
Abstract
Objective
Infants with posterior tongue-tie (PTT) can have substantial difficulty with breastfeeding and bottle-feeding. This study aimed to address the dearth in investigational objective data surrounding PTT release to better quantify the postoperative impacts of frenotomy for ankyloglossia.
Study Design
Prospective randomized, controlled trial.
Setting
Private practice clinic.
Methods
In a prospective, randomized controlled trial, infants 3 to 16 weeks of age with PTT undergoing frenotomy were examined using a bottle-feeding system capable of objectively measuring tongue function. Validated patient-reported outcome measures were also obtained simultaneously.
Results
Forty-seven infants with PTT were enrolled into an observational/control arm (n = 23) or interventional/surgical treatment arm (n = 24). The total cohort consisted of 29 (61.7%) male infants with a median age of 39 days. At the day 10 time point, the interventional arm demonstrated statistically significant improvement in 11 objectively obtained feeding metrics, indicating faster tongue speed, more rhythmic and coordinated sucking motions, and a tongue more capable of adapting to varying feeding demands. Significant improvement in breastfeeding self-efficacy was reported in the interventional group while poor self-confidence persisted in the observational group. Infant reflux symptoms improved in the interventional group while not in the control group. Nipple pain also persisted in the control group but improved in the surgical cohort.
Conclusions
When measured 10 days after frenotomy for PTT, infants improve feeding parameters using an objective bottle-feeding system. Similar improvements are seen with patient-reported outcomes when PTT is released. Posterior tongue-tie is a valid clinical concern, and surgical release can improve infant and maternal symptoms.
Infant feeding problems are among the most common difficulties encountered by both medical practitioners and families caring for them. Despite recent advances in understanding oral breastfeeding physiology1,2 and anatomy,3,4 management of those problems remains challenging. It is estimated 25% to 45% of infants experience feeding difficulties at some point. 5 Previous studies demonstrate that ankyloglossia may contribute to feeding problems.6-10
Tongue physiology during breastfeeding and bottle-feeding remains misunderstood. Recent studies have demonstrated that mid-tongue elevation toward the palate is the initiating step of seal formation. 1 Common teaching holds that tongue protrusion beyond the gumline precludes the diagnosis of ankyloglossia, despite a lack of supporting evidence. More recently, studies have evaluated surgical release of mid-tongue restriction in the form of posterior tongue-tie (PTT).11-13 While several studies have demonstrated that PTT release improves infant feeding, the overall body of evidence is still lacking. 14 Given the incidence of frenotomy (especially for PTT) is significantly increasing,15,16 there is need for higher-quality evidence to determine whether surgical interventions are warranted.
Advances in feeding technology have allowed clinicians to accurately measure and compare tongue function metrics. The nfant Feeding Solution (nFS; NFANT Labs) is a device approved by the US Food and Drug Administration (FDA) for quantifying sucking signals during bottle-feeding. nFS has been used to study critical feeding care questions related to preterm and full-term infants with feeding challenges, 17 as well as differences between sucking patterns of preterm vs full-term infants 18 and those with neonatal brain injury. 19
Our previous studies have shown improvement in maternal and infant feeding symptoms following frenotomy.11,12 However, no published studies have demonstrated quantifiable impairment in lingual function in the presence of PTT or improvement in lingual function after frenotomy. In addition, data showing that PTT release improves bottle-feeding symptoms do not currently exist. This study uses an objective bottle-feeding system to measure lingual function surrounding PTT release while corroborating findings with maternal-reported symptom changes. We hypothesize that PTT release objectively and subjectively improves infant feeding.
Materials and Methods
Study Design and Participants
Study participants included mothers and infants, ages 3 weeks to 4 months (≥36 weeks gestational age), who underwent surgical correction for PTT. To avoid introduction of the bottle in dyads nursing exclusively, infants were required to be already partially bottle-feeding. Participants were recruited and enrolled by the principal investigator (PI: B.A.G.) into a single-institution, randomized controlled trial (RCT) within a private practice setting (clinicaltrials.gov registration: NCT03793414) approved by an institutional review board (Providence Health & Services IRB #STUDY2018000616). Participants were ensured study participation involved minimal risk and was voluntary.
Age-eligible dyads were recruited when scheduling appointments; parent(s) were directed to review study information to minimize the chance of withdrawal. Because each nFS system is allocated to 1 patient and cannot be reused, study adherence was emphasized to parent(s) to avoid the monetary losses associated with study withdrawal. Participants were followed up to 20 days after randomization into either a surgical arm involving frenotomy on the day of enrollment or an observational/control arm that delayed frenotomy until ~10 days after enrollment and randomization.
Randomization Scheme
Simple randomization of this convenience sample was accomplished by the PI using a virtual coin toss (in the presence of the parents) after study counseling and informed study consent.
Study participant dyads completed all survey measures during initial encounters. For dyads randomized into the surgical treatment arm, outcome measures were completed approximately 10 days postprocedure. For dyads randomized into the control arm, outcome measures were completed immediately prior to frenotomy (10 days after enrollment) and another 10 days postprocedure (day 20; Figure 1 ) if they chose to proceed with frenotomy. Dyads randomized to the control arm continued with therapies employed before study enrollment (eg, lactation support, suck training, and/or physical/craniosacral therapy).
