
Abstract
Objective
This study sought to evaluate the role and trajectory of spontaneous swallowing frequency (SFA) in patients with head and neck cancer (HNC) undergoing chemoradiotherapy (C/RT).
Study Design. Prospective cohort.
Setting
University comprehensive cancer center.
Methods
A prospective cohort of 80 patients with HNC was followed from baseline to 3 months post-C/RT. Subjects were evaluated for performance on swallowing function, functional diet consumed, weight, swallowing frequency rate, perceived xerostomia, perceived pain, and mucositis. Relationships were evaluated using univariate correlations, t tests, and repeated-measures analysis of variance. The diagnostic accuracy of SFA to express dysphagia was calculated by area under the curve (AUROC) and displayed using receiver operator characteristic curves.
Results
In general, patients with HNC demonstrated a parabolic decline in most measures over the C/RT trajectory. SFA and perceived xerostomia did not show improved recovery by 3 months. SFA was related to swallow function, xerostomia, and functional diet consumed posttreatment and pain at 3 months. The ability of SFA to correctly identify clinical dysphagia (Mann Assessment of Swallowing–Cancer version [MASA-C]) and reduced oral intake (Functional Oral Intake Scale [FOIS]) at posttreatment was strong (AUROC MASA-C: 0.824 [95% CI, 0.63-1.00], P < .0018; AUROC FOIS: 0.96 [95% CI, 0.87-0.96], P < .0001).
Conclusion
This exploratory study suggests SFA may provide a useful method to identify dysphagia after HNC treatment. Furthermore, SFA may offer a simple, objective measure of swallowing function change in HNC over the C/RT trajectory.
Head and neck cancer (HNC) is associated with significant morbidities from the medical treatments used to control the cancer. A common morbidity occurring during and following HNC treatment is difficulty swallowing (dysphagia). More than 70% of patients will have some form of swallowing difficulty during or after medical treatment for their cancer.1-3 Recent intervention studies have focused on preventing dysphagia by applying preventative strategies such as encouraging eating and/or exercising during the HNC treatment period. Studies generally support these swallowing interventions and report positive outcomes (reduced severity of dysphagia and associated morbidities) by maintaining the viability of upper respiratory tract functions for swallowing.4-6 One well-recognized protective behavior of the upper respiratory tract is spontaneous swallowing.
Spontaneous swallowing reflexively clears the upper airway of unwanted materials. Upper airway clearance via spontaneous swallowing has been associated with a group of aerodigestive reflexes that support airway protection. 7 Reduced frequency of spontaneous swallowing has been associated with presence of dysphagia and increased risk of aspiration of food or liquid into the airway, increasing the risk of chest infections.8-11 Furthermore, slower spontaneous swallow frequency rates have been reported in patient groups at risk for dysphagia, including Parkinson’s disease, 8 elderly hospitalized patients, 9 and most recently in acute stroke patients.10,11
Recent data have suggested that spontaneous swallowing rates may alter over time in response to treatment, recovery, and decline and may be furthered lowered in multiple clinical conditions contributing to ongoing dysphagia.2,12 Based on these prior observations, this study proposed to investigate the role and trajectory of spontaneous swallowing frequency in patients with HNC over the chemoradiation period. Specifically, we hypothesized that spontaneous swallowing frequency would demonstrate early decline and be directly related to dysphagia severity in patients with HNC. Moreover, it would perform well in comparison to swallow function testing as a sensitive marker of swallowing decline.
Methods
Patients
A cohort of 100 patients was screened for inclusion in this study. Of these, 80 patients with confirmed HNC who were undergoing planned chemoradiotherapy (CR/T) were prospectively recruited. Patients were included based upon HNC confirmed by clinical exam, positive cross-sectional imaging and biopsy, and no history of dysphagia-related illness such as previous cancer, neurodegenerative disease, stroke, or history of nonoral feeding. Patients with extensive neck dissection or surgical intervention in the head neck region that could contribute to dysphagia were excluded. All eligible patients were identified by the attending physician and referred to the study coordinator. All enrolled patients provided signed study consent. The local institutional review board approved the study protocol (University of Florida, UF_IRB01).
Evaluations
Patient study assessments were completed at 3 time points: baseline (BL; within the first 5 days of C/RT initiation), 6 weeks (at the completion of C/RT), and 3 months after completion of C/RT.
Outcome Measures
Each evaluation consisted of a clinical assessment of swallowing function using the Mann Assessment of Swallowing–Cancer version (MASA-C) 13 and the Functional Oral Intake Scale (FOIS). 14 Patient perception of pain intensity was assessed with a visual analog (VAS) scale. 15 Body weight was measured in pounds. The University of Michigan Xerostomia Scale 16 and the World Health Authority Mucositis scale 17 were used to document xerostomia and mucositis, respectively.
