
Abstract
Objective
The objective of this quality initiative project was to modify our existing institutional drug-induced sleep endoscopy (DISE) protocol so that the surgeon could consistently determine obstructive breathing patterns while minimizing children’s discomfort.
Methods
A quality initiative study utilizing the well-described plan-do-study-act (PDSA) process was conducted at a tertiary hospital for children with polysomnogram-documented obstructive sleep apnea who were undergoing DISE. A 4-point Likert measurement tool was created. Change in each Likert rating with subsequent PDSA cycle was tested with the Wilcoxon rank sum test (Mann-Whitney), and change across all PDSA cycles was tested with the Kruskal-Wallis equality-of-populations rank test.
Results
After a series of 4 PDSA cycles with 81 children, the DISE protocol was streamlined from 14 to 9 steps. There was significant improvement for all aspects of the DISE, with a final overall median rating of 1 (excellent) for intravenous (IV) placement, scope insertion, and anesthesiologist and surgeon satisfaction (P < .01)
Discussion
For sleep surgeons, DISE is quickly becoming what bronchoscopy is to the airway surgeon. Utilizing inhalational agents to obtain IV access and insert the flexible scope in the rapid “on-off” fashion optimizes DISE success regardless of the primary sedation medication and allows ample time for these agents to dissipate.
Implications for Practice
Adoption of a DISE protocol that includes nasal premedication and inhalational volatile gases for IV and scope insertion at the onset provides a more predictable level of sedation that is well tolerated by the patient, enabling the otolaryngologist to create an obstructive sleep apnea treatment plan.
Drug-induced sleep endoscopy (DISE) is increasingly utilized by pediatric otolaryngologists to determine the anatomic site of obstruction for children with polysomnogram (PSG)–confirmed obstructive sleep apnea (OSA). This is especially true for children with persistent OSA following a tonsillectomy with or without adenoidectomy (T&A). Since the success of T&A is variable, DISE has increased in popularity as a diagnostic and planning tool. In a meta-analysis of 1079 patients, Durr et al found that at least one-third of children experienced persistent OSA following a T&A. 1 The cure rate is even lower for children with Down syndrome. 2 DISE-directed surgery has efficacious outcomes.3-8 In a 2016 multi-institutional survey on pediatric DISE practice patterns, there was a low rate of agreement among otolaryngologists on how to perform DISE (33%). 9 Although many institutions have a standard DISE protocol, none has been widely accepted. 9 The wide variability of DISE protocols potentially compromises DISE findings, interpretation, and generalizability of investigations. In the 2021 expert consensus statement on pediatric DISE, the panel acknowledged an opportunity for quality improvement (QI) regarding the sedation for pediatric DISE since there is significant practice variation in this area. 10
A variety of medications are utilized for DISE depending on the institution. 9 The medications administered for the pharmacologic induction of sleep in DISE include dexmedetomidine,11,12 propofol,13-17 midazolam,18-20 and ketamine. 21 Each agent has benefits and downsides—no perfect pharmacologic agent exists. In addition, no perfect metric of a child’s level of sedation exists (eg, bispectral index [BIS] or other devices). The most common DISE agents are dexmedetomidine, a selective α2 adrenergic agonist, and propofol, which interacts with the GABA receptors (gamma-aminobutyric acid). Propofol and dexmedetomidine have been identified as the optimal sedation agents.9,10 In contrast to propofol, dexmedetomidine’s clinical effect closely resembles natural non-REM sleep, without significant respiratory depression.22,23 In addition, increasing doses of dexmedetomidine is not associated with the clinical signs of drug-induced airway hypotonia that are observed with propofol. 24 When compared with propofol, dexmedetomidine required less artificial airway support during cine magnetic resonance imaging sleep studies in children with OSA.25-27 Another common agent is ketamine, which is sedating and dissociative and does not depress respiration. Unfortunately, it may increase upper airway muscle tone, which subsequently may alter the natural obstructive breathing pattern. 28 In combination with dexmedetomidine, ketamine was associated with fewer oxygen desaturations, a higher rate of successful DISE completion, and better maintenance of blood pressure as compared with propofol alone or propofol + sevoflurane. 21 The ideal pharmacologic agent for DISE should have negligible effects on upper airway muscle tone and sleep architecture, be easy to titrate, and have minimal side effects.
The anesthetic and surgical goal of DISE is to choose a combination and sequence of pharmacologic agents that simulate natural sleep, are well tolerated by the child, and allow accurate identification of the obstructive breathing pattern for development of a surgical plan. When a standard DISE protocol was created at Children’s Hospital Colorado, the guiding principle was to select medications that had the least effect on airway tone and respiratory pattern. The rationale was that by limiting the pharmacologic agents administered, our DISE findings would be more accurate. Dexmedetomidine was chosen as the primary sedation agent since it simulates non-REM sleep without producing respiratory depression and has minimal effects on upper airway tone or cross-sectional area.23,29 Systematic reviews also report dexmedetomidine to have the most favorable sedation properties for DISE.30,31 Nitrous oxide, rather than sevoflurane, was selected as the initial inhalational sedation agent of choice since it has minimal effects on airway tone.29,32 Despite the adoption of a standard protocol, DISE outcomes were unpredictable. Through a series of plan-do-study-act (PDSA) cycles, the aim of this project was to modify our existing institutional DISE protocol so that the surgeon could reliably determine the obstructive breathing pattern for children with PSG-proven OSA while minimizing patient discomfort and optimizing the anesthetic.
