
Abstract
Objective
To compare the cost-effectiveness of sialendoscopy with gland excision for the management of submandibular gland sialolithiasis.
Study Design
Cost-effectiveness analysis.
Setting
Outpatient surgery centers.
Methods
A Markov decision model compared the cost-effectiveness of sialendoscopy versus gland excision for managing submandibular gland sialolithiasis. Surgical outcome probabilities were found in the primary literature. The quality of life of patients was represented by health utilities, and costs were estimated from a third-party payer’s perspective. The effectiveness of each intervention was measured in quality-adjusted life-years (QALYs). The incremental costs and effectiveness of each intervention were compared, and a willingness-to-pay ratio of $150,000 per QALY was considered cost-effective. One-way, multivariate, and probabilistic sensitivity analyses were performed to challenge model conclusions.
Results
Over 10 years, sialendoscopy yielded 9.00 QALYs at an average cost of $8306, while gland excision produced 8.94 QALYs at an average cost of $6103. The ICER for sialendoscopy was $36,717 per QALY gained, making sialendoscopy cost-effective by our best estimates. The model was sensitive to the probability of success and the cost of sialendoscopy. Sialendoscopy must meet a probability-of-success threshold of 0.61 (61%) and cost ≤$11,996 to remain cost-effective. A Monte Carlo simulation revealed sialendoscopy to be cost-effective 60% of the time.
Conclusion
Sialendoscopy appears to be a cost-effective management strategy for sialolithiasis of the submandibular gland when certain thresholds are maintained. Further studies elucidating the clinical factors that determine successful sialendoscopy may be aided by these thresholds as well as future comparisons of novel technology.
Keywords
Sialolithiasis is a major cause of salivary gland disease with the incidence reported to range from 1 in 10,000 to 300,000 individuals per year. 1 Salivary calculi mainly occur in the submandibular gland (80%-90%), likely due to the length and route of Wharton’s duct and the more mucinous and mineral-rich composition of submandibular gland saliva.2,3 Conservative management consists of antibiotics, anti-inflammatory agents, and salivary mobilization measures. When medical management is ineffective, surgical intervention is considered.
Historically, stones that were not easily palpable in the floor of mouth were managed by transcervical submandibular gland excision. However, open resection of the gland comes with a noticeable scar and possible complications that may adversely affect quality of life, such as xerostomia or nerve damage.3,4 In a study of 48 patients who underwent submandibular gland excision for sialolithiasis, a significant percentage of the gland specimens exhibited normal histologic findings, disproving the previously accepted belief that salivary glands with sialolithiasis are nonfunctional. 5 In light of this discovery, the treatment of sialolithiasis has shifted toward a more conservative approach.
Since its introduction in the early 1990s, minimally invasive sialendoscopy has become an increasingly popular surgical alternative that allows for preservation of the natural form and function of the gland. By using a small-diameter semirigid endoscope, sialolithiasis and other diseases of the salivary glands can be managed with a variety of instruments through a working channel. 6 Although sialendoscopy is associated with lower morbidity than traditional surgery, achieving the goals of treatment is not guaranteed. Factors associated with successful outcomes are more nuanced than those of open gland excision and largely depend on stone size, shape, location, and number, as well as the experience of the surgeon.4,7,8 Sialendoscopy also appears to be more costly than traditional gland excision. An upfront investment is required for equipment, with ongoing maintenance and repair. Reimbursement for the procedure, though not well established, usually exceeds simple gland excision. Finally, as sialendoscopy is relatively new and may not be routinely taught in training, the learning curve involved to acquire technical proficiency must be considered.4,9
With the continued establishment of sialendoscopy as an alternative to gland excision, surgeons must decide on the most appropriate modality for each case of sialolithiasis. In addition to clinical factors that have been described to aid in this decision process, we have examined a cost-effective analysis as an important dimension to help determine best practice.
Methods
Decision Model
We compared the cost-effectiveness of 2 operative strategies for the management of submandibular gland sialolithiasis in otherwise healthy middle-aged individuals: gland preservation with sialendoscopy versus transcervical gland excision. We constructed a Markov decision model to simulate treatments, complications, revision surgery, and recurrence in this patient population. The state transition diagram in Figure 1 demonstrates how patients flow through the model in each of the 2 treatment arms. The full decision tree can be visualized in Supplemental Figure S1 (available online). The model was analyzed from a third-party payer’s perspective via 1-year Markov cycles with a 10-year time horizon. The model was built with TreeAge Pro 2020 (TreeAge Software), and the .trex file was provided to the journal. All values for transition probabilities, costs, and health utilities, including their studied ranges, are presented in Table 1 and described in turn.
