
Abstract
The aging US population requires an increasing volume of otolaryngology–head and neck surgery services, yet the otolaryngologist physician workforce remains static. Advanced practice providers (APPs), including physician assistants and nurse practitioners, improve access across the continuum of primary and subspecialty health care. The rapid growth of APP service is evidenced by a 51% increase in APP Medicare billing for otolaryngology procedures over 5 years. APPs increasingly participate in delivering otolaryngology care; however, reaping the benefits of enhanced patient access and modernizing care delivery is predicated on successful integration of APPs into practices. Few data are available on how best to incorporate APPs into team-based models or how to restructure practices to allow graduated responsibility that supports autonomy and effective teamwork. We compare national APP and physician workforce trends in otolaryngology, consider approaches to optimizing efficiency by integrating APPs, and identify opportunities for improving data collection and practice.
Keywords
The Department of Health and Human Services has projected a workforce deficit of 1620 otolaryngologist–head and neck surgeons in the United States by 2025, 1 and 1 in 5 counties has seen a recent decline in the ratio of otolaryngologists to overall population. In contrast to the relatively static otolaryngologist workforce, the advanced practice provider (APP) workforce grew approximately 35% over the past 5 years with a 51% increase in the number of unique APPs billing for common otolaryngology procedures. 2 APPs, including certified registered nurse practitioners (CRNPs) and physician assistants (PAs), are thus playing an increasingly important role in filling gaps in access to otolaryngology specialty care.
While APPs have a vital and growing role in health care delivery in otolaryngology, few data are available regarding best practices for incorporating APPs into teams. Part of the challenge in standardizing approaches lies in the diversity of practice settings, which include inpatient and outpatient care within private and academic centers. For example, the needs in a rural setting with a low density of practicing otolaryngologists may be very different from those of a large referral center seeking to coordinate multidisciplinary care or streamline inpatient care. A growing national APP footprint has practical implications for patient access, satisfaction, and care, yet challenges exist in determining the optimal integration and use of APPs in these highly variable otolaryngology practice environments.
