
Abstract
Objective
The extent of neck dissection in papillary thyroid carcinoma (PTC) patients with lateral neck metastasis is controversial. This work aims to screen the patients suitable for superselective neck dissections including only levels III-IV.
Study Design
Prospective observational cohort study.
Setting
The study was conducted in a high-volume tertiary care setting.
Methods
A total of 134 consecutive previously untreated PTC patients with lateral neck metastases and subjected to 154 therapeutic lateral neck dissections (including levels II, III, IV, and VB) between June 2018 and March 2021 were enrolled. Fine-needle aspiration was performed preoperatively at each suspicious neck level. Clinical predictors were analyzed for occult lymph node metastases at levels II and VB.
Results
As a result, 44.8% and 5.8% of neck specimens exhibited metastatic lymph nodes at levels II and VB. In addition, univariate and multivariate analyses showed that the primary tumor in the ipsilateral thyroid upper lobe (P = .016, odds ratio = 3.528) and clinically multiple metastatic lymph nodes in level III-IV (P = .005, odds ratio = 6.414) were independent predictive factors for occult level II metastases. All 3 (1.9%) occult metastases at level VB were found in necks with preoperative multiple lymph node metastases.
Conclusions
A superselective lateral neck dissection including levels III to IV may be considered in patients with PTC when the preoperative evaluation identifies a single lymph node metastasis located at levels III to IV and the primary tumor is not in the upper lobe of the ipsilateral thyroid.
Keywords
Over the past few decades, thyroid cancer incidence has steadily been on the rise, with papillary thyroid carcinoma (PTC) accounting for the majority of cases. 1 PTC tends to metastasize to cervical lymph nodes, and this occurs in 30% to 80% of patients.2,3 The ratio is even higher if micrometastasis is included. 4 Notably, cervical lymph node metastasis (LNM) is a vital determinant of mortality and locoregional recurrence, and surgery is the first treatment option for LNM.5-8
Based on the current guidelines of the American Thyroid Association, “therapeutic lateral neck compartmental lymph node dissection is recommended for patients with biopsy-proven metastatic lateral cervical lymphadenopathy.” 6 Nonetheless, the precise scope of lateral neck dissection (LND) is unclear. Scholars have undoubtedly argued that the “berry-picking” strategy, in which only grossly abnormal lymph nodes are excised, is insufficient.9,10 Other authors have recommended dissection of levels II through V. 11 However, a considerable number of researchers believe that patients without extensive LNM may not require comprehensive neck dissection, and some levels could be omitted in the absence of suspected lymph nodes. 12 Based on the usual pattern of lymphatic spread for PTC, neck levels II and V exhibit a lower incidence of metastasis than do levels III and IV. 13 Dissection of levels II and V involves the spinal accessory nerve. Traction or dissection of this nerve potentially causes shoulder dysfunction, which impairs the quality of life. 14 The incidence of shoulder dysfunction ranges from 1.5% to 27% for comprehensive neck dissection. 12 A limited LND excluding these levels may reduce complications and shorten the length of the lower neck incision, thereby improving the cosmetic outcome of PTC patients with a younger age of onset and a normal life span.
A precise prediction of LNM at different cervical levels is the premise of limited LND. Ultrasound is the first approach used to evaluate cervical lymph nodes; however, it has a shortcoming of operator dependence. Fine-needle aspiration (FNA) is the most accurate and cost-effective method used for the detection of metastatic lymph nodes; in addition, measuring thyroglobulin (Tg) in the needle-washout fluid could further improve its diagnostic performance. 6 This study attempts to evaluate the diagnostic value of preoperative FNA for the detection of metastatic lymph nodes at different neck levels. Moreover, we aim to identify the predictive factors for occult metastasis at certain levels. The findings will boost clinical decisions in establishing the scope of neck dissection for patients with PTC with LNM in the lateral neck.
Patients and Methods
Study Population
This prospective study was approved by the institutional review board of Peking University Cancer Hospital (No. 2018KT101). Consecutive PTC patients with lateral neck metastases of a single surgeon were recruited between June 2018 and March 2021 from the Department of Head and Neck Surgery. All patients were initially treated. Patients with a previous history of neck surgery or thermal ablation in the neck, with nonpapillary cancer, or with distant metastases were excluded. Written and informed consent was obtained from all study participants.