Methods
A multidisciplinary team (MDT) comprised an operating room registered nurse (ORRN), pediatric anesthesiologist, and pediatric otolaryngologist and was created to assess the DISE protocol at Colorado Children’s Hospital. SQUIRE guidelines were followed (Standards for Quality Improvement Reporting Excellence). Approval was obtained by the Colorado Multiple Institutional Review Board (protocol 20-1163). Although the hospital had a DISE protocol, it was established by institutional consensus due to a lack of high-quality evidence. The MDT unanimously agreed that there were multiple QI opportunities: patient tolerance of the most stimulating portions of the DISE procedure, protocol compliance, adequate depth of sedation, and anesthesiologist and surgeon satisfaction
Measures
A series of PDSA cycles were performed to achieve our objective. In brief, PDSA cycles are an iterative process where a small change is made in the current workflow and the results are analyzed. Subsequent interventions are planned, designed, studied, and acted on until the process has been optimized and the QI objective achieved. 33
At our institution, it is standard to perform PSG prior to DISE. DISE is performed on those children who have at least moderate OSA (obstructive apnea-hypopnea index [OAHI] ≥5 events/h) or marked increased work of breathing by video. The preoperative PSG informs anesthesia of the child’s asleep gas exchange and the OAHI, and the video description of the child’s obstructive breathing pattern helps the surgeon determine when the proper depth of sedation has been achieved. Our protocol prior to undertaking this QI project is viewable as Supplemental Figure S1 (available online).
Aspects of the DISE protocol that were felt to be QI opportunities were premedication with intranasal dexmedetomidine, use of inhalational anesthetic agents, timing of intravenous (IV) placement, and scope insertion with respect to the administration of anesthetic medications. Elements of the protocol that remained constant were SpO2 monitoring following premedication, operating room (OR) environment being dark and quiet, body positioning, and avoidance of topical decongestants or topical anesthetics. Of note, once the intranasal dexmedetomidine dose had been administered in the preoperative holding area, a continuous pulse oxygen monitor was placed on the child and monitored by the preoperative nursing staff.
Since there is no validated measurement tool to assess DISE, the MDT created one to collect qualitative and quantitative data for the PDSA cycles. The outcome measures assessed were the following: sedation level upon entry into the OR, patient’s tolerance of IV placement and scope insertion, and DISE success from both the anesthesiologist’s perspective and the surgeon’s. A 4-point Likert scale was created for each variable ( Table 1 ). The Likert scale emphasized not only efficiency but also patient comfort and whether the child’s sedation level enabled the surgeon to create a management plan. The Likert rating was assigned by the ORRN, who was responsible for the data collection during the DISE procedure. On the rare occasion that the ORRN was unsure of the Likert rating, she would ask the surgeon or anesthesiologist for input. As the DISE protocol evolved during the PDSA cycles, the measurement tool was adjusted to reflect changes in each PDSA cycle’s protocol. From the surgeon’s perspective, the DISE was rated as poor if the surgeon felt that the obstructive breathing pattern during the procedure was inconsistent with the PSG findings regardless of how well the child’s sedation went—at our institution, part of the PSG report includes video characteristics of the child’s sleep and provides the basis for comparison of PSG findings with the intraoperative DISE findings. The MDT agreed that the series of PDSA cycles would continue until (1) it established an effective protocol that was well tolerated by the patient and (2) the anesthesiologist rated the case as good or excellent. Effective is defined as enabling the surgeon to create an OSA management plan. After each PDSA cycle, the MDT met, analyzed the Likert scores, and initiated rescue steps to create the next PDSA cycle. In summary, protocol modifications included adjustments in medication selection, dose administration, and the timing of when specific actions would occur.
Likert Ratings of Components of DISE Procedure by Plan-Do-Study-Act Cycle.
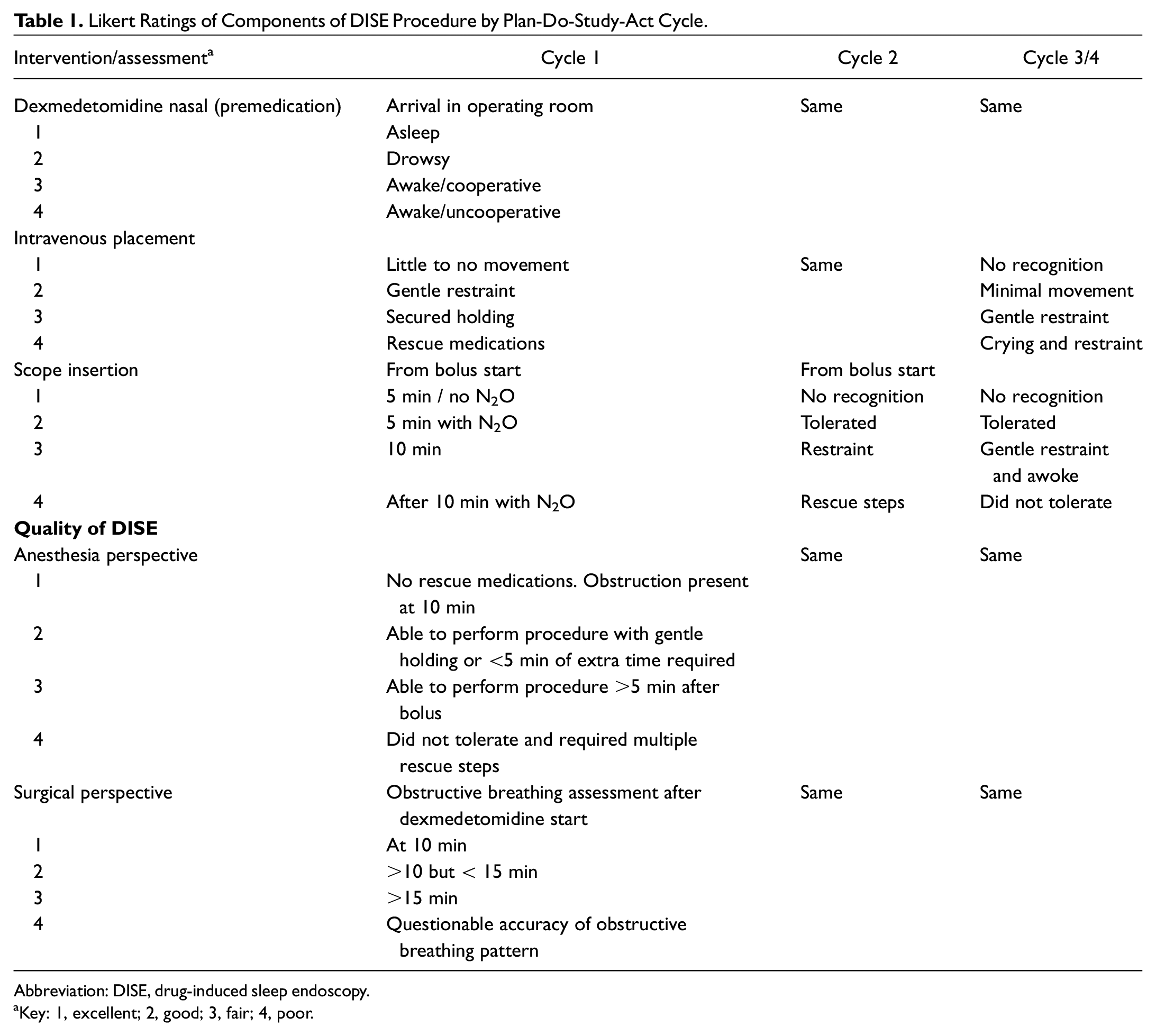
Abbreviation: DISE, drug-induced sleep endoscopy.
