
Abstract
Objective
To compare rates of cochlear implant referral and cochlear implantation across different races and to compare audiometric profiles of these patients.
Study Design
Retrospective study.
Setting
Academic tertiary care institution.
Methods
Demographic and audiometric data were collected for patients who underwent cochlear implant evaluation or cochlear implantation from 2010 to 2020.
Results
A total of 504 patients underwent cochlear implant evaluation; 388 met cochlear implant candidacy criteria, and 258 underwent implantation. Of the patients referred for cochlear implant evaluation, 68.5% were White, 18.5% were Black, and 12.3% were Asian, while the institution’s primary service area is 46.9% White, 42.3% Black, and 7.7% Asian (P < .001). Black patients referred for cochlear implant evaluation had significantly worse hearing (mean pure-tone average [PTA] 84.5 dB, 26.1% word recognition) than White patients (mean PTA 78.2 dB, P = .005; 35.7% word recognition, P = .015) and Asians patients (mean PTA 77.9 dB, P = .04; 36.5% word recognition, P = .04). Black patients who underwent cochlear implant evaluation also had significantly worse AzBio scores than White patients: 24.5% versus 36.7% (P = .003). There was no significant difference in cochlear implantation rates between Black and White candidates (P = .06).
Conclusion
Black patients undergo cochlear implant evaluation and cochlear implantation at rates disproportionately lower than expected based on local demographics. In addition, Black patients have significantly worse hearing at the time of cochlear implant referral than White and Asian patients. Identifying and increasing awareness of these disparities are essential steps to improving cochlear implant access for potentially disadvantaged populations.
Keywords
Approximately 15% of adults in the United States experience debilitating hearing loss, leaving them susceptible to increased rates of hospitalization, depression, dementia, and death.1-3 A cochlear implant (CI) is a cost-effective device that can restore hearing in individuals with severe to profound sensorineural hearing loss, 4 yet only 5% to 7% of adults who could benefit from an implant undergo cochlear implantation.5-7 Lack of awareness among primary care physicians, insufficient screening, limited patient understanding, financial constraints, and distance to CI centers have previously been cited as possible explanations for low referral and implantation rates.5-11 Patient demographics, however, may also play a significant role in the relatively low CI utilization rates in adults.8-13
Until recently, the vast majority of the published literature on racial and socioeconomic disparities in cochlear implantation has focused on the pediatric population.14-19 White and Asian children have been shown to undergo cochlear implantation at higher rates than their Black and Hispanic counterparts.15,18,19 Furthermore, pediatric patients with private insurance and higher median household incomes are more likely to undergo cochlear implantation.14-17 These studies have highlighted at-risk populations who may benefit from interventions to increase awareness of CI and potentially improve implantation rates. Recently published studies of adult patients have similarly demonstrated that non-White adults undergo cochlear implantation at lower rates than White adults, but the data remain limited.12,13 Given the debilitating nature of adult hearing loss and the known benefits of cochlear implantation, it is important to expand upon the existing literature to identify similarly vulnerable adult populations who may benefit from increased outreach and education about cochlear implantation.
Among all states in the United States, Georgia has the fourth highest percentage of Black residents, at 32.6%. 20 Atlanta, Georgia, alone is composed of 51% Black residents, which is much greater than other urban settings, including New York City (24.3%), Los Angeles (8.9%), Chicago (29.6%), and Houston (22.6%). 21 Emory Healthcare serves the patients of Atlanta and its surrounding communities, making its patient population an appropriate, and relatively unique, sample to evaluate health disparities among adults undergoing CI evaluation (CIE) and cochlear implantation. Furthermore, Emory is the predominant CI provider in the Atlanta area, and approximately 49.5% of Georgia’s Black residents reside in Emory Healthcare’s primary service area.20-22 This study aims to compare rates of CI referral and implantation across patients of different racial and socioeconomic backgrounds. This study will also compare the audiometric profiles across races of patients who are referred for CI. Overall, we intend to bring attention to vulnerable patient populations who may benefit from more intensive outreach, screening and support with a larger end goal of improving CI access and utilization.