The primary outcome variable for this study was spontaneous swallowing frequency analysis (SFA). Spontaneous swallowing frequency rate was evaluated by the simple acoustic recording technique extensively described in prior research.2,10-12,18-20 A small adhesive “sensor patch” was adhered to the anterolateral part of the neck (lateral and slightly below the cricoid cartilage just over the upper trachea). 19 Recording was obtained using a small microphone (VT506; Voice Technologies) and digital voice recorder (Olympus DS-40). Participants sat quietly for a period of 10 minutes watching a soundless video of underwater marine life (The Blue Planet, BBC) while the acoustic signature of spontaneous swallows was recorded. This period of recording has been previously identified as adequate to provide a valid swallow frequency recording. 10 The final numeric swallow frequency rate (ie, swallow per minute [SPM]) was calculated offline from the recording by an independent blinded evaluator. 19 All recordings were completed at rest and least 1 hour following any oral intake. Furthermore, each recording was collected at each study assessment session in an evaluation room (prior to radiation, posttreatment, and at 3-month return appointment).
Follow-up
During the investigation period, each participant’s progress was independently monitored via chart and phone review as well as biweekly face-to-face contact with an independent researcher to identify compliance with the CR/T treatment schedule, as well as the occurrence of any negative end points such as death, hospitalization, dehydration, or the occurrence of alternate feeding.
Statistical Analysis
Descriptive statistics and graphic analyses were conducted to understand the distribution of the data and summarized by mean, median, standard deviation, and ranges. Univariate analyses were applied to evaluate relationships between variables, using Pearson and Spearman correlation coefficients and repeated-measures analysis of variance (ANOVA). Proportions were compared using contingency tables and χ2 analysis. Accepted cut point for dysphagia severity, as categorical response variables (eg, MASA-C), was compared using independent t tests. The primary comparator for swallowing impairment detection rate from SFA was the proportion of subjects meeting the referent cut point for dysphagia (MASA-C score ≤185). The sensitivity and comparability of SFA to express clinically identified dysphagia and its severity were explored using receiver operator curves (ROCs). The accuracy of SFA in the identification of different degrees of dysphagia (as measured by MASA-C and FOIS) was analyzed in terms of sensitivity, specificity, positive and negative predictive values, and likelihood ratios (95% CIs calculated using standard methods). The threshold was investigated and expressed with ROCs. A priori cut points for dysphagia were reviewed and Youden’s index (j) used to an identify appropriate cutoff. Equality was represented by the diagonal line from (0, 0) to (1, 1) on the ROC graph. Area under the curve was calculated according to Hanley and McNeil. 21 All analyses were conducted using SPSS 26.0. 22
Results
Demographics
Eighty patients presenting with confirmed HNC (70:10 male/female) completed baseline assessments and swallowing evaluations ( Table 1 ). Mean (SD) time from cancer diagnosis to treatment was 9 (11) days (95% CI, 0.11-21.1). The mean (SD) age of the cohort was 61.8 (9.3) years (95% CI, 59.7-63.9). Most subjects underwent C/RT (80%). All RT was conducted with intensity modulated radiation therapy (IMRT) protocols, and mean (SD) RT dose was 71.4 (3.8) Gy (95% CI, 70.58-72.27). Almost 50% of tumors were located in the base of tongue and tonsillar regions. Other sites included a variety of other oral or oropharyngeal locations. Over the total study trajectory, 59 subjects completed 6-week testing, and 35 completed 3-month testing. Primary reasons for dropout included lost/or partial follow-up (11), death (7), withdrawal from the study (9), transferred care to alternate health facility (10), discontinued clinic visits (4), or cancer recurrence (4).
Characteristics of Study Sample (n = 80).
