
Abstract
Objective
To evaluate outcomes following salvage microsurgery (MS) and salvage stereotactic radiosurgery (SRS) after failure of primary treatment for vestibular schwannomas (VS).
Study Design
Retrospective chart review.
Setting
Tertiary referral center.
Methods
Patients with more than 1 intervention for their VS were divided into 4 groups: MS followed by SRS (n = 61), MS followed by MS (n = 9), SRS followed by MS (n = 7), and SRS followed by SRS (n = 7), and outcomes were evaluated.
Results
A total of 77 patients were included (84 procedures). In group 1 (MS then SRS), 3% developed a decline in facial function, 3% developed trigeminal sensory loss, and 13% patients had gradual improvement of facial nerve function following SRS. Group 2 (MS then MS) had the highest rates of facial nerve deterioration, although all but 1 patient achieved a House-Brackmann score of II or III. Gross-total resection (GTR) was achieved in 56% of patients. When a different approach was used for salvage resection, GTR occurred more commonly, and facial nerve outcomes were similar. In group 3 (SRS then MS), GTR occurred in 43% of cases, and 2 of 7 patients developed worsened facial function. In group 4 (SRS then SRS), no patient developed facial weakness after reirradiation, and 1 developed a trigeminal nerve deficit.
Conclusions
For MS recurrences/residuals, SRS is the mainstay of treatment and does not preclude facial function recovery. If salvage microsurgery is required, an alternate approach should be considered. For SRS failures, when MS is required, less-than GTR may be preferable, and reirradiation is a potential safe alternative.
The current management of vestibular schwannomas (VS) includes observation, microsurgery (MS), and stereotactic radiosurgery (SRS). While most often, the 2 latter modalities offer definitive tumor control, both approaches have the potential for treatment failures. Recurrent disease after total microsurgical resection of VS is rare.1-3 Recurrences are most often found along the facial nerve, on the cochlear or vestibular nerves when preserved, or in the fundus of the internal auditory canal. Although many neurotologists and neurosurgeons will advocate for gross total resection (GTR) of VS, this is not always pursued given the benign nature of the pathology. Less-than-total tumor resection may be used when there is a significant risk of injury to neural structures. In fact, planned subtotal resection with or without subsequent SRS is a known concept, especially in cases in which the facial nerve would otherwise be at high risk of injury.4-10 In cases of recurrent and residual disease, treatment options include observation, revision surgery, and radiosurgery.
SRS has been used for the past 40 years in the management of VS, has excellent tumor control rates, and avoids potential for catastrophic risks inherent to skull base surgery. SRS may be considered as a primary modality in certain patient groups, including the elderly, those unfit for surgery, and commonly for small- to medium-sized tumors depending on patient preference. Nonetheless, failures after radiosurgery may also occur.
The goal of the current study is to review our experience with failure of primary interventions for VS, with an emphasis on the time interval between treatments, functional outcomes, and complications.
Methods
A retrospective review was performed of patients who required more than 1 treatment intervention for a single VS between January 2011 and June 2020. Patients with at least 1 follow-up imaging study after the second intervention (either MS or irradiation) were included, and patients with neurofibromatosis type 2 were excluded. Next, patients were divided into 4 groups: (1) MS followed by SRS, (2) MS followed by MS, (3) SRS followed by MS, and (4) SRS followed by SRS. We decided to include the MS followed by SRS group even if, often, residual disease was left intentionally. Although the term failure may not be entirely accurate for such patients, this is an increasingly important group to consider. If a patient underwent more than 2 interventions, each additional intervention was assessed individually.
Collected information included age at diagnosis, tumor size (largest diameter measured in the cerebellopontine angle along the axis of the tumor), and all treatments for the VS. Facial nerve outcomes were recorded using House-Brackmann (HB) grade. Additional symptoms, such as facial numbness and facial twitching, were also recorded. For salvage MS, surgical approach and intraoperative and postoperative complications were noted. For salvage or adjuvant radiosurgery, dosage and complications were recorded. All patients were treated with Gamma Knife, at a uniform margin dose between 12 and 13 Gy.
Statistical analysis was performed using Microsoft Excel. Descriptive statistics of continuous variables are reported in mean, median, and range. When applicable, a Student t test and Pearson chi-square test was used. Statistical significance was defined as P < .05. The study protocol was approved by the Institutional Review Board of NYU Langone Health (protocol numbers 20-01790).
