
Abstract
Objectives
To review the normative data for acid, weakly acid, and nonacid proximal esophageal (PRE) and hypopharyngeal reflux (HRE) events in diagnosing laryngopharyngeal reflux (LPR) using ambulatory reflux monitoring.
Data Sources
PubMed, Cochrane Library, and Scopus.
Review Methods
A literature search was conducted about the normative data for PRE and HRE on multichannel intraluminal impedance–pH monitoring (MII-pH), hypopharyngeal-esophageal MII-pH (HEMII-pH), or oropharyngeal pH monitoring using PICOTS (population, intervention, comparison, outcome, timing, and setting) and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statements. Outcomes reviewed included device characteristics, impedance/pH sensor placements, study duration, number/average and percentiles of PRE or HRE occurrence, and the event characteristics (pH, composition, and position).
Results
Of 154 identified studies, 18 met criteria for analysis, including 720 healthy individuals. HEMII-pH, MII-pH, and oropharyngeal pH monitoring were used in 7, 6, and 5 studies, respectively. The definition and inclusion/exclusion criteria of healthy individuals varied substantially across studies, with 6 studies considering only digestive symptoms to exclude potential LPR patients. Substantial heterogeneity across studies was noted, including impedance/pH sensor placements/configurations and definitions of composition (liquid, gas, mixed) and type (acid, weakly acid, nonacid) of PRE/HRE. The 95th percentile thresholds were 10 to 73 events for PRE, 0 to 10 events for HRE on HEMII-pH, and 40 to 128 for events with pH <6.0 on oropharyngeal pH monitoring. Most HREs were nonacid and occurred upright. The mean HRE among healthy individuals was 1.
Conclusion
The low number of studies and the heterogeneity in inclusion criteria, definitions, and characterization of PRE and HRE limit the establishment of consensual normative criteria for LPR on ambulatory reflux monitoring. Future large multicenter studies are needed.
Laryngopharyngeal reflux (LPR) is an inflammatory condition of the upper aerodigestive tract tissues related to direct and indirect effect of gastroduodenal content reflux, which induces morphological changes in the upper aerodigestive tract. 1 LPR-related symptoms are found in 10% to 30% of outpatients consulting in the otolaryngology department2,3 and up to 50% of patients with dysphonia. 4 Symptoms and signs associated with LPR are nonspecific and may be encountered in many other otolaryngological conditions, including primary voice disorders, chronic rhinosinusitis, allergy, or chronic laryngopharyngitis due to tobacco or alcohol.1,5,6 The poor specificity of both symptoms and laryngoscopic findings for LPR highlights the important role of objective reflux assessments in the diagnosis of LPR, such as ambulatory reflux monitoring. Over the years, several types of ambulatory reflux monitoring modalities have been developed for the diagnosis of gastroesophageal reflux, including pH testing and multichannel intraluminal impedance (MII) measurements, as well as devices that allow analyses at various anatomic locations. Of these, the combined hypopharyngeal-esophageal MII–pH monitoring (HEMII-pH) and oropharyngeal pH study (Restech) were 2 technologies specifically designed for the diagnosis of LPR. 1 Although these approaches are recognized as the primary ways to objectively measure LPR and support the diagnosis, there are, to date, no consensus criteria regarding the thresholds of esophago-hypopharyngeal reflux episodes to define LPR.
Given the significant heterogeneity in technologies used, study protocols employed, and cohort inclusion and exclusion criteria, we hypothesized that a universal, gold-standard normative value for LPR across diagnostic modalities may be elusive under the currently available data in the literature. However, a careful analysis of the aggregate data to date would allow better insight into the current understanding of LPR diagnostic challenges and future research needs. The aim of this study was to systematically review the current literature regarding the normative ambulatory reflux monitoring data for LPR events using HEMII-pH, MII-pH, and oropharyngeal pH study.
Materials and Methods
Search Strategy
Three independent authors (J.R.L., F.B., C.M.C.-E.) conducted an electronic search using PubMed, Cochrane Library, and Scopus to identify studies investigating the normative data for LPR events on ambulatory reflux monitoring. The following search terms were used as both keywords and medical subject heading terms, where applicable: reflux, laryngitis, laryngopharyngeal, gastroesophageal, silent reflux, pH study, impedance, monitoring, normative, healthy, criteria, diagnosis, and data. Studies were considered if they had database abstracts, available full texts, or titles containing the search terms. Results of the search strategy were reviewed for relevance, and the reference lists of these articles were examined for additional pertinent studies.