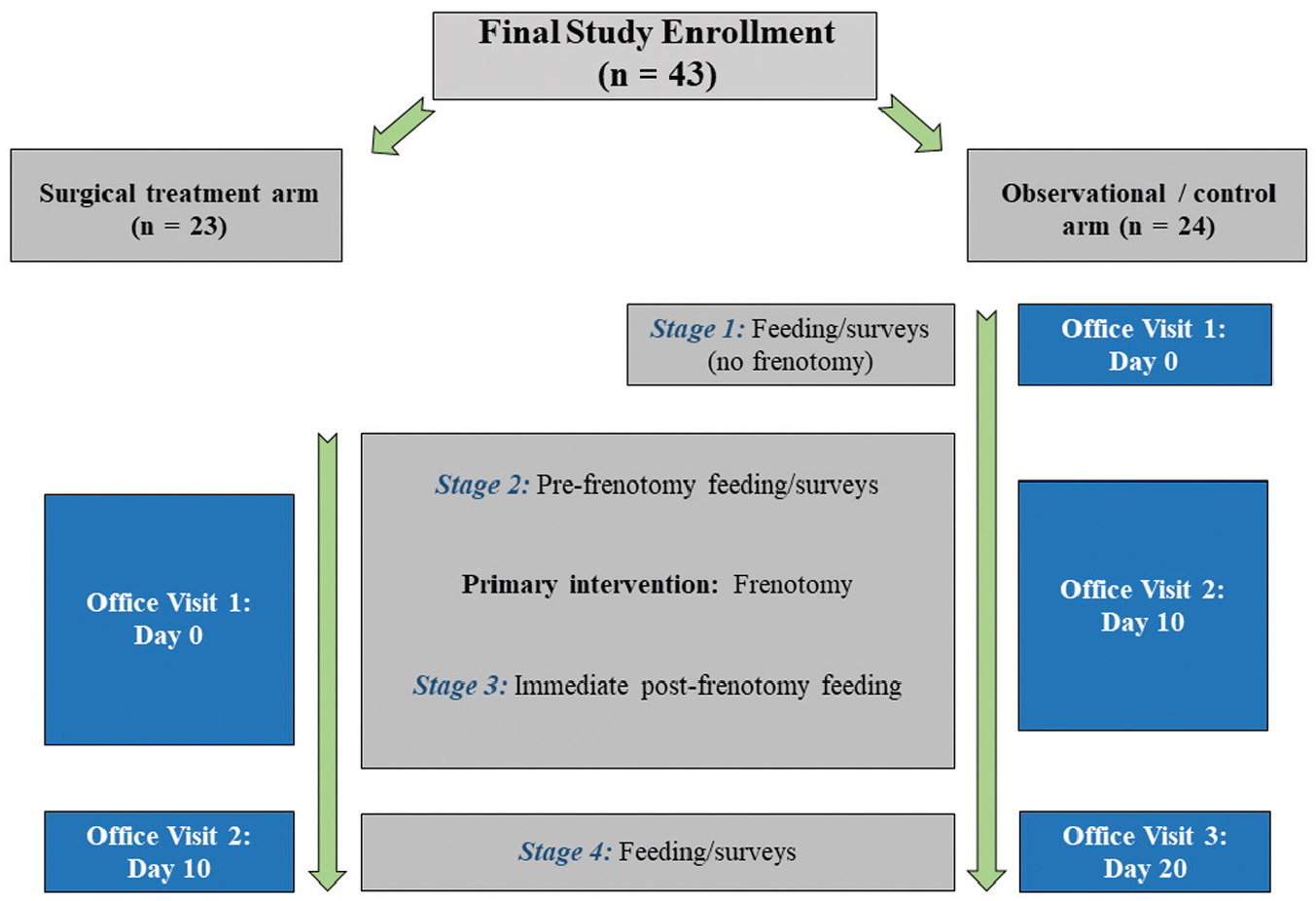
Timelines for survey completion and treatments.
Infant Assessment
Mandatory evaluation by lactation consultants before referral was a prerequisite for consultation. Latch assessment was considered in decision making to determine whether frenotomy was offered. Targeted examination was completed to determine if PTT was present, examining for palpably restricted frenulum with lingual elevation, limitation of lateral movement, abnormal floor of mouth elevation with tongue elevation, and frenulum attachment location. Sucking evaluations were performed, noting gum/lip grip, cupping/seal of the tongue against the finger, and the nature of the sucking tongue movements. Standardized frenulum grading followed the Coryllos classification system. 20
Exclusion Criteria
Infants were not considered for participation if they presented with comorbid diagnoses of the heart, lungs, or brain. Additional exclusions included infants born from multiple births or diagnoses that potentially impair breastfeeding success (eg, neurological conditions, cleft lip/palate, abnormalities of the throat/esophagus) or a mother’s diagnosis of insufficient glandular tissue. Infants with anterior tongue-tie (type 1/2) 20 or lip-tie were also excluded.
Study Intervention
Informed consent was obtained from the parent(s) before infants were moved to a laser-safe operatory. Topical anesthetic gel (3% lidocaine/3% tetracaine) was applied with a Q-tip. Frenotomy was performed with a 10,600-nm CO2 laser (LS-1005; LightScalpel) with variable pulsed settings using a 250-micron diameter focal spot handpiece. For infants <6 weeks of age, lasing settings were 2-W, 5-ms pulses at 50 Hz (average power = 0.5 W). For infants ≥6 weeks of age, lasing settings were 2-W, 10-ms pulses at 40 Hz (average power = 0.8 W). The tongue was elevated using a grooved director; starting at the leading edge of the frenulum, midline tissue was incised and an ~1-mm deep central window was opened in the mucosa overlying the genioglossus muscle. The window was extended laterally on both sides to release mucosa, taking care to not disturb the fascia of the genioglossus, resulting in a diamond-shaped wound. The baby was returned to the parent(s) where stretching exercises were advised to avoid reattachment of tissue by gently elevating the tongue and massaging the wound, a common practice of the lead author.