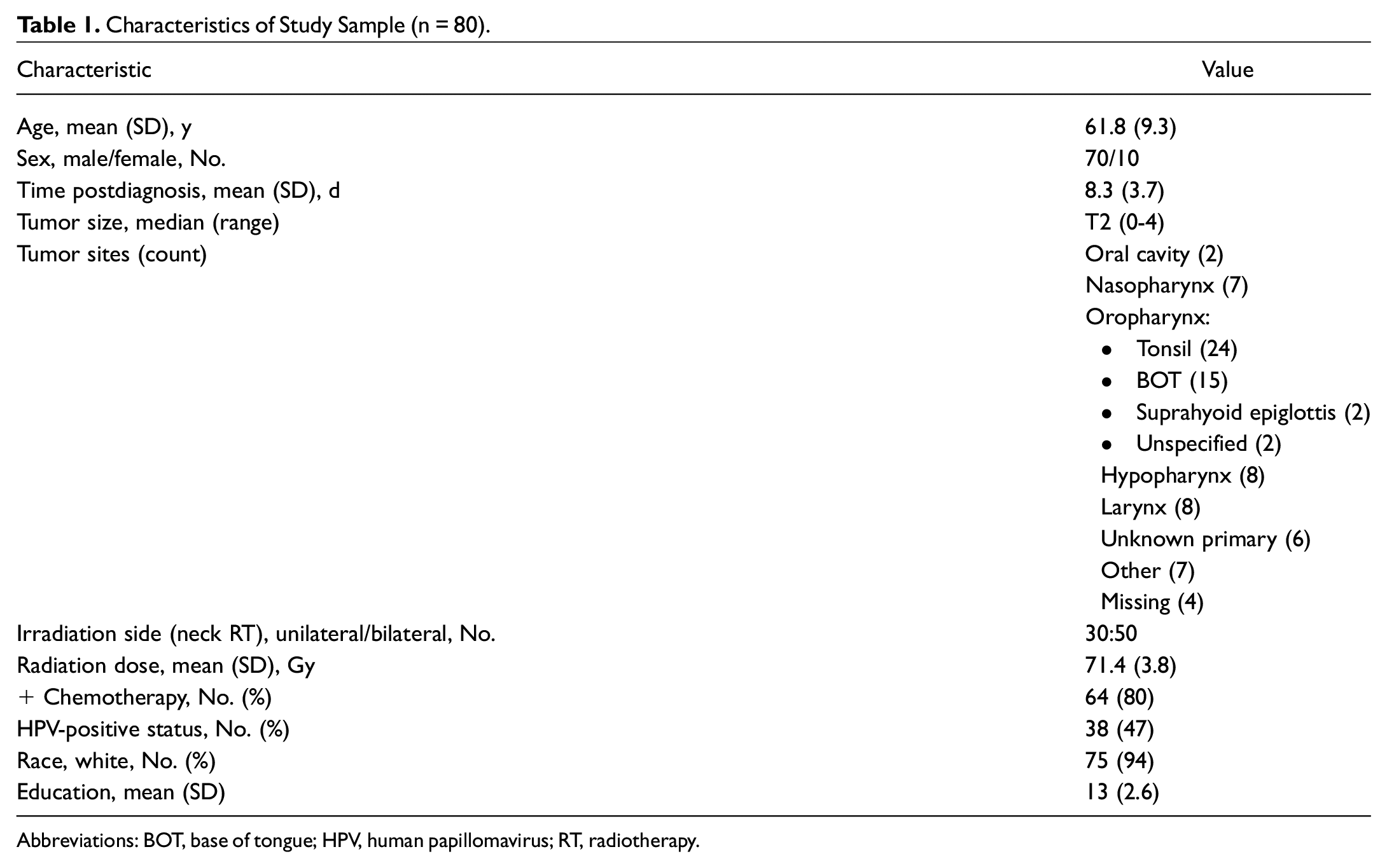
Abbreviations: BOT, base of tongue; HPV, human papillomavirus; RT, radiotherapy.
Change in Functioning
Swallow function
At baseline, the mean (SD) swallowing score (MASA-C) for the group was 191 (5.9; 95% CI, 190.4-192.7). The number of patients rating below the cut point for normal swallowing function (≤185) at this point was 10 (12%), with a mean (SD) of 180.1 (5.9). Similarly, those presenting with slight modifications from normal diet consumed (FOIS level 5/6) was noted in 11 (14%) patients prior to treatment. One patient received a prophylactic percutaneous gastrostomy (PEG), while 18 patients (22%) received reactive PEG feeding over the C/RT period. Over the C/RT treatment trajectory, clinical swallowing function demonstrated a pattern of decline with partial recovery by 3 months in both swallowing score and oral intake level ( Table 2 ). MASA-C scores were significantly lower for patients feeding by PEG tube (mean [SD], 157 [24]; 95% CI, 145-168) vs orally (mean [SD], 176 [12.1]; 95% CI, 172-179) at the posttreatment time point (P < .003).