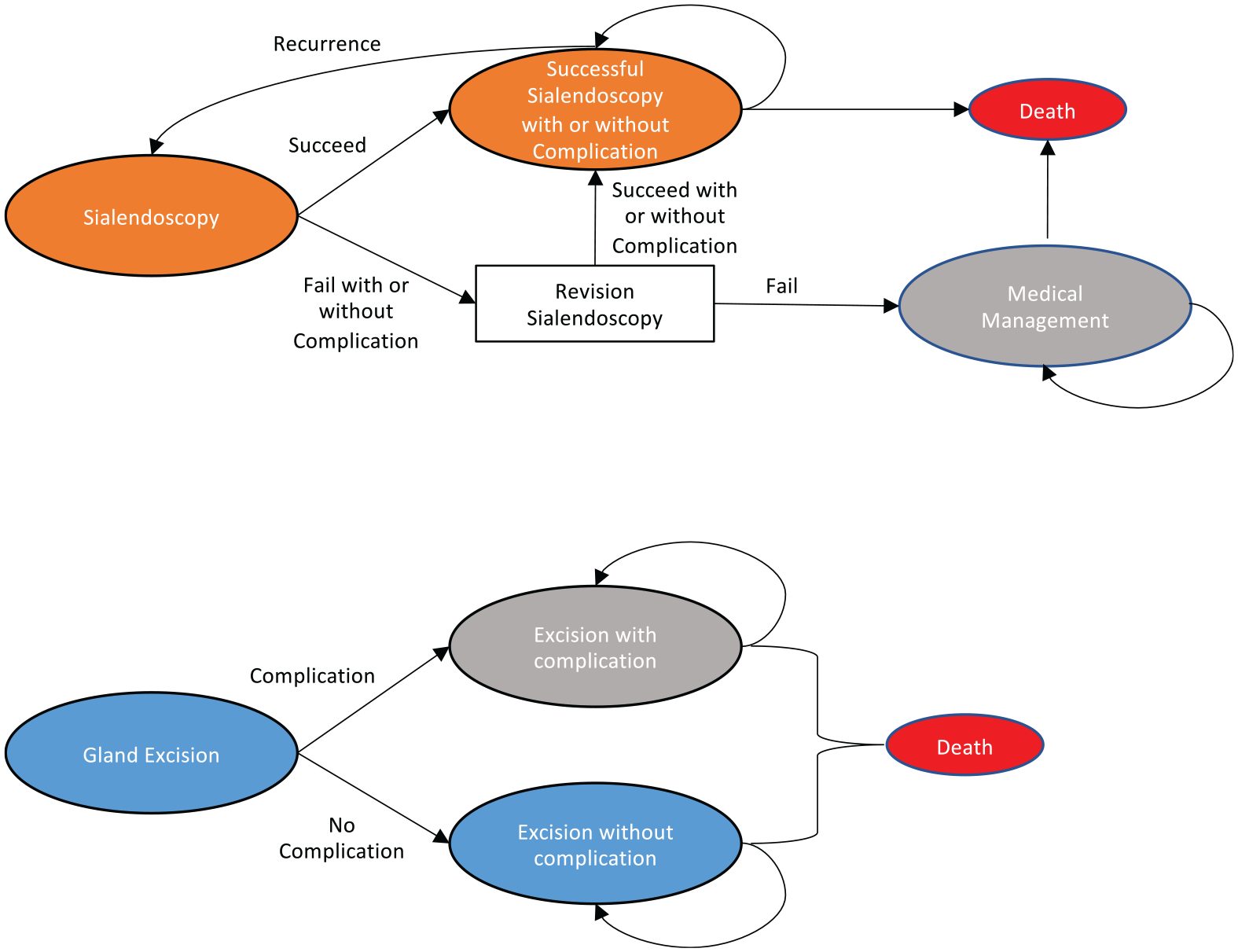
State transition diagram. The model’s health states are represented by ovals. Patients transition between health states according to surgical outcome probabilities. Costs and quality-adjusted life-years are tabulated over 10 years.
Model Inputs.