Bottle-feeding Outcomes
Measurements during bottle-feeding were obtained for both treatment arms using the nFS, which measures tongue movement, transmitting wirelessly to a tablet that permits real-time assessment. The system consists of couplings that connect to bottles ( Figure 2 ); these allow liquid to flow while connected to a Bluetooth sensor that detects the movement of a cantilever located within the nipple. Data were analyzed postfeeding using algorithms to identify features of waveforms created from each suck. These features include basic curve descriptors (ie, signal wavelets), wavelet variability that evaluates skill/maturation, and metrics of sucking coordination/maturation. Multiple measures were averaged over each sucking burst for the entire feed. Feeding sessions were completed in the office in the presence of the PI; parents fed the baby using the nFS, and when the session was terminated, captured data were automatically transmitted.

Components of the bottle-feeding system. (A) Bottle coupling with nipple cantilever. (B) Wireless sensor. (C) Recording tablet. (D) Fully assembled system.
Symptom-Based Outcome Measures
During each visit, participating mothers were asked to complete 3 surveys: the Breastfeeding Self-Efficacy Scale–Short Form (BSES-SF; ©2003; University of Toronto), 21 the Gastroesophageal Symptom Questionnaire for Infants (GSQ-I; ©2004, Pfizer), 22 and a visual analog scale (VAS) to evaluate current breastfeeding pain on a continuum. The BSES-SF is a validated, 14-item survey that measures breastfeeding efficacy and confidence using scales between 0 (not at all confident) and 5 (very confident). Total scores are summarized (range, 0-70), where higher scores indicate lower breastfeeding impairment/higher confidence. The GSQ-I quantifies the duration and severity of 6 to 8 symptoms associated with infant reflux. Respondents indicate how many times symptoms occurred within the previous 7 days with follow-up questions to rate symptoms between 1 (not at all severe) and 7 (most severe). Last, mothers were asked to report pain severity, using a standard VAS associated with current breastfeeding between 0 (no pain) to 10 (worst pain). Response data were tabulated by a research assistant who was not clinically involved and did not have direct contact with participant dyads or with the PI during data entry.
Sample Size and Biostatistical Analyses
Sample size was estimated using differences in paired-sampling mean values for peak bottle measures between baseline and day 10 follow-up. Assuming a 2-tailed test, a .05 α level, an 80% power (1 –β) error probability, a conventional within-subject Pearson correlation (R = 0.50), and an equal standard deviation value of 9.8, a total of 23 subjects were required to detect a mean difference of at least 6.0 points (~11%) for each treatment arm. Post hoc analyses using those parameters indicated adequate power to identify between-group differences of at least 8.3 points on average using a total of 46 subjects.
Patient-level data were assigned unique study identification numbers while protected health information was removed prior to database entry and review. Descriptive analyses and statistical comparisons were completed using SPSS software (version 26.0; SPSS, Inc). Mann-Whitney U and Pearson χ2 testing was used to compare independent, between-group differences for scaled and prevalence measures, respectively. Unadjusted type I error probabilities (P values) were provided with both summary and variance measures, including means, SDs, 95% CIs for mean differences, medians, and interquartile ranges (IQRs) between independent groups. Due to the large number of independent outcomes evaluated simultaneously, which can result in higher false-positive rates, familywise error rates were controlled using the Benjamini-Hochberg stepwise correction procedure (q values) and a highly conservative false discovery rate (FDR) of 5.0% to control for possible false-positive increases. 23
Results
Final Study Population
A total of 48 mother/infant dyads met inclusion criteria and were recruited between August 2019 and March 2020 prior to randomization to either the surgical treatment arm (n = 24) or the observational treatment arm (n = 24) at the initial visit ( Figure 3 ). No adverse events or unanticipated problems were experienced during the study duration. All continuous measures were found to have non-Gaussian distribution. Bivariate comparisons of study dyad characteristics are described in Table 1 with no significant differences between treatment arms. Bivariate comparisons made of objective nFS measures are described in Table 2 , showing no significant differences between randomized treatment arms with the exception of number of sucks/event (P = .02) and burst duration (P = .04) prior to FDR adjustment. Bivariate comparisons of symptom-based outcomes ( Table 3 ) showed no statistical difference in any measure, with the exception of worse arching back symptom severity reported within the GSQ-I by the observational arm (P = .03), prior to FDR adjustment. Following analysis, 7 subjects in the control arm elected not to proceed with frenotomy ( Figure 3 ).