Key: 1, excellent; 2, good; 3, fair; 4, poor.
Intervention/Study of Intervention
The objective of the first PDSA cycle (PDSA-1) was to determine the efficacy of our existing protocol, which attempted to minimize the use of inhalational anesthetics and rely on dexmedetomidine alone to simulate sleep. Our primary concern with inhalational anesthetic agents was evidence that they may alter the obstructive breathing pattern that one would observe during natural sleep. 34 Topical EMLA cream was applied to facilitate IV placement per the discretion of the pediatric anesthesiologist. Given that some children would not tolerate IV placement with a dexmedetomidine nasal premedication alone, nitrous oxide followed by sevoflurane was the rescue medication and utilized on an as-needed basis.
For the second PDSA cycle (PDSA-2), the objective was to improve protocol compliance with topical EMLA for IV placement in an attempt to continue avoiding the administration of sevoflurane. Administration of nitrous oxide 1 minute prior to scope insertion was also adopted as standard and no longer used as a rescue technique. We hypothesized that these protocol modifications during the most stimulating aspects of DISE may improve the global scores.
Due to Likert scores >2, PDSA-3 was designed to assess whether using a short-acting inhalational anesthetic proactively, rather than as a rescue option, would improve outcomes. Topical EMLA cream was removed from the protocol since inhalational agents would be used to render brief general anesthesia. To improve patient tolerance of scope insertion, the scope was inserted into the nasopharynx within seconds of securing the IV line while the child was still anesthetized by the inhalational agents. This method became known as the “sevo on-off” technique, utilizing a quick inhaled induction (“sevo on”) with IV placement and nasal scope placement, followed immediately by turning sevoflurane off (“sevo off”) and relying on minute ventilation by the patient to exhale the anesthetic so that it would have minimal effect on the upper airway tone.
The final PDSA cycle (PDSA-4) was to confirm that the success of PDSA-3 was sustainable. The MDT discussed whether a dexmedetomidine premedication was necessary now that inhalational agents were being utilized for the invasive aspects of DISE, and the decision was to maintain it for PDSA-4. We unanimously felt that the dexmedetomidine premedication would provide the primary benefit of a loading dose. We also recognized the additional benefit of administration of a premedication for these patients, as many had preexisting procedural anxiety and/or special needs that would necessitate it for comfort and anxiolysis.
Analysis
For data analysis, only the Likert ratings for the initial method to obtain IV access or insert the scope were utilized. Likert ratings for rescue steps in the algorithm were utilized solely to plan the next PDSA cycle. For analysis purposes, PDSA-3 and PDSA-4 were combined since no protocol changes were implemented, and they are subsequently referred to as PDSA-3/4. Intranasal dexmedetomidine premedication doses were tested for differences in rating with the Kruskal-Wallis equality-of-populations rank test. Change in each Likert rating with subsequent PDSA cycle was tested with the Wilcoxon rank-sum test (Mann-Whitney), and change across all PDSA cycles was tested with the Kruskal-Wallis equality-of-populations rank test. All analyses were performed with Stata/SE 15.1 (StataCorp). All statistical tests were 2-sided, and a significance level of 0.05 was used for all analyses.
