
Abstract
Candidacy evaluation for hypoglossal nerve stimulation (HGNS) is resource intensive. This proof-of-concept study investigates use of in-office volitional snore during flexible laryngoscopy as an efficient, cost-effective screening tool for HGNS evaluation. Adults with moderate to severe obstructive sleep apnea that failed continuous positive airway pressure treatment (n = 41) underwent evaluation for HGNS from 2018 to 2019. Volitional snore and drug-induced sleep endoscopy (DISE) data were collected and scored by VOTE classification (velum/palate, oropharynx, tongue base, epiglottis). A chi-square test of independence was performed that demonstrated a significant relationship between volitional snore and DISE (χ2 = 4.39, P = .036) for velum collapse pattern. Sensitivity and specificity of volitional snore for detecting velum collapse pattern were 93.6% (95% CI, 75.6%-99.2%) and 40% (95% CI, 12.2%-73.8%), respectively, illustrating its utility in screening for HGNS. Patients who demonstrate anterior-posterior velum collapse on volitional snore may be excellent candidates for confirmatory DISE at the time of HGNS implantation.
Keywords
Hypoglossal nerve stimulation (HGNS) is a promising surgical treatment for patients with obstructive sleep apnea that has failed first-line continuous positive airway pressure (CPAP) treatment.1,2 Patient selection is critical for HGNS success. Food and Drug Administration criteria include moderate to severe obstructive sleep apnea (apnea-hypopnea index [AHI], 15-65), body mass index <32 kg/m2, and absence of complete concentric velum collapse during drug-induced sleep endoscopy (DISE), which may predict HGNS outcomes.3-6
Candidacy evaluation for HGNS is a resource-intensive process with separate operative encounters for DISE and HGNS implantation. DISE is typically performed under anesthesiologist-supervised sedation in an operating room or procedural suite, with costs of $6000 to $12,000. 7 Previous studies have used volitional snore during endoscopic upper airway examination to predict patterns of sleep-disordered breathing.8,9 However, the relationship between in-office volitional snore and DISE in HGNS screening remains unknown, posing an opportunity to streamline patient care and decrease perioperative resource utilization.
Here we evaluate volitional snore during in-office flexible laryngoscopy as a screening tool for HGNS. The primary objective is to identify a correlation between volitional snore and DISE in determining velum collapse pattern.
Methods
The University of Michigan Institutional Review Board (HUM00155002) approved this prospective cohort study. The sample included adult patients (N = 41) with polysomnography-confirmed moderate to severe obstructive sleep apnea (AHI, 15-65) whose CPAP treatment failed and who underwent evaluation for HGNS (Inspire Medical Systems) from 2018 to 2019. 10 CPAP failure included usage <5 nights per week and <4 hours per night or AHI >20, excluding central sleep apnea.
Volitional snore and DISE data were recorded, and airway obstruction was scored by VOTE classification (velum/palate, oropharynx, tongue base, epiglottis). 11 For volitional snore, a single sleep surgeon performed flexible laryngoscopy to examine the upper airway while the patient performed a volitional snore by using maximal effort to create an audible snoring sound with the mouth open in a supine position. During DISE, an anesthesiologist administered propofol at 150 mcg/kg/min, increasing it by 25 mcg/kg/min every 5 minutes until the patient began snoring, with a target reading of 60 to 70 on the bispectral index monitor. The same sleep surgeon performed awake and standard sleep endoscopy. Topical anesthetic and decongestant were not used in either examination. The recorded studies were scored by 2 independent blinded observers: an experienced sleep surgeon and 1 midlevel otolaryngology resident trained in VOTE classification.
A chi-square test of independence with Yates correction, given the sample size, was performed to examine the relationship between volitional snore and DISE for identifying velum collapse pattern—specifically, anterior-posterior versus concentric/lateral. All cases were analyzed. Sensitivity, specificity, positive and negative predictive values, and accuracy are expressed as percentages. Confidence intervals are “exact” Clopper-Pearson confidence intervals.