Study Selection and Data Synthesis
The criteria for consideration of study inclusion for the systematic review were based on the population, intervention, comparison, outcome, timing, and setting (PICOTS) framework. 7 The review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist for systematic reviews. 8 For each included study, 2 authors independently reviewed and extracted the data. Any discrepancies in synthesized data were discussed and resolved by the remaining coauthors.
Types of studies
Studies were included if they investigated the ambulatory reflux monitoring findings in healthy, asymptomatic adults with no LPR or esophageal symptoms, through retrospective or prospective, controlled or uncontrolled studies. All studies evaluating these approaches were included in the review: HEMII-pH, MII-pH, and oropharyngeal pH study (Restech). The studies had to be published in English or French peer-reviewed journals. Only studies reporting data for more than 10 individuals were considered.
Populations, inclusion/exclusion criteria
Eligible studies should include healthy adults without symptoms and signs of LPR. Studies were only included if the authors clearly provided the inclusion and exclusion criteria used. Controlled, comparative studies were eligible as long as the study cohorts contained an arm of healthy, asymptomatic individuals. Studies investigating normative data for gastroesophageal reflux disease (GERD) without proximal esophageal/hypopharyngeal findings were not considered.
Among controlled studies, the criteria for LPR diagnosis were analyzed. Patients with esophago-hypopharyngeal reflux episodes detected by HEMII-pH, MII-pH, or oropharyngeal pH study were considered LPR patients. Patients with reflux esophagitis or positive DeMeester score and increased reflux burden, ambulatory reflux monitoring, but no hypopharyngeal reflux episodes were considered GERD, but not LPR, patients. Subjects with only a clinical diagnosis of LPR without objective testing were considered “suspected LPR patients.”
Outcomes
The following outcomes were reviewed: testing modality used (HEMII-pH, MII-pH, or oropharyngeal pH study); probe placement; placement and number of impedance segments and pH electrodes; definitions of proximal (PRE) or hypopharyngeal (HRE) reflux episodes and liquid, gas, or mixed events; definitions of acidic, weakly acidic, mixed, nonacidic, and variant reflux episodes; and time of recording. Moreover, the following characteristics of the included studies were also collected: number of subjects, age, sex, inclusion/exclusion criteria for healthy individuals, and, in controlled studies, potential LPR patients and the method/criteria used for the reflux diagnosis.
The Tool to Assess Risk of Bias in Cohort Studies developed by the Clarity Group and Evidence Partners was used by 2 authors (J.R.L. and C.M.C.-E.) for the bias/heterogeneity analyses of the included studies. 9
Intervention and comparison
Because the objective of this systematic review is to analyze the normative data for LPR events, the included studies did not have to detail treatment approaches or response.
Timing and setting
As this was an analysis of normative data in healthy individuals, there were no criteria for specific stage or timing in the “disease process” of the study population.
Results
A total of 154 articles were identified and 18 studies met our inclusion criteria ( Figure 1 ).10-26 MII-pH and HEMII-pH were used in 13 studies ( Table 1 )10-12,14-17,19-23 while oropharyngeal pH monitoring was used in 5 studies ( Table 2 ).13,18,24-27 There were 16 prospective controlled (n = 6) or uncontrolled (n = 10) studies and 2 retrospective cohorts. Two studies were excluded due to patient overlap 28 and the inclusion of patients with nonerosive reflux disease as “healthy” controls. 29 A meta-analysis was found that specifically focused on normative criteria for acidic LPR using findings from dual- or triple-channel esophageal pH monitoring, without inclusion of impedance data. 30

Flowchart. (HE)MII-pH, (hypopharyngeal-esophageal) multichannel intraluminal impedance pH monitoring.
Features of Included Studies Using Multichannel Intraluminal Impedance pH Monitoring.
Abbreviations: BMI, body mass index; EL, evidence level; GERD, gastroesophageal reflux disease; Gr, grade; HEMII-pH, hypopharyngeal-esophageal multichannel intraluminal impedance–pH monitoring; HRE, hypopharyngeal reflux episodes; IE, impedance electrodes; LES, lower esophageal sphincter; LPR, laryngopharyngeal reflux; M, manufacturer; md, median; MII-pH, multichannel intraluminal impedance–pH monitoring; NA, not available; NS, nonsignificant; PE, proximal esophagus; PRE, proximal esophageal reflux episodes; UES, upper esophageal sphincter.