Results
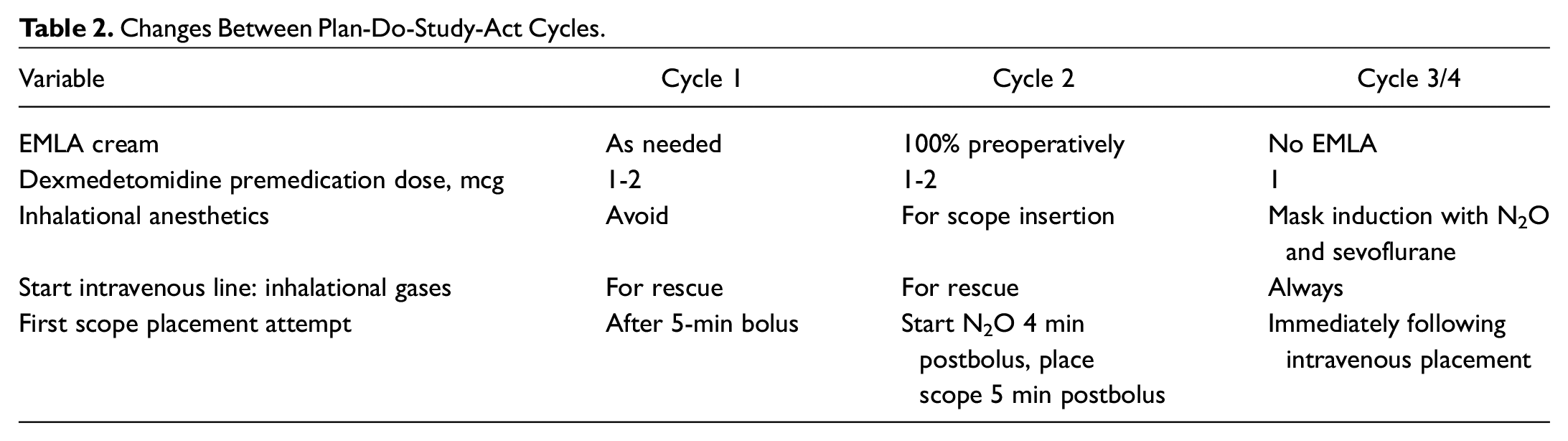
PDSA cycles 1, 2, and 3/4 had 12, 20, and 49 patients, respectively. Table 2 highlights the changes for each cycle. Figure 1 summarizes the results for the main outcome measures for each PDSA cycle.
Changes Between Plan-Do-Study-Act Cycles.
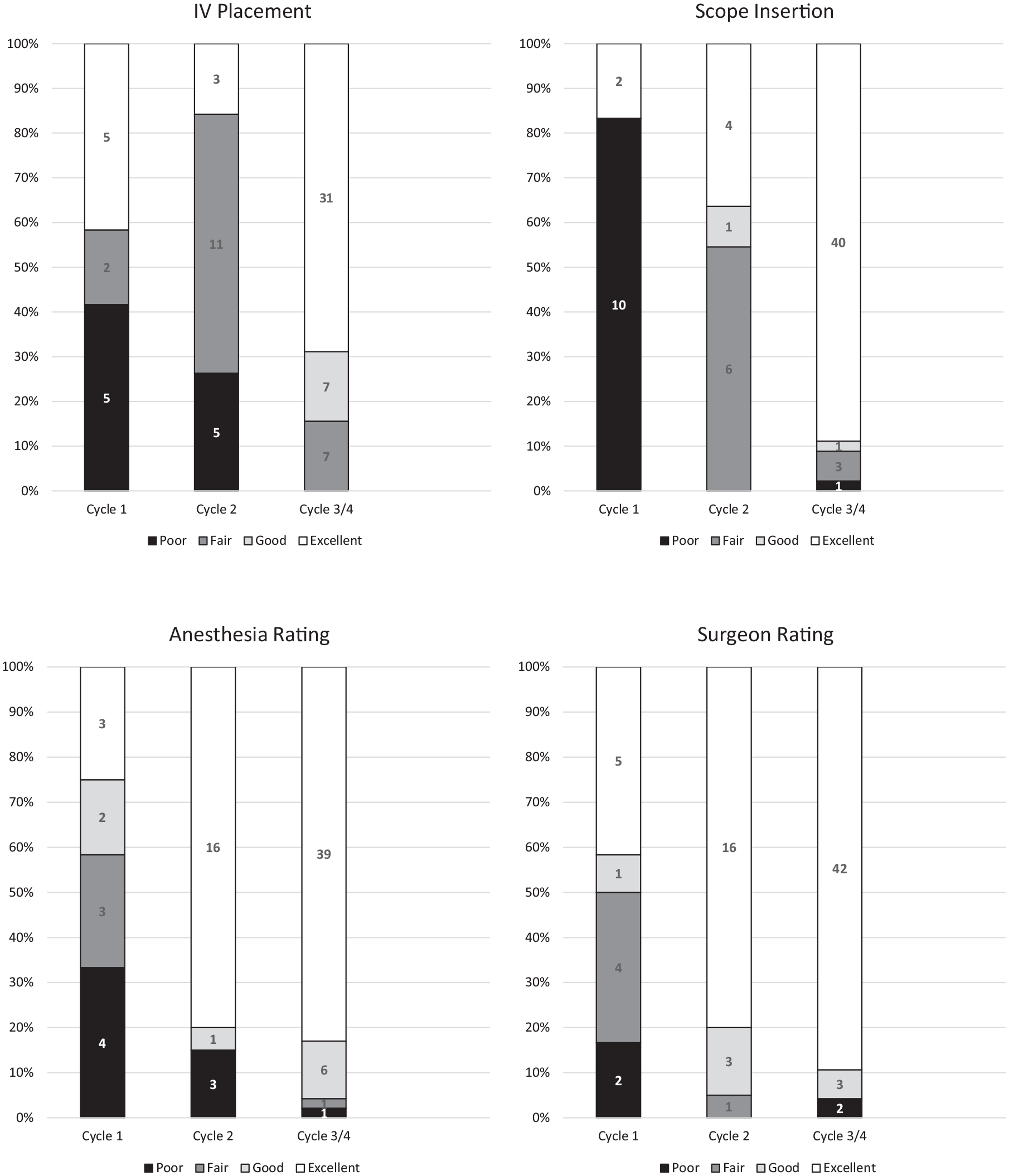
Likert rating distribution by plan-do-study-act cycle for (A-D) IV placement, scope insertion, anesthesia rating, and surgeon rating. IV, intravenous.