Preoperative Evaluation
Ultrasound examinations using a scanner with a 12- to 15-MHz linear transducer was preoperatively performed, and suspicious lymph nodes were mapped and reported. The criteria of positive ultrasound included at least 1 of the following: hyperechogenicity, cystic changes, unbalanced inner echo, calcification, and roughly round shape (long/transverse diameter ratio <1.5).15,16
The most suspicious lymph node meeting the criteria at each level was selected for FNA. FNA was not performed without lymph nodes meeting the criteria at a certain level. A total of 12 levels were excluded from washout Tg testing since the levels had already been positively confirmed through FNA-C before visiting our institute. For other levels, the FNA was performed by a similar group of experienced, high-volume thyroid surgeons in charge of the operations. They used a high-resolution ultrasound (Mindray M9, Shenzhen, China) equipped with high-frequency linear array transducers. One to 4 suspicious lymph nodes were aspirated in each neck using a 23- or 25-gauge needle attached to a 2-mL disposable syringe. Some of the aspirated material was directly smeared onto glass slides then immediately immersed in 95% alcohol for staining. The remaining material in the syringe was injected in a preserving fluid for cell block processing when needed. The same needle and syringe set were rinsed using 1 mL of normal saline for the measurement of washout Tg levels. For FNA-C, malignant or suspected malignant were counted as positive; for FNA-Tg, the cutoff value for metastasis was 1.0 ng/dL, as previously reported. 17 Either FNA-C positive or FNA-Tg positive was counted as FNA positive.
Levels of the lateral neck were defined following the classification standard proposed by the American Head and Neck Society and the Committee for Head and Neck Surgery. 18 Level II extends from the skull base to the inferior border of the hyoid bone. The lymph nodes were divided into sublevel IIA and IIB using a vertical plane defined by the spinal accessory nerve. The inferior border of the cricoid cartilage was used to define the boundary between levels III/IV and levels VA/VB. The anterior boundary of levels II-IV is the lateral border of the sternohyoid muscle, and the posterior boundary is the posterior border of the sternocleidomastoid muscle. 19
All cases were divided into 3 groups based on the number and location of metastatic nodes, including (1) single-node metastasis, (2) multiple-node metastases in 1 level, and (3) multiple-level metastases. The process of grouping is illustrated in Figure 1 .
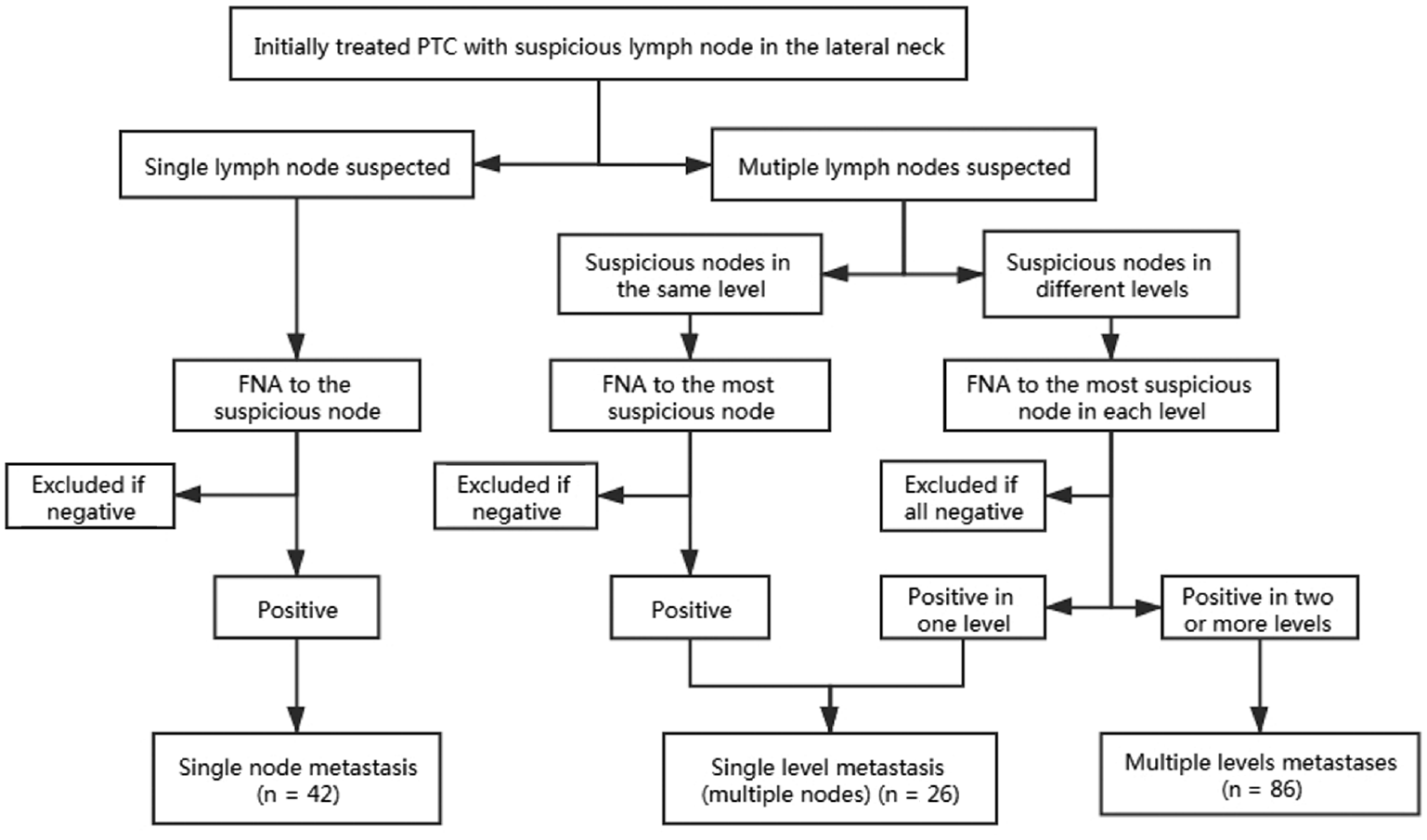
Flow chart of grouping lateral necks by preoperative fine-needle aspiration. PTC, papillary thyroid carcinoma; FNA, fine-needle aspiration.