Features of Included Studies Using Oropharyngeal pH Study.
Abbreviations: BMI, body mass index; EL, evidence level; GERD, gastroesophageal reflux disease; Gr, grade; HRE, hypopharyngeal reflux episodes; IE, impedance electrodes; LPR, laryngopharyngeal reflux; md, median; NA, not available; NS, nonsignificant; —, no information available.
The included studies comprised a total of 720 healthy individuals, with 363 (50.4%) women and a mean age of 35.7 years. The mean body mass index, which was provided in 6 studies,14-17,20,24 was 22.8 kg/m2. The inclusion and exclusion criteria substantially varied among studies ( Table 3 ). Six studies based the inclusion of healthy individuals on the lack of gastroesophageal reflux symptoms without consideration for laryngopharyngeal reflux symptoms.10-12,15,20,25 LPR symptoms were considered in 11 studies.* The inclusion criteria of healthy subjects were not provided in 1 study. 22 Heterogeneity among included articles in inclusion/exclusion criteria, ambulatory reflux monitoring characteristics, and outcomes measures, as well as the nonnormal distribution of measured outcomes, precluded statistically pooling the data into a formal meta-analysis, thereby limiting the analysis to a qualitative rather than quantitative summary of the available information.
Inclusion or Exclusion Criteria of Healthy Individuals.
Abbreviations: GER, gastroesophageal reflux; GERD-HRQoL, gastroesophageal reflux disease–high related quality of life; GERDQ, gastroesophageal reflux disease questionnaire; GI, gastrointestinal; HP, Helicobacter pylori; LPR, laryngopharyngeal reflux; NA, not available; PPI, proton pump inhibitor; RFS, reflux finding score; RSI, reflux symptom score.
Study Characteristics and Level of Evidence
There were 4 prospective controlled studies (evidence level [EL] = B), 9 prospective uncontrolled studies (EL = C), and 2 retrospective chart reviews (EL = D). One controlled study compared healthy individuals with patients with LPR or chronic rhinosinusitis. 27 There was an important heterogeneity between studies regarding the inclusion and exclusion criteria used to include healthy individuals. Among the controlled studies, the LPR diagnosis substantially varied. In the study by Xiao et al, 15 LPR diagnosis was defined as a percentage of total time for which the pH value below 4, detected 5 cm above the lower esophageal sphincter (LES), was >4.2%. Jetté et al 19 considered LPR in patients with >31 PRE, while Hoppo et al 16 made the diagnosis in individuals with ≥1 HRE. In these 3 controlled studies, the mean age of healthy controls was significantly lower than the mean age of LPR patients. The bias analysis is available in Appendix 1 (in the online version of the article). The inclusion and exclusion criteria were evaluated as highly reliable in 4 studies.