For PDSA-1, 3 dosages of preoperative intranasal dexmedetomidine were administered due to anesthesia provider discretion based on clinical judgment and patient comorbidities. There was no significant difference (P > .05) in the level of sedation for the different doses. Five children had topical EMLA cream applied preoperatively, and 4 of these patients tolerated insertion of the IV line without any inhalation agents. Of 12 children, only 2 (16%) tolerated scope insertion without nitrous oxide at 5 minutes. Given that topical EMLA cream improved outcomes for IV insertion and few children tolerated insertion of the scope without inhalational agents, the protocol was modified so that it was standard to apply topical EMLA cream and that nitrous oxide would always be administered 1 minute prior to scope insertion.
For PDSA-2, the recommended 2-mcg/kg intranasal dexmedetomidine premedication was administered to 12 of 20 children. Children received the lower dose at the discretion of the anesthesiologist. The overall ranking for this cycle was 3.0. Of note, 12 of 20 children required sevoflurane rescue to insert the IV line, and the surgeon inserted the scope for 8 of these children while they were still under the effect of sevoflurane. For the 12 children who did not have the scope inserted with the placement of the IV line, all of them tolerated scope placement with nitrous oxide. The median Likert ranking was 3 (interquartile range [IQR], 3-4) for IV insertion and 3 (IQR, 1-3) for scope insertion ( Table 3 ). Despite poor patient tolerance to the procedure, the surgeon and anesthesiologist were satisfied, with a median Likert ranking of 1 (IQR, 1-1).
Change in Likert Rating by Plan-Do-Study-Act Cycle. a
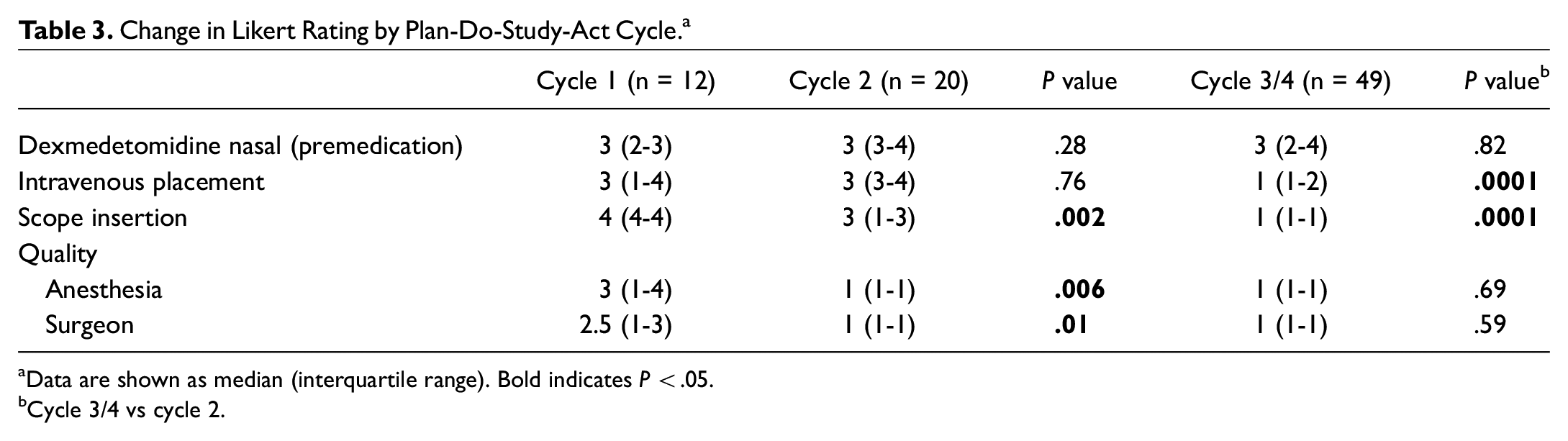
Data are shown as median (interquartile range). Bold indicates P < .05.
Cycle 3/4 vs cycle 2.
Following PDSA-2, the MDT agreed that the DISE protocol was neither reliable nor efficient due to the fair ranking (median, 3) for IV placement and scope insertion, which represents how the child has tolerated the procedure. Of the 20 children, 12 (60%) received the highest dexmedetomidine premedication dose, but several pediatric anesthesiologists raised concerns about the higher dose for children with Down syndrome due to bradycardia/arrhythmia risks. Subsequently, the standard dexmedetomidine premedication dose was decreased to 1 mcg/kg. Since 60% of the children required sevoflurane during PDSA-2 as a rescue technique, the protocol was modified to proactively administer volatile gases at the beginning of DISE in the rapid on-off method described previously. The rationale was that patient tolerance would improve and that, by the time the dexmedetomidine bolus was complete, there would be minimal residual effects from the brief administration of volatile gas. Sevoflurane is an inhaled anesthetic agent with very low solubility whose effect wears off quickly. A spontaneously breathing patient will have a normal or high-normal minute ventilation, thereby exhaling the sevoflurane in a matter of minutes. 34 Additionally, the MDT recognized that the creation of a linear protocol without rescue strategies would increase protocol adherence and therefore overall success.
For PDSA-3/4, compliance with the dexmedetomidine premedication dose of 1 mcg/kg was 88%. Patient tolerance for IV and scope placement improved dramatically with a median rating of 1 (IQR, 1-2) for both steps ( Table 3 ). The anesthesiologists and otolaryngologists also rated the overall DISE as 1 (IQR, 1-1). Propofol was not necessary for any child.
A separate analysis of the dexmedetomidine premedication dose for all PDSA cycles combined did not demonstrate a significant difference for a 2- versus 1-mcg/kg dose in a child’s level of drowsiness upon arriving in the OR (P = .15). Table 4 details the complications.