Comparisons of Infant/Mother Characteristics Between Treatment Arms at Enrollment/Initial Visit (Day 0). a
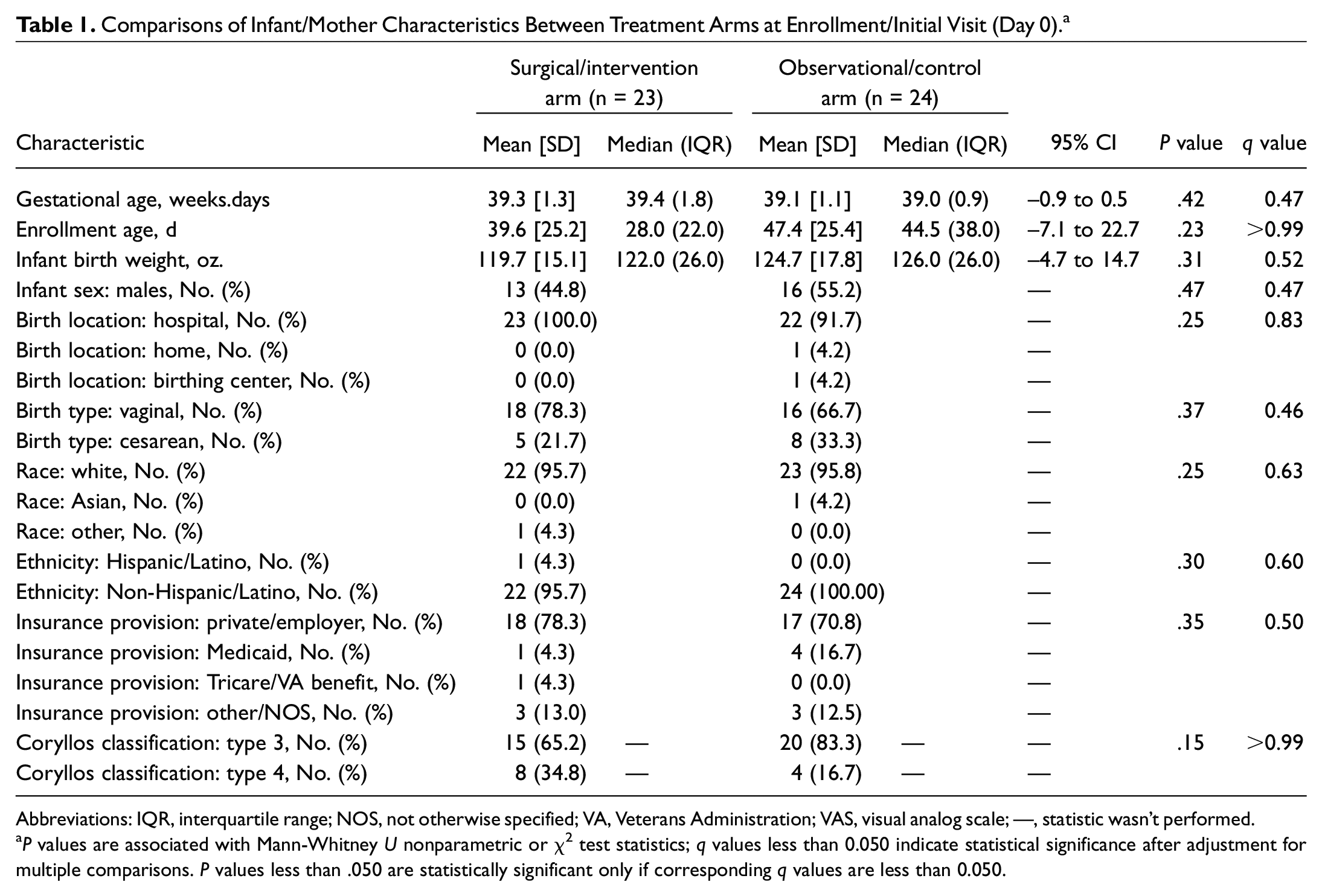
Abbreviations: IQR, interquartile range; NOS, not otherwise specified; VA, Veterans Administration; VAS, visual analog scale; —, statistic wasn’t performed.
P values are associated with Mann-Whitney U nonparametric or χ2 test statistics; q values less than 0.050 indicate statistical significance after adjustment for multiple comparisons. P values less than .050 are statistically significant only if corresponding q values are less than 0.050.
Comparisons of Bottle Measures Between Treatment Arms During Prefrenotomy Feeding (Stage 2). a
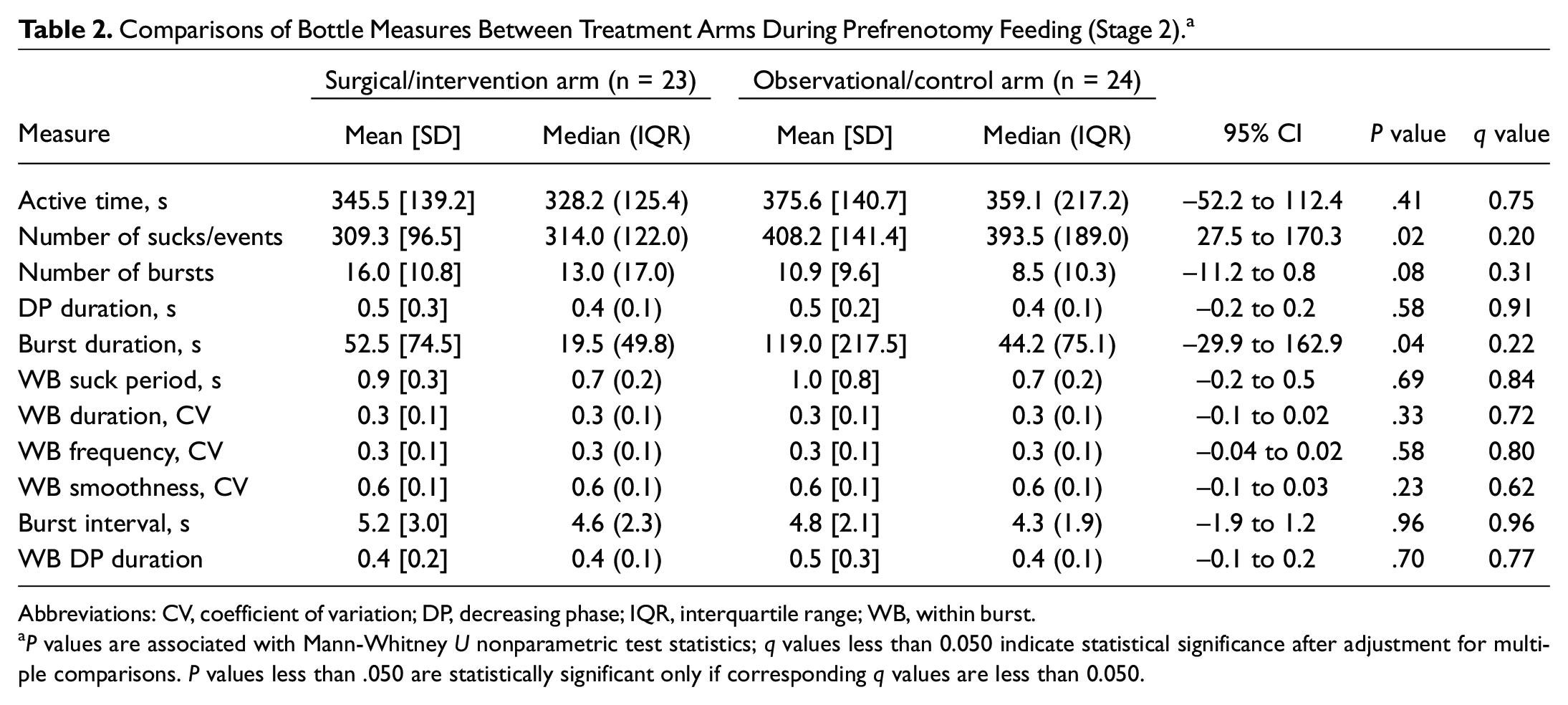
Abbreviations: CV, coefficient of variation; DP, decreasing phase; IQR, interquartile range; WB, within burst.