Note that the exclusion criteria were assessed through structured or unstructured questionnaire in all studies with the exception of the study by Ayazi et al, 25 which excluded gastrointestinal dysmotility and other esophageal diseases after dual-probe esophageal pH monitoring, video esophagram, and esophageal manometry. Based on the type of ambulatory reflux monitoring used, the assessment of normative data for HRE was performed in 8 studies.13-18,21,23 Among them, the definition of HRE was clearly provided in 7 studies.14-18,21,23 The classification of reflux events according to the pH level (acid, weakly acid, nonacid, superimposed acid, and acid-to-nonacid) was available in 7 studies.10-12,14-16,20 The composition of reflux events, including gas, liquid, and mixed compositions, was clearly provided/defined in 10 studies.10-12,14-17,20,21,23 Overall, comprehensive information inclusive of clear definitions of reflux events, acidity of episodes, and composition of PRE/HRE was fully available in 3 studies.14-16
Device and Ambulatory Reflux Monitoring System
The following systems for ambulatory reflux monitoring were used in the included studies: MII-pH without hypopharyngeal impedance channels (n = 6),10-12,19,20,22 HEMII-pH (n = 7),14-17,21,23,27 and oropharyngeal pH study (n = 2).13,18,24-26 In 2 studies, patients underwent simultaneous oropharyngeal and esophageal pH monitoring.13,26 The placement of MII-pH or HEMII-pH probes was guided by esophageal manometry,10-14,17,19-22 transnasal esophagoscopy, 16 or flexible laryngoscopy.23,27 The placements of oropharyngeal pH study devices were confirmed visually.18,24-26 Information on methodology of catheter placement was lacking in 1 study. 15 The duration of ambulatory reflux monitoring ranged from 14 to 24 hours ( Tables 1 and 2 ). Among the 6 studies using MII-pH without hypopharyngeal pH or impedance sensors, pH monitoring was measured using 1 (n = 4)10-12,22 or 2 (n = 2) esophageal sensors (n = 2).19,20 The location and number of impedance electrodes used in MII-pH or HEMII-pH varied substantially among studies ( Table 1 ). Depending on the device, the hypopharyngeal pH sensor was located 0.5 to 1.0 cm above the upper esophageal sphincter (UES)14-17,21,23 or in the oropharyngeal cavity.13,18,24-26
Reflux Event Definition
The definitions of PRE or HRE were available in 11 studies using MII-pH or HEMII-pH ( Table 4 ). PRE was uniformly defined across studies. The definition of HRE significantly differed across studies ( Table 4 ). The definitions of the composition of reflux event (gas vs liquid vs mixed) were available in 11 studies ( Table 4 ). We found 2 different definitions of gas and liquid reflux events, although in both cases, 10 of 11 studies agreed on 1 of the 2 definitions ( Table 4 ). Mixed reflux events were defined in 3 different ways, with 7 studies using the definition of gaseous reflux episode occurring before or during a liquid reflux event ( Table 4 ). The types of reflux events (acid vs weakly acidic vs alkaline) were classified according to the pH level, as shown in Table 5 . In general, acid reflux events were defined by pH <4, while weakly acidic reflux comprised events with pH between 4 and 7. There was some heterogeneity among authors in the definition of weakly acidic vs nonacid or weakly alkaline PRE or HRE, namely, those events with pH >4. While some studies classified events with pH between 4 and 7 as weakly acidic events and those with pH >7 as weakly alkaline events, others summarily labeled all events with pH >4 as nonacidic.