Methods
This retrospective study was approved by the Emory University Institutional Review Board (No. 00001295). Medical records were reviewed to identify adult patients aged 18 years and older who underwent CIE and/or cochlear implantation at Emory Healthcare between January 1, 2010, and August 1, 2020. Patients with single-sided deafness were excluded. Demographic data collected included age, gender, ethnicity, race, language, insurance provider, and zip code. Language was categorized as English, sign language, unknown, or other (including Amharic, Bengali, Chinese, Korean, Spanish, and Vietnamese). Insurance provider was categorized as public (including Veterans Affairs), private, or self-pay. Patient home zip codes corresponded to their residence at the time of data collection. Median household income was categorized as greater or less than $50,000 based on patient zip code using Zip Atlas, a detailed demographic database for all 50 states in the United States. 23 Racial demographics were collected for Emory Healthcare’s Primary Service Area, which covers 6 Atlanta-area counties including Dekalb, Fulton, Cobb, Gwinnett, Henry, and Clayton counties. 22
Audiometric data collected via manual record review included pure-tone thresholds, word recognition score (WRS), open-set sentence testing scores in quiet (AzBio), and CI candidacy status. All audiometric testing was performed in English using recorded materials. A 3-frequency pure-tone average (PTA) was calculated using the air conduction thresholds at 500, 1000, and 2000 Hz. Results for the better-hearing ear were reported for PTA, WRS, and AzBio. Patients were identified as candidates for cochlear implantation by Federal Drug Administration criteria (≤50% aided sentence recognition in the ear to be implanted and ≤60% in the contralateral ear) if they had private insurance and by Medicare criteria (≤40% aided sentence recognition) if they had Medicare insurance at the time of CIE. 24
Statistical analysis was performed using SPSS (version 27.0, IBM Corporation, Armonk, New York). Outcome variables assessed include age, gender, ethnicity, race, type of insurance, language, and median household income category. Two-sample t tests and 1-way analysis of variance were used to assess continuous variables, including age and audiometric data. Chi-squared analyses were performed to compare categorical demographic characteristics. Fisher exact test was performed when more than 20% of expected cells had values <5. Odds ratios (OR) and corresponding 95% confidence intervals (CI) were calculated for categorical variables analyzed. All variables with a P value <.05 were considered statistically significant.
Results
Patient Demographics
During the study period, 504 patients were referred for CIE. The mean age of the patients undergoing CIE was 65.7 (±18.4) years; 51.4% (259) of patients were female, 68.5% (345) of patients self-identified as White, 18.5% (93) as Black, and 12.3% (62) as Asian. The remaining 0.8% (4) of patients identified as either multiple races or Native Hawaiian/Pacific Islander. Of all patients, 81.2% (409) were English speaking, and 51% (257) had public insurance ( Table 1 ).
Patient Summary.
Abbreviation: CI, cochlear implant.
Of the patients who underwent CIE, 77% (388) met CI candidacy criteria. The mean age of the CI candidates was 64.7 (±18.7) years, and 53.9% (209) were female. The racial distribution of CI candidates was 68.8% (267) White, 20.4% (79) Black, and 9.8% (38) Asian. Of the candidates, 85.1% (330) were English speaking, and 50.8% (197) had private insurance.
Of the 388 CI candidates, 67% (258) underwent implantation. The mean age of the patients at the time of implantation was 63.1 (±16.4) years, and 56.6% (146) of patients implanted were female. The racial distribution of patients who underwent implantation was 74% (191) White, 18.6% (48) Black, and 6.2% (16) Asian. Of all implanted patients, 89.1% (230) were English speaking, and 50.2% (130) of patients who underwent implantation had private insurance.
Racial Trends in CI Referral Rates
Black patients represented 18.5% of patients who underwent CIE. This is significantly less than their proportion of both the local and state populations ( Figure 1 ). Black residents constitute 42.3% of Emory’s primary service area (P < .001), 51% of the city of Atlanta (P < .001), and 32.6% of the state of Georgia (P < .001).20,21,23 In contrast, the proportion of White and Asian patients who underwent CIE was significantly greater than their representation in the local population: 68.5% of patients who underwent CIE were White, whereas White residents make up 46.9% of Emory’s primary service area (P < .001), 40.9% of Atlanta (P < .001), and 60.2% of Georgia (P < .001).20,21,23 Likewise, 12.3% of patients who underwent CIE were Asian, while Asian residents account for 7.7% of Emory’s primary service area (P < .001), 4.4% of Atlanta (P < .001), and 4.4% of Georgia (P < .001).20,21,23 Similarly disproportionate numbers were demonstrated for patients who underwent cochlear implantation ( Figure 2 ).
