RC, rotary chair; VEMP, vestibular evoked myogenic potential; vHIT, video head impulse test.
Data reported as mean ± SD (No. of patients) except for DP-3 values, which are reported as mean standardized score (No. of patients).
Risk-of-Bias and Methodological Quality Assessment
The risk-of-bias assessment for the studies is presented in Table 4 . There was wide variability in the risk of bias and methodological quality among the studies included. Some items on the Downs and Black risk-of-bias assessment were consistently present or nearly consistently present. These included clear objectives and outcome measures, as well as a description of patient characteristics and interventions. However, some items were inconsistently or questionably present across studies. These included blinding of reviewers to participant group, appropriate adjustment for confounding variables, and whether or not the recruitment pool and/or study participants were representative of the larger population. Nearly all studies reviewed did not include power analyses in their statistical methods. Overall, results of the Downs and Black risk-of-bias assessment suggest that most studies were of low to moderate quality. A meta-analysis was not performed given the heterogeneity and low to moderate quality of the studies.
Quality Appraisal of Articles per the Downs and Black Risk-of-Bias Assessment. a
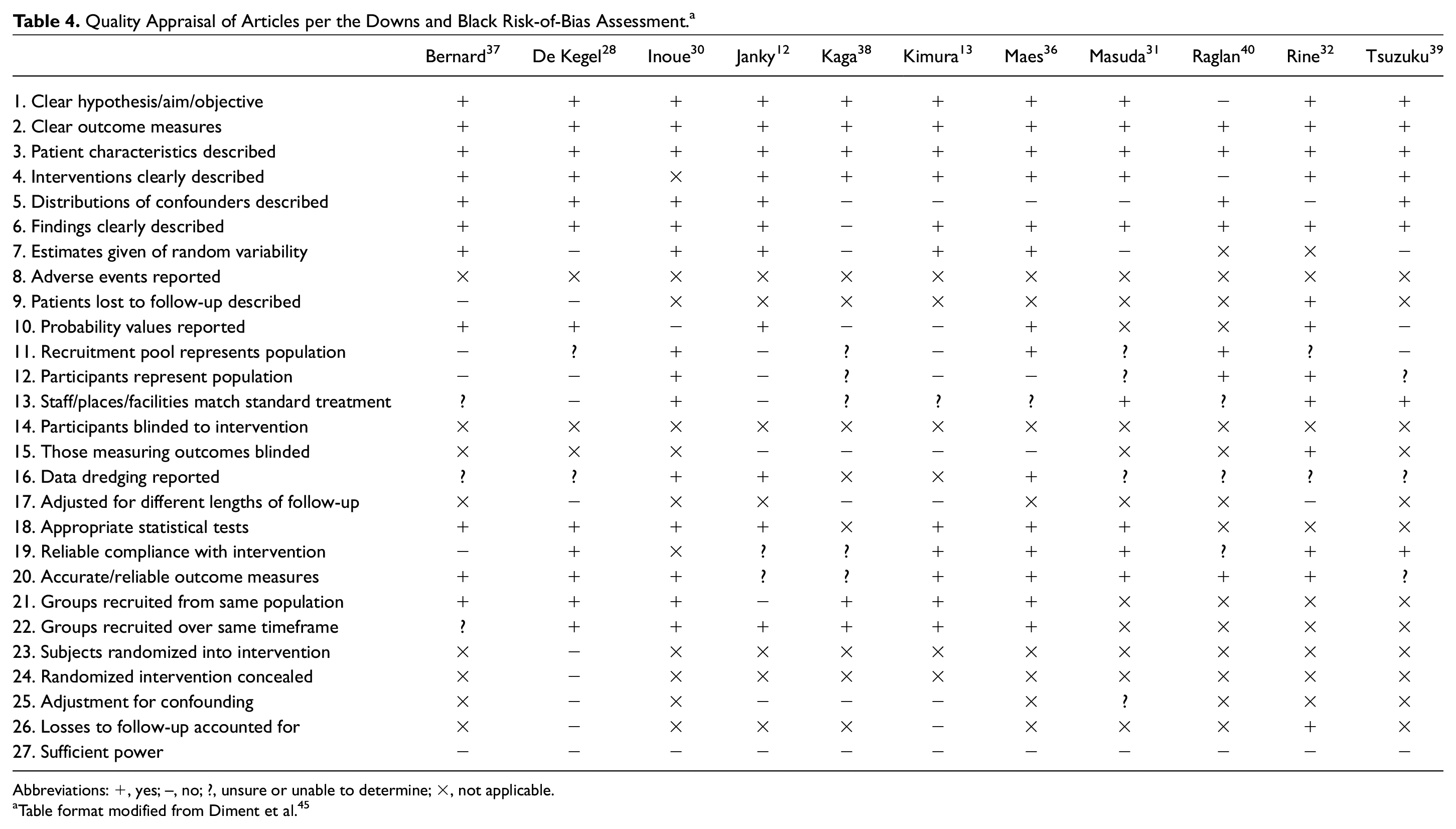
Abbreviations: +, yes; –, no; ?, unsure or unable to determine; ×, not applicable.