Results
Patients (N = 41) were identified as possible candidates for HGNS based on history and examination. Baseline data for study participants are in Table 1 .
Baseline Demographic and Polysomnographic Data for Patients Undergoing DISE (N = 41).
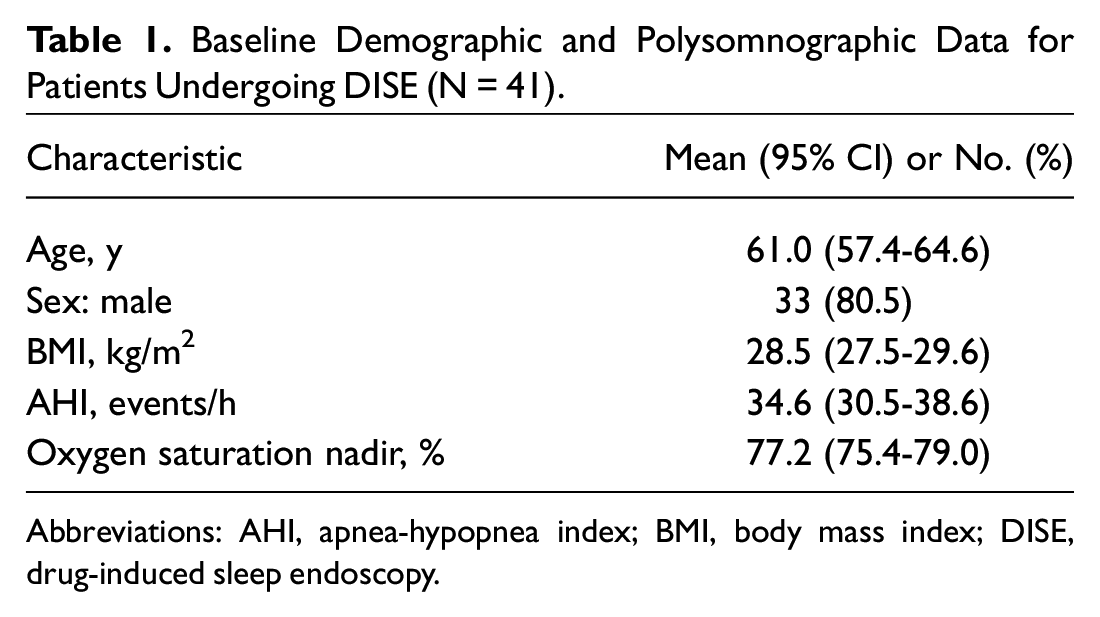
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; DISE, drug-induced sleep endoscopy.
There was a significant relationship for velum collapse pattern (anterior-posterior vs concentric/lateral) between volitional snore and DISE (χ2 = 4.39, P = .036). The sensitivity of volitional snore for detecting velum collapse pattern was 93.6% (95% CI, 75.6%-99.2%), with a specificity of 40% (95% CI, 12.2%-73.8%) and an accuracy of 80.5% (95% CI, 65.1%-91.2%). A contingency matrix comparing collapse pattern on volitional snore versus DISE is presented in Table 2 .
Contingency Matrix: In-Office Awake Snore vs DISE Assessment of Velum.
