
Abstract
The “tonsil riots” of 1906 were panics that developed at several public schools in historically immigrant-dominated neighborhoods of New York City (NYC). Per archived newspaper articles, several NYC public schools asked for parental consent to have Board of Health physicians come and perform tonsillectomy and adenoidectomy on their students. When children subsequently returned home from school “drooling mouthfuls of blood and barely able to speak,” mothers reacted with panic and flocked to the schools demanding the safe return of their children. Police, ultimately, had to be called in to manage the crowds, and the events of 1906 largely faded from the public eye. However, these events can offer important lessons in communication and cultural humility as the United States continues its mass vaccination against coronavirus disease 2019.
The 100-year history of the tonsillectomy is contentious, with a relatively unknown, yet fascinating, controversy—the “tonsil riots” of 1906, which took place at public schools in New York City (NYC) and resulted in an enhanced local police presence for several months after. Although the events have faded from public memory, archived newspaper articles covering the riots, published locally by the New-York Daily Tribune and the New York Times, offer a glimpse into a story that touches on issues relevant to this day, such as informed consent, vaccine hesitancy, and public mistrust of the medical system.1-3
Tonsil Riots of 1906
The tonsil riots of 1906 were unorganized, spontaneous panics that developed at several public schools in historically, immigrant-dominated neighborhoods of NYC. The first and largest panic occurred in the Lower East Side on June 28, 1906, a Manhattan neighborhood well known for its population of Jewish and Italian immigrants.
At the turn of the 20th century in America, there were considerable public health efforts ongoing aimed at combating disease spread among the crowded dwellings that housed lower-income families, such as those of the Lower East Side. 4 These included campaigns promoting vaccination against smallpox, water treatment, and reducing the number of school absences due to recurrent respiratory infections. 4 Removing tonsils and adenoids in school-aged children, a novel procedure at the time, was promoted by surgical specialists as a solution to simultaneously reduce social disparity and curb the spread of disease in these crowded, low-income communities. 5
The tonsil riots began after a public school principal, referred to as Miss Simpson by newspapers, invited NYC Board of Health physicians to come into her school and treat students afflicted with recurrent upper respiratory diseases ( Figure 1 ).2,6 Hoping to save parents a trip uptown to where the hospitals were located, public schools set up surgical clinics in one of their classrooms and asked for parental consent to have Board of Health physicians come and perform tonsillectomy and adenoidectomy on the children.1-3 As noted in the available sources, this “consent” came in the form of a permission slip with a “yes” or “no” option for schoolchildren to take home and get signed.1-3 With limited ability to read English and no information regarding risks or alternatives to the surgery, some simply checked “yes” without understanding the implication.
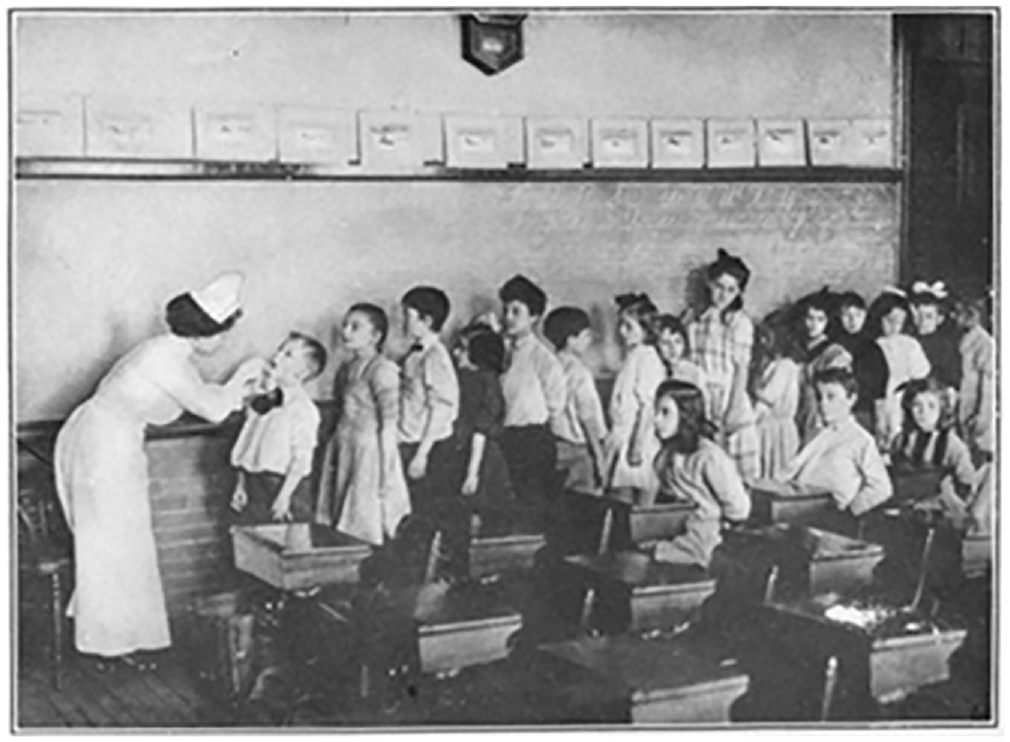
Depiction of routine throat inspections commonplace in schools. Used with permission from Gulick and Ayres. 6