Table format modified from Diment et al. 45
Discussion
The vestibular system helps to maintain clear vision when a person is in motion, and it provides strong internal signals to maintain balance and aid in coordination. In adults, vestibular dysfunction can cause dizziness, visual dysfunction, or balance problems. However, considerably less is known about how vestibular dysfunction in children affects their daily life and development. This could be in part because young children lack the verbal communication skills needed to articulate their symptoms. To complicate matters, children who have experienced these symptoms from birth or infancy may not recognize their symptoms as abnormal or may have learned to compensate for their dysfunction. 42 Epidemiologic evidence in children with hearing loss suggests that anywhere from 15% to 85% of children with congenital or early-onset hearing loss may have vestibular impairment.17,18 This systematic review sought to summarize the impact of vestibular dysfunction on developmental milestones in children with hearing loss.
Gross Motor Development in Children With Hearing Loss and Vestibular Dysfunction
This study examined the association between vestibular function and gross motor development in children with hearing loss. Across 11 studies identified through this systematic review, 10 showed evidence for an association between vestibular function and acquisition of gross motor milestones. This conclusion was often reached by comparing children with hearing loss and normal vestibular function and those with severe bilateral vestibular dysfunction. In children with poorer vestibular function, these studies often found delayed acquisition of milestones (eg, achieving head control, sitting upright, or independent walking) or lower scores on standardized scales of gross motor performance (eg, Peabody Developmental Motor Scales 2, Developmental Profile 3).
The conclusions that most studies reached were based on broad categorization of vestibular function (ie, normal vestibular function, unilateral or mild dysfunction, and bilateral or severe dysfunction). While some studies compared milder levels of vestibular dysfunction with normal and severely abnormal vestibular function, few reported whether they had adequate statistical power to ascertain small differences between groups. The limited nature of the reported data precludes insight into whether milder forms of vestibular dysfunction significantly affect gross motor acquisition. It appears that children with hearing loss who also have severe bilateral vestibular dysfunction demonstrate delayed gross motor milestones. However, it is unclear whether there is a dose-dependent impact of vestibular dysfunction on gross motor milestone acquisition.
Methodological Limitations in Existing Literature
The inability to draw conclusions in the milder vestibular dysfunction group was typically a result of limitations in methodology as identified in the Downs and Black quality assessment ( Table 4 ). Studies were frequently case series with relatively small sample sizes and low to moderate quality based on the risk-of-bias assessment. As a result, there is a significant chance for bias to affect the results of this systematic review. Selection bias is a particular concern, and it is hard to generalize these findings to children with hearing loss as a general cohort.
The studies used different assessments or batteries of tests for measuring vestibular function and gross motor performance, making comparison of results challenging. Many studies did not collect vestibular and gross motor measures on all participants. This made sense for individual studies, as they involved children of different age ranges and had inclusion criteria ( Table 1 ) that would make certain testing measures more appropriate. However, this limits the ability to draw conclusions about the effects of vestibular dysfunction on gross motor development in children with hearing loss. Similarly, the variability of testing strategies prevents determination of the relative impact of certain patterns of vestibular impairment (eg, otolith vs canal) on gross motor development. Studies often had a preponderance of children in the severe bilateral dysfunction group relative to a milder unilateral impairment group. When 3 groups of varying vestibular impairment severity were available, the sample sizes were small, and the studies did not always report whether there was adequate power to discern differences among the groups. Prior research has indicated that the rates of severe bilateral vestibular loss should be similar to the rates of mild unilateral vestibular dysfunction in children. 43
Future Research Needs
As a whole, this area of research is still emerging. Over half of the studies included in this systematic review were published in the last 5 years (ie, 2015-2020; Table 1 ). Much of the work has been published by a few specific research groups and therefore has overlapping groups of authors. Only a few of the studies in this review were designed to examine vestibular function and its impacts on gross motor milestone acquisition in children with hearing loss.13,30-32,39 Four articles described observational studies or case series on a particular subpopulation with hearing loss in which vestibular function was characterized and motor outcomes measured.36-39 One study included some children with normal hearing, 37 which was not the intended target population for this study. While our systematic review excluded studies on syndromes that affect multiple sensory systems, additional work is needed focusing on multisensory impairments and controlling for common comorbid conditions that also likely contribute to motor milestone development and balance such as visual impairment.