Change in Oral Status, Pain, and Swallowing Measures (Baseline to 3 Months). a
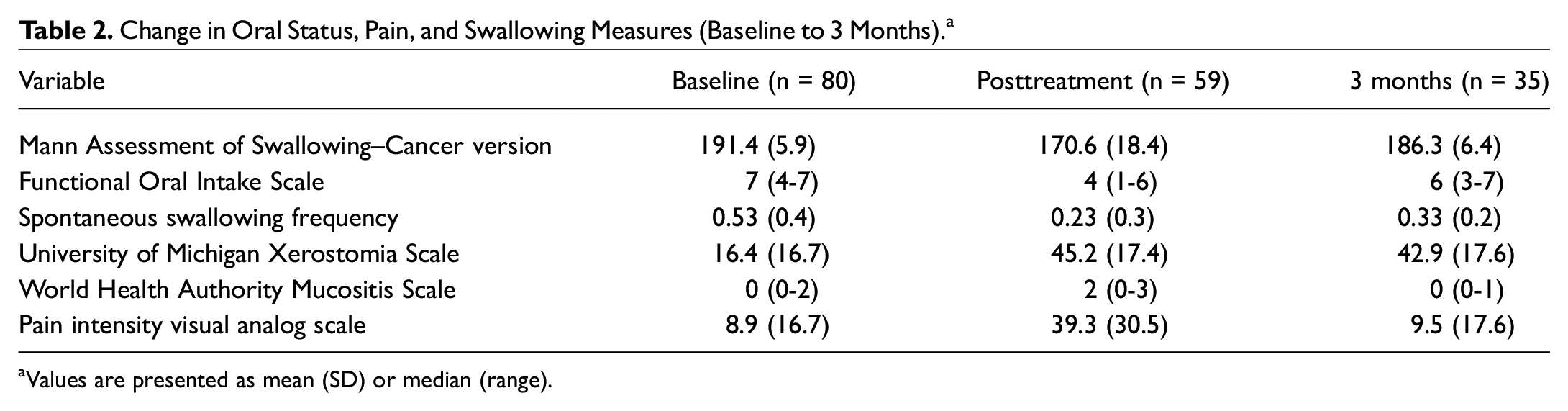
Values are presented as mean (SD) or median (range).
Swallowing frequency
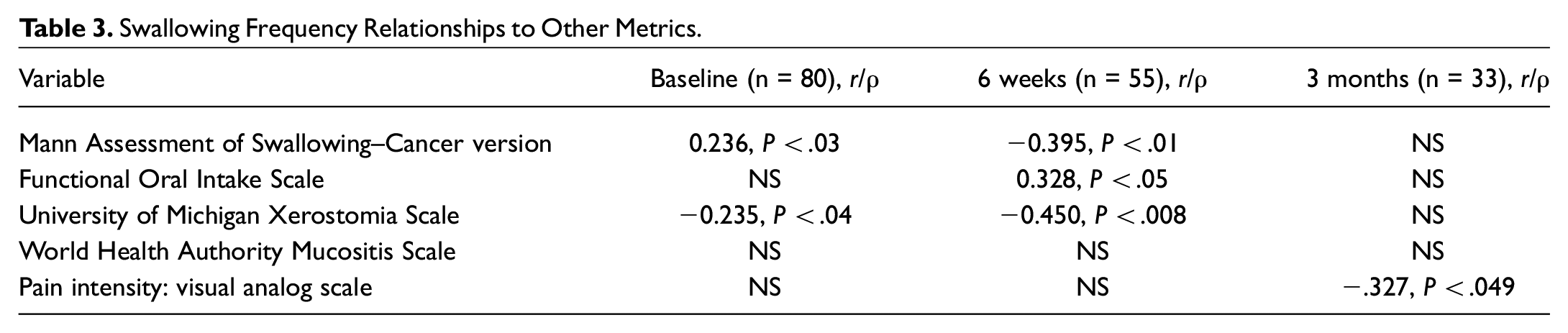
Swallowing frequency demonstrated a significant pattern of decline with incomplete recovery from baseline to 3 months posttreatment, F(2, 44) = 4.023, P < .025 ( Figure 1 ). The largest decline was identified up to the posttreatment time point (mean [SD] change, 0.32 [0.5]; 95% CI, 0.15-0.46). A nonsignificant increase in swallow frequency was noted at the 3-month time point. Over 67% of patients showed a significant decline in spontaneous swallowing at posttreatment, and 60% (21/35) remained low at 3 months. Univariate relationships demonstrated that spontaneous swallowing frequency was significantly related to age, swallowing function (MASA-C), and xerostomia at baseline. Posttreatment SFA was related to swallow function (MASA-C), functional diet (FOIS) consumed, and xerostomia ( Table 3 ). At 3 months, SFA was related to perceived pain intensity (r = −.327, P < .04). Swallowing frequency demonstrated a significant linear decline in mean rate across dysphagia severity levels (MASA-C) posttreatment, F(3, 56) = 2.44, P < .04 ( Figure 2 ). It was not significantly related to tumor characteristics, Gy received, or the presence of PEG feeding at any time point.