Complications and Prevalence by Plan-Do-Study-Act Cycle. a
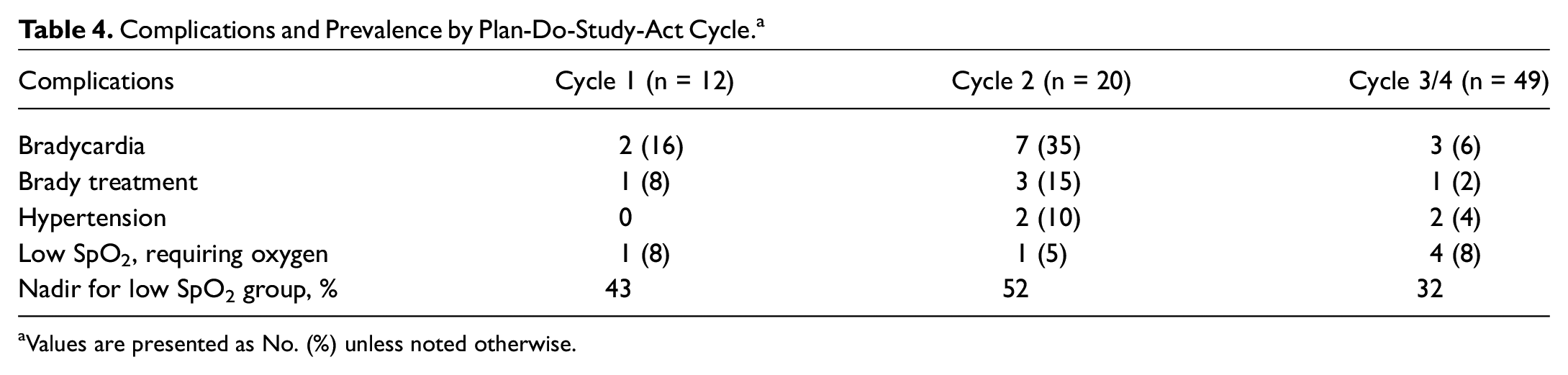
Values are presented as No. (%) unless noted otherwise.
Discussion
For sleep surgeons, DISE is quickly becoming what bronchoscopy is to the airway surgeon. DISE is a diagnostic tool to identify the anatomic sites of obstruction for children with OSA, enabling surgeons to formulate a management plan. By recognizing the unpredictable anesthetic plans and outcomes of DISE at our institution, a QI process was initiated to develop an effective, reliable, and reproducible protocol that is well tolerated by the patient and satisfactory to the anesthesiologist and surgeon. The initial objective of this QI process was to determine if dexmedetomidine alone was effective in simulating sleep and provided enough sedation for DISE to be tolerated by the child while identifying the obstructive breathing pattern. Our goal was to minimize any agents that might affect upper airway tone and alter the obstructive breathing pattern that occurs during natural unmedicated sleep. Unfortunately, our dexmedetomidine-only approach was poorly tolerated by the patient.
The major lessons learned from this project was simplifying the protocol by eliminating contingency steps and adopting a rapid on-off induction of general anesthesia for improved patient tolerance. By proactively utilizing inhalational agents at the beginning of the procedure, all aspects of DISE were rated as excellent. We feel that by delaying the DISE assessment until the 10-minute dexmedetomidine bolus is complete, we minimized the cofounding variable of inhalational gases being included as part of the protocol.
Since many patients in the early PDSA cycles required activation of the rescue pathways, the anesthesiologist’s and surgeon’s satisfaction did not reflect the challenges that it took to arrive at the final assessment stage. The MDT anticipates that if anesthesiologists today were to use the protocol from PDSA-2, the satisfaction scores would be much lower. The improved ranking from PDSA-1 to PDSA-2 reflects an interval change for individuals who did not know that there would be better options until they observed those in later cycles. After PDSA-2, the MDT recognized that proactively administering inhalational anesthesia was necessary for IV placement and insertion of the flexible scope—these are the 2 most stimulating steps of the DISE procedure. Utilizing sevoflurane in a rapid on-off fashion allows the patient to tolerate the worst parts of the procedure while minimizing the physiologic effects of sevoflurane. Now that a streamlined, highly standardized DISE protocol exists for this challenging patient population, our definition of success has also risen. The initial protocol included 14 steps and multiple rescue options, and by PDSA-3, the protocol was reduced to 9 linear steps with just 1 rescue option. Administration of low-dose propofol following the dexmedetomidine bolus is employed only if the child has not demonstrated an obstructive breathing pattern. Figure 2 depicts the final protocol that we utilize at our institution for the DISE procedure.