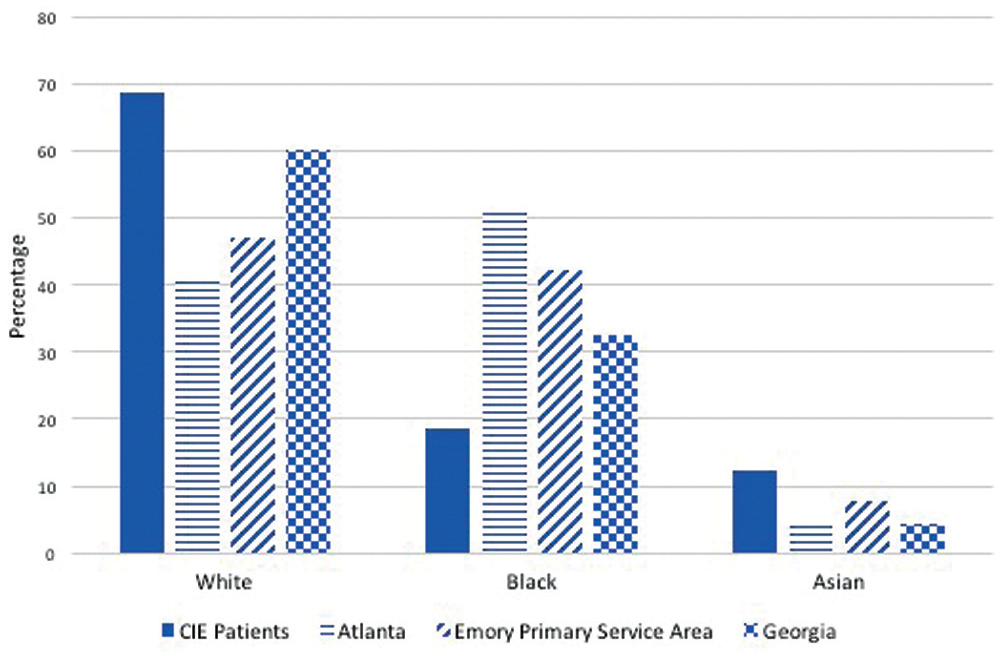
Demographic comparison of patients undergoing cochlear implant evaluation (CIE). Percentage of all patients who underwent CIE compared with local population demographics.
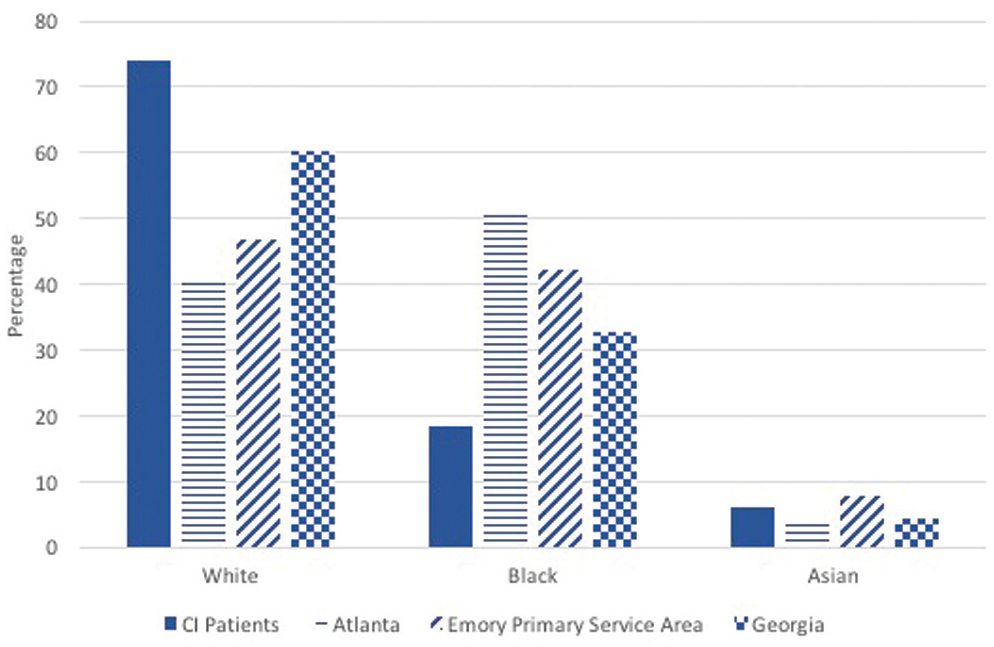
Demographic comparison of patients undergoing cochlear implantation (CI). Percentage of all CI candidates who underwent CI compared with local population demographics.