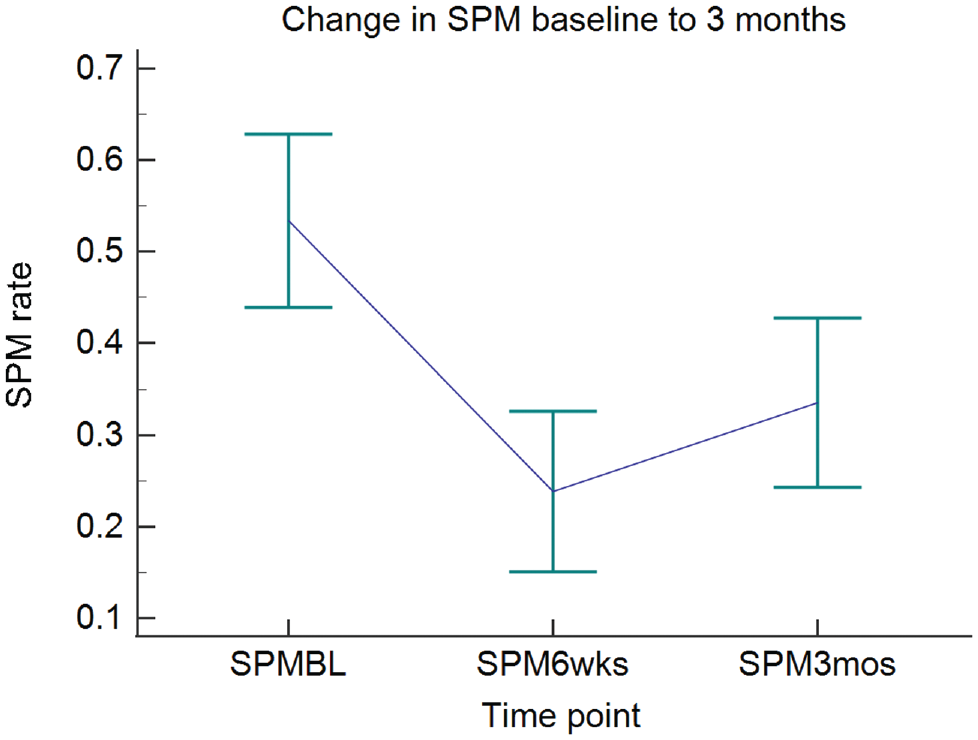
Change in swallow frequency rate across head and neck treatment trajectory. SPM, swallow per minute.
Swallowing Frequency Relationships to Other Metrics.
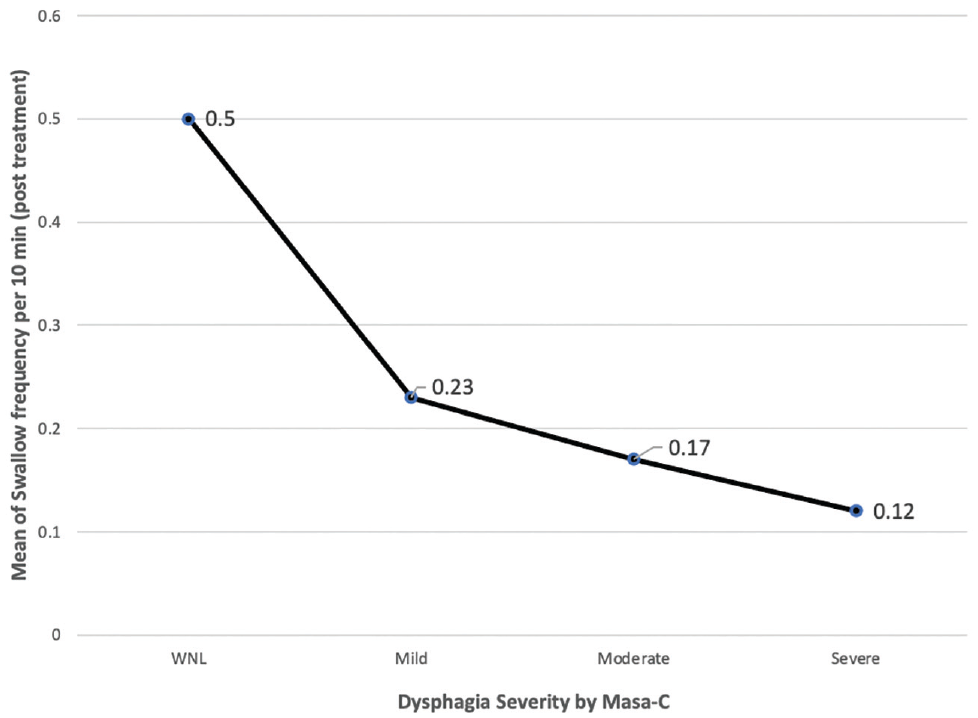
Swallowing frequency by dysphagia severity at posttreatment. MASA-C, Mann Assessment of Swallowing–Cancer version.