Future work that describes relationships in the context of degree of hearing loss and/or etiology may help to better inform screening processes and clinical pathways for those children at greatest risk for vestibular impairment and delayed motor milestones. Although many of the included articles described etiologies that were included in their populations, they did not necessarily report their findings by etiology. Seven articles in our systematic review examined particular etiologies of hearing loss (ie, inner ear anomalies,13,38,39,44 CMV,36,37,44 or connexin 26 mutations36,40,44). The articles on CMV and inner ear anomalies had mixed conclusions on whether these etiologies of hearing loss were consistently associated with vestibular dysfunction and gross motor delays. In contrast, all 3 articles with connexin 26 mutations found little vestibular dysfunction, with only Inoue et al 44 finding 1 of 13 patients with connexin 26 mutations to have delayed head control and none to have delayed independent walking. However, most studies did not have a sufficient number of participants to make meaningful conclusions about the effects of etiology or severity of hearing loss on vestibular dysfunction and gross motor milestone acquisition.
This research area would benefit from future studies to help inform clinical practice. In particular, there is a need for higher-quality studies, as demonstrated by the results of the Downs and Black quality assessment ( Table 4 ). Given that many of these studies were case series or observational studies, it is important that future research incorporate more rigorous sampling methods and blinding of the researchers. Additionally, studies that are designed to control for common confounding factors are needed. Larger studies with more power could be helpful in making statistically significant conclusions about differences in gross motor development among children with hearing loss who present with different levels of vestibular dysfunction. In addition, developing a minimum standard battery to assess vestibular loss and gross motor development across children with hearing loss could be helpful in comparing results across studies and increase the ability to draw more consistent conclusions about vestibular dysfunction in children with hearing loss. Furthermore, studies such as a longitudinal natural history study could be helpful in understanding how vestibular dysfunction and gross motor development affect children with hearing loss over time. Many of these studies were cross-sectional, and only one 28 followed patients over time. As a result, it is difficult to say how vestibular dysfunction affects children with hearing loss in their gross motor development over time. Moreover, it would be helpful to know how delayed gross motor development early in life affects children with hearing loss in other domains of development over time, such as academic success, ability to socialize, and participation in organized activities (eg, sports). This information could be helpful to characterize the need, or lack thereof, for targeted vestibular intervention. Emerging evidence from a 2019 systematic review by Melo and colleagues showed that vestibular rehabilitation exercise programs likely improve the balance and posturomotor control in children with sensorineural hearing loss; however, the current literature is of low quality. 25
Conclusion
The role that vestibular dysfunction plays on the acquisition of gross motor milestones in children with hearing loss and the long-term physical impact of this vestibular dysfunction are emerging but important areas of research. This systematic review identified 11 studies that examined the association between vestibular dysfunction and gross motor development in children with hearing loss. The majority of the studies showed that delayed motor milestone acquisition was associated with severely abnormal vestibular testing results. However, concerns about the quality of the studies and variability in assessment methods pose challenges in drawing more detailed conclusions about gross motor milestones and vestibular testing results in children with hearing loss. Future research with more rigorous study methodology and larger sample sizes is needed to further our understanding of the impact that vestibular dysfunction has on the acquisition of gross motor milestones in children with hearing loss.
Supplemental Material
sj-docx-1-oto-10.1177_0194599820983726 – Supplemental material for Vestibular Dysfunction and Gross Motor Milestone Acquisition in Children With Hearing Loss: A Systematic Review
Supplemental material, sj-docx-1-oto-10.1177_0194599820983726 for Vestibular Dysfunction and Gross Motor Milestone Acquisition in Children With Hearing Loss: A Systematic Review by Anisha Singh, Eileen M. Raynor, Janet W. Lee, Sherri L. Smith, Hannah Heet, Doug Garrison, Jordan Wrigley, David M. Kaylie and Kristal M. Riska in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-2-oto-10.1177_0194599820983726 – Supplemental material for Vestibular Dysfunction and Gross Motor Milestone Acquisition in Children With Hearing Loss: A Systematic Review
Supplemental material, sj-docx-2-oto-10.1177_0194599820983726 for Vestibular Dysfunction and Gross Motor Milestone Acquisition in Children With Hearing Loss: A Systematic Review by Anisha Singh, Eileen M. Raynor, Janet W. Lee, Sherri L. Smith, Hannah Heet, Doug Garrison, Jordan Wrigley, David M. Kaylie and Kristal M. Riska in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
We thank Leila Ledbetter, MLIS, for her guidance and technical assistance on systematic review practices.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.