Results
A total of 77 patients were included in our analysis. Six individuals had more than 1 additional intervention, and each of these was evaluated separately, resulting in a total of 84 procedures. Patients undergoing primary surgical resection first were younger than patients undergoing radiosurgery (mean age of 50.3 vs 63.2 years, P < .001). Tumors were larger in patients undergoing primary MS compared with primary SRS (median 31 mm vs 21 mm, P < .001). A summary of patient demographics can be found in Table 1 .
Demographic Information.
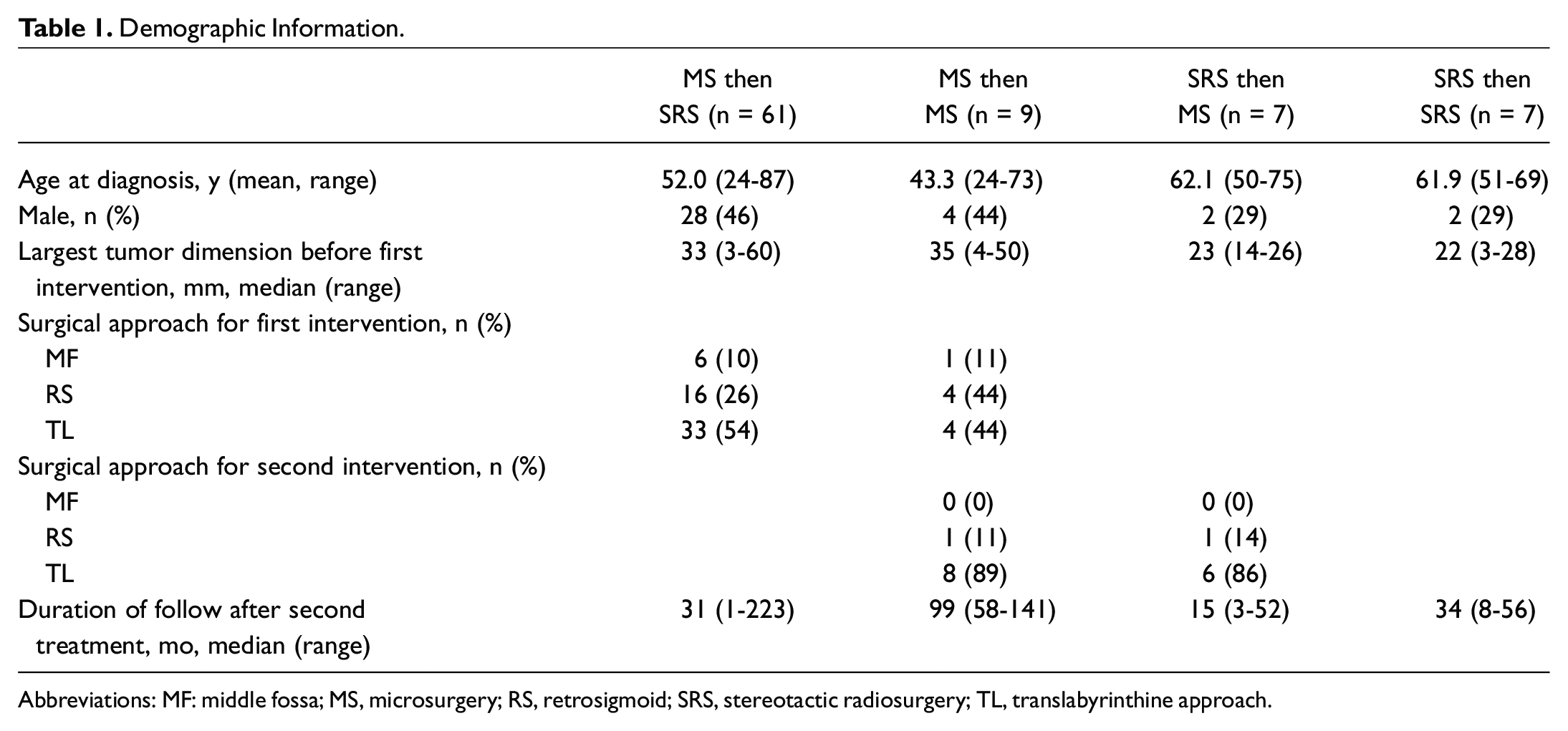
Abbreviations: MF: middle fossa; MS, microsurgery; RS, retrosigmoid; SRS, stereotactic radiosurgery; TL, translabyrinthine approach.
MS Followed by SRS
A total of 61 patients underwent MS followed by SRS. Initial surgical approaches included translabyrinthine craniotomy in 54% of patients, retrosigmoid (RS) in 26% of patients, and middle cranial fossa (MF) in 10% of patients. In this group, the median interval between MS and SRS was 34 months (mean 61.8 months), and the median duration of follow-up after the second intervention was 31 months.