P values are associated with Mann-Whitney U nonparametric test statistics; q values less than 0.050 indicate statistical significance after adjustment for multiple comparisons. P values less than .050 are statistically significant only if corresponding q values are less than 0.050.
Comparisons of Infant/Mother Symptom-Based Outcome Measures Between Treatment Arms at Enrollment/Initial Visit (Day 0). a
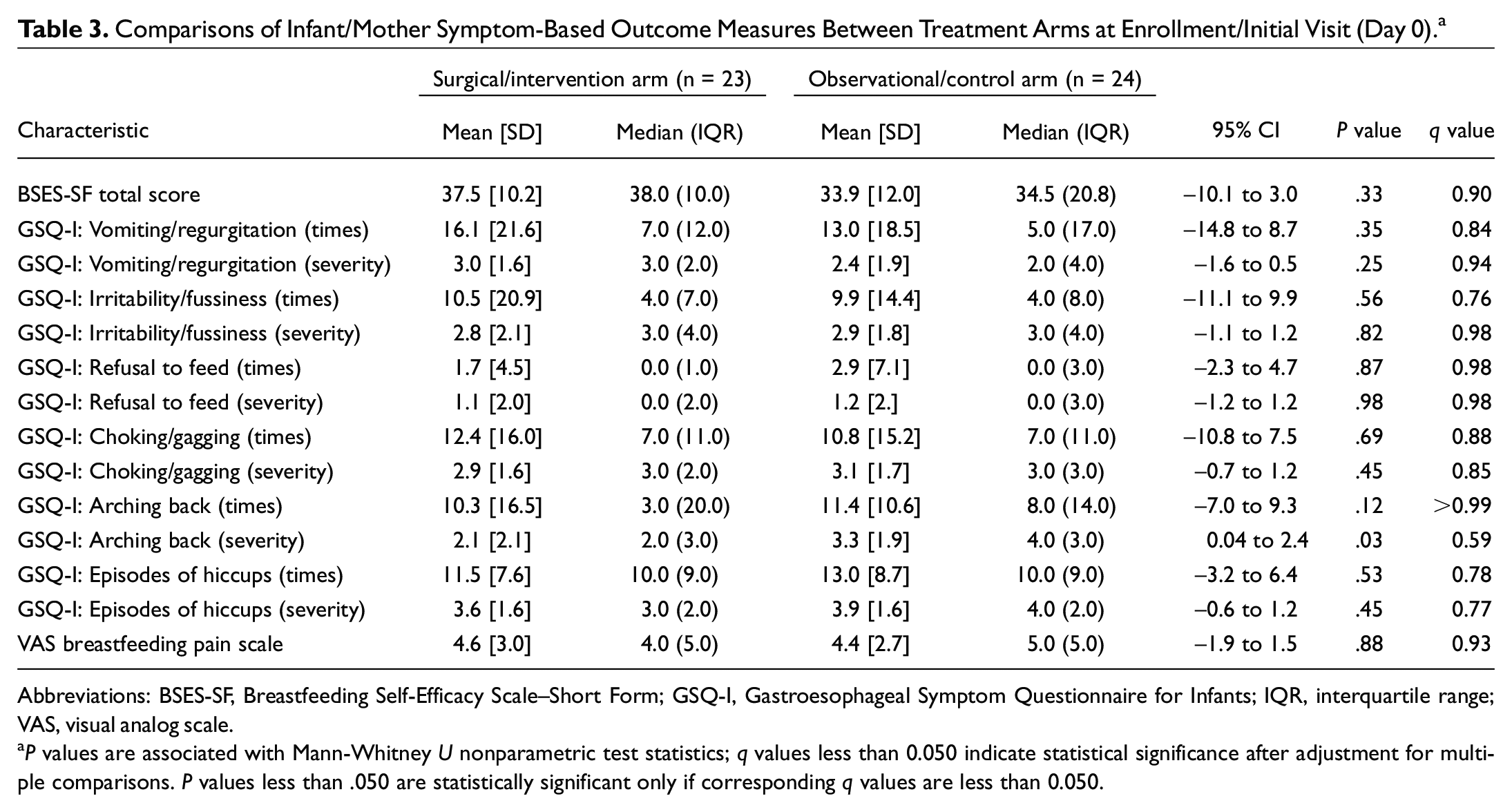
Abbreviations: BSES-SF, Breastfeeding Self-Efficacy Scale–Short Form; GSQ-I, Gastroesophageal Symptom Questionnaire for Infants; IQR, interquartile range; VAS, visual analog scale.
