
Abstract
Objectives
(1) To compare perioperative outcomes and overall survival of patients with oropharyngeal salivary gland malignancies (OPSGMs) treated with transoral robotic surgery (TORS) versus other approaches. (2) To identify clinical factors associated with a robotic surgical approach.
Study Design
Retrospective analysis of the National Cancer Database (NCDB).
Setting
NCDB.
Methods
Data obtained from the NCDB were analyzed between 2010 and 2017 for patients with T1-T4a OPSGMs without distant metastases treated surgically. Patients were stratified by surgical approach (TORS vs nonrobotic), and clinicopathologic factors were compared with the t test or chi-square test for continuous or categorical variables, respectively. Overall survival was analyzed by patient demographics and clinical factors according to Kaplan-Meier and Cox proportional hazards models. Factors associated with TORS were assessed with logistic regression.
Results
A total of 785 patients were analyzed. A non–soft palate primary site (odds ratio, 12.9; 95% CI, 6.6-25.2) and treatment at an academic facility (odds ratio, 2.0; 95% CI, 1.2-3.5) were independently associated with TORS. There were no significant differences in the positive margin rate, 30-day mortality, or overall survival between the groups. The 30-day unplanned readmission rate was higher in patients treated with TORS versus nonrobotic resections (5.8% vs 1.7%, P = .0004). When stratified by tumor subsite, there was a significant decrease in hospital length of stay in patients with tongue base tumors undergoing TORS versus nonrobotic resections (P = .029).
Conclusion
This study suggests that TORS may be a viable treatment modality for appropriately selected patients with OPSGM.
The majority of oropharyngeal malignancies are p16+ squamous cell carcinomas, while a minority arise in the minor salivary glands of the oropharynx.1,2 The most common histologic types of minor oropharyngeal salivary gland malignancies (OPSGMs) are mucoepidermoid carcinoma, adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and adenocarcinoma.3,4 Together these OPSGMs represent a rare and heterogeneous group, with diverse histopathologic characteristics and clinical behavior.3,4 The current National Comprehensive Cancer Network guidelines recommend primary surgical treatment of salivary gland malignancies because they tend to be relatively resistant to radiotherapy as primary treatment. 5 The traditional surgical approach to the oropharynx is transoral, transmandibular, or transcervical pharyngotomy 6 ; however, the development of transoral robotic surgery (TORS) has expanded minimally invasive surgical access to the oropharynx. 7 Most literature on TORS is isolated to oropharyngeal squamous cell carcinoma (OPSCC), and data on patients with OPSGM undergoing TORS are promising but limited to small case series.8,9 Villanueva et al reported a locoregional control rate of 80% in 10 patients with OPSGM with T1 and T2 cancer undergoing TORS. 8 Similarly, in a multi-institutional review of 20 patients undergoing endoscopic transoral resection, Schoppy et al cited 90% disease-free survival. 9 Because OPSGMs appear to be at an increased risk of positive margins as compared with p16+ OPSCC due to their propensity for submucosal spread and perineural invasion in some histologic types (ie, adenoid cystic carcinoma), oncologic outcomes from OPSCC cannot necessarily be applied to OPSGM. 10
Therefore, the primary objective of this study was to describe the perioperative outcomes and survival of patients with OPSGM undergoing TORS as compared with other surgical approaches by using the National Cancer Database (NCDB). As a secondary objective, clinical factors associated with surgical approach were investigated as well.
Methods
To investigate this objective, we performed a retrospective review of all patients ≥18 years old with an OPSGM using the NCDB. Our study was deemed exempt from institutional review board review by Rutgers Robert Wood Johnson University Hospital. The NCDB is a registry maintained by the Commission on Cancer (American College of Surgeons) and the American Cancer Society, and it collects cases from >1500 facilities and encompasses approximately 70% of newly diagnosed cancers in the United States. There are established criteria to certify the quality of the submitted data, as well as an application process to obtain the data. After the distribution of the data, the Commission on Cancer and the American Cancer Society are not responsible for the analysis and conclusions presented.