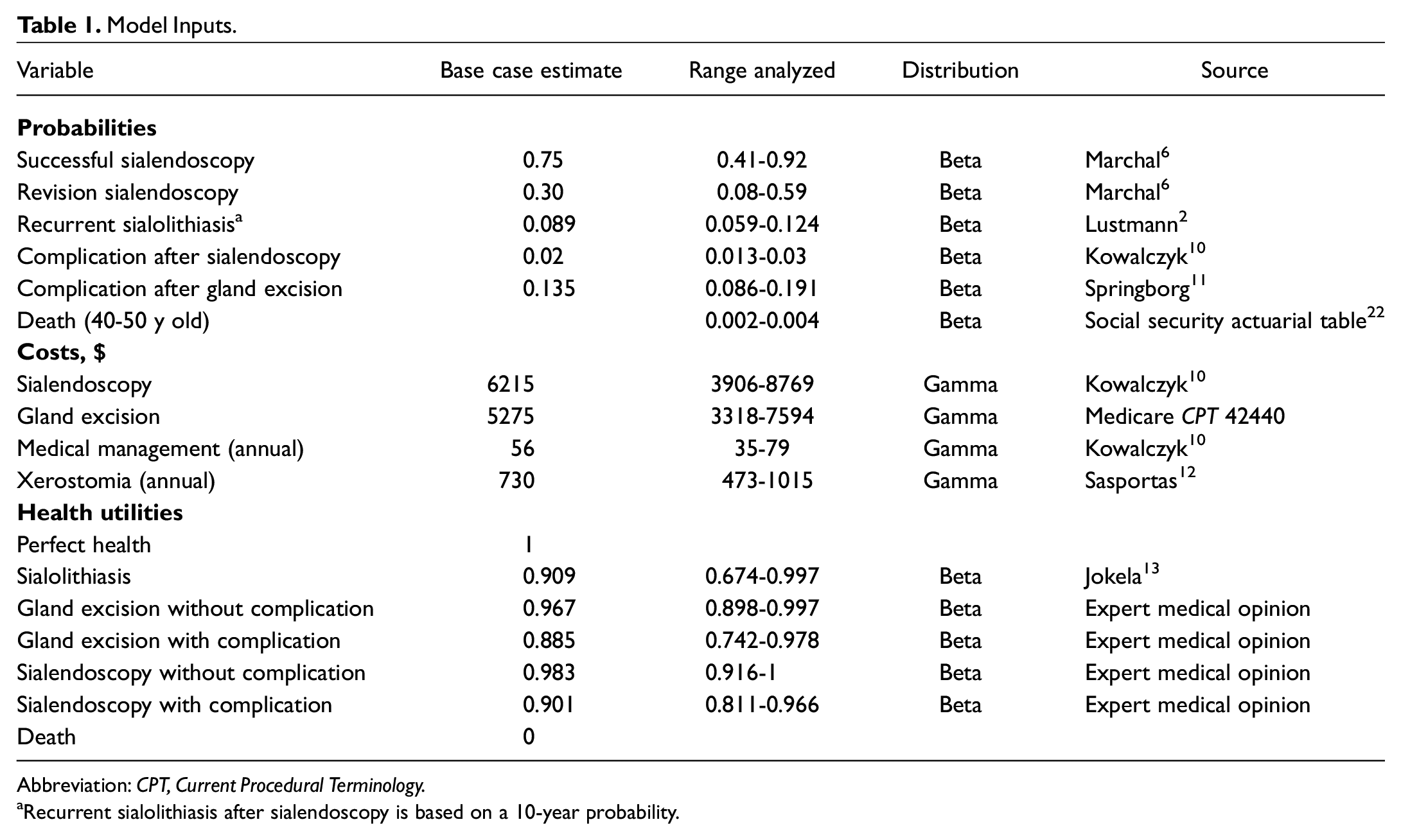
Abbreviation: CPT, Current Procedural Terminology.
Recurrent sialolithiasis after sialendoscopy is based on a 10-year probability.
Model Probabilities
In our model, patients with submandibular gland sialolithiasis were treated with either gland preservation by sialendoscopy or transcervical gland excision. In the sialendoscopy arm, the main probabilistic branch point was whether the stone(s) was successfully retrieved by any endoscopic method (basket/forceps, laser, balloon dilation, etc). To be consistent with published operative outcomes, there is a revision rate of 30% integrated into the model for patients whose primary sialendoscopy fails. 6 If revision sialendoscopy does not eradicate disease, patients are assumed to be treated with conservative measures only for the remainder of the time horizon. Probabilities of long-term complications and recurrent sialolithiasis after sialendoscopy were also incorporated into the model.2,10
In the gland excision arm, the main probabilistic branch point was the incidence of long-term complications. Patients have reported a variety of adverse events after transcervical excision of the submandibular gland, such as xerostomia, paresthesia of the surgical site, and nerve dysfunction. As a baseline estimate of the probability of complication after gland excision, we used the rate of the most common chronic complication cited in the literature: xerostomia. 11 The full spectrum of complications that might occur after gland excision was considered in estimating quality of life after surgery (see Health Utilities section).
The rate of death of patients in each arm did not differ since the disease does not affect mortality. Medicare actuarial tables were used to estimate annual mortality for accurate quantitative analysis.
Costs
This analysis was performed from a third-party payer’s perspective. In the sialendoscopy arm, we considered the major surgical cost of sialendoscopy, the cost of revision, and annual costs for conservative medical management in cases where sialendoscopy failed. The base case estimate of the surgical cost of sialendoscopy was found in primary literature, which was based on institutional Medicare charges and reimbursements. 10 In the gland excision arm of the model, the cost of submandibular gland excision was estimated from a direct lookup of the Medicare charge and reimbursement data per the CPT code for gland excision (42440; Current Procedural Terminology). We also considered an annual cost for xerostomia if patients experienced a long-term complication.10,12 All costs were converted to 2019 dollars via a Consumer Price Index calculator and discounted at 3% per year.