Contrast-enhanced computed tomography (CT) of the neck was performed in 114 patients (85%), with a reconstructed slice thickness of 2 mm. The locations of the primary tumors were primarily described based on ultrasound images and the CT coronal view if available. The thyroid was divided equally into 3 anatomical portions from the upper pole to the lower pole, named as the upper, middle, and lower lobe. Tumor location was determined based on the center of the main lesion. The diffuse sclerosis variant of PTC was located in the middle lobe. The primary tumor location was in the contralateral lobe if there was no visible tumor in the ipsilateral thyroid of lateral LNM based on preoperative imaging.
Lymph Node Dissection and Histopathological Examination
All patients underwent total thyroidectomy with central neck dissection and LND. The extent of dissection included levels II (IIA and IIB), III, IV, and VB. The spinal accessory nerve, sternocleidomastoid muscle, and internal jugular vein were spared during neck dissection. The boundaries between the different levels were equal to those used in the ultrasound examination and were marked with sutures during the operation. Based on the suture marks, the LND specimens were divided into levels and sublevels (IIA, IIB, III, IV, and VB), labeled, and then separately processed.
The final pathological diagnosis was conducted by at least 2 expert pathologists after reviewing the surgical specimens. The following factors were assessed: primary tumor size (longest diameter of the largest lesion), multifocality, extrathyroidal extension, underlying thyroiditis, and LNM. The thyroid cancer stage was determined based on the guidelines of the American Joint Committee on Cancer (eighth edition). 20
Statistical Analysis
Continuous variables were described by the median and range, whereas categorical variables were described by numbers and percentages. The diagnostic value of FNA for predicting metastatic lymph nodes was characterized by sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), respectively. Clinical and pathological characteristics were analyzed to identify predictive factors related to occult level II LNM. Univariate analysis of patients with and without occult level II metastasis was performed using the 2-sided Pearson test or Fisher exact test. Significant variables with P < .05 in the univariate analysis were included in a multivariate logistic regression analysis. The results were reported as the odds ratio (OR) with a 95% confidence interval (CI). Two-sided P values of <.05 were considered statistically significant. All statistical analyses were performed using the IBM SPSS software version 22.0 (IBM, Armonk, New York, USA).
Results
Clinicopathological Features of PTC Patients
A total of 134 consecutive patients were eventually enrolled, comprising 50 men and 84 women; the median age was 36.5 years (range, 18–81 years). The median size of the primary thyroid cancer was 1.6 cm (range, 0.2–6.5 cm). Notably, 22 (16.4%) patients had microcarcinoma. Gross extrathyroidal extension and multifocality of primary tumors were found in 37 (27.6%) and 76 (56.7%) patients, respectively. Altogether, 37 (24.0%) lateral necks had tumors originating from the upper lobe of the ipsilateral thyroid gland.