Xerostomia
At baseline, the mean (SD) University of Michigan Xerostomia (UMXS) score for the group was 15.41 (18.9; 95% CI, 12.6-20.1). This score demonstrated an inverse parabolic curve rising significantly over the C/RT treatment trajectory to a mean (SD) of 46.89 (17.8; 95% CI, 40.8-49.5) but only declining marginally at 3 months to a mean (SD) of 41.44 (17.1; 95% CI, 36.4-49.3). The total mean increase in dryness for the group was >35% postbaseline ( Table 2 ). At baseline and posttreatment, UMXS score was significantly related to swallowing frequency rate (r = −.246, P < .04 and r = −.450, P < .008, respectively) but not at the 3-month reevaluation ( Table 3 ). Similarly, UMXS score was significantly associated with dysphagia (by MASA-C) at both baseline (t = −3.48, P < .001) and posttreatment (t = −3.593, P < .001) but not at 3 months.
Pain
At baseline, the mean (SD) VAS pain intensity score was 8.9 (16.7; 95% CI, 5.3-12.4). Perceived pain intensity demonstrated an inverse parabolic curve across the treatment trajectory, rising significantly posttreatment and declining almost to baseline levels at 3 months. Over 25% of patients experienced a ≥20% rise in perceived pain by the posttreatment time point. Pain intensity was significantly related to functional diet (FOIS) consumed at baseline (r = −.408, P < .0001) and swallowing function (MASA-C) at baseline (r = −.356, P < .001). Posttreatment pain intensity was related to swallow function (MASA-C) (r = −.455, P < .0001) but not FOIS level. Moreover, it was not related to PEG feeding at any time point. Pain intensity was related to swallowing frequency only at the 3-month time point ( Table 3 ).
Mucositis
At baseline, mucositis as measured by the WHO Mucositis Scale was present in only 18 (22%) of patients with a median level of zero (range, 0-2). Posttreatment, mucositis was noted in 29 (50%) subjects but only 8 (23%) patients at 3 months. Mucositis was not related to swallowing frequency, swallowing function (MASA-C), functional diet (FOIS), or PEG feeding at any time point. Mean mucositis rating was significantly higher in patients with xerostomia, F(3, 59) = 7.37, P < .0001, and pain, F(3, 55) = 3.63, P < .018, at the posttreatment point only.
Accuracy of SFA to Predict Swallowing Impairment
The accuracy and comparability of SFA to express impairment in HNC swallowing function were examined and displayed using receiver operator characteristic curves. The primary comparator for this analysis was the proportion of patients falling below the dysphagia cut point on the MASA-C (≤185). Due to the limited numbers of subjects meeting this cut point at baseline and 3 months, modeling was only performed at the post treatment time point ( Figure 3 ). The Youden index of 0.63 (95% CI, 0.29-0.96) indicated an acceptable balance of sensitivity and specificity for comparison. The resulting cut point for swallowing frequency level associated with dysphagia (identified by MASA-C) was ≤0.3 (SPM). The area under the curve (AUROC) for this comparison was 0.824 (95% CI, 0.63-1.00), P < .0018. Sensitivity (Se: 96.4) and specificity (Sp: 66.7) for this criterion were high. Furthermore, the predictive values (positive predictive value [PPV] = 93.1, negative predictive value [NPV] = 80) and likelihood ratios (+LR = 2.89, –LR = 0.05) were robust. The prevalence of dysphagia posttreatment as identified by this criterion was 70%.