P values are associated with Mann-Whitney U nonparametric test statistics; q values less than 0.050 indicate statistical significance after adjustment for multiple comparisons. P values less than .050 are statistically significant only if corresponding q values are less than 0.050.

Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
Differences in Bottle-feeding Measures
Even after FDR adjustment, comparing treatment arms in the average magnitude of change identified significant differences in active time, number of sucks/events, number of bursts, decreasing phase (DP) duration (seconds), burst duration, within-burst (WB) suck period, WB duration (coefficient of variation [CV]), WB frequency (CV), WB smoothness (CV), burst intervals, and WB DP duration ( Table 4 ).
Between-Group Differences in Reported Improvement in Outcome Measures for Independent Treatment Arms Between Day 0 and Day 10 Clinical Evaluations. a
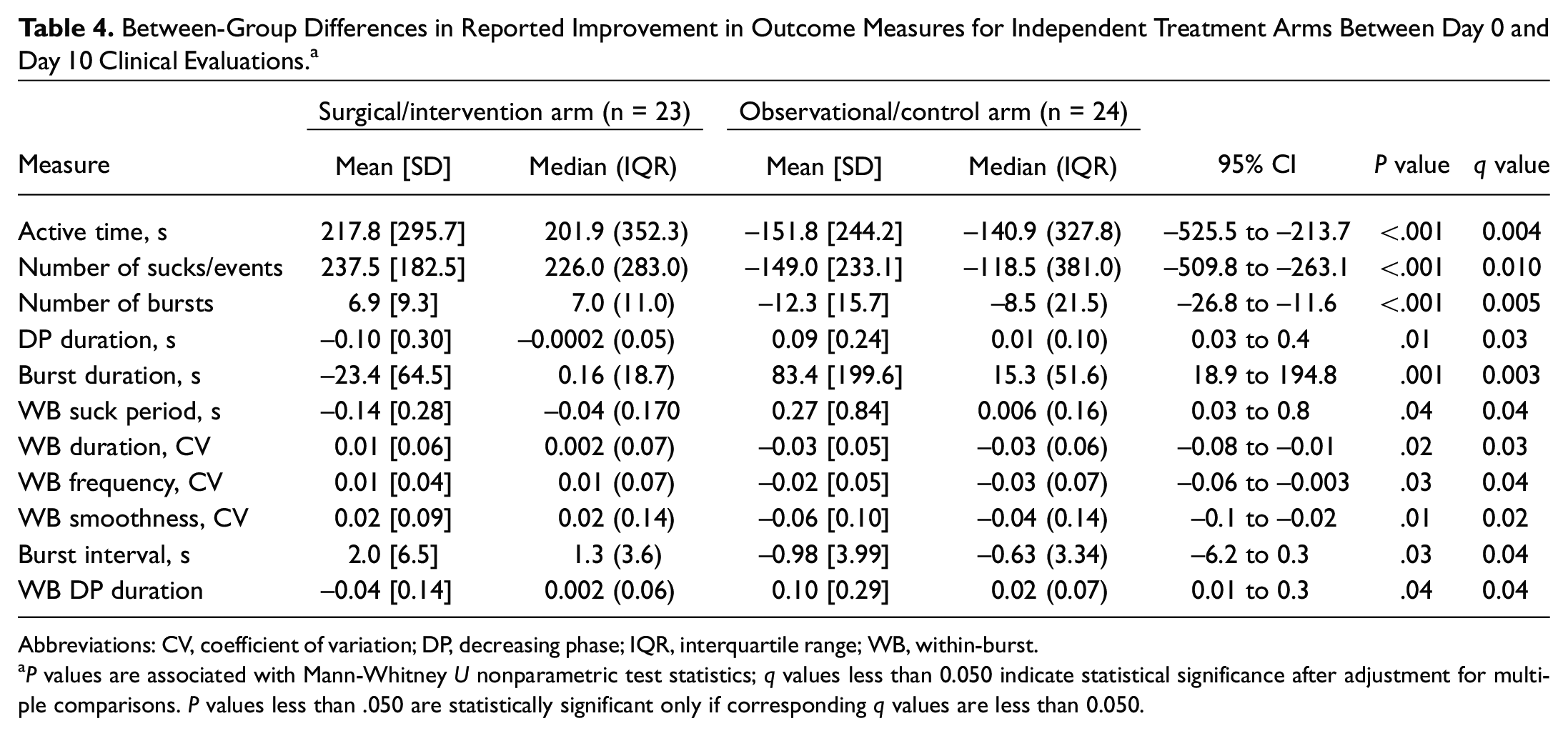
Abbreviations: CV, coefficient of variation; DP, decreasing phase; IQR, interquartile range; WB, within-burst.
P values are associated with Mann-Whitney U nonparametric test statistics; q values less than 0.050 indicate statistical significance after adjustment for multiple comparisons. P values less than .050 are statistically significant only if corresponding q values are less than 0.050.
Differences in Symptom-Based Outcome Measures
Comparing improvement between treatment groups ( Table 5 ) identified significant differences in the magnitude of change from enrollment at day 10 follow-up for BSES-SF total scores, the number of times infants experienced vomiting/regurgitation, refusal to feed, choking/gagging, arching back, and episodes of hiccups. Similarly, between-group comparisons identified significant differences at day 10 follow-up in the severity of vomiting/regurgitation, irritability/fussiness, refusal to feed, arching back, and hiccups. The between-group reduction in the VAS scale was also significantly better for study participants receiving frenotomy at day 10.