We initially queried the NCDB for all patients ≥18 years old with an OPSGM treated between 2010 and 2017 using topographic and morphologic codes from the International Classification of Diseases for Oncology, Third Edition. Histologic codes included those for mucoepidermoid carcinoma (8430), adenoid cystic carcinoma (8200), polymorphous low-grade adenocarcinoma (8525), adenocarcinoma not otherwise specified (8140), and other rare types (8550, 8562, 8310, 8147, 8440, 8480, 8290, 8500, 8980, 8940). Topographic codes identified the base of tongue (C01.9, C02.4), tonsil/lateral pharyngeal wall (C09.0, C09.1, C09.8, C09.9, C10.2), soft palate (C05.1, C05.2), and other (posterior pharyngeal wall [C10.3], vallecula [C10.0], and overlapping lesion/not otherwise specified [C10.8, C10.9]). Patients with distant metastatic disease (M1) and T4b tumors were excluded.
Baseline patient characteristics included a comparison of age, sex, race, insurance status, Charlson-Deyo comorbidity class, facility type, year of treatment, tumor subsite, histologic type, grade, T stage, and N stage. The American Joint Committee on Cancer manual, seventh edition, was used for staging information. Additional treatment with a neck dissection, adjuvant radiation therapy, and adjuvant chemotherapy was also recorded.
Patients were then stratified into 2 groups based on the surgical approach used for the resection (TORS vs nonrobotic). The 2 groups were then compared with the t test for continuous variables and the chi-square test or Fisher exact test for categorical variables. Clinically relevant factors that were statistically significant or nearly statistically significant (P < .1) on univariable testing were then included in the initial multivariable logistic regression model. A backward elimination procedure was used to obtain a model containing only predictor variables whose coefficients were significant at the 0.05 level. Estimated odds ratios (ORs) and associated 95% CIs were calculated for each model. Survival functions for clinically relevant variables were estimated via the Kaplan-Meier method. Univariable and multivariable survival analyses were conducted per Cox proportional hazards models. Estimated hazard ratios (HRs) and associated 95% CIs were calculated for each model. Log-minus-log plots were used for testing the proportional hazards assumption. Because surgical approach was the main variable of interest, it was included in the multivariable model. Length of hospital stay was compared between groups with the Kaplan-Meier method. Subgroup analysis by tumor subsite was also performed, and unplanned 30-day readmissions and mortality were compared between groups. SPSS version 26 software (IBM) was used for data analysis.