Bilateral metastasis was observed in 20 (14.9%) patients. As shown by the preoperative imaging, the median size of the largest positive lymph nodes was 1.5 cm (range, 0.4–5.5 cm). The extranodal extension was noted in 85 (55.2%) patients ( Table 1 ).
Patient Characteristics.
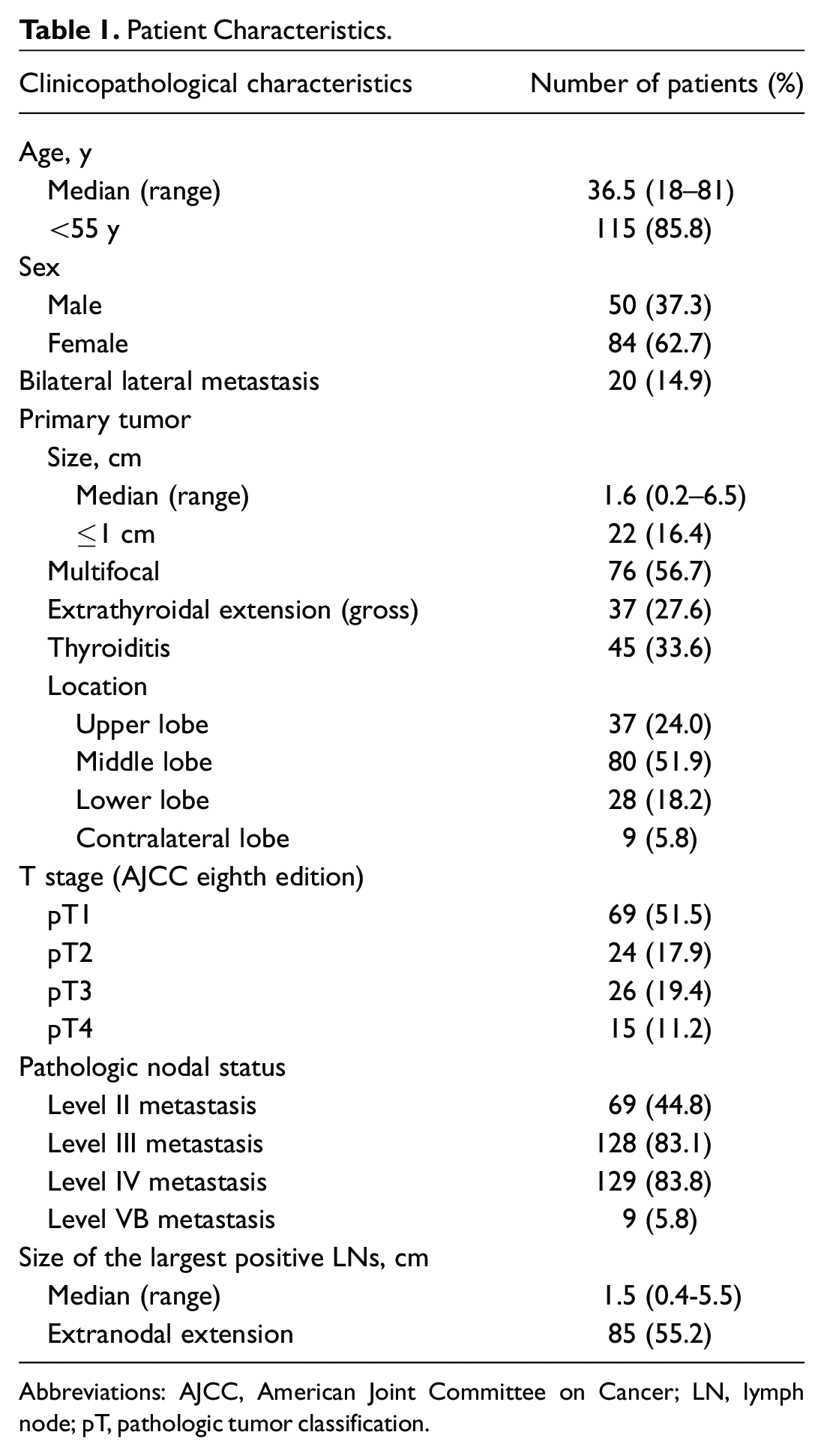
Abbreviations: AJCC, American Joint Committee on Cancer; LN, lymph node; pT, pathologic tumor classification.
Diagnostic Value of Preoperative FNA for Identifying Metastatic Neck Levels
A total of 367 FNAs were performed; 269 of these were positive (either cytologically positive or washout Tg elevated). The diagnostic accuracy increased from level II to level VB. The sensitivity, specificity, PPV, and NPV of FNA for identifying metastatic levels are summarized in Table 2 .