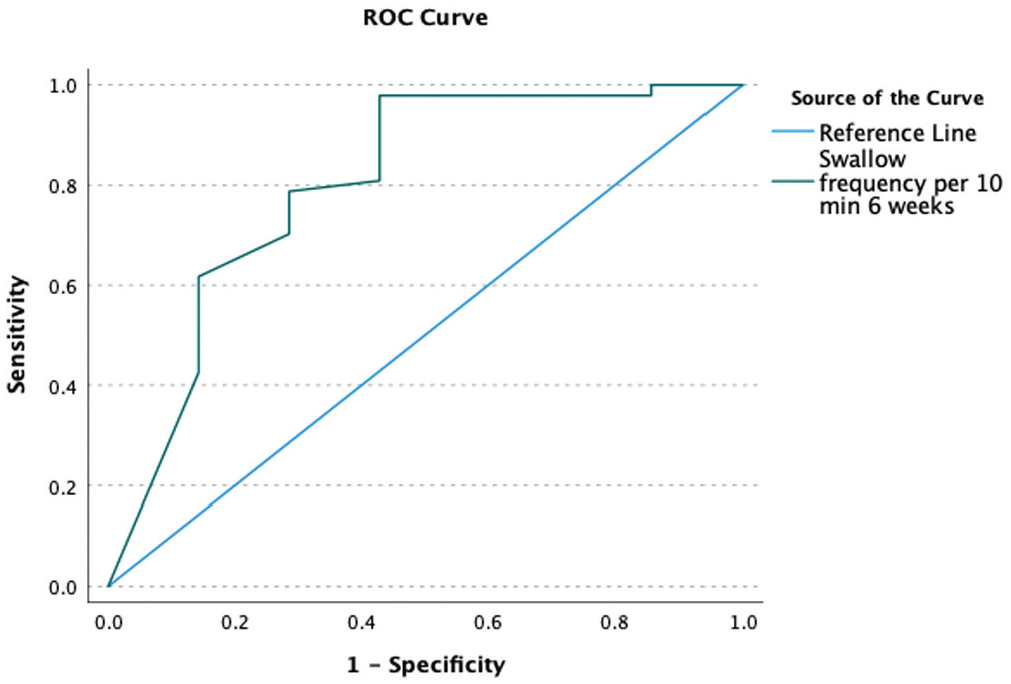
Receiver operator curve for post treatment swallowing frequency compared to standard referent: dysphagia by the Mann Assessment of Swallowing–Cancer version.
The secondary AUROC analysis focused upon reduced functional oral intake score (FOIS ≤5) ( Figure 4 ). The Youden index of 0.90 (95% CI, 0.78-0.96) indicated a good balance of sensitivity and specificity for this comparison. The resulting cut point for swallowing frequency level associated with reduced functional oral intake was ≤0.47 (SPM). AUROC for this comparison was 0.96 (95% CI, 0.87-0.96; P < .0001). Sensitivity (Se: 94.3) and specificity (Sp: 75) for this criterion were high. Furthermore, the predictive values (PPV = 86.0, NPV = 88.97) and likelihood ratios (+LR = 3.77, –LR = 0.075) were strong. The prevalence of dysphagia posttreatment as identified by this criterion was 79%.
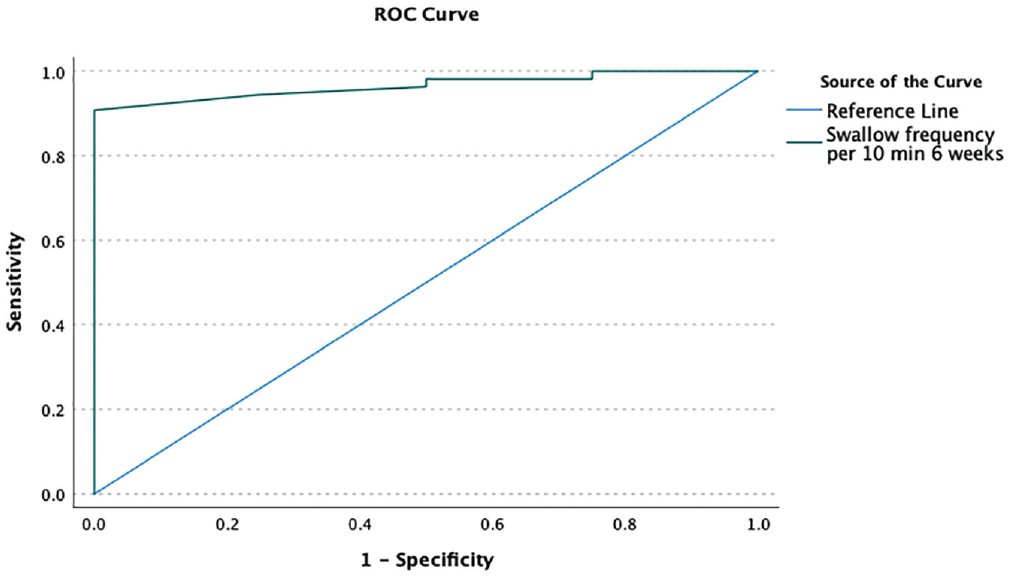
Receiver operator curve for posttreatment swallowing frequency compared to standard referent: reduced oral intake, Functional Oral Intake Scale ≤5.