When children subsequently returned home early from school “drooling mouthfuls of blood and barely able to speak,” 3 their mothers reacted with panic, not understanding, to what had occurred. The tonsillectomies performed at government-funded schools by government-employed physicians were disturbing surprises, especially in the context of a long history of government-sanctioned persecution these immigrants previously experienced. Jewish immigration to America throughout the late 19th and early 20th centuries was largely born out of Eastern European antisemitism and Russian government-sanctioned attacks against Jewish populations, called pogroms. 7 Soon, rumors of government-sanctioned violence, including the deaths of some children as a result of the procedure, circulated quickly in these tight-knit communities,1-3 mimicking the pogroms that had driven their relatives out of Eastern Europe just decades earlier. Thousands of parents descended on the locked doors of several public schools the afternoon of June 28, 1906, smashing windows, climbing ladders, and assaulting nearby individuals wearing glasses who were assumed to be physicians.1-3
Distraught family members flocked to the schools demanding the safe return of their children, and rioting eventually spread to the neighboring public schools in the Italian quarter.2,3 Police were called in to manage the crowds, and children across the city were released early from classes. 2 Over several days, with repeated assurances from school officials and observations that the children who underwent these operations recovered quickly and seemingly without lasting harm, the elevated tensions began to ease.1-3 Police continued to maintain a heavy presence until the end of the school year, some weeks later, but overall, the events of 1906 largely faded from the public eye. 3
Legacy and Lessons of the Tonsil Riots
The events of 1906 described above showcase how a single incident based on inherent mistrust of the medical system, compounded by ineffective communication, can produce even greater mistrust for the future. Repeated missteps and offenses by government and medical professionals alike, done without concern for the historical background of the marginalized groups they are caring for, have plagued the history of American medicine from the 20th century into modern times.8,9 These missteps have a cumulative impact, with each offense validating the future concerns and hesitancy with which a historically marginalized patient enters into the vulnerable state of the patient-physician relationship.
The tonsil riots offer important lessons in how to promote better trust with patients. First, this incident highlights the need for clear communication between clinicians and patients, especially those patients of lower-income and immigrant backgrounds. Not only should discussion of treatment be in the native language of the patient, but it should also avoid medical jargon, address medical uncertainty inherent in all medical interventions, and keep in mind the principle of patient autonomy in all decision making. Informed consent is more than just a permission slip; these conversations require artful communication, simplified medical terminology, and feedback to ensure understanding. This is especially true when dealing with patients from lower socioeconomic backgrounds, where lower levels of health literacy may complicate the process of informed consent. Only through tailored communication can an informed decision be made. And if that informed decision is to not procced with treatment, health care professionals must respect a patient’s choice without influence from his or her provider.
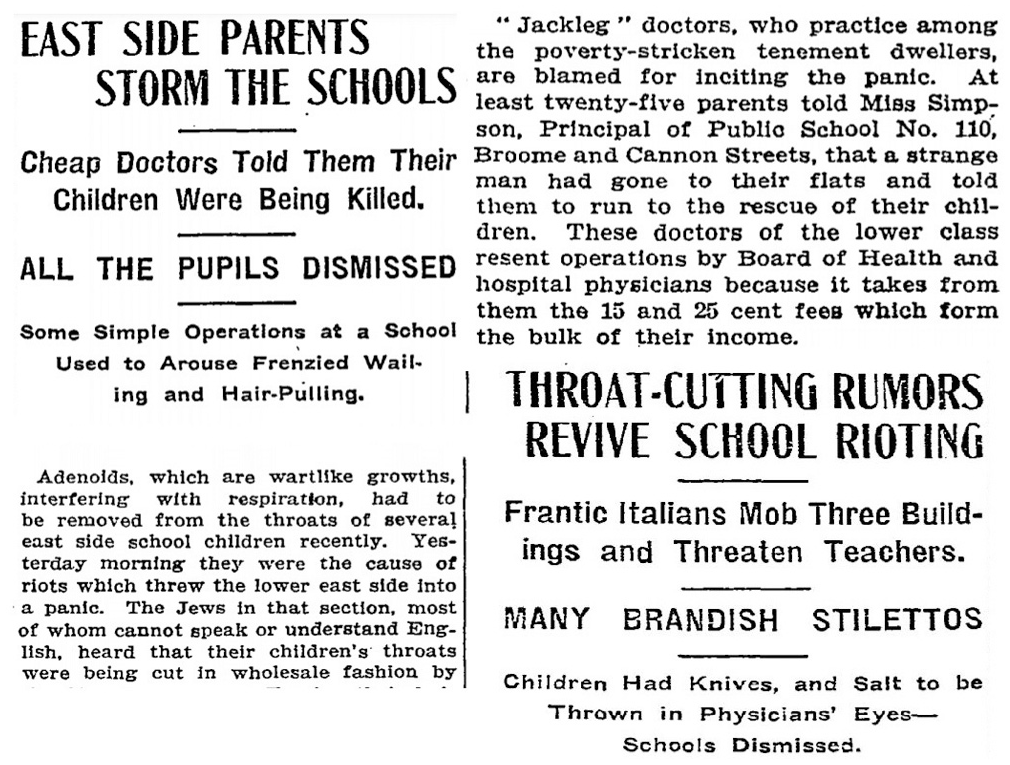
Second, health care professionals must also understand how the prior experiences of marginalized groups shape current perceptions of medicine. While this chronicle brings special attention to the medical mistrust among early Ashkenazi Jewish immigrants formed by their experience with antisemitism in Europe, the prior medical experiences of black Americans in Tuskegee and the LGBTQ community during the AIDS epidemic have also induced a lasting legacy of medical hesitancy.8,9 This mistrust has been further compounded by demeaning communication. For example, the primary sources covering the tonsil riots are filled with caricatures such as “Jackleg” Jewish doctors or the “frantic Italian mob”—portrayed as groups of people who have let greed or emotions supersede the best interests of the schoolchildren ( Figure 2 ).1-3 These references, which came from both journalistic embellishment and direct quotations from the school principals, capture a tone of superiority over those “rioters.” This dichotomy between those who know less and those who know better impairs the process of shared decision making.
Finally, health care professionals need to be humble, culturally aware, and knowledgeable of prior relevant experiences if they hope to reach communities previously marginalized by the American health care system. This lesson is particularly important as the United States attempts to combat the coronavirus disease 2019 pandemic through mass vaccination campaigns. Surveys have shown significant vaccine hesitancy rates among all Americans, but particularly among black Americans, with research showing how large a role institutional distrust in health care plays in rates of vaccine hesitancy among black Americans.8,10 Although the path forward is not entirely clear, keeping in mind our past failures will equip us with an awareness needed to sensitively communicate and promote better trust with our diverse public and patients.