Audiometric Testing Results
The mean PTA and WRS for all patients who underwent CIE were 79.3 (±19.0) dB and 34.4% (±22.4%). The mean aided AzBio score was 35.6% (±32.4%; Table 2 ).
Audiometric Results. a
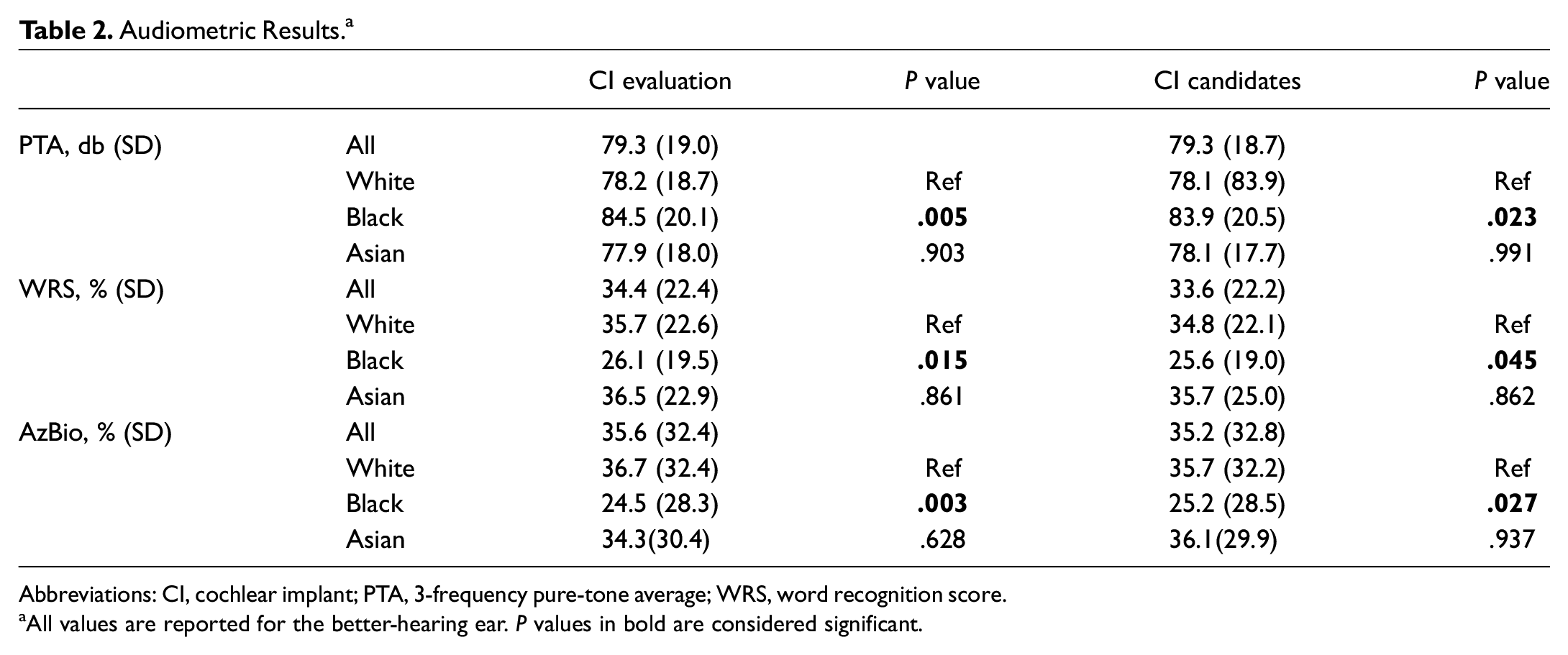
Abbreviations: CI, cochlear implant; PTA, 3-frequency pure-tone average; WRS, word recognition score.
All values are reported for the better-hearing ear. P values in bold are considered significant.