Results
There were 785 patients who met inclusion criteria. The majority (n = 647, 82.4%) were treated with a nonrobotic approach. Their characteristics are summarized in Table 1 , stratified by the surgical approach. There were no statistically significant differences between the groups in age, sex, race, insurance status, comorbidity (Charlson-Deyo comorbidity class), histologic type, or receipt of adjuvant treatment.
Baseline Patient Characteristics by Surgical Approach. a
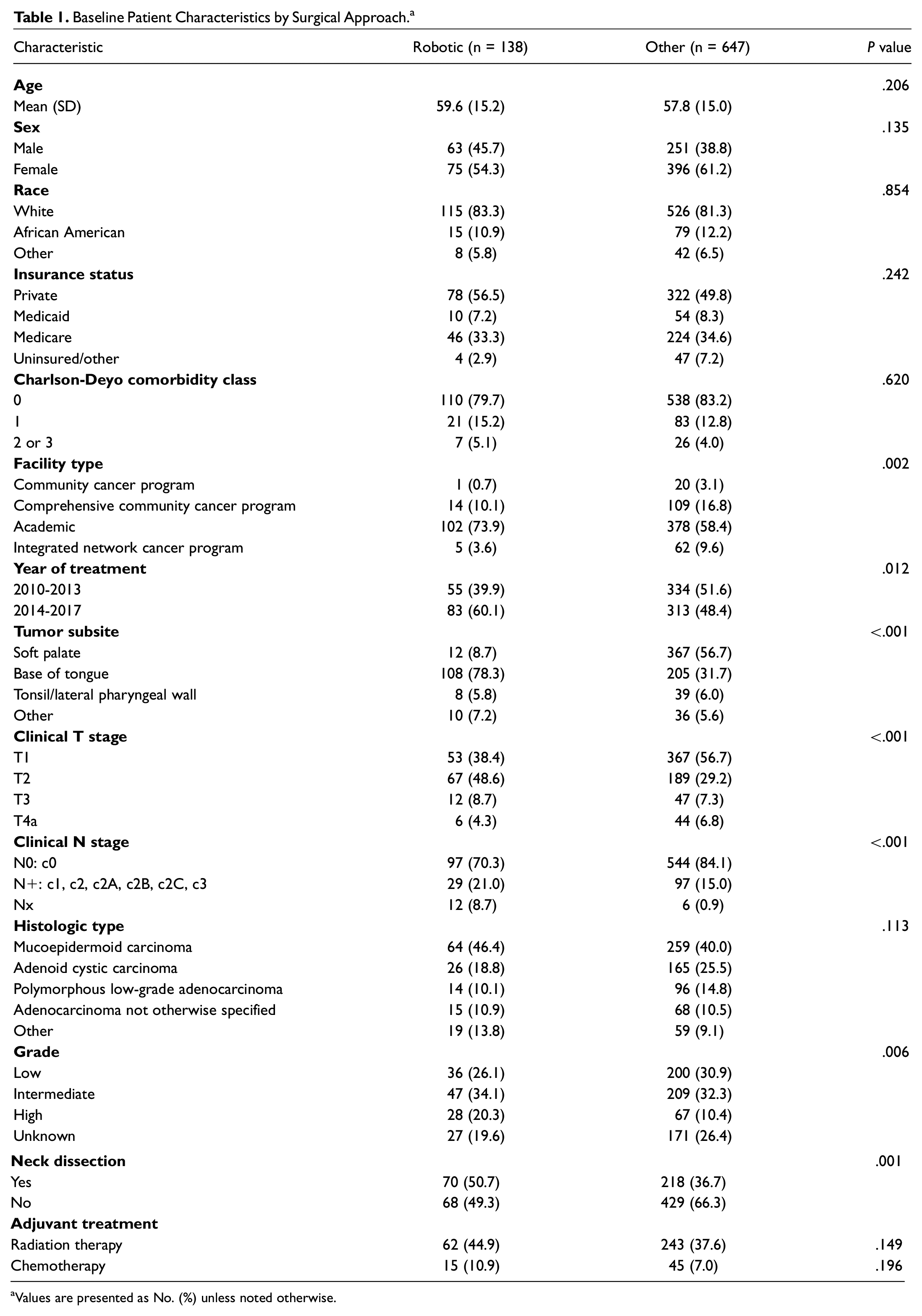
Values are presented as No. (%) unless noted otherwise.
On univariable analysis, multiple factors were associated with surgical approach. Facility type was associated with surgical approach (P < .002), with robotic resections more common at academic facilities. The use of TORS increased over the study period (P = .012). Tumor subsite was associated with surgical approach as well (P < .001). Soft palate tumors were more commonly resected via a nonrobotic approach (n = 367, 96.8%). Base of tongue tumors were the most common subsite undergoing TORS (n = 108, 78.3%), although a nonrobotic approach was used in the majority of base of tongue resections (n = 205, 65.5%). Clinical T stage was associated with surgical approach (P < .001), with TORS more typically used for T2 tumors and nonrobotic resections more often performed for T1 tumors. Nonrobotic resections were more likely to be stage cN0 than those removed robotically (84.1% vs 70.3%, P < .001). Correspondingly, patients undergoing TORS were more likely to have a neck dissection than patients undergoing a nonrobotic resection (50.7% vs 36.7%, P = .001). Finally, there were significant differences in tumor grade between the groups (P < .006).
On multivariable testing, tumor grade, stage, and year of treatment were no longer associated with surgical approach. The clinical variables independently associated with surgical approach are summarized in Table 2 . A non–soft palate primary site (OR, 12.9; 95% CI, 6.6-25.2) and treatment at an academic facility (OR, 2.0; 95% CI, 1.2-3.5) were both predictive of TORS.
Clinical Predictors of a Robotic Approach on Multivariable Analyses.