Health Utilities
Health utilities are values between 0 (death) and 1 (perfect health) that represent the quality of life of a patient in a given disease state. Typically, values are estimated by patient or expert opinion surveys. Here, the health utility of patients with submandibular gland sialolithiasis was available in peer-reviewed literature. 13 The remaining health utilities, not well described in the literature, were estimated by expert surveys. In brief, 15 board-certified otolaryngologists who were not part of the research team were issued a survey containing 3 vignettes for the disease states in question. Experts were asked to estimate health utilities on a number line and provide feedback. The modified Delphi method was employed to allow for consensus agreement of final base case health utility values. 14 The survey is provided as Supplemental Figure S2 (available online).
Analysis
Our base case analysis used our best estimates of probabilities, costs, and health utilities to determine the average cost and effectiveness of the gland preservation by sialendoscopy and gland excision strategies over the time horizon of the model. The effectiveness of each strategy was measured in quality-adjusted life-years (QALYs), which measure disease burden by accounting for quality and quantity of life. QALYs are the product of a patient’s health utility over a duration. All QALYs were discounted at 3% per year.
The cost-effectiveness of each strategy was then determined by calculating an incremental cost-effectiveness ratio (ICER), which represents the incremental cost of each QALY gained between the 2 strategies (ICER = Cost1– Cost2 / QALY1– QALY2). In the United States, $150,000 per QALY gained is in the range of generally accepted “willingness to pay” thresholds. 15 It is important to note that willingness-to-pay thresholds vary by person, region, health care system, or country. We considered anything <$150,000 per QALY as cost-effective over its comparator (www.ICER.org).
We conducted 1-way deterministic sensitivity analyses on all variables to assess how each variable might drive cost-effectiveness conclusions. Each variable was analyzed over a specified range to determine thresholds that could change the conclusions of our analysis. For the 1-way sensitivity analyses, each input was varied over an established distribution in isolation. A 2-way sensitivity analysis is also included with 2 variables: the cost of sialendoscopy and the probability of successful sialendoscopy. The interplay between these variables is visualized while holding all others constant.
We conducted a probabilistic sensitivity analysis based on a Monte Carlo simulation that evaluated uncertainty over 5000 unique iterations. In each iteration, variables were simultaneously assigned a random value from their respective distributions before running the cost-effectiveness analysis. Once tabulated, the Monte Carlo simulation reported the percentage of iterations where one strategy is more cost-effective over the other.
For all sensitivity analyses and the Monte Carlo simulation, cost estimates were modeled with gamma distributions, which represent probability distributions that, like cost, are bound by the interval 0 to infinity. Transition probabilities and health utilities were modeled with beta distributions, which are bound by the interval 0 to 1.
This study received approval exemption status from the University of Southern California Institutional Review Board.
Results
Base Case Analysis
The base case cost-effectiveness analysis found that sialendoscopy cost $8306 on average while gland excision cost $6103. The effectiveness of sialendoscopy yielded 9.00 QALYs while gland excision yielded 8.94 QALYs. Therefore, the ICER for sialendoscopy versus gland excision was $36,717 per QALY gained. This is under the willingness-to-pay threshold of $150,000 per QALY gained, making sialendoscopy cost-effective by our best estimates of all variables ( Table 2 ).
Base Case Analysis.
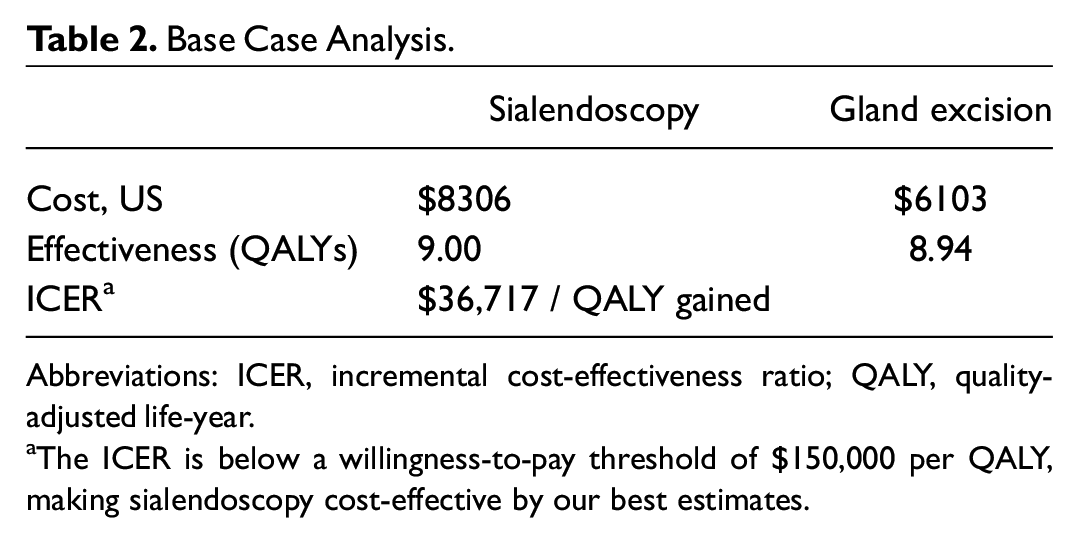
Abbreviations: ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life-year.