Black patients referred for CIE performed significantly worse than White and Asian patients did on audiometric testing. The mean unaided PTA for Black patients was 84.5 (±20.1) dB, compared with 78.2 (±18.7) dB for White (P = .005) and 77.9 (±18.0) dB for Asian patients (P = .04). The mean unaided WRS for Black patients was 26.1% (±19.5), compared with 35.7% (±22.6%) for White (P = .015) and 36.5% (±22.9) for Asian patients (P = .04). The mean aided AzBio score for Black patients was 24.5% (±28.3%) compared with 36.7% (±32.4%) for White patients (P = .003) and 34.3% (±30.4%) for Asian patients (P = .075). These differences were also demonstrated among patients who met CI candidacy criteria ( Table 2 ).
Rates of CI Candidacy Across Races
Of White patients, 77% (267) met CI candidacy criteria compared with 85% (79) of Black patients (P = .095) and 61% (38) of Asian patients (P = .008; Table 3 ). Black and Asian CI candidates were significantly younger than White CI candidates: 61.4 (±16.4) years and 62.0 (±19.3) years compared with 66.0 (±19.1) years (P = .048; Table 1 ). Gender was not significantly associated with CI candidacy when comparing White patients to Black and Asian patients. However, Asian patients with public insurance and a median household income of less than $50,000 were significantly less likely to meet CI candidacy criteria (P = .007 and P = .002, respectively). A significantly greater proportion of Black patients with median household income greater than $50,000 met candidacy criteria than White patients with a median household income greater than $50,000 (P = .01).
Cochlear Implant Candidacy and Surgery Rates by Race. a
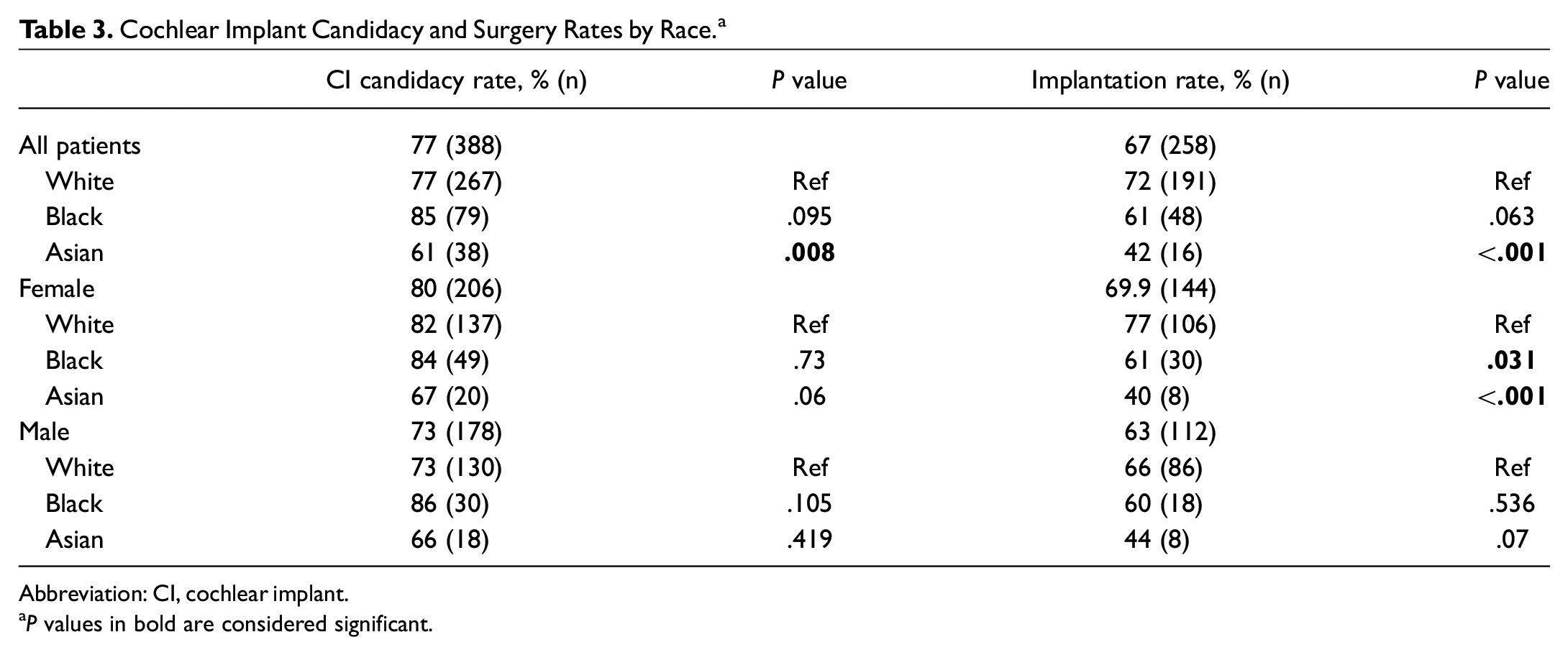
Abbreviation: CI, cochlear implant.