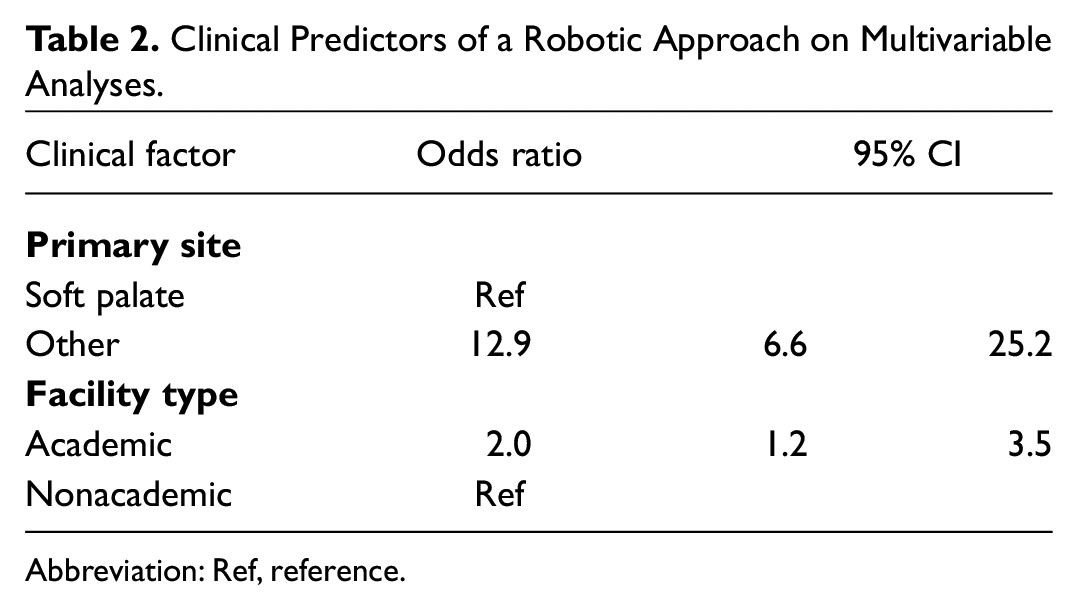
Abbreviation: Ref, reference.
Table 3 details the results of the univariable and multivariable survival analyses. The factors independently associated with OS on multivariable analysis were as follows: age (HR, 1.06; 95% CI, 1.04-1.08), high-grade tumor (reference, low grade; HR, 3.12; 95% CI, 1.66-5.86), stage T4a (reference, T1; HR, 2.59; 95% CI, 1.32-5.08), and stage N+ (reference, N0; HR, 2.33; 95% CI, 1.39-3.93). Notably, surgical approach was not associated with OS in either model.
Predictors of Overall Survival.
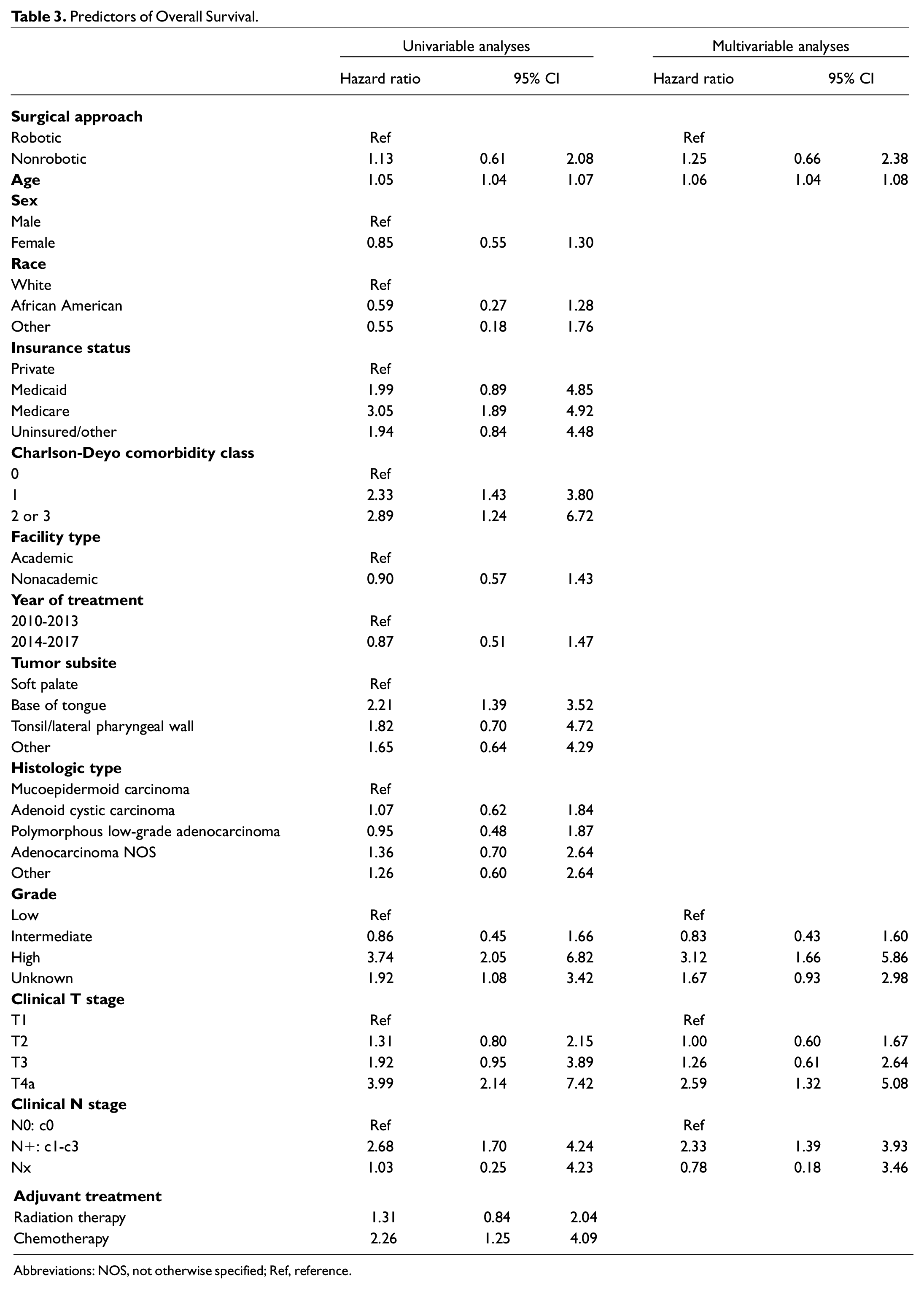
Abbreviations: NOS, not otherwise specified; Ref, reference.