Discussion
This study has confirmed the early decline and relationship of swallowing frequency to dysphagia severity over the C/RT period. Moreover, the data suggest that spontaneous swallowing frequency does not return to pretreatment levels by 3 months post-C/RT treatment. This incomplete recovery pattern appears similar to xerostomia in this same study population, with up to 60% of individuals remaining significantly affected by 3 months following treatment.
Spontaneous swallowing frequency analysis as measured in this study provides simple, objective, and robust accuracy in the identification of dysphagia post-HNC treatment. ROC analysis demonstrated good sensitivity, specificity, and yield in relation to the criterion referents (dysphagia by MASA-C and FOIS ≤5). Furthermore, both the predictive values and the likelihood ratios were strong, demonstrating its value in the identification of swallowing disability at this time point. The criterion cut point for dysphagia by swallowing frequency was identified as ≤0.3 SPM and reduced functional oral intake at ≤0.47 SPM. These different thresholds for clinically significant dysphagia vs reduced functional oral intake may suggest different underlying mechanisms. For example, patients who do not demonstrate a clinically significant dysphagia profile may reduce their level of oral intake secondary to factors such as dryness or pain. Alternatively, as the mechanism declines further, reflected by a lower SFA rate, patients may begin to show clinically significant dysphagia as measured by MASA-C. SFA may therefore perform like a heart rate monitor, providing a useful adjunct to subjective clinical evaluation or monitoring of diet alteration, that is rapid (10 minutes) and portable, requires few resources, and is both patient language and cognition independent.
The relationship between swallowing frequency and perceived xerostomia is consistent with previous investigations. For example, xerostomia has long been recognized to affect swallowing in healthy, aged, and HNC individuals following C/RT. Similarly, perceived xerostomia has been related to reduced salivary flow, salivary composition, the role of medications, and level of hydration. 23 In this study, xerostomia was related to swallowing frequency at both baseline and posttreatment. While baseline interrelationships are understandable based upon prior information, the univariate interaction at posttreatment seems more directly related to the C/RT treatment. Swallowing frequency and xerostomia, while related to changes in functional diet consumed posttreatment, were not related to the presence of nonoral feeding at any time point. This finding may suggest that after early reductions in swallowing frequency, the addition of a reactive PEG feeding may not significantly alter the SFA rate.
Future studies may wish to explore the impact of oral moisture, salivary flow, hydration, and hydration markers in this relationship. In addition, increasing the number of surveillance points may shed further light on these relationships and the timing of changes in the respective measures.
Perceived pain was significantly related to swallowing frequency only at the 3-month time point. This observation suggests that increases in perceived pain, as noted in the posttreatment evaluation, were not a primary driving factor in reduced SFA rate. This lack of a relationship between SFA rate and pain at the posttreatment time point may be confounded by the introduction of strong medication used to control pain. The inverse relationship at 3 months suggests that residual pain may be a factor in the continuation of reduced swallowing frequency. Additional research on the time course of perceived pain and impact of medication over time on swallowing frequency should provide clarification of these relationships.
Many of the findings presented here should be considered exploratory. Unfortunately, multivariate exploration was affected by sample size attrition across the study. Although not an uncommon problem in studies of HNC, this severity-related dropout within our study population reduced the power to investigate complex relationships at the later time points. Future studies should look to evaluate SFA sensitivity to change beyond the immediate acute period and monitor more closely daily SFA recovery. Likewise, due to the design of this cohort study, we were unable to obtain routine imaging studies on all patients in the cohort. This lack of confirmation with imaging evaluation for dysphagia should be seen as a limitation in that some aspects of dysphagia may have been underrepresented from clinical evaluations alone. Despite these weaknesses, we believe our study offers new information to direct research in this area. This study’s strengths include standardized inclusion/exclusion criteria, moderate-sized patient sample, >60% retention of sample across time points, and independent outcome monitoring via face-to-face measurement at all time points.
In summary, this investigation has provided unique data supporting SFA as a potential monitor for swallow system integrity across the HNC treatment trajectory. It suggests that SFA may respond to treatment, recovery, and functional feeding changes in this group. While the data mirror some findings from studies of other populations using this metric,9-12 the pattern in HNC develops across time and interacts with additional developing oral morbidities. Future studies may look to apply SFA as a simple, portable, language-independent method to identify dysphagia early and track swallow change across the HNC trajectory.