In terms of functional outcomes, only 2 patients (3%) had a deterioration of their facial nerve function after SRS (from HB grade 1 to 4 in a 91-year-old man with a recurrent 6.4-mL tumor who is now 98 years old, and HB grade 2 to 3 in another patient). This deterioration occurred at 6 and 2 months after SRS, respectively. Eight patients (13%) had improvement of their postoperative facial function during the follow-up period. In addition, 2 patients developed facial spasms following SRS, and 2 patients developed new subjective trigeminal nerve deficits (numbness, reported as not bothersome). Among the patients who underwent either an MF or RS approach to resection, hearing was preserved in 10 of 16 patients who were hearing-preservation candidates. However, after SRS, only 3 patients had any residual hearing (and only 1 had a word recognition score greater than 50%). There were no other associated complications recorded (see Table 2 ).
Summary of Outcomes per Group After Second Intervention.
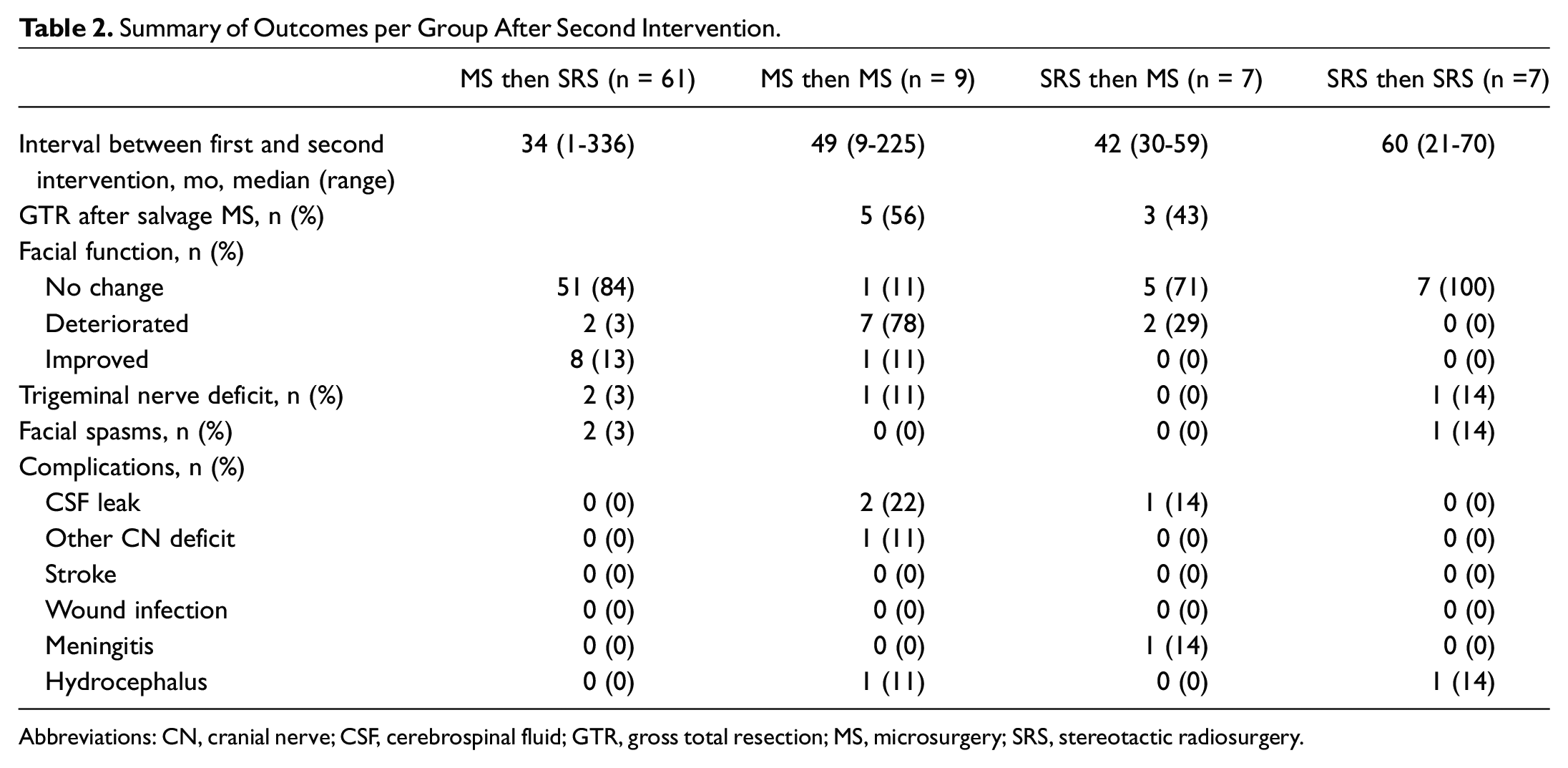
Abbreviations: CN, cranial nerve; CSF, cerebrospinal fluid; GTR, gross total resection; MS, microsurgery; SRS, stereotactic radiosurgery.