Figure 1 illustrates the comparison of hospital length of stay between groups, stratified by tumor subsite. There was a significant decrease in hospital length of stay in patients with tongue base tumors undergoing TORS versus nonrobotic resections (P = .029); however, there was no difference in patients with tumors of other oropharyngeal subsites (P = .476). Table 4 compares the 30-day mortality, 30-day unplanned readmission rate, and surgical margin status between the groups. There was no significant difference in 30-day mortality between TORS and nonrobotic approaches (0.7% vs 0.2%, P = .305). However, TORS was associated with greater rates of unplanned 30-day readmissions as compared with nonrobotic resections (5.8% vs 1.7%, P = .004). Finally, the overall rate of positive margins was 21.0% (n = 165), which did not significantly differ between patients receiving TORS and other approaches (23.6% vs 20.4%, respectively; P = .358).
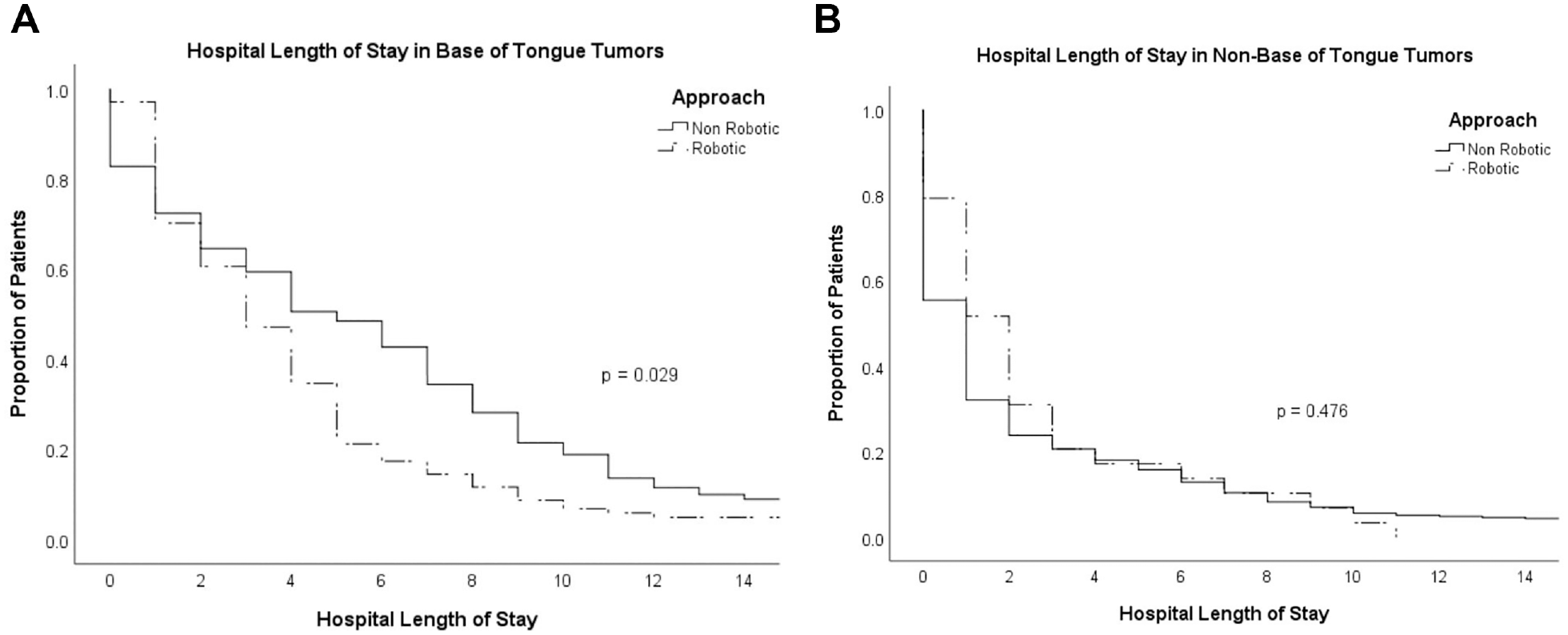
(A) Reduced length of hospital stay in patients with tongue base tumors undergoing TORS versus nonrobotic resections. (B) No significant difference in hospital length of stay among patients with tumors of other oropharyngeal subsites undergoing TORS versus nonrobotic resections. TORS, transoral robotic surgery.
Surgical Margin Status and 30-Day Unplanned Readmissions and Mortality by Surgical Approach. a
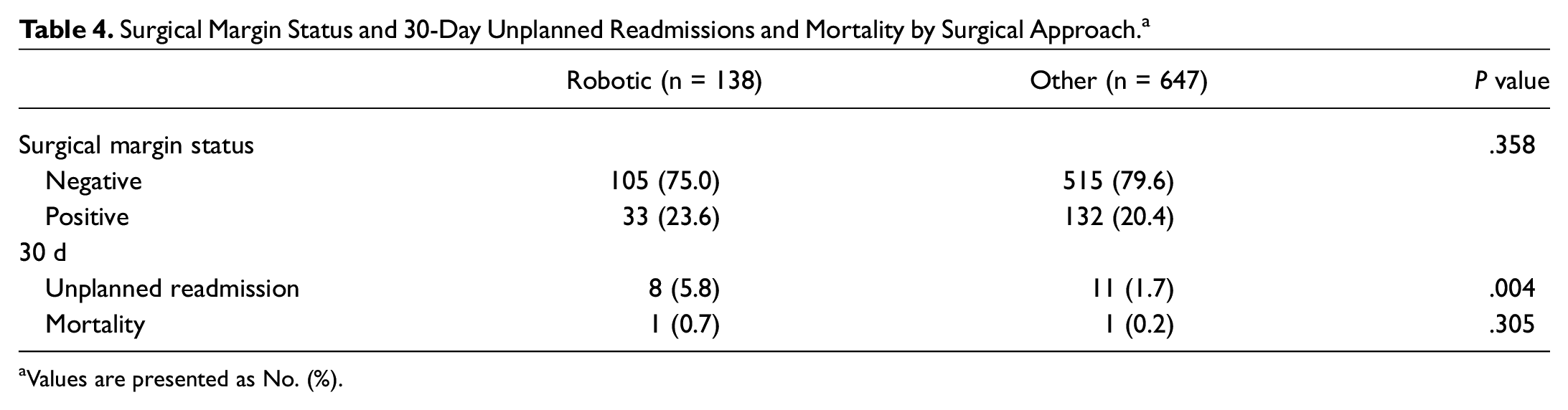
Values are presented as No. (%).