Definitions of Proximal Esophageal and Hypopharyngeal Reflux Episodes According to Studies.
Abbreviations: GER, gastroesophageal reflux; HRE, hypopharyngeal reflux episode(s); LES, lower esophageal sphincter; LPR, laryngopharyngeal reflux; UES, upper esophageal sphincter.
Definition of the Reflux Events According to pH.
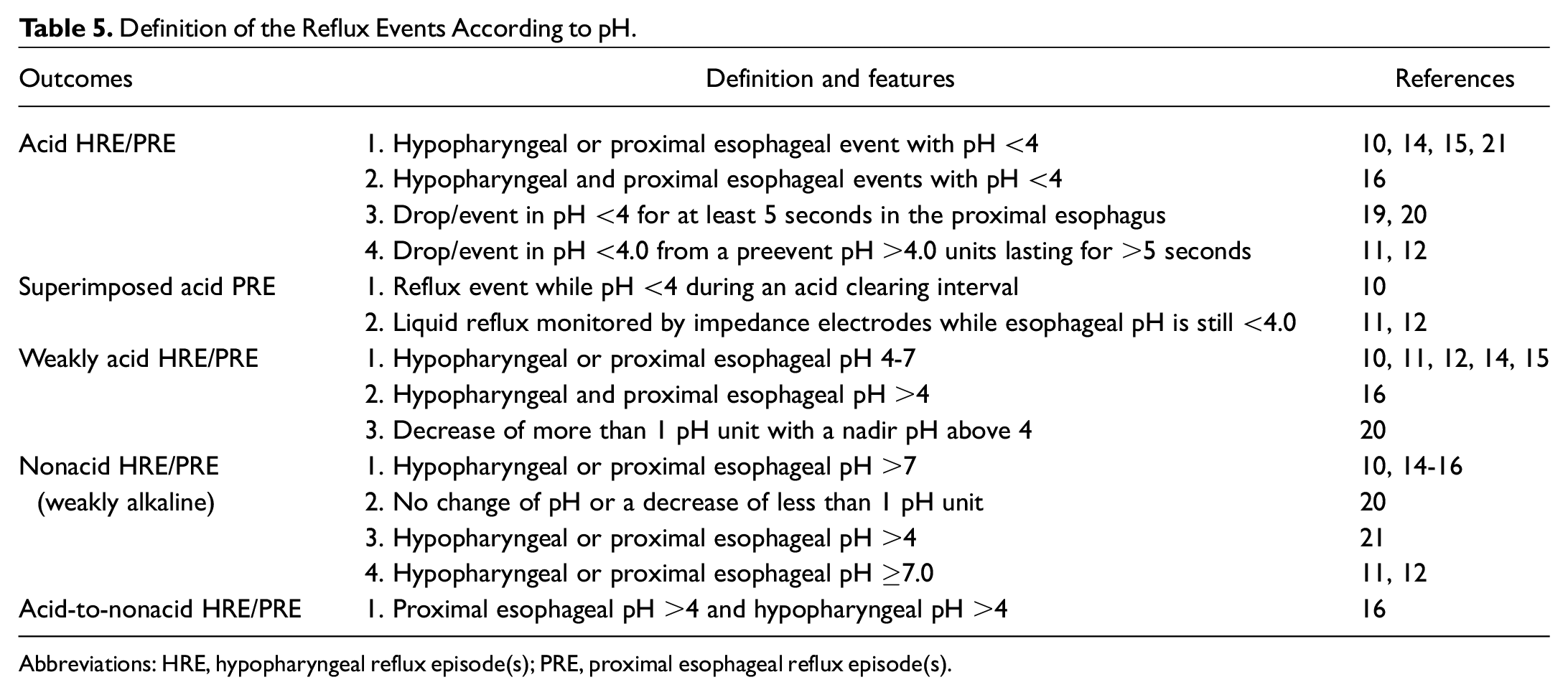
Abbreviations: HRE, hypopharyngeal reflux episode(s); PRE, proximal esophageal reflux episode(s).
No definitions of weakly acidic or nonacid pharyngeal events were provided in studies using oropharyngeal pH monitoring, as it is a pH-only technology where reflux events themselves are defined by pH value decrease.
Proximal Esophageal Reflux Episodes
The normative value for PRE was determined by the 95th percentile number of events among healthy individuals in most studies.10-12,20 The following 95th percentile values for PRE were established: 10, 14 31, 10 32, 12 34 (female) to 70 (male), 11 and 73. 20 Considering the acidity of the PRE, the 95th percentile number of acid (pH <4.0) PRE ranged from 4 to 34,10,12,14,20 while the 95th percentile number of weakly acidic (pH 4.0 to 7.0) PRE ranged from 0 to 25.10,12,14,20 For weakly alkaline events (pH >7), the 95th percentile value ranged from 0 to 56.10,12,14 Desjardin et al 17 reported their results in terms of mean number of events, with mean PRE pH <4 of 1 and mean PRE pH <5 of 1. In the study by Jetté et al, 19 the mean number of PREs was 23.8 ± 14.0, with a higher number of acid (pH <4) events (14.7 ± 11.3) compared to nonacid (pH >4) events (9.0 ± 6.7). According to studies where the data were reported,10-12,14 most PREs occurred during daytime and in the upright position, and they may be more frequently gaseous 20 ( Table 1 ). Acid PREs, but not nonacid PREs, were reported to be more frequent in LPR patients compared to healthy controls in 1 study. 21
Hypo- and Oropharyngeal Reflux Episodes
Hypopharyngeal reflux event (HEMII-pH studies)
The 95th percentile values of HRE measured by HEMII-pH ranged from 016 to 10. 14 The 95th percentile values of acid, weakly acidic, and nonacid HRE were 0, 0, and 2, respectively, in the study by Wang et al, 14 who were also the only authors assessing the 25th, 75th, and 95th percentiles of HRE and their pH compositions. Xiao et al 15 only provided the 75th percentile of HRE, which was found to be 1 event. In this study, 7 individuals (35%) had ≥1 HRE, while in the study by Wang et al, 14 there were 6 individuals (16.2%) with ≥1 HRE, with the majority of HREs being nonacidic. Hoppo et al 16 identified HRE in only 1 individual (3.1%). Hou et al 21 reported average and standard deviation of HRE in healthy controls, taking into account the pH composition of events. The average numbers of acid and nonacid HRE in healthy individuals were 0 ± 0 and 21 ± 7 (SD = 14-28), respectively. 21 In the study by Desjardin et al, 17 the mean values of HRE with pH <4 and with pH <5 were both 1.