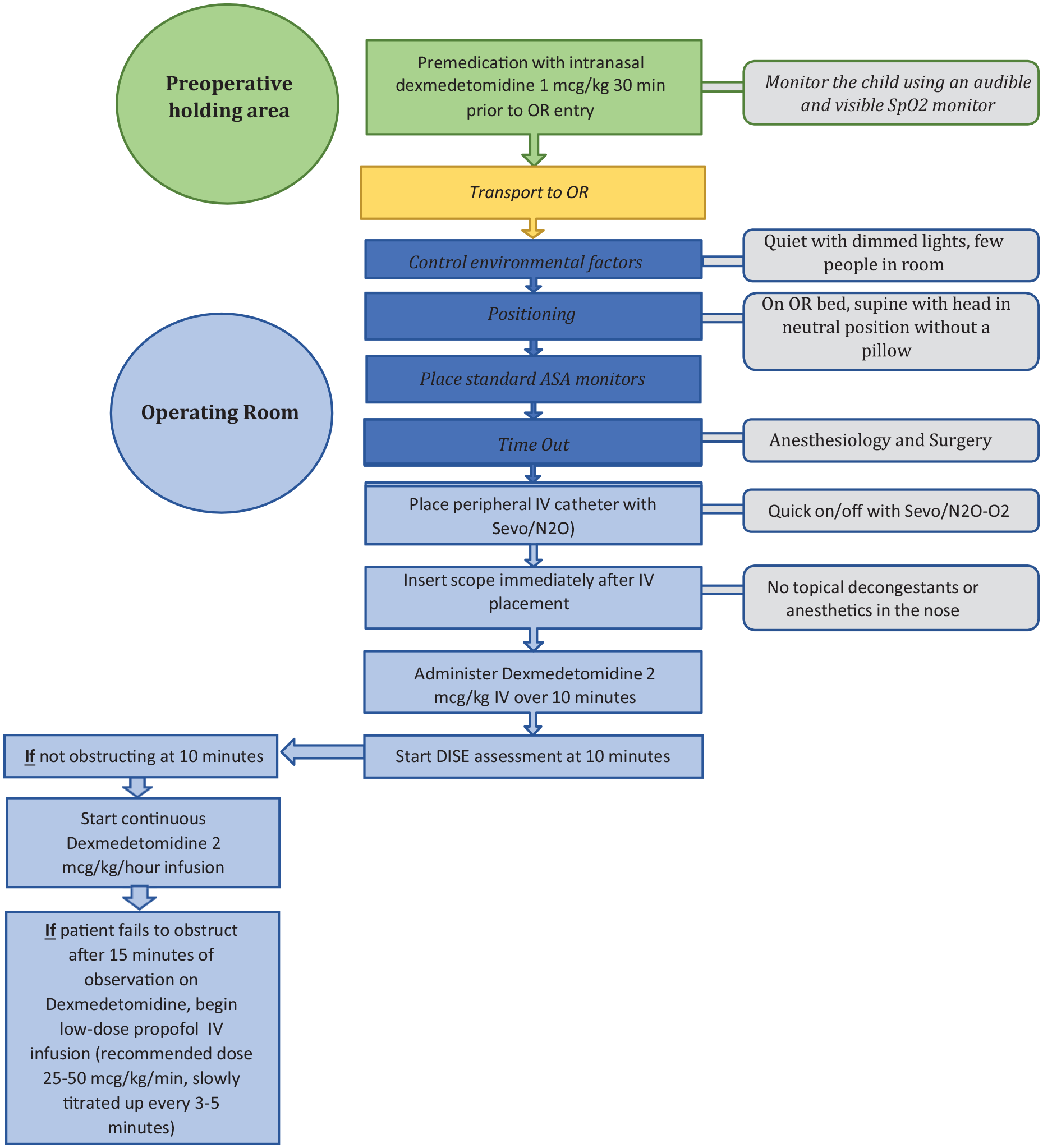
Streamlined DISE protocol following completion of PDSA-4. DISE, drug-induced sleep endoscopy; IV, intravenous; OR, operating room; PDSA-4, plan-do-study-act (final cycle).
Our QI initiative provided a protocol that was tolerated better by the patient and yielded more consistent outcomes. Nitrous oxide and sevoflurane are known for their very short duration of action.34,35 Therefore, the rapid on-off sequence allows for (1) the induction of general anesthesia, (2) the placement of the IV line and scope, and (3) then waiting to begin the assessment of the obstructive breathing pattern until the bolus is complete allows ample time to overcome any residual effects of these agents on the airway. Our revised protocol simulated the obstructive breathing pattern seen on the PSG and allowed the surgeon to create a management plan within 15 minutes. There was minimal reported morbidity and high concordance of satisfaction by surgeons and anesthesiologists.
Of note, this QI project was not designed to assess the protocol’s accuracy in simulating a child’s obstructive breathing pattern during unmedicated natural sleep but to create a reliable DISE protocol. Assessing the efficacy of a DISE protocol is complicated, and DISE-directed surgical success is multifactorial. Surgical outcomes are linked to the accuracy of DISE replicating a child’s true obstructive breathing pattern, a surgeon’s interpretation of DISE findings, selection of surgical treatment plan, and the technical success of the surgery. The interrater reliability of DISE is variable 36 and depends on the surgeon’s experience. 37 Regardless of all these factors, anatomic obstruction is just 1 component explaining why individuals have OSA. A patient’s arousal threshold, loop gain, and pharyngeal muscle responsiveness contribute to the presence of OSA. 38 An operation may be unsuccessful due to physiologic characteristics rather than the DISE’s accuracy or the technical aspects of the surgery.
As for intranasal dexmedetomidine, the benefit is 2-fold: to provide some sedation for OR entry and to serve as a loading dose for the procedure. Intranasal dexmedetomidine has been shown to be effective in reducing children’s separation anxiety from their parents.39,40 Its high bioavailability (80%) and <30-minute onset of action are also favorable. The loading dose may increase the likelihood of performing the DISE assessment at 10 minutes, although this was not part of our assessment of the protocol. We recommend that the child enter the OR approximately 30 minutes after dexmedetomidine administration to optimize its sedation benefit. A higher dose (2 mcg/kg) may optimize outcomes by increasing sedation levels, but our small cohort was underpowered to identify a statistical difference. Of note, a premedication dose of 1 mcg/kg was widely adopted by the pediatric anesthesiologists at our institution since it lessened the risk of bradycardia and arrhythmia for children with congenital heart disease and/or conduction abnormalities.
Overall, the complication rate of this protocol was low with the primary complication being bradycardia. The threshold to respond to bradycardia was variable; some anesthesiologists premedicate with atropine to minimize the risk. Our QI project did not investigate the use of an atropine pretreatment, nor did it measure the bias of individual anesthesiologists or surgeons. Not surprising, there were some children with severe desaturations in the OR. Intervention or treatment of desaturation was performed via stepwise airway manipulation with jaw thrust, administration of supplemental oxygen, and assisted ventilation with positive pressure by mask. The threshold for such intervention was based on clinical judgment, the child’s baseline asleep oxygenation from the PSG data, the intraoperative vital signs, and the anesthesiologist’s comfort level with the patient’s physiology in those moments. For children who had clinically significant oxygen desaturation during the DISE procedure, we left the flexible nasopharyngoscope in place, laying the scope on the child’s cheek and performing gentle mask ventilation over the nose, mouth, and scope with a partial or adequate mask seal. Following the last PDSA cycle, the protocol was officially modified to utilize supplemental oxygen and/or supportive airway maneuvers proactively for children with borderline SpO2 during the initial portion of the procedure but to remove it at least 2 minutes prior to the end of the bolus. Removal of the oxygen/airway maneuvers allows the child to achieve the natural breathing pattern for assessment by the surgeon.