P values in bold are considered significant.
Rates of Cochlear Implantation Across Races
Of White CI candidates, 72% (191) underwent implantation compared with 61% (48) of Black CI candidates (P = .06) and 42% of Asian CI candidates (P < .001; Table 3 ). Black patients who underwent cochlear implantation had significantly worse PTAs than White patients ( Table 2 ). Among female CI candidates, Black females (P = .03) and Asian females (P < .001) were significantly less likely to undergo implantation than White females were. This difference was not seen when comparing White male candidates to Black male candidates (P = .54) or Asian male candidates (P = .07). Among patients with a median household income of less than $50,000, Asian patients were less likely to undergo implantation (P = .001). Median household income was not significantly associated with the likelihood of Black patients undergoing implantation in comparison with White patients (P > .05). Across all races, type of insurance provider was also not significantly associated with undergoing cochlear implantation (P > .05).
Discussion
This study demonstrates racial disparities among patients who are referred for CI evaluation and, consequently, among patients who go on to undergo cochlear implantation. Only 18.5% of patients referred for CIE were of Black race. This is significantly disproportionate to Emory Healthcare’s primary service area and the state of Georgia, which are, respectively, 42.3% and 32.6% Black (P < .001).20,23 White and Asian patients, on the other hand, were referred for CIE at rates greater than their representation in the local population ( Figure 1 ).
Our findings are consistent with recent reports from other academic CI centers. Holder et al demonstrated an underrepresentation of African Americans undergoing CIE at Vanderbilt University: 7% of patients were African American, compared with Nashville, Tennessee’s 17.1% Black/African American population. 11 Tolisano et al 13 similarly reported on the “homogeneity” of patients undergoing CIE at UT Southwestern in Dallas, Texas; their patients were 88.2% White and 91.3% non-Hispanic, in contrast to Dallas–Fort Worth’s 47% White and 71% non-Hispanic population. 13
Our study also demonstrates that Black patients who are referred for CI evaluation have worse hearing than White and Asian patients on standard audiometry as well as on CI candidacy testing. This is consistent with Dornhoffer et al, 12 who demonstrated worse aided hearing scores among non-White patients compared with White patients. Delayed presentation for CIE can be attributed to both patient and physician factors. Familiarity with cochlear implantation remains low among primary care physicians, and consequently, many patients remain unaware of the device. 6 Lack of CI awareness is further exacerbated among patients with lower health literacy, which has historically limited Black patients’ navigation of the health care system. 25
In addition to primary care providers, audiologists and even otolaryngologists may also play a role in patients’ delayed referral for CI. Poorly defined criteria for CIE referral has been commonly cited as contributing to low CI referral rates across the United States.6,7 In an effort to improve CI referral rates, Zwolan et al 26 proposed a 60/60 guideline that recommends that patients with a PTA ≥60 dB and a WRS ≤60% be referred for CIE. They found that, when applied, the 60/60 rule was 96.3% sensitive and 65.6% specific for identifying CI candidates. 26 The severity of hearing loss of our study population as a whole ( Table 2 ) exceeds Zwolan’s proposed 60/60 guideline for CIE referral, indicating a possible delayed referral for patients across all races.