The ICER is below a willingness-to-pay threshold of $150,000 per QALY, making sialendoscopy cost-effective by our best estimates.
Sensitivity Analyses
Our cost-effectiveness model was sensitive to the health utilities, the cost of sialendoscopy, and the probability of successful sialendoscopy. The sensitivity of the model to the health utilities must be taken in context. Since these variables were estimated by experts considering the value of one in reference to all others, it is not logical to dramatically change one while holding all others constant. Therefore, the sensitivity thresholds of the health utilities were not further analyzed. Conversely, the uncertainty in values for the probability of success and the cost of sialendoscopy reveal useful information.
The 1-way sensitivity analysis of the probability of successful sialendoscopy revealed that it is cost-effective as long as the probability of retrieval of the stone(s) was at least 0.61 (61%; Figure 2 ). Below this value, the added cost of revision surgery and the risk of ultimate failure made sialendoscopy less cost-effective than gland excision.
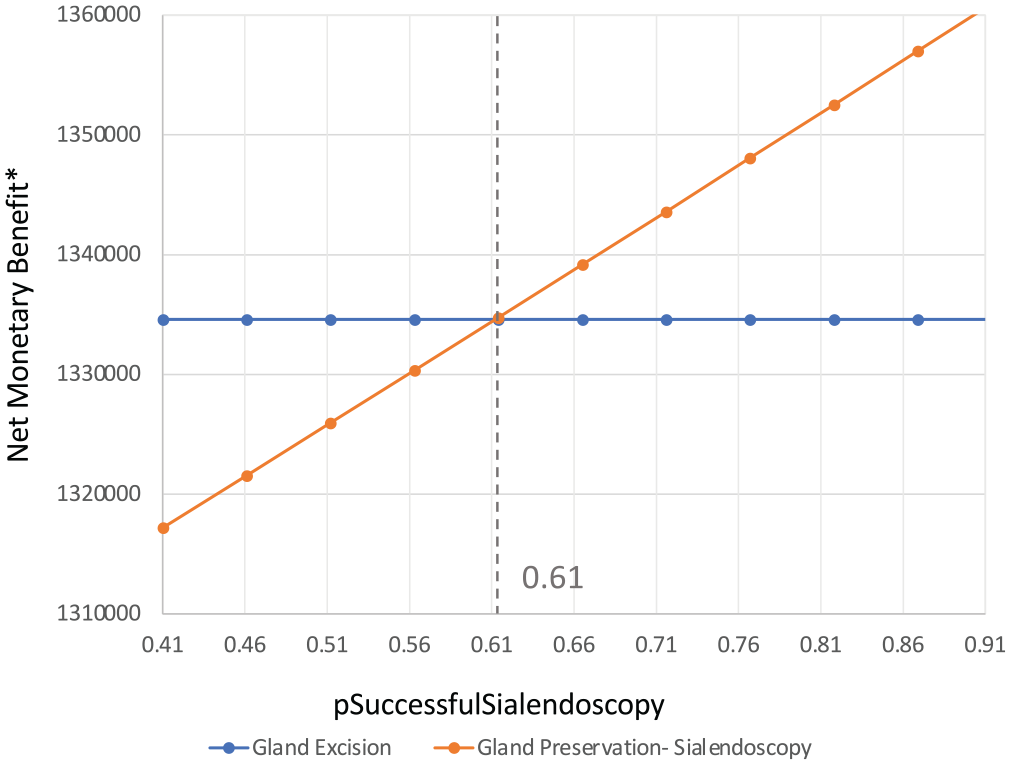
One-way sensitivity analysis: probability of successful sialendoscopy. When the probability of successful sialendoscopy exceeds 0.61, sialendoscopy is cost-effective over gland excision.
Similarly, there was a threshold at which the cost of sialendoscopy became less cost-effective than gland excision. This threshold was found at $11,996, well above our baseline cost of $6215 for the procedure ( Figure 3 ). However, the total cost may reach this amount if the primary attempt is ineffective and the patient undergoes a revision procedure. The interplay between these 2 variables is visualized by a 2-way sensitivity analysis, where the 2 variables are examined over their ranges while holding the rest of the variables in the model constant ( Figure 4 ).