One strength of this project was the creation of a dedicated MDT consisting of an ORRN who was a leader in the OR, a pediatric anesthesiologist who was highly involved with and dedicated to the otolaryngology surgical service, and a sleep medicine–trained pediatric otolaryngologist. Another strength is limiting DISE to those children with at least moderate OSA (ie, OAHI ≥5 events/h or at least 1 obstructive event every 12 minutes) or increased work of breathing from the PSG video assessment. Children with less severe OSA may require prolonged monitoring to detect an obstructive event that may be subtle obstructive hypopnea (reduction in airflow by 30%). Since our aim is to replicate natural sleep, we do not perform DISE on a child with mild OSA (<5 events/h) and no increased work of breathing by video. If a child with mild OSA exhibits frequent obstruction during DISE, it remains unknown if the medication effect has amplified an accurate obstructive breathing pattern or created a false one.
There were several limitations inherent in this QI project. Most important, each child’s response to a standard premedication, as well as tolerance of a stimulating procedure, is highly variable. Although IV insertion was a primary outcome variable in our PDSA cycle analysis, it was an indirect measure of the success of the intranasal dexmedetomidine premedication for PDSA-1 and PDSA-2. Due to the confounding factors of the dexmedetomidine premedication dose, the difficulty of IV access for some children, and the technical ability of the individual inserting the IV line, ranking of IV placement has the most variability. As another limitation, since the study was a QI project, it was not limited to a select group of anesthesiologists and attending surgeons. To overcome this obstacle, the MDT placed an updated protocol on the surgeon’s surgical preference cards and the internal anesthesiology departmental website. On the day of the DISE procedure, the ORRN would hand deliver the current PDSA cycle protocol and discuss expectations with each anesthesiologist assigned a specific patient. Despite an ORRN being present for each procedure, there were still times when a surgeon or anesthesiologist’s preference or clinical judgment resulted in a major protocol deviation. Bias was additionally introduced since the surgeon and anesthesiologist were not blinded to the protocol. Since there are no validated pediatric DISE sedation scales, the surgeon utilized the PSG asleep video description and baseline asleep SpO2 to provide guidance when a child was at the appropriate depth of sedation to assess the airway. Our approach is aligned with the DISE consensus statement, which stated that the level of sedation should be “titrated to audible snoring, an obstructive breathing patent or both.” 10 Of note, although some DISE protocols may use BIS monitoring, BIS has been neither validated in pediatric patients nor shown to be a useful assessment tool in the level of sedation or anesthesia (and therefore observable obstruction) in pediatric patients undergoing DISE. We can only assume but cannot demonstrate objectively that we achieved the appropriate sedation level at the time of our airway assessment. We further assume that protocol mimics natural sleep by utilizing dexmedetomidine as our primary sedation agent and allowing enough time (10 minutes) for the volatile agents to dissipate.
An additional limitation of this project was that only dexmedetomidine was tested as the primary sedation agent. At some institutions, propofol is the primary medication. It was not our intention to compare our protocol with those using other sedative agents. No comments can be made if our final protocol is more efficacious than those currently being used at different institutions. A multicentered trial would help to answer this challenging question and could be a future direction of our group. Alternatively, we aimed to design a series of PDSA cycles to establish a protocol that would consistently determine the obstructive breathing pattern for children and enable the creation of an OSA treatment plan while minimizing morbidity. Subsequently, this protocol is not entirely generalizable to all institutions. However, the MDT feels strongly that utilizing inhalational agents to obtain IV access and insert the flexible scope in the rapid on-off fashion optimizes DISE success regardless of the primary sedation medication. Multiple publications have established the efficacy of DISE-directed surgery.5-8 However, there are no QI publications that analyze the effectiveness of a specific DISE protocol.
As for implications to practice, a brief exposure to general anesthesia with a washout period is associated with increased patient tolerance and DISE quality. Since there is no universally accepted DISE protocol, it is important that institutions iteratively analyze their DISE protocols to ensure that they are providing consistent and reproducible results with minimal morbidity. For those institutions that do not have a standardized DISE protocol, one can adopt the Children’s Hospital Colorado protocol and be reassured that the protocol had been vetted for safety, reliability, and tolerability. Further research is also necessary to determine if there is a minimal OAHI threshold that is necessary prior to recommending DISE.
Conclusion
Administration of general anesthesia with inhalational anesthetics at the beginning of DISE to secure the IV line and insertion of the flexible scope in the rapid on-off technique optimizes patient tolerance and the success of the procedure when compared with administering dexmedetomidine. As a result of this QI process, the MDT was successful in optimizing patient tolerance and improving surgeon and anesthesiologist satisfaction while eliminating contingency steps. The final protocol ( Figure 2 ) provided a more predictable level of sedation, allowing the surgeon to appropriately view the patient’s anatomy during a state of simulated sleep and formulate an OSA management plan.
Supplemental Material
sj-pdf-1-oto-10.1177_01945998211036645 – Supplemental material for The Quest for a DISE Protocol
Supplemental material, sj-pdf-1-oto-10.1177_01945998211036645 for The Quest for a DISE Protocol by Kristin L. Mooney, Melissa Brooks Peterson, Jonathan R. Skirko and Norman R. Friedman in Otolaryngology–Head and Neck Surgery
Footnotes
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.