Diagnostic Value of Preoperative Fine-Needle Aspiration at Different Cervical Levels in Comparison With Histopathology.
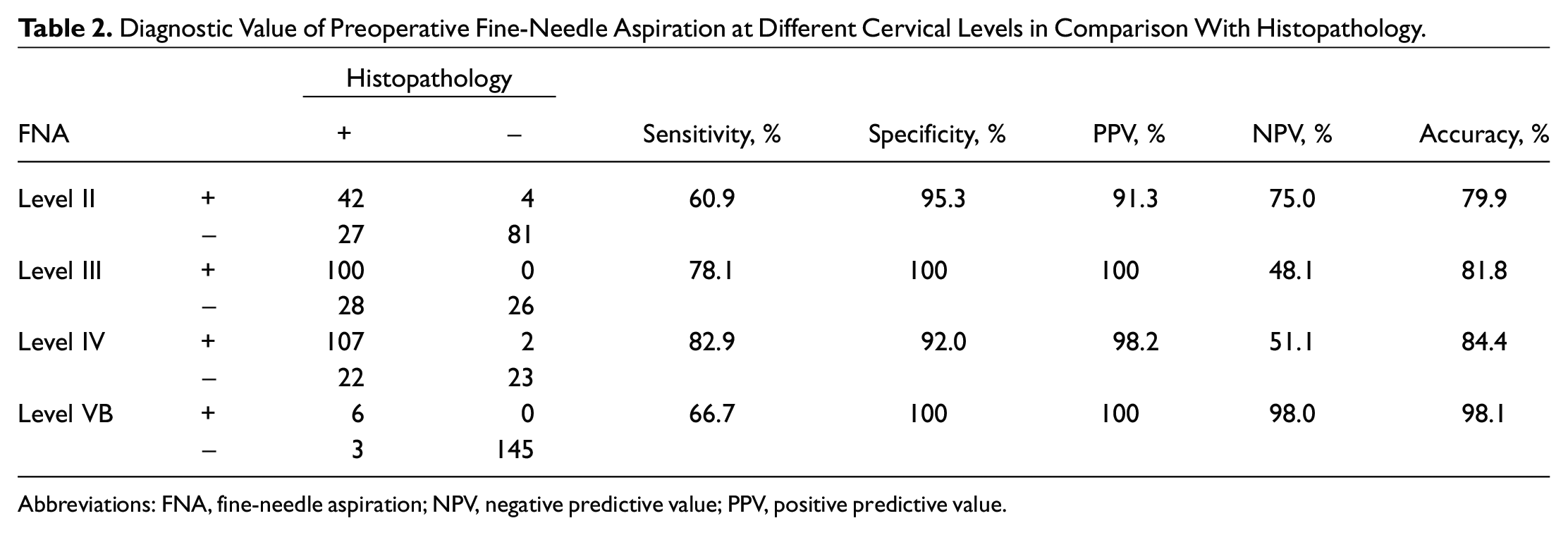
Abbreviations: FNA, fine-needle aspiration; NPV, negative predictive value; PPV, positive predictive value.
Preoperative FNA demonstrated a single-level LNM in 74 necks (48%) and multiple levels LNM in 80 necks (52%); 34 necks were single-level LNM in histopathology. Ultrasound and FNA diagnosed 42 single LNM (27%) and 112 multiple lymph node metastases (73%); histopathology confirmed 25 single LNM.
Predictive Factor of Occult LNM in Level VB or Level II
A total of 9 cases (5.8%) had histologically positive lymph nodes in level VB; 6 were correctly diagnosed by FNA before surgery. The NPV of FNA in diagnosing level VB metastasis was up to 98.0%. All patients with occult-level VB metastases exhibited simultaneous positive level III and IV lymph nodes; isolated metastatic level V lymph nodes were not found.
In total, 46 (30%) cases had clinically positive lymph nodes in level II; the remaining 108 necks were clinically negative. Occult metastases in level II were observed in 27 (25%) necks, and 25 of them were located in sublevel IIA, with the other 2 in both IIA and IIB.
Clinicopathologic variables were examined for the prediction of occult level II LNM ( Table 3 ). Univariate analysis revealed that occult LNM in level II was frequently found in patients with clinically multiple LNM in neck levels III and IV as compared with those with single LNM at these levels (P = .002). When clinicopathologic factors of the primary tumor were considered, the occult LNM incidence at level II was greater when the tumor was located in the upper lobe of the ipsilateral thyroid (P = .018).