Discussion
In contrast to OPSCC, in which (chemo)radiation therapy and surgically based treatment generally offer comparable oncologic outcomes, surgical resection is recommended as the frontline therapy in salivary gland malignancies. 5 Surgical access to the oropharynx can be challenging, and traditional surgical approaches to the oropharynx include transoral, transmandibular, or transcervical pharyngotomy. 6 In one of the larger institutional reviews of patients with OPSGM (N = 67), the majority (61%) had a transmandibular approach, while transoral (33%) and transcervical (7%) procedures were less commonly utilized. 10 Notably, this study period occurred between 1985 and 2005, prior to the development of TORS, which gained US Food and Drug Administration approval for T1 and T2 tumors and has expanded minimally invasive access to the oropharynx. 7 Excellent outcomes in OPSCC have been also reported with transoral laser microsurgery, although widespread national use has not been adopted as with TORS.7,11,12 Nationally, the use of TORS in OPSCC has been increasing, and this study indicates increasing national utilization of TORS in OPSGM as well. 13
The distribution of affected oropharyngeal subsites in OPSGM differs from OPSCC. While OPSCC typically occurs in the palatine tonsils followed by the base of tongue, 13 OPSGMs usually develop in the soft palate or base of tongue. 14 TORS is particularly useful in patients with tumors of the tongue base, while those located in the soft palate are more amenable to direct transoral visualization without additional approaches. Accordingly, tumor location (non–soft palate) was independently associated with a robotic approach on multivariable analysis in our review. Additionally, treatment at an academic center was associated with the use of TORS. Similar findings were reported by Cracciolo et al in a NCDB review of surgically treated OPSCC. 11
Obtaining negative margins in this population is imperative to optimize oncologic outcomes. Multiple studies have demonstrated significantly worse outcomes in patients with positive margins.4,10,15-17 OPSGMs appear to be at an increased risk of positive margins, due to their propensity for submucosal spread and perineural invasion in some histologic types (ie, adenoid cystic carcinoma). 10 Iyer et al reported a positive margin rate of 46% in their series of 67 patients. 10 In surgically treated OPSCC, TORS has been associated with a reduced risk of positive margins as compared with open approaches in the primary and recurrent setting.13,18 Although there is limited information on TORS for OPSGM, results from small case series appear promising.8,9 Schoppy et al cited a positive margin rate of 5% in a series of 20 patients undergoing transoral endoscopic resection (18 TORS, 2 transoral laser microsurgery). 9 Similarly, Villaneuva noted a 100% negative margin rate in 10 patients with T1/2 OPSGM undergoing TORS. 8 In our study, however, the overall positive margin rate was 21.0%, but this did not significantly differ by surgical approach. 8
In terms of long-term outcomes, overall survival did not differ by surgical approach in our study. In a 2020 NCDB study, slightly higher 5-year OS was reported in patients with OPSCC undergoing TORS versus other approaches. 13 In our cohort, previously identified clinical factors, such as tumors with high-grade pathology, T4 stage, and clinically positive lymph nodes, adversely affected OS as well. Schoppy et al cited 90% OS at 36 months, and 80% locoregional control was achieved in the series by Villaneuva et al.8,9 With a median follow-up of 86 months in their 67 patients with OPSGM, Iver et al indicated a 5-year OS of 80%. 10 Clinical stage, anatomic subsite, and margin status were predictive of OS. 10 Locoregional recurrence occurred in 18% of patients, which was associated with T stage and margin status. 10 In 2018 Goel et al performed a review of 1426 OPSGMs using the SEER database (Surveillance, Epidemiology, and End Results). 14 They found 5- and 10-year disease-specific survival rates of 75% and 62%, respectively. 14 Independent prognosticators were grade, tumor stage, nodal status, and age. 14 Information on margin status and surgical approach was not available. 14 Distant recurrence appears to be the most common pattern for disease failure in patients with minor salivary gland malignancies, particularly those with adenoid cystic carcinoma.4,10 Hay et al stated that distal failure occurred in 49% of patients with adenoid cystic carcinoma of the minor salivary glands. 4