This group was further divided into 3 subgroups: (1) patients with recurrent tumor after GTR, (2) patients with residual tumor with an intent to observe, and (3) patients with residual tumor and intent to undergo postoperative SRS. Patients were classified as having recurrent tumor when their initial postoperative magnetic resonance images (MRIs) revealed no residual disease. Patients with residual tumor and intent to observe were those in whom a decision was made to leave residual tumor of any size behind for different reasons (adherent to facial nerve, bleeding) but in whom the initial plan was to observe the behavior of the residual. Finally, patients classified as residual tumor with intent to undergo postoperative SRS were those in whom SRS was either discussed preoperatively or immediately postoperatively. This information was extracted from progress notes. In cases of residual disease in which the intent was to observe initially, the median interval between MS and SRS was 50 months. When the intent was to treat, the median time interval was 6 months. In cases of recurrence, the median interval between MS and SRS was 113 months. When comparing patients with intent to observe to those with an intent for SRS for residual, age and maximum residual dimension were not significantly different between groups (P = .24 and P = .06, respectively). Maximal tumor dimension prior to primary surgery was different between groups (P = .013), with larger tumors being more likely to undergo planned postoperative SRS. Within the group treated intentionally postoperatively, there were 3 cases of improved facial nerve function and no cases of deterioration. The differences between patients can be found in Table 3 .
Characteristics of Patients Who Underwent MS Followed by SRS.
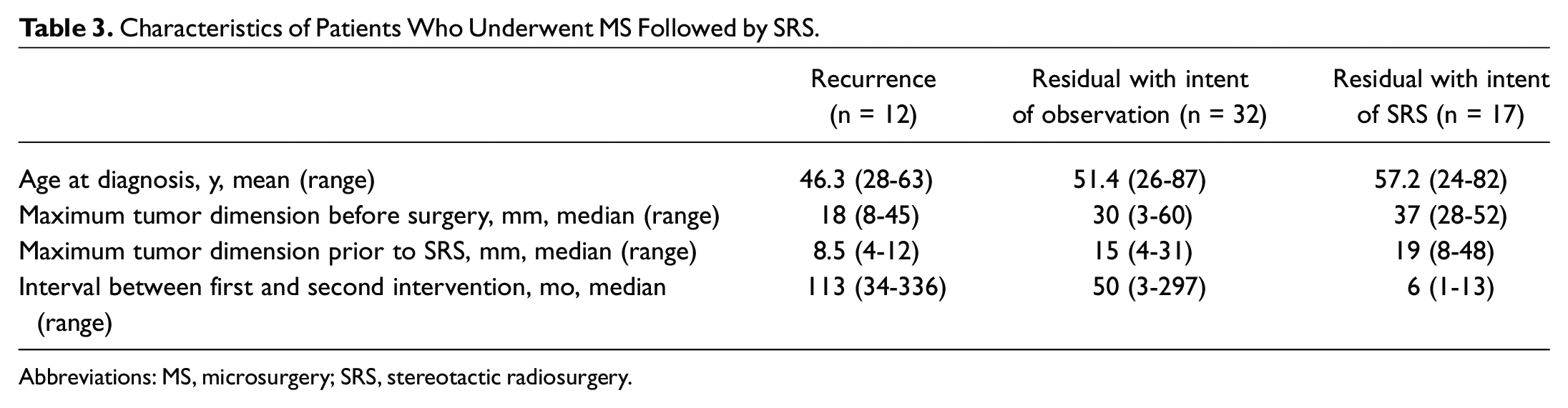
Abbreviations: MS, microsurgery; SRS, stereotactic radiosurgery.
MS Followed by MS
A total of 9 patients underwent MS followed by MS, with a mean age of 43.3 years at diagnosis. This group was the youngest in the cohort. The median interval between resections was 49 months (mean 69.7 months), and the median duration of follow-up in this group was 99 months. Of note, the median largest dimension before the second intervention in this group was 25 mm, compared with 15 mm for the patients in the MS followed by SRS (with intent to observe) group.