Otolaryngology Workforce Trends
Ge et al 2 studied APP utilization trends in otolaryngology from 2012 to 2017 in the Medicare population and found that there was a 51% increase in the number of otolaryngology APPs, compared to a 2.2% increase in otolaryngology physician providers. The growing APP workforce increased its total share of both new patient visits (from 4% to 7%) and established patient visits (from 11% to 15%) during that time. Patel et al 3 similarly found a near-linear growth in number of otolaryngology APPs, with corresponding increases in total Medicare-allowed reimbursement, total number of services performed, and total number of Medicare fee-for-service patients treated by the APP workforce, particularly in regions with lower density of otolaryngologists. APP and physician workforce trends in otolaryngology are shown ( Figure 1 ).
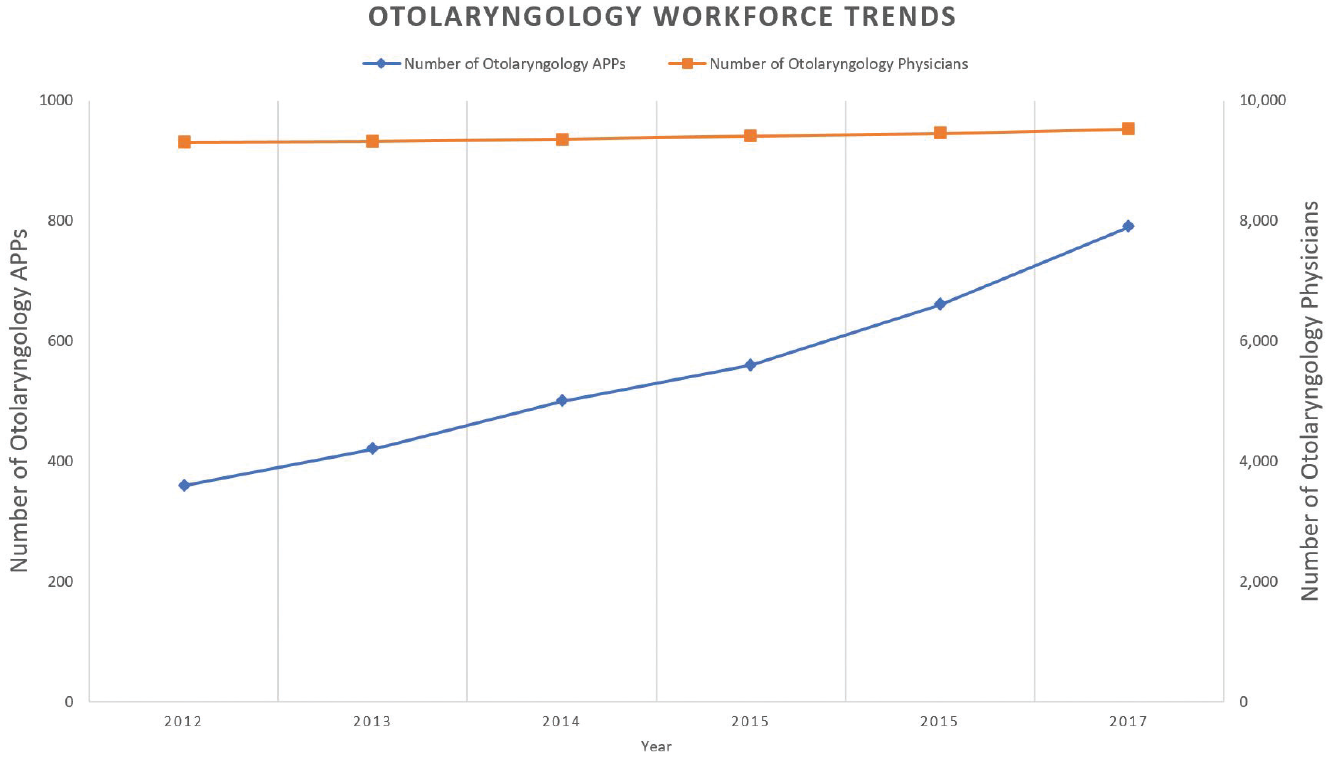
Otolaryngology workforce trends based on Association of American Medical Colleges physician specialty data report and Medicare provider utilization and payment data, 2012-2017.
Patients, physicians, and APPs may all have differing notions regarding the optimal approach to integrating APPs in patient care. Providing specialty-specific training, evaluating competency, and defining scope of practice for APPs are nuanced, with responsibility shared by both governing boards and supervising physicians. As summarized in Table 1 , CRNPs are registered nurses who have undergone additional education and clinical training at the master’s or doctoral degree level. PAs complete a 2-year master’s degree with didactic and clinical experience. CRNPs are generally governed by a joint committee between the state nursing board and medical board. PAs are governed by their respective state medical boards. These governing bodies set scope of practice standards and training requirements for allowable otolaryngologic procedures. While nurse practitioners (NPs) have independent practice authority in 22 states, NPs and PAs generally work with a supervising or collaborating physician.4-6 CRNPs and PAs both have prescribing authority and overlap in scope of practice within otolaryngology, despite differences in training and licensure.
Advanced Practice Providers’ Summary of Education, Training, and Scope of Practice.