Relationship Between Clinical and Histological Features of Occult Level II Lymph Node Metastasis. a
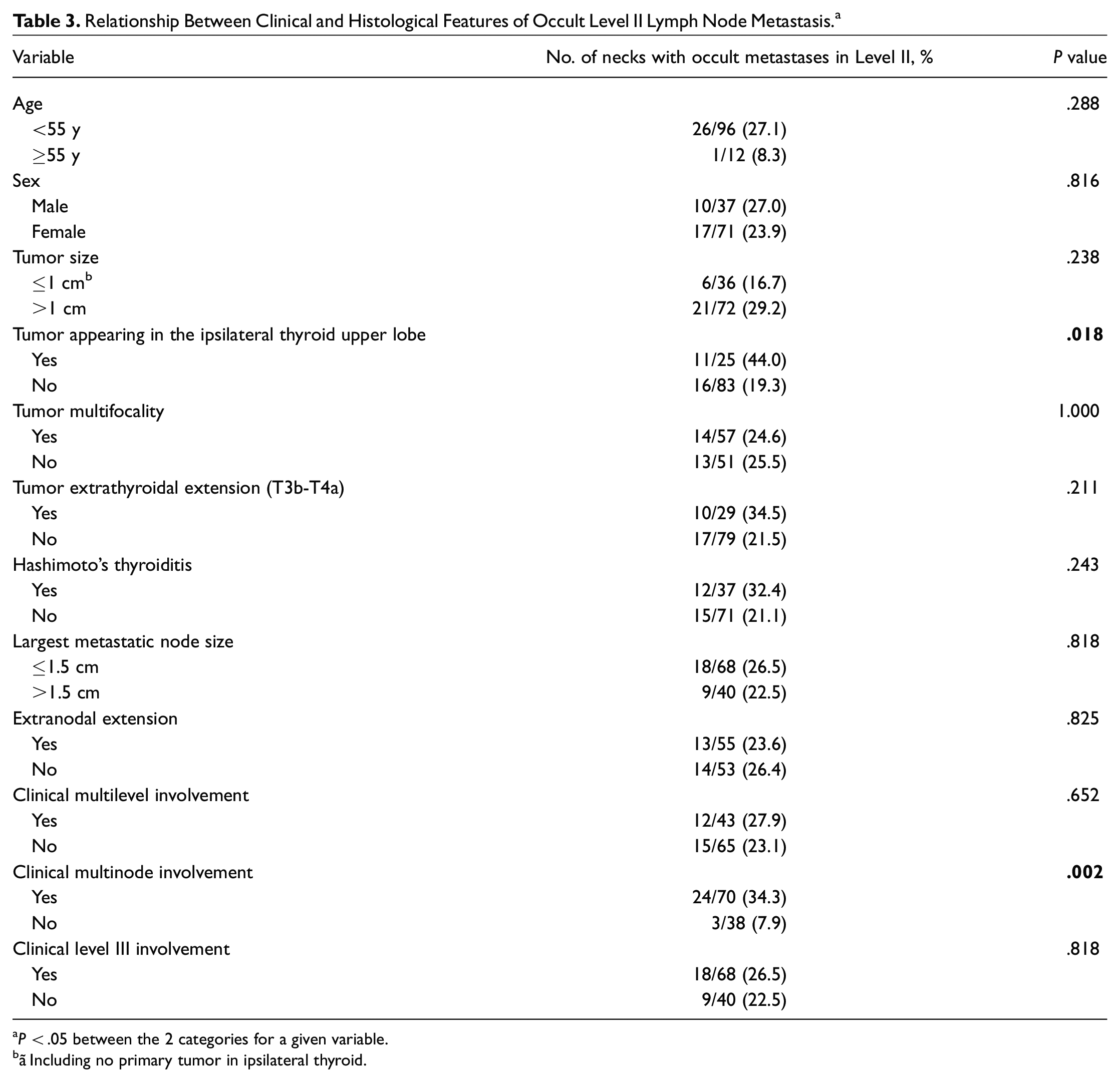
P < .05 between the 2 categories for a given variable.
ãIncluding no primary tumor in ipsilateral thyroid.
Two variables were included in a multivariate logistic regression analysis. Primary tumor in the ipsilateral thyroid upper lobe (P = .016, OR = 3.528) and clinically single metastatic lymph node in level III-IV (P = .005, OR = 6.414) were independent predictive factors for occult level II metastases ( Table 4 ). When neither of these predictive factors was present, the probability of occult LNM at level II was 3.3% (1/30).