The functional outcomes of transoral surgery in the treatment of oropharyngeal malignancies are well described in the literature for OPSCC and can likely be transferable to this population.18-26 Given the national treatment trends for OPSCC since the advent of TORS, most studies have either described functional outcomes of patients undergoing TORS ± adjuvant therapy or compared TORS with radiation therapy–based treatment.20-26 Direct comparative data are limited on TORS versus open approaches in the primary setting.18,19 In a small nonrandomized prospective series, Lee et al compared outcomes between 27 patients with T1-T3 tonsil cancer undergoing TORS and 14 patients undergoing a mandibulotomy. 19 Although potential confounding variables may influence surgical approach, the authors reported lower rates of positive margins, a shorter hospital stay, more rapid swallowing recovery, and a shorter operative time in the TORS group. 19 Similarly, White et al compared functional and oncologic outcomes in 128 patients with recurrent OPSCC who were matched by tumor stage and underwent TORS or traditional approaches. 18 The TORS group had a shorter hospital stay, a lower rate of gastric feeding tube and tracheostomy placement, as well as reduced blood loss and operative time as compared with the cohort undergoing traditional approaches. 18 Information on most of these outcomes cannot be assessed via the NCDB, with the exception of hospital length of stay. This variable was analyzed by subgroups according to tumor site, and TORS was associated with a shorter duration of hospital stay in the subset of patients with tongue base tumors while there was no difference in patients with tumors involving other oropharyngeal subsites. It is likely that these results can be explained by the avoidance of the traditional approaches, which are associated with greater morbidity as compared with TORS.
A primary concern with TORS is the potential risk of postoperative hemorrhage. Rates in the literature have been variable, although a recent meta-analysis reported a median rate of 6.5%. 27 Life-threatening bleeding occurs less often, and prophylactic arterial ligation has been recommended to further reduce this risk. 28 This, with greater rates of intermediate- and high-grade tumors, may help explain the significantly higher rates of neck dissections performed in the TORS group. Postoperative bleeding, dehydration, and pain have been cited as the most common causes of unplanned readmissions after TORS.29,30 In our study, unplanned 30-day readmissions were more common in the TORS cohort, although our rate of 5.8% is lower than comparable studies based on institutional data 29 (7.7%) or the Nationwide Readmissions Database 30 (12.3%). Importantly, it is not possible to discern the reason for postoperative readmission in the NCDB. In addition, this may be underestimated in the NCDB due to inadequately capturing patients readmitted at other institutions.
In summary, the surgical management of OPSGMs can be challenging because of their location and propensity for submucosal spread. Given their relative resistance to radiation therapy, the primary question regarding management is which surgical approach to choose. While soft palate tumors may be favorable for a direct transoral excision, base of tongue involvement likely requires additional exposure for adequate visualization. Although retrospective and subject to limitations, this national review suggests that TORS is at least not inferior to open approaches from an oncologic view in appropriately selected patients. Additionally, TORS offers functional advantages over other approaches, which are comprehensively discussed elsewhere in the literature. In this series it demonstrated a shorter length of hospital stay in patients with tongue base tumors.18-26 The primary disadvantage may be a higher rate of unplanned hospital readmissions, likely attributed to postoperative hemorrhage or dehydration. This study involving the NCDB allows an analysis of surgical approach to these uncommon malignancies, which would otherwise be obtainable from only a large multi-institutional study.
Our study has a number of limitations. Although the NCDB offers several benefits over other databases, coding errors, selection bias, and incomplete/missing data limit its use, as with all database studies. Additionally, the NCDB provides information only on overall survival and does not contain information regarding disease recurrence, previous treatment, and cause of death, all of which would be useful information in this patient cohort. Finally, the potential functional benefits may be the most significant advantage of TORS versus traditional approaches, yet that information is not available in the NCDB.
Conclusion
This study suggests that TORS may be a viable treatment modality for appropriately selected patients with OPSGMs, with similar rates of positive margins and overall survival as compared with other surgical approaches.
Footnotes
This article has been accepted for presentation at the American Head and Neck Society Meeting; July 22-25, 2021; Chicago, Illinois.