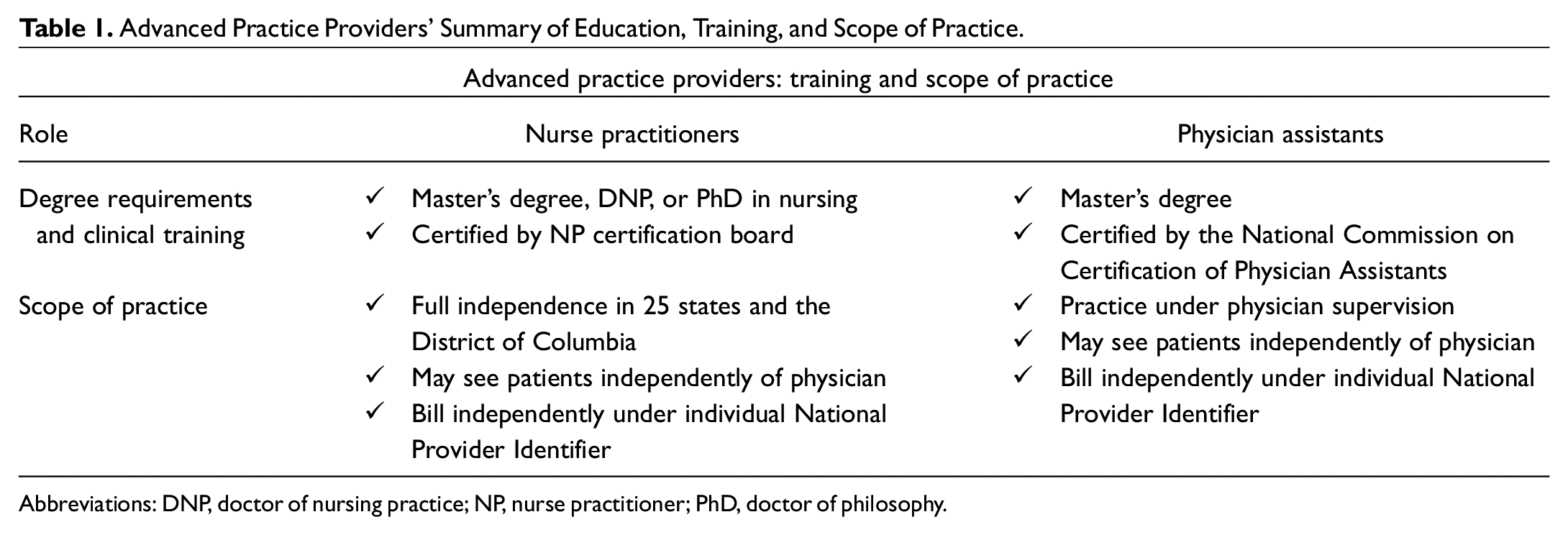
Abbreviations: DNP, doctor of nursing practice; NP, nurse practitioner; PhD, doctor of philosophy.
Optimization of APPs in Otolaryngology
Otolaryngology care increasingly occurs in the context of team-based practice. The contribution of APPs to quality of care may be evaluated using patient access and patient satisfaction metrics.5-7 For example, hiring APPs in the Dartmouth Head and Neck Tumor Clinic was associated with an increased number of new patient visits and decreased wait times while maintaining patient satisfaction and surgeon productivity. 8 Formalization of APP training and competency in otolaryngology may facilitate this type of integration into the care team. Improved outcomes data collection can better support and establish models for coordinated, team-based care from otolaryngology physicians and APPs. APPs can play a key role in managing volume efficiently, as well as diagnosing and treating a variety of otolaryngology conditions. The approach to integrating APPs should consider patient-centered factors, particularly in relation to access, as well as preferences of providers and operational efficiencies.
Many variables affect the optimal utilization and compensation of an APP within an otolaryngology practice, as well as selection of type of APP ( Table 2 ). For example, CRNPs have certifications specific to populations (eg, pediatric, adult, or general) or emphasizing inpatient vs outpatient settings, whereas PA training encompasses the general population.9,10 Compensation models may include a fixed-salary model, productivity-based compensation, or a hybrid of both. Practice models include fully integrated care teams, collaborative practice with direct supervision, semiautonomous practice, or fully independent practice models. The options are infinite, and there is no singular model that is appropriate for all practices, contexts, subspecialties, and locations. A few principles hold across settings, however. It is advantageous to (1) reduce the impact of lower reimbursement for APP vs physician care; (2) increase availability of surgeons for consults, referrals, and surgical cases; and (3) use the APP workforce to improve patient access and satisfaction.
Practical Considerations in Engagement of Advanced Practice Providers.