Between-Group Differences in Reported Improvement in Outcome Measures for Independent Treatment Arms Between Day 0 and Day 10 Clinical Evaluations. a
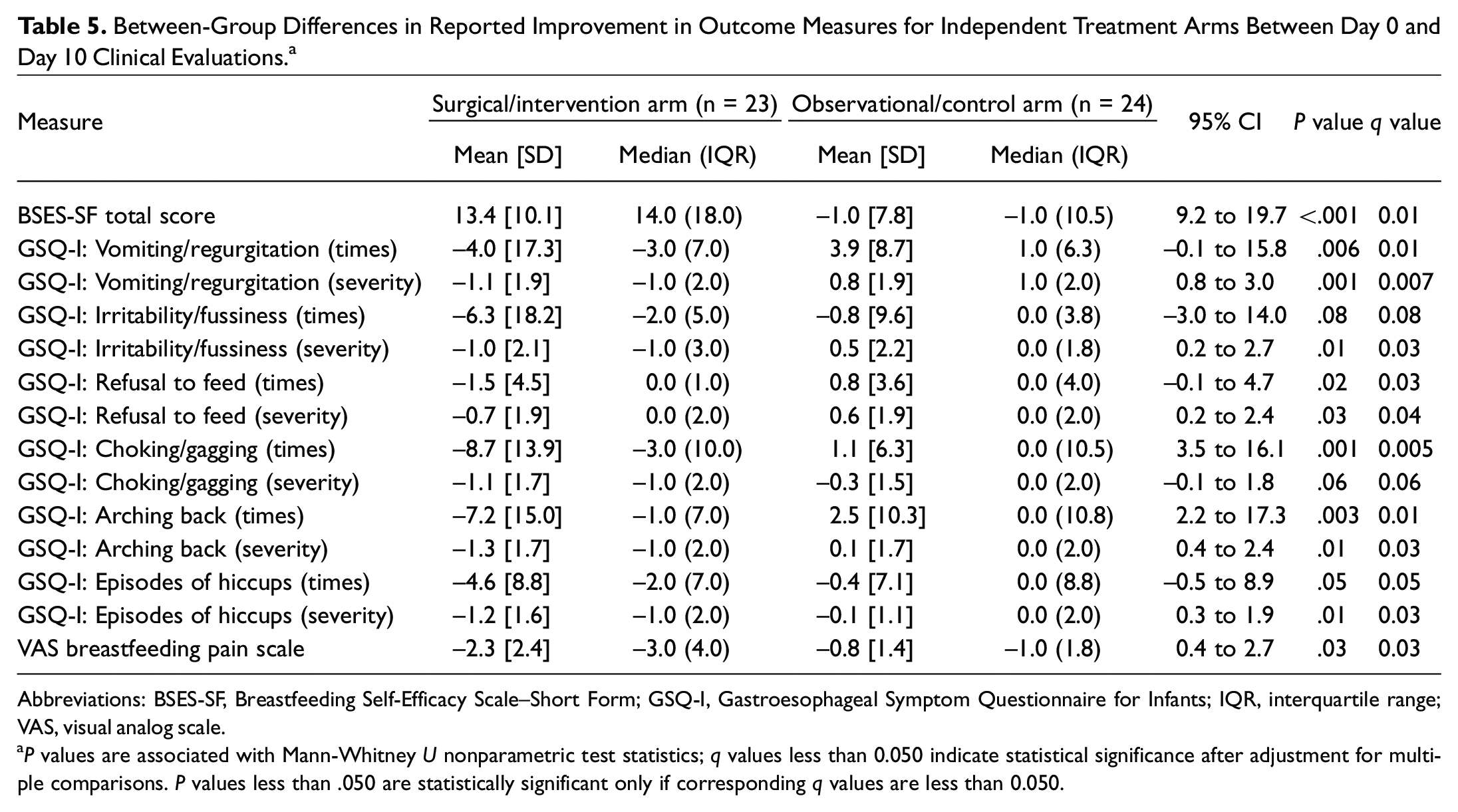
Abbreviations: BSES-SF, Breastfeeding Self-Efficacy Scale–Short Form; GSQ-I, Gastroesophageal Symptom Questionnaire for Infants; IQR, interquartile range; VAS, visual analog scale.
P values are associated with Mann-Whitney U nonparametric test statistics; q values less than 0.050 indicate statistical significance after adjustment for multiple comparisons. P values less than .050 are statistically significant only if corresponding q values are less than 0.050.
Discussion
As rates of breastfeeding continue to rise, medical practitioners increasingly need to provide care to support nursing. Prior to 2008, most practitioners felt that the tongue mechanically extracted milk via peristaltic waves. 24 Using submental breastfeeding ultrasound, researchers demonstrated the tongue movements needed for intraoral vacuum, primarily mid-tongue elevation toward the palate. 1 These findings were subsequently confirmed in a biomedical model. 2 Unfortunately, understanding of tongue physiology during breastfeeding and bottle-feeding has not been widely disseminated, leading to minimization of ankyloglossia as a contributing factor in feeding difficulties. Five RCTs have shown benefit to frenotomy, all of which focus on treatment of visible anterior tongue-tie.6-10 Other studies have demonstrated that treatment of PTT benefits breastfeeding dyads.11,12,25,26 Diagnosis of PTT remains difficult without appropriate evaluation of restriction of mid-tongue movement. 20 To date, there have been no RCTs studying PTT release or studies objectively measuring tongue function with frenotomy. The current study adds to the literature by addressing both.