At the time of revision surgery, GTR was achieved in 5 of 9 patients. Facial nerve function deteriorated from baseline in 7 of 9 patients. Specifically, 2 patients worsened from HB grade 1 to 2, 4 patients from HB grade 1 to 3, and finally 1 patient went from HB grade 2 to 6 (see Table 4 ).
Specifics of Facial Nerve Deterioration.
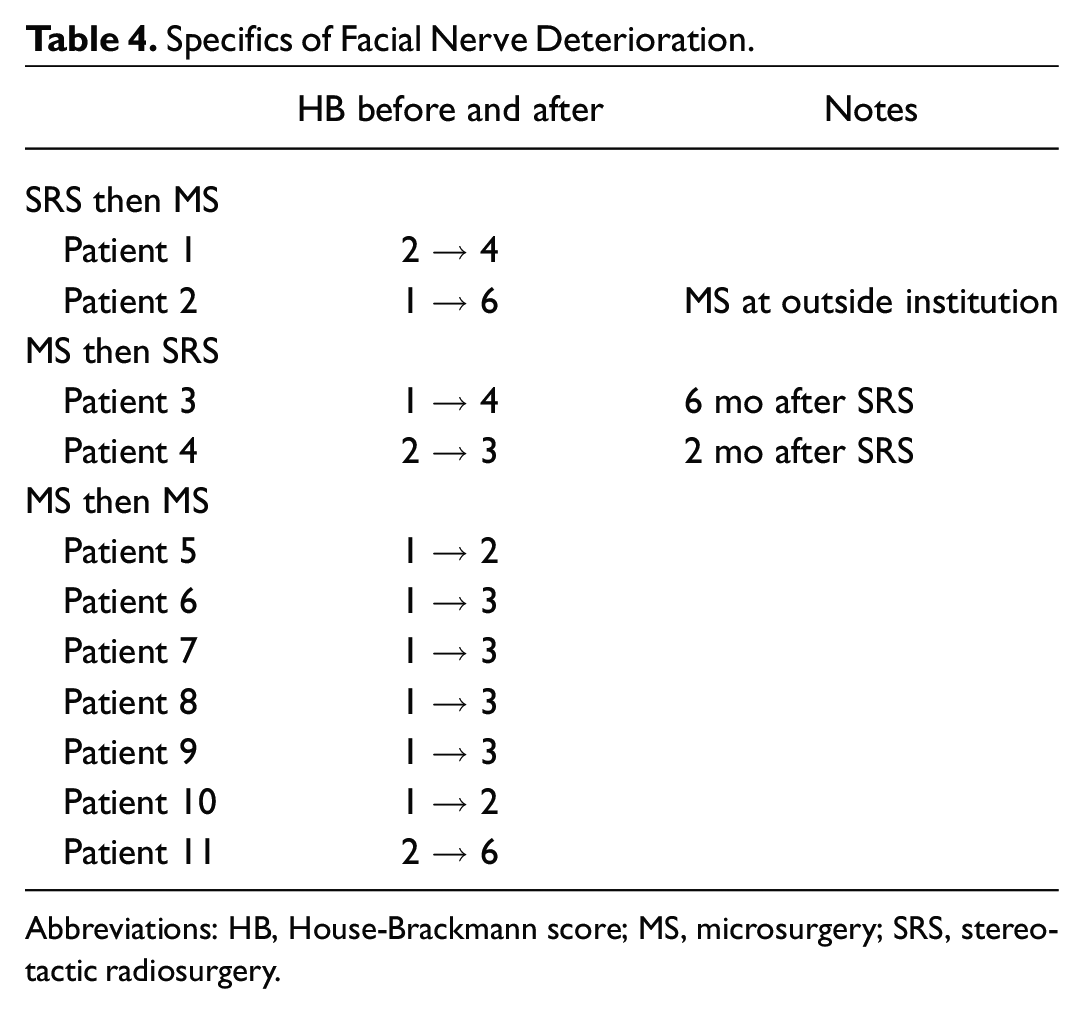
Abbreviations: HB, House-Brackmann score; MS, microsurgery; SRS, stereotactic radiosurgery.
Within this group, we compared the 5 patients who underwent the same approach to the 4 patients who underwent a different approach. Although too small to perform a statistical analysis, there were 2 postoperative cerebrospinal fluid (CSF) leaks in the group who underwent the same approach, compared with none in the group who underwent a different approach. Facial nerve outcomes were similar between groups (see Table 5 ).
MS Followed by MS: Outcomes With Same Versus Different Surgical Approach.