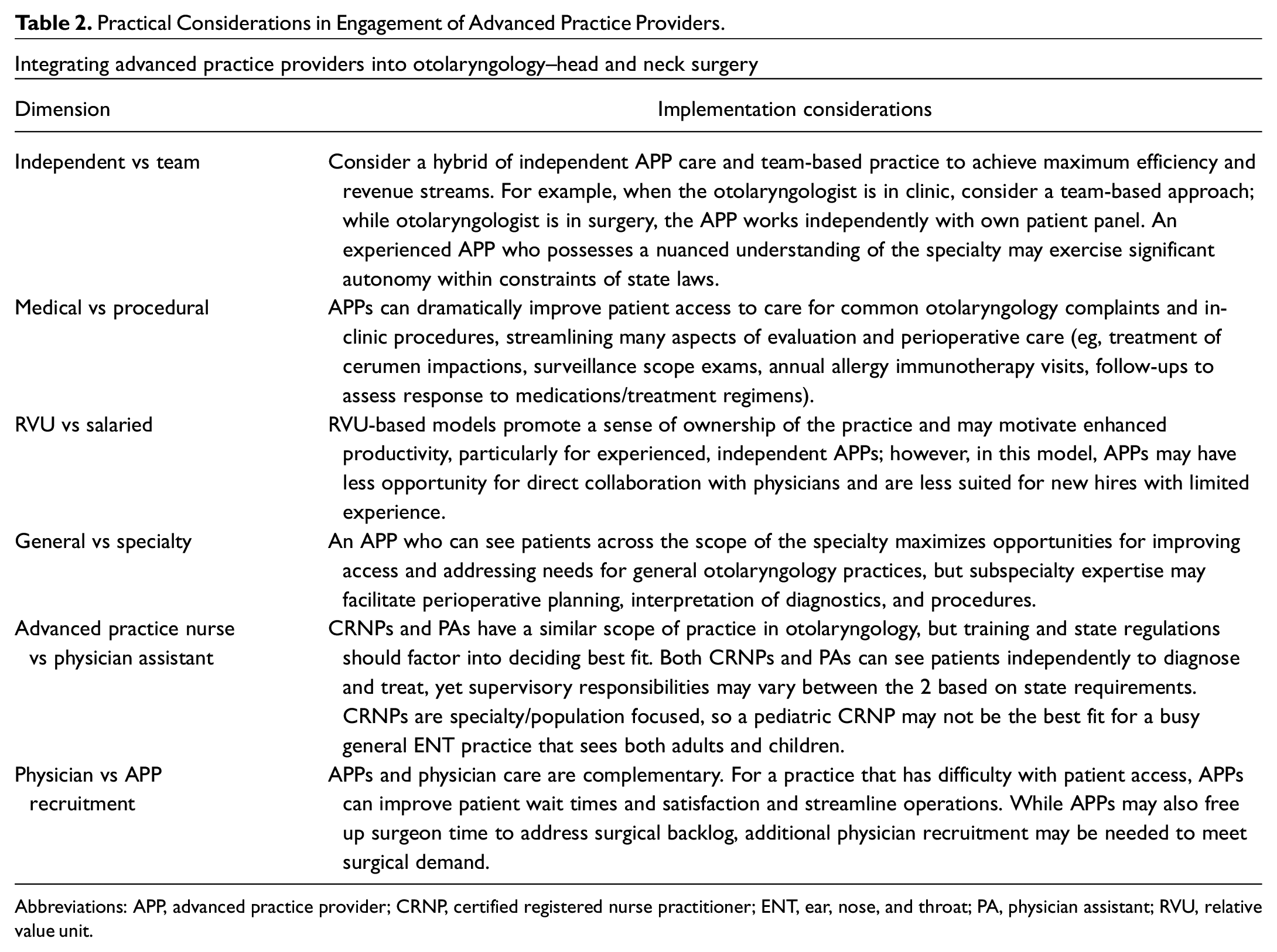
Abbreviations: APP, advanced practice provider; CRNP, certified registered nurse practitioner; ENT, ear, nose, and throat; PA, physician assistant; RVU, relative value unit.
Conclusion
The demand for health care services in otolaryngology care will increasingly exceed otolaryngologist surgeon workforce capacity. APPs are valuable partners in meeting growing needs of the population. While further data are needed to determine the optimal models of high-quality care, it is clear that APPs will be play an ever-greater role in shaping the specialty. Successful growth in otolaryngology–head and neck surgery requires a culture that supports effective integration of APPs across diverse practice settings. Progress also requires open-mindedness on the part of both providers and patients in embracing evolving models of care.
Footnotes
Acknowledgements
We thank Nui Dhepyasuwan, MEd, Director for Quality and Performance Measurement, and Elise Swinehart, Senior Director for Membership & Global Affairs, for assistance with procuring data on Academy membership.