The most pertinent results of this study lie with the data obtained from the nFS feeding system used to quantify tongue mechanics. For the first time, PTT release has been shown to objectively improve tongue function. These findings can be divided into 4 groups. First, the improvement in active feeding time, number of sucks/events, burst duration, burst interval, and number of bursts indicate that babies in the surgical group were more active in feeding. Fatigue is a common clinical finding in babies with PTT due to compensation for tongue restriction with the use of masticatory muscles. Release of the PTT improved feeding stamina by allowing the tongue to adopt normal vacuum through improved tongue suction generation, indicating a more rhythmic and orderly feeding pattern. Second, DP duration and within-burst DP duration were faster in the surgical group. These metrics measure the speed of the latter half of the suck cycle. These findings demonstrate that the tethered control group had persistently hindered sucking than those whose PTT was released. Commonly, infants with tongue-tie can spend prolonged time feeding with minimal transfer of milk, resulting in incomplete breast drainage. Our previous study demonstrated a 155% increase in feeding efficiency in babies following frenotomy, 11 and this study corroborates those findings by demonstrating that the tongue can move faster following release. Third, we found improvement in within-burst duration, frequency, and smoothness metrics. These measure the ability of the infant to adapt to changes in feeding conditions, and a higher coefficient of variation correlates with greater feeding skill. 18 Infants in the control arm had less variability (more rigid feeding patterns), demonstrating that PTT release allowed greater adaptation in feeding patterns. These data may explain why untied babies more easily adapt to changes in feeding routines (ie, switching between methods of feeding), changing anatomy (ie, eruption of teeth), and changes in milk flow. Finally, the within-burst suck period was faster in the surgical group. This demonstrates that within a burst of sucks, the infant was able to generate faster sucks if the tongue was released, providing objective evidence for the improved feeding efficiency reported by parents. Because it is the first of its kind, this study establishes the connection between surgical release of PTT and objective measures of tongue function. Combined, these findings set the framework for future comparative studies to further investigate the behavior of infants with PTT.
As was demonstrated in our previous studies, maternal reported outcomes were consistently better for infants who underwent frenotomy. Average breastfeeding self-confidence scores using the BSES-SF improved from 37.5 to 50.9 in the surgical group while slightly worsening in controls. A study by Nanishi et al 27 indicated that scores >50 predicted a better chance at continued breastfeeding, indicating BSES-SF score improvement in this study crossed a clinically relevant threshold.
Similar to our previous findings, this study demonstrated reduced frequency of reported reflux symptoms in the intervention group.11,12 We demonstrated that report of vomiting frequency and severity, irritability/fussiness, infant refusal to feed frequency and severity, choking/gagging, back arching frequency/severity, and frequency/severity of hiccups were all statistically better in the surgical group than controls. One proposed mechanism worsening reflux symptoms is aerophagia due to incomplete seal from impaired tongue movement, allowing air entry into the oral cavity. Mills et al 28 recently demonstrated the presence of oral and pharyngeal air using magnetic resonance imaging (MRI). Recent evidence suggests detrimental effects of indiscriminate use of antireflux medications. 29 Given the detrimental effect reflux symptoms have on both infants and family, these results suggest evaluation of tongue function as a treatment paradigm.
Finally, this study demonstrates treatment of PTT can result in a significant decrease in nipple pain (previous RCTs only studied anterior ankyloglossia). This result is corroborated by our previous study looking at a cohort of babies who were treated for anterior tongue-tie without releasing the posterior aspect of the restriction who continued to cause a similar degree of nipple pain; it was not until the PTT was released that pain resolved. 12
There are study limitations that warrant mention, the most important being limited sample size and inherent analytical restrictions that accompany smaller study populations. In addition, a short follow-up period may not allow for differences (spontaneous or treatment related) to be determined fully which could change with a longer observational period. The authors acknowledge that the randomization method chosen was not optimal and may have resulted in allocation bias. Another methodological concern involves the use of a convenience sample (instead of a consecutive or random sample), which limits the external validity of these results. Similarly, while statistical differences were identified, minimal clinically important differences have not been defined for either bottle-feeding metrics or symptom-based outcomes. While these exploratory metrics provide a basis for future study to enhance external validity, reported effect sizes may not be clinically discernible. For symptom-based outcome measures, procedural bias may exist. The presence of the wound that results from PTT release and the subsequent need for wound aftercare prevent parental blinding between the 2 arms of the study. As a result, parents may report improved outcomes to justify the pursuit of surgical intervention. Several factors limited additional study enrollment. As this study was not funded by research grant or industry support, the associated cost of the nFS limited enrollment. Additional sample size limitations included parental refusal in participating in an RCT and the inherent risk of randomization to the control arm given feeding difficulties. Furthermore, there are inherent problems with a crossover design for the observational group: patient dropout, lack of randomization of that arm, and potential carryover effect from nonsurgical treatments while waiting for surgical intervention. 30 While all 24 control subjects were included in the between-group analysis, data for the 17 subjects who did subsequently cross over were not incorporated into this investigation and will be the focus of additional study (crossover data for the 7 who did not proceed with frenotomy were unable to be recorded). Because the groups were compared at day 10, the authors acknowledge the possibility that clinical improvement could have occurred afterward without surgical intervention or that improvement seen in the surgical group could have regressed afterwards. In addition, following the infants for 30 days without treatment may have resolved the concerns, although other studies indicate a higher likelihood of breastfeeding termination when frenotomy is delayed.31-33 The global coronavirus disease 2019 pandemic further limited enrollment and study continuation.
Conclusion
This randomized, controlled study demonstrates that PTT release improves both patient-reported outcome measures and objective infant feeding parameters 10 days after frenotomy. Improvement in breastfeeding self-confidence, infant reflux symptoms, and maternal nipple pain reflect an improvement in breastfeeding quality following PTT release. Our demonstration of physical improvement in sucking metrics using an objective tool definitively demonstrates that PTT is a valid clinical entity that warrants medical attention when feeding difficulties are present.
Footnotes
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.