Another significant barrier to cochlear implantation is insurance coverage of the device and the surgical procedure. Georgia Medicaid does not cover cochlear implantation in adults, and consequently, none of the patients in our study had Medicaid insurance. Approximately 540,000 adult Georgians have Medicaid insurance, and another 1.4 million are uninsured.27-29 Almost half (47.8%) of Georgia Medicaid enrollees are of Black race. 30 Georgia’s large uninsured and underinsured population certainly contributes to the proportionally low number of Black patients undergoing CIE and CI at our institution. Along the same lines, Medicare Part A covers only 80% of the cost of an implant, leaving the remaining charges to be covered by the patient through the Medicare Part B supplement or self-pay. 31 Among our implantees, all patients with Medicare insurance had Part B supplemental coverage. These data emphasize the known impact of inadequate insurance coverage on access to cochlear implantation. While interventions aimed at screening and evaluation can prove useful, it is imperative to recognize the financial and insurance barriers that exacerbate disparities in CI referral and implantation rates.
Moreover, at our institution, only 5% of patients seen by audiology and 7% of patients seen by otology for any reason, not just CI, have Medicaid insurance. Most of these Medicaid patients are of Black race: 57% of audiology Medicaid and 54% of otology Medicaid patients are Black. This suggests that Medicaid patients not only lack access to cochlear implantation, but also have limited access to hearing health care services.
Notably, our study did not demonstrate a significant difference in the rate of cochlear implantation between White and Black CI candidates. This is in contrast to previous findings that non-White CI candidates are less likely to undergo cochlear implantation than White candidates are. 13 Neither our study nor the study by Tolisano et al 13 investigated the reasons why some patients did not undergo CI; however, the more profound, debilitating nature of hearing loss among Black patients in comparison with White patients in our study may explain Black patients’ motivation to seek and accept hearing rehabilitation. Along the same lines, health care providers may more easily identify these patients as at risk for hearing-related morbidities and refer for a hearing evaluation. The similar rates of cochlear implantation across Black and White CI candidates at our institution is further evidence that a significant barrier exists at the level of the initial referral.
The racial disparities demonstrated in adult cochlear implantation are not unique. Disparities in access to care among the Black community have been reported among patients suffering from head and neck cancer, breast cancer, and HIV/AIDS, among others.32-34 Sims et al 9 found that patient-physician mistrust, social stigma, financial cost, and lack of education about cochlear implantation were key barriers to Black patients pursuing evaluation and, ultimately, implantation. Those same factors have been identified as barriers to care for Black patients across multiple health care settings.25,32-34 Inadequate or altogether lack of insurance coverage in adults further exacerbates these disparities. The demonstration of similar racial inequities among Black patients across multiple health care domains highlights the need for large-scale interventions to improve access to both cochlear implantation and health care at large.
Study Limitations
Race, ethnicity, and language data are self-reported and limited the analysis of these demographic variables. A total of 123 (24.4%) and 71 (14.1%) patients did not identify their ethnicity and language, respectively, in the CIE patient cohort. In addition, the retrospective nature of this study precludes any investigation into patient decision making. We did not capture or investigate patients who were referred for, but did not undergo, CIE, nor do we have information as to why some CI candidates did not undergo surgery. Possible reasons that CI candidates did not undergo cochlear implantation include medical comorbidities, patient decision-making factors, decision to pursue surgery elsewhere, and CI surgery being completed after study end date. Identifying the tenets by which patients make the decision to pursue hearing or surgical intervention is critical to illuminating areas for intervention and/or improvement.
In this study, we have chosen to focus on race as a social determinant of health. While we were able to identify a vulnerable racial group, we acknowledge that this study does not address the ethnic heterogeneity within each racial group. Nevertheless, our study can serve as a foundation for future studies to further evaluate these at-risk racial groups.
Future Directions
As we work to address these disparities in care, it is necessary to identify key areas for intervention. Studies that seek to improve understanding of barriers non-White patients may face in pursuing audiological evaluation and hearing rehabilitation (surgical and nonsurgical) would provide useful information. One must also consider health care provider biases in referring patients for audiological services or cochlear implantation—a process that is very subjective. Implicit biases in medicine have been studied across many fields, but special attention to these same decision-making barriers have not been examined as they relate to hearing rehabilitation.35,36 Lastly, we cannot ignore the insurance barrier that makes cochlear implantation financially inaccessible to many adult patients.
Conclusion
This study demonstrates that Black patients undergo CI evaluation and cochlear implantation at rates disproportionately lower than expected based on local population demographics. In addition, Black patients referred for CIE have significantly worse hearing than White and Asian patients. Identifying and increasing awareness of these disparities are critical steps to improving CI access for potentially disadvantaged populations.