Most HREs were gaseous 21 and occurred during daytime and in the upright position ( Table 1 ).14,18 In 1 study assessing mean nocturnal baseline impedance (MNBI), the pharyngeal baseline impedance was found to be higher among LPR patients compared to healthy controls. 23
Oropharyngeal reflux event (Restech)
The 95th percentiles of oropharyngeal events according to the pH thresholds measured on oropharyngeal pH monitoring are described in Table 2 . Overall, the 95th percentiles of oropharyngeal events at thresholds of pH <4, pH <5, and pH <6.0 ranged from 0 to 2.5, 0 to 107.5, and 40 to 128, respectively.12,18 The data were significantly different within studies depending on patient positions (upright vs supine).13,18,26 The mean percentage time with pH <4 was 0% in the study by Ayazi et al, 25 while it ranged from 0% to 16.7% with a threshold of pH <5.5. 24 Similar to studies using HEMII-pH or MII-pH, the presentation of results of studies using oropharyngeal pH monitoring varied significantly among studies.
Discussion
To date, there are no international consensus guidelines or gold standard for the diagnosis of LPR through objective assessments. 1 The HEMII-pH or MII-pH and oropharyngeal pH monitoring have been recognized as the more reliable approaches, as they provide objective data about the occurrence of reflux events in the upper aerodigestive tract of patients with LPR-associated symptoms or findings. 31 In this systematic review, we tried to analyze the current evidence regarding normative data of both HEMII-pH or MII-pH and oropharyngeal pH monitoring in order to propose agreeable thresholds. However, upon detailed review and analyses of the literature to date, we were unable to determine common thresholds for PRE or HRE across studies for several methodological reasons, chiefly the significant heterogeneity in inclusion criteria, definitions, and study protocol.
The definition and inclusion criteria of healthy individuals varied substantially among studies, an important source of heterogeneity. Some studies based their inclusion criteria on the presence or absence of typical esophageal symptoms of GERD,10-12,15,20,25 which are, in practice, often absent in patients presenting for the evaluation of LPR.1,32 In other words, some LPR patients may present with primarily laryngeal symptoms alone, with little to no esophageal GERD symptoms, and they may, consequently, be misclassified as healthy controls in studies that used esophageal symptoms as inclusion criteria. Moreover, in most studies, the exclusion of underlying major esophageal motility disorders was based on medical records or patient recall, which remains insufficient to conclusively exclude these disorders. 33 The inclusion of smokers and alcoholics in some healthy cohorts serves as another potential source of heterogeneity, as tobacco and alcohol may both impair the tonicity of esophageal sphincters, thereby increasing the risk of LPR. 34 Given that the use of these substances may also be an important and independent risk factor themselves for developing laryngeal symptoms, separate analyses may be needed for normative ambulatory reflux monitoring data between those with and without a history of tobacco or alcohol consumption. In most studies included in this systematic review, the mean age of the subjects enrolled was low (overall range of mean age: 23.9-46 years). Whether the normative values observed by these studies are generalizable to patients in other age groups remains unclear. Further studies inclusive of subjects from all age groups with appropriate subgroup analyses are needed to ensure applicability of the values generated.
The heterogeneity among studies in the number, placement, and specificity of the pH sensors and impedance electrodes also hindered standardized pooling of data across study cohorts. While HEMII-pH and oropharyngeal pH monitoring both aim to objectively quantify pharyngeal reflux events, information generated by these 2 modalities could not appropriately be pooled due to their differences in technique, equipment, location of sensors, and data used to define reflux events (impedance vs pH only). This was illustrated by Ummarino et al, 35 who performed oropharyngeal pH monitoring and HEMII-pH testing simultaneously on the same individuals and showed that fewer reflux episodes were identified by oropharyngeal pH monitoring. This may be due to the detection solely of change in pH with oropharyngeal pH monitoring, independent of true reflux events. Events that are weakly acidic or nonacidic and could only be identified with impedance technology and thus the specificity of oropharyngeal pH monitoring may be limited by the lack of simultaneous esophageal data to verify full-column reflux events. Indeed, several prior studies have shown poor correlation between findings on oropharyngeal pH monitoring and response to acid-suppressive therapies.36,37 The advantages/disadvantages, indications, and roles of HEMII-pH, MII-pH, or oropharyngeal pH monitoring in the evaluation for LPR need further evaluation and consensus guidance but are beyond the scope of this analysis.