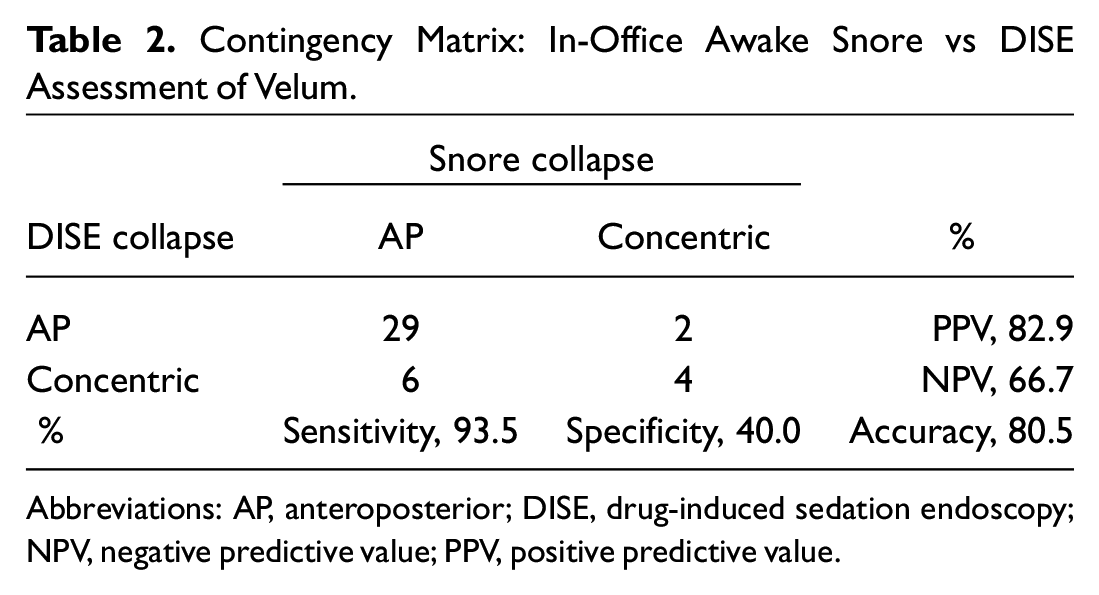
Abbreviations: AP, anteroposterior; DISE, drug-induced sedation endoscopy; NPV, negative predictive value; PPV, positive predictive value.
There was no significant concordance between volitional snore and DISE at other anatomic sites ( Table 3 ). No significant difference in study interpretation was identified between the observers for volitional snore (χ2 = 0.1488, P = .69, 92% concordance) and DISE (χ2 = 0.084, P = .77, 88% concordance).
Concordance Between In-Office Examination and DISE Findings by Site of Partial or Complete Obstruction (N = 41). a

Abbreviation: DISE, drug-induced sleep endoscopy.
Bold indicates significance.
Discussion
This is the first study exploring in-office volitional snore during flexible laryngoscopy as a screening tool prior to DISE, presenting the opportunity to improve resource utilization and cost related to preoperative HGNS screening. Given the 93.6% sensitivity of volitional snore, patients with anterior-posterior collapse on volitional snore may be excellent candidates for confirmatory sleep endoscopy at time of HGNS implantation, a current practice in several European centers.
Of note, volitional snore demonstrated low specificity (40%), and there was no significant concordance between volitional snore and DISE at other anatomic sites. This highlights the known value of DISE in HGNS candidacy evaluation and indicates that volitional snore can serve as an adjunct to, but not a replacement for, DISE. 12 A recent retrospective study identified examination characteristics, including lower Friedman tongue position and Mallampati score, to be significantly associated with superior postoperative AHI improvement, which may also be considered. 13
The study limitations include a small number of patients, although volitional snore still demonstrated significant prognostic value in this sample. The statistically significant relationship between volitional snore and DISE in terms of pattern of collapse at the velum shows a valid proof of concept for further multi-institutional study. Additionally, the setting was a single academic center with experienced sleep surgeons. Still, there was no significant difference in study interpretation between blinded observers.13-15
Optimizing HGNS candidacy evaluation will streamline patient care and decrease perioperative resource utilization. Specifically, future HGNS evaluation may use volitional snore as a screening tool, followed by confirmatory DISE at time of HGNS implantation. Additional studies are indicated to assess the utility of volitional snore in HGNS screening, including a prospective trial of clinical and polysomnogram outcomes for patients who undergo volitional snore followed by DISE.
Conclusion
This study demonstrates the sensitivity of volitional snore during in-office flexible laryngoscopy to predict velum collapse pattern, providing significant prognostic value as a screening tool for HGNS. Patients with anterior-posterior velum collapse on volitional snore may be excellent candidates for confirmatory sleep endoscopy at time of HGNS implantation, reducing perioperative resource utilization.
Footnotes
This article was presented for the AAO-HNSF 2020 Virtual Annual Meeting & OTO Experience; September 13–October 25, 2020.