Multivariate Analysis for the Identification of Prognostic Factors for Occult Level II Lymph Node Metastasis.
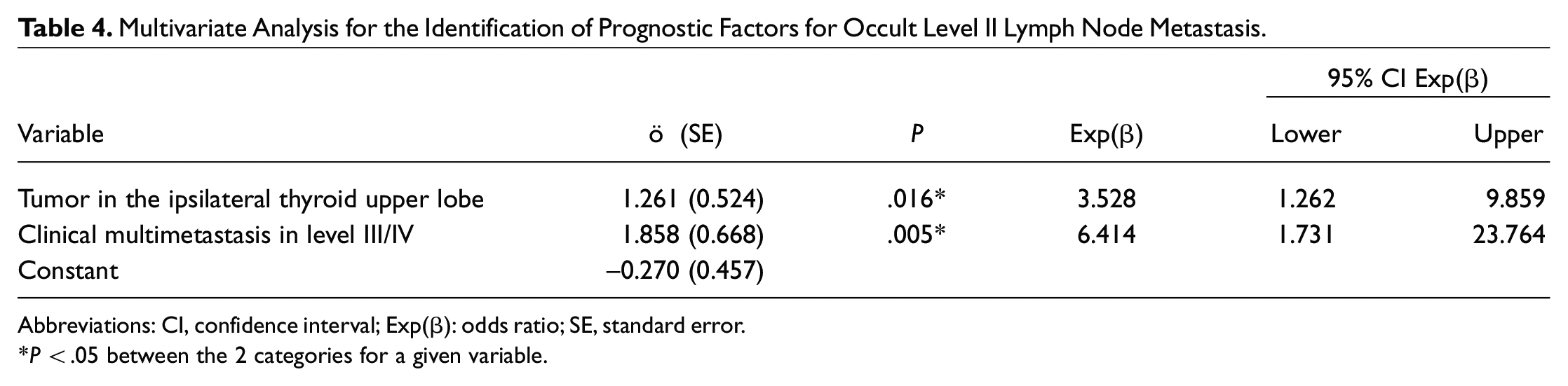
Abbreviations: CI, confidence interval; Exp(β): odds ratio; SE, standard error.
P < .05 between the 2 categories for a given variable.
Surgery-Related Outcomes and Follow-up
A total of 7 of 134 patients (5.2%) developed transient “shoulder syndrome,” encompassing shoulder dysfunction and pain, all of whom completely recovered. Further, a chyle leak occurred in 3 patients (2.2%), including 1 who developed chylothorax and required closed thoracic drainage. All recovered after dietary management, and none needed a second operation. One patient (0.7%) had a wound infection but healed after being administered antibiotics.
All patients received thyroid-stimulating hormone suppression therapy. The median follow-up time was 22 months (range, 3-36 months). Recurrences of the ipsilateral lateral neck (one in level IV and another in level VA) were reported in 2 patients. One patient had a contralateral cervical recurrence, and another developed central compartment recurrences. None developed distant metastases.
Discussion
The extent of neck dissection for PTC patients with lateral neck metastasis remains controversial. This is primarily attributed to a lack of evidence showing that LNM affects overall survival. A modified radical neck dissection including levels II to V is the formal approach to treat metastatic PTC to lateral cervical lymph nodes. Nonetheless, recent studies have opposed extensive LND due to the potential increase in morbidity. Furthermore, there is no significant benefit of survival compared with selective neck dissection.12,21
Several lines of evidence indicate that the incidence of involved lymph nodes is lower at levels II and V than at levels III and IV. 13 This is possibly because the pattern of LNM is sequential. Levels II and V lymph nodes are located far away from the primary tumor compared with levels III and IV. Our findings are consistent with this rule. This means that these 2 levels should be routinely included in therapeutic neck dissection procedures for N1b PTC patients.
Level V has the lowest incidence of metastasis; its proportion is between 8.5% and 53.3% based on the literature.12,13 Most metastases from PTC occur at sublevel VB, and involvement of sublevel VA is rare. Scholars unanimously agree that therapeutic dissection of level V is indicated when there is clinical evidence of disease involving this area 22 or for those with 3-level simultaneous metastasis. 21 We also found that level VB metastases are relatively infrequent; the percentage was even lower than that of many previous studies. The possible reasons include the following. First, only sublevel VB lymph nodes were removed. Second, specimens were sorted by intraoperative labeling based on preoperative imaging, which was different from previous retrospective studies. Third, this study included only initial operation cases, and the LNM might be less extensive. In line with other studies, most metastatic lymph nodes could be diagnosed before surgery, and occult metastasis only occurs when multiple levels are positive in preoperative FNA. As such, when clinical LNM only involves 1 level except for level V, level V can be spared to minimize potential morbidity.