The definitions of acid, weakly acid, or nonacid, as well as gas, liquid, or mixed reflux events, need further standardization for the diagnosis of LPR disease. Some consensus definitions have been developed for the evaluation of typical esophageal manifestations of GERD38,39 and were used in some included studies for LPR,10,11,14,16 although they are not universally employed in otolaryngology or specifically validated for the LPR population. Given the increasing evidence demonstrating the important role of weakly acidic or nonacid HRE in LPR,40-42 it would be crucial to ensure standardization in the criteria by which these events are classified to allow accurate comparisons across studies. A better understanding and more concrete classifications of acid vs nonacid reflux episodes may also carry important therapeutic implications, allowing more personalized treatment approaches, such as the initial choice of antisecretory agents (eg, proton pump inhibitors) vs antireflux barrier agents (eg, alginate). 41
Despite the differences and limitations in pooling the data across the included studies, an important measure that seemed increasingly required to diagnose LPR was reporting the number and pH of hypo- or oropharyngeal reflux episodes as a superior method to using proximal esophageal reflux episodes alone (which may not make it into the pharynx). Indeed, some studies found that PRE may be cleared very quickly in healthy subjects. 11 Moreover, the pH nature of the refluxate may change while migrating from the esophagus to the hypopharynx, 11 with the number of nonacid hypopharyngeal reflux episodes being more prevalent than acid events in LPR patients. 36 The buffering capacity of saliva may be indirectly highlighted by the higher number of HRE with pH >4 in healthy individuals, although this may also pose further diagnostic challenges and further refute the ability to truly diagnose reflux events when pH-only technologies are used. Based on our systematic review and analysis, the current article provides some recommendations on the inclusion/exclusion criteria and definitions for standardization of future studies ( Table 6 ). In particular, technical/methodological recommendations were focused on HEMII-pH, given the current lack of standardization and significant heterogeneity in employment of this technology. Standardization of methodologies is key in better understanding LPR. Reflux events measured by MII-pH in the hypopharynx of more than 1 episode (acidic, weakly acidic, or nonacidic) may be employed in defining disease. Alternatively, a combination of test results (distal esophageal pH, pepsin assay, MII-pH, oropharyngeal pH) may be employed to improve sensitivity and specificity in detecting LPR, but they all must stand the rigor of outcome studies. Studies showing higher prevalence of a test finding should be replaced by those showing favorable treatment response as a function of test results.
Proposition of Recommendations for Future Studies.

Abbreviations: HEMII-pH, hypopharyngeal-esophageal multichannel intraluminal impedance–pH monitoring; HRE, hypopharyngeal reflux episodes; LES, lower esophageal sphincter; PRE, proximal esophageal reflux episode; —, no information available.
To allow comparison with studies conducted in gastroenterology, our propositions of definitions were based on the consensus report of Sifrim et al. 38
Our study has several strengths, including the comprehensive review of the literature to date on healthy subjects using currently available ambulatory reflux monitoring technology to help establish normative guidelines. Reviews and recommendations were provided by a diverse, international group of clinicians and investigators with expertise in LPR. Included studies also represent a wide range of geographical locations and patient populations. However, this systematic review also has several limitations. First, the relatively low number of healthy individuals in all included studies may limit the findings and analyses. Second, many local and geographical factors may affect and confound the risk of gastroesophageal dysfunction and reflux, such as diet, genetic differences, and lifestyle variations. These factors, many of which remain insufficiently understood in LPR, may serve as another important source of heterogeneity across studies.
Conclusion
Ambulatory reflux monitoring remains a crucial and the most objective way to guide the diagnosis and management of LPR. The significant heterogeneity among studies to date with regards to inclusion criteria, definitions, system setup, and interpretation precludes the establishment of universal normative thresholds. Further large multicenter studies based on standardized testing protocols are needed to help determine appropriate reference ranges for clinical use.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211029831 – Supplemental material for Normative Ambulatory Reflux Monitoring Metrics for Laryngopharyngeal Reflux: A Systematic Review of 720 Healthy Individuals
Supplemental material, sj-docx-1-oto-10.1177_01945998211029831 for Normative Ambulatory Reflux Monitoring Metrics for Laryngopharyngeal Reflux: A Systematic Review of 720 Healthy Individuals by Jerome R. Lechien, Walter W. Chan, Lee M. Akst, Toshitaka Hoppo, Blair A. Jobe, Carlos M. Chiesa-Estomba, Vinciane Muls, Francois Bobin, Sven Saussez, Thomas L. Carroll, Michael F. Vaezi and Jonathan M. Bock in Otolaryngology–Head and Neck Surgery
Footnotes
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.