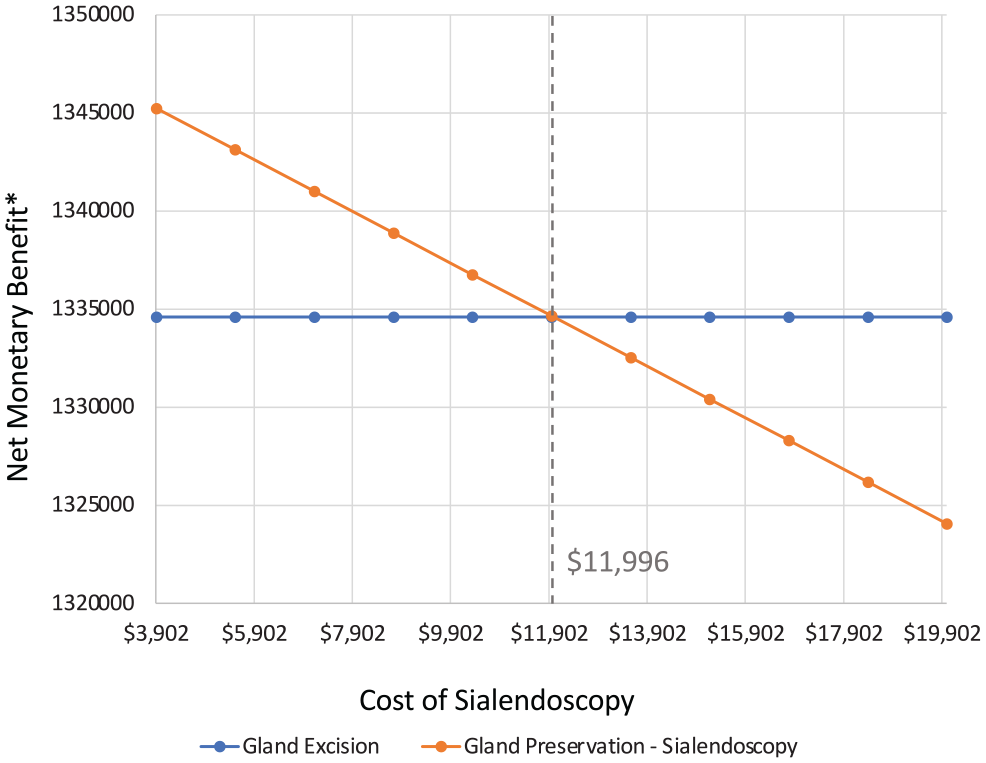
One-way sensitivity analysis: cost of sialendoscopy. The cost of sialendoscopy must be below a threshold of $11,996 to be cost-effective over gland excision.
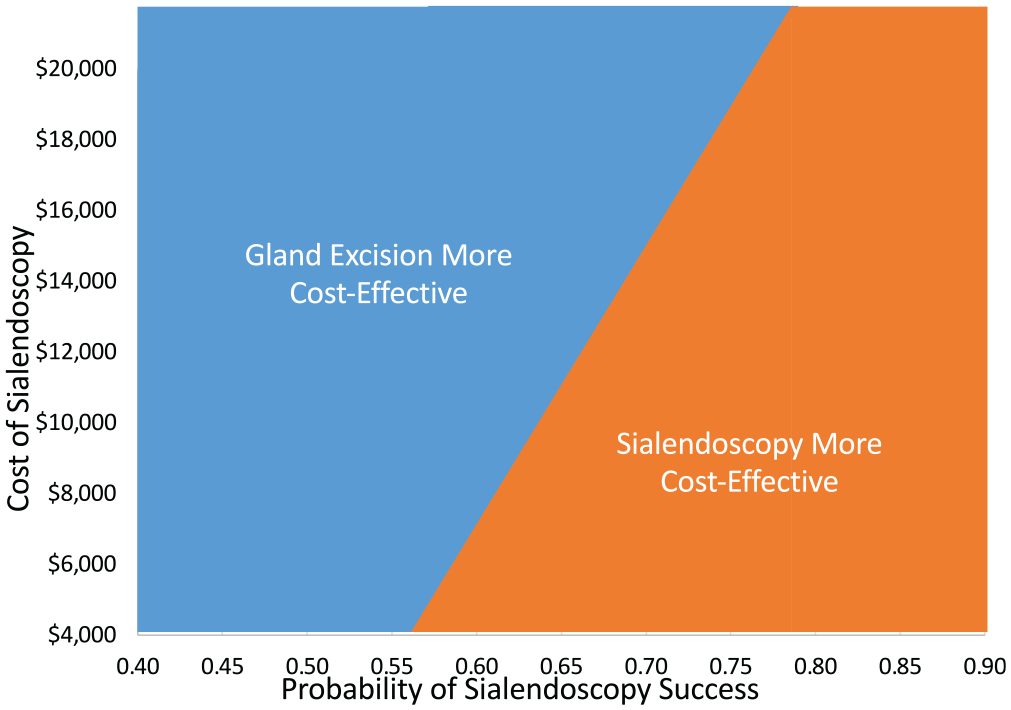
Two-way sensitivity analysis: cost of sialendoscopy vs probability of success. Cost-effectiveness is determined by the interplay of 2 key variables in our model. Cost and probability of successful sialendoscopy are positively correlated.
Probabilistic Sensitivity Analysis
The result of a Monte Carlo simulation revealed that sialendoscopy was cost-effective over gland excision 60% of the time. This analysis accounted for 5000 unique combinations of variable model inputs. The result of the Monte Carlo simulation is visualized as a scatterplot in Figure 5 . A willingness-to-pay trend line of $150,000/QALY was included to delineate each iteration where sialendoscopy was considered cost-effective (to the right of the line) versus that where gland excision was cost-effective (to the left).
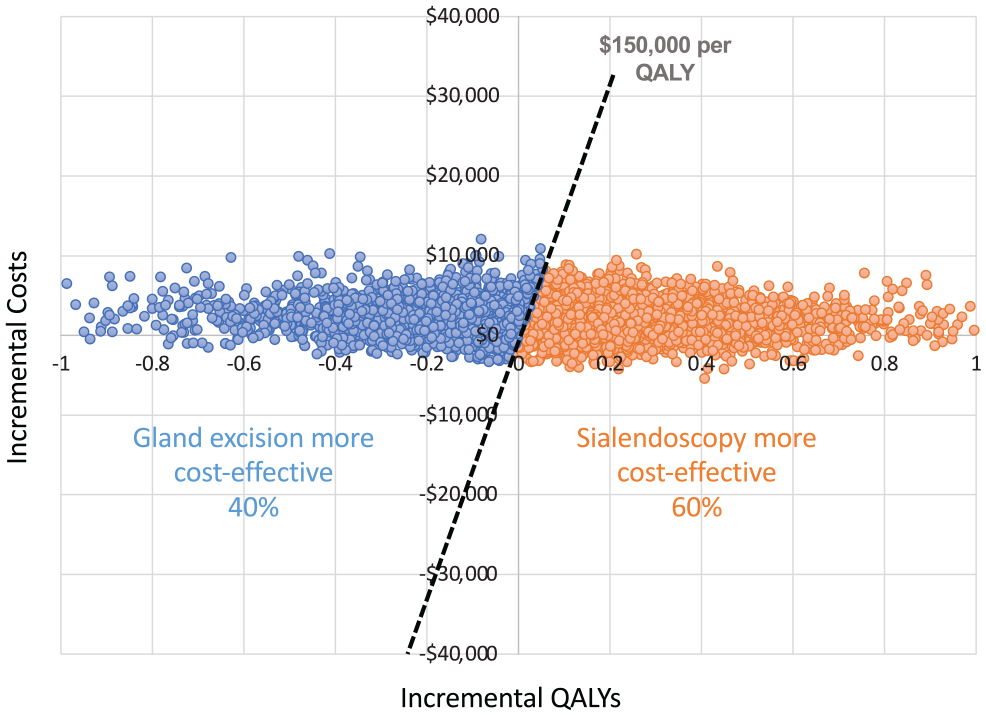
Probabilistic sensitivity analysis: Monte Carlo simulation. Each iteration is represented by a dot that falls below or above the willingness-to-pay threshold of $150,000 per quality-adjusted life-year (QALY). Sialendoscopy is cost-effective in 60% of variable combinations.
Discussion
Sialolithiasis of the submandibular gland is a challenging disease, often leading patients to seek definitive management. With the introduction of sialendoscopy as a minimally invasive management strategy, an increasing number of specialists are integrating it into their practices. Although the procedure has gained acceptance over the past few decades, a significant number of revision operations and failed attempts persist.4,9,16,17 This calls into question the value of the procedure as it pertains to cost and investment in time and technology. To date, the factors that determine whether the procedure is cost-effective are not well described. We compared sialendoscopy with traditional transcervical gland excision using the comprehensive analytic methods afforded by cost-effectiveness analysis. Our findings help define value to salivary gland disease interventions by considering outcomes, cost, and long-term quality of life for patients.
Our base case analysis revealed that, by our best estimation, sialendoscopy is a cost-effective intervention when compared with gland excision for submandibular sialolithiasis. Although the procedure is more costly than gland excision, it is more effective overall by offering better quality of life in the years after surgery (QALYs). The added cost is well under what is generally accepted as cost-effective in the United States ($150,000 per QALY). This result held up to random variability in 60% of iterations in our Monte Carlo simulation, making a robust argument for sialendoscopy. There are, however, key variables upon which this cost-effectiveness conclusion depends.
Our model was sensitive to the probability of successful outcomes with sialendoscopy. When the probability of success reaches ≥0.61 (≥61%), then sialendoscopy is considered a cost-effective option gland excision. In studies that have characterized stones treated with sialendoscopy, size criteria of 4 to 5 mm have been suggested as being amenable for retrieval by basket or forceps.16-18 Larger stones may require a combination of techniques, such as laser lithotripsy or open approaches, and may increase the chance for revision or outright failure. 17 Other factors that have been cited as reasons for increased difficulty include increased time to treatment, 16 adherence of stones to the duct, 7 and the orientation of the stone. 19 Therefore, a comprehensive disease history, physical examination, and imaging workup prior to surgery are essential in assessing the likelihood of successful sialendoscopy. This study provides a target probability at or above which sialendoscopy is the preferred treatment. Future studies that evaluate clinical factors determining success may use the 0.61 probability threshold as a target when recommending an optimal management strategy. Additionally, quality measures may use this target to assess the appropriateness of sialendoscopy.
By our estimation, the cost of sialendoscopy per procedure must remain under roughly $12,000 to remain cost-effective. This is about double the cost of our baseline estimate from review of the literature. 10 Nevertheless, reimbursement for the procedure has not been well established. To date, Medicare has not designated a CPT code for sialendoscopy, leaving practitioners to bill comparable codes with wide variability in reimbursement depending on the payer. Studies in Europe have generated a more precise measure of cost in their countries, but given the disparate nature of their health care systems as compared with the United States, direct comparison is not applicable.4,13 Our model estimates the 10-year average cost of sialendoscopy to be about $2000 more than gland excision. This does not take into account the initial investment of endoscopes and accessories, which can reach multiple tens of thousands of dollars. 4 The cost to repair a single broken scope alone would render that procedure non–cost-effective, and subsequent successful operations must be completed to make up for the cost of repair. We can estimate the burden of investment and find the number needed to successfully treat before sialendoscopy becomes cost-effective. For example, an initial investment of $25,000 would require roughly 5 successful operations for the cumulative cost of the procedures plus equipment to fall under our cost-effectiveness threshold (assuming $6200 per procedure). If a hospital or practice group can justify this investment by demonstrating clinical volume and practitioner competence with this equipment, it would be a significant gain for patients.
It is important to note limitations of this study. As in all cost-effectiveness analyses, the base case estimates for variables in the model are inherently uncertain due to variations in practice settings, patient characteristics and selection, and surgeon outcomes. Additionally, expert opinion surveys, although accepted as a method for valuing health states, are considered more uncertain than patient surveys.20,21 These sources of uncertainty are mitigated by our sensitivity analyses. If any variable for a particular surgeon, patient population, or health care system is dramatically different from our baseline estimates, we are able to identify and probe it for significant thresholds. Additionally, our probabilistic sensitivity analysis (Monte Carlo simulation) evaluates model inputs over a wide range simultaneously and in combination. The fact that sialendoscopy was more cost-effective 60% of the time means that even when accounting for 5000 combinations of values, the results were significantly in favor of sialendoscopy.
Further limitation is noted where the model is a simplification of what can become a convoluted clinical scenario. For example, surgeons and their patients may select different strategies for treatment of submandibular gland sialolithiasis other than ones that we have considered. Two specific scenarios come to mind: (1) the patient agrees to convert to open gland excision intraoperatively if sialendoscopy is unsuccessful, or (2) the patient decides to opt for gland excision at a second stage only once an attempt at sialendoscopy is unsuccessful. These scenarios were not included in the model because they are, without the need for modeling, obviously more cost-effective (scenario 1) or less (scenario 2). Converting to open excision intraoperatively can save the major cost of revision surgery, while undergoing sequential operations is the opposite scenario. While there will be patients who will agree to the former strategy or fall into the latter, we cannot predict who will fit into these categories and have evaluated only the initial treatment decision branch point. If a patient is amenable to intraoperative conversion, then this strategy should strongly be considered.
Finally, we acknowledge that some patients may require >1 revision sialendoscopy before treatment is considered a success. However, our model cannot simulate revision rates in perpetuity and is therefore limited to 1 revision for some patients whose treatment initially fails. Fortunately, the percentage of patients who require ≥3 sialendoscopies is likely small and would not affect our conclusions significantly. In addition, we incorporated a recurrence rate for sialolithiasis in the same gland, which can result in multiple revisions for a small subset of patients. Despite these limitations, we believe that this analysis is helpful in determining the appropriateness of gland preservation with sialendoscopy, particularly in the United States, where our health insurance and reimbursement structures are unique when compared with the rest of the world.
Conclusion
Sialendoscopy appears to be a cost-effective management strategy for sialolithiasis of the submandibular gland when the probable outcome of successful stone removal reaches ≥61%. An operation that exceeds approximately $12,000 would not be considered cost-effective by our best estimation. Further studies elucidating the clinical factors that determine successful sialendoscopy may be aided by these thresholds as well as future comparisons of novel technology.
Supplemental Material
sj-pdf-1-oto-10.1177_01945998211026847 – Supplemental material for Cost-effectiveness Analysis of Submandibular Gland Preservation With Sialendoscopy for the Management of Sialolithiasis
Supplemental material, sj-pdf-1-oto-10.1177_01945998211026847 for Cost-effectiveness Analysis of Submandibular Gland Preservation With Sialendoscopy for the Management of Sialolithiasis by Joseph R. Acevedo, Ashley C. Hsu, Jeffrey C. Yu, Dale H. Rice, Daniel I. Kwon, Raymond W. Kung and Niels C. Kokot in Otolaryngology–Head and Neck Surgery
Footnotes
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.