The management of neck level II is controversial because of the relatively low sensitivity and specificity of imaging for detecting LNM in this region. 23 FNA-C and FNA-Tg were combined with ultrasound to reduce false-positive rates. When the preoperative ultrasound or FNA was negative, the incidence of level II occult metastasis in our study population was 25%. This agrees with 19.2% to 34.5% in previous studies.23,24 This indicates that prophylactic dissection of neck level II appears unnecessary in 3/4 of patients.
Considering the morphology of the thyroid, the superior portion of the thyroid gland has a relatively small amount of tissue. Tumors in this area might be assumed to cause early extrathyroidal extension and regional metastasis. Studies showed that superior located PTC is a risk factor for clinical and occult lateral LNM.25-28 These findings suggest that a more radical surgery should be considered in PTC patients with primary tumors located in the superior lobe of the thyroid.
The regional spread pattern of PTC is also identified by the location of the primary tumor. Tumors originating from the middle and lower lobe of the thyroid gland appear to run through the lymphatic vessels along the middle and lower thyroid veins, involving the central compartment and levels III to IV in the lateral neck. Conversely, the upper lobe of the gland is in the drainage area of the superior thyroid vein; the lymphatic vessels also follow its path to lymph nodes in level II, skipping level VI and level III-IV. 29 Therefore, assessment or treatment for level II LNM is specifically important when PTC lesions are located in the superior pole of the thyroid.
The involvement of adjacent neck levels is another predictive factor associated with occult level II LNM. One study found that image-based isolated lateral level IV metastasis is an independent predictor of negative level II pathologically. 23 Through preoperative ultrasound and postoperative pathology, a different study showed that occult LNM in level II is frequently found in patients with simultaneous metastatic lymph nodes at neck levels III and IV compared with patients with metastatic lymph nodes in neck levels III or IV alone. 24 Herein, we used different preoperative evaluation methods. Improved accuracy of the ultrasound has been shown with the addition of FNA cytology with or without Tg assay in the detection of lateral neck node metastasis.6,30 This might lead to a strict criterion of multilevel metastases. Although more occult LNMs in level II were in patients with multilevel metastases, no statistical significance was observed. Instead, a clinically solitary abnormal lymph node in neck level III or IV had a lower risk of occult metastasis in level II. Despite the limited accuracy of ultrasound in diagnosing abnormal lymph nodes in the setting of finding solitary abnormal nodes, 31 it helps in eliminating potential cases of multilevel metastasis.
This article aimed to identify patients for limited LND without prophylactic level II and V lymphadenectomy and to attain complete cancer clearance with minimal postoperative complications. Kim and colleagues 32 reported that superselective neck dissection displayed minimal morbidity and did not compromise oncologic outcomes in patients with clinically unconfirmed suspicious lateral neck nodes. Based on our criterion (ie, the primary tumor not located in the upper lobe of ipsilateral thyroid with clinically single LNM in level III-IV), the incidence of occult-level II metastasis was 3.3%, without metastasis in level V. Since occult lateral neck lymph node is present in 20% to 69% of PTC patients with cN0 stage disease,33-36 prophylactic level II and V dissection may be unnecessary in these patients.
The short follow-up period and insufficiency of long-time outcome data are the shortcomings of this work. Therefore, further prospective controlled studies are necessary to focus on the contrast between limited neck dissection and comprehensive neck dissection, to achieve a balance between radical resection of cancer and quality of life.
Conclusions
Metastases to neck level VB occur only in PTC patients with clinical level V involvement or multiple-level metastases. Besides, primary tumors in the upper lobe of the ipsilateral thyroid and clinical multiple LNM in neck levels III-IV are significantly associated with occult LNM occurrence in level II. Therefore, we recommend a superselective LND including level III-IV to be performed in PTC patients without primary tumor located in the upper lobe of the ipsilateral thyroid or multiple LNM in levels III-IV during preoperative evaluation.
Footnotes
Author Contributions
Disclosures
Data Statement
The data may be shared with the researchers working on this subject if required for doing a meta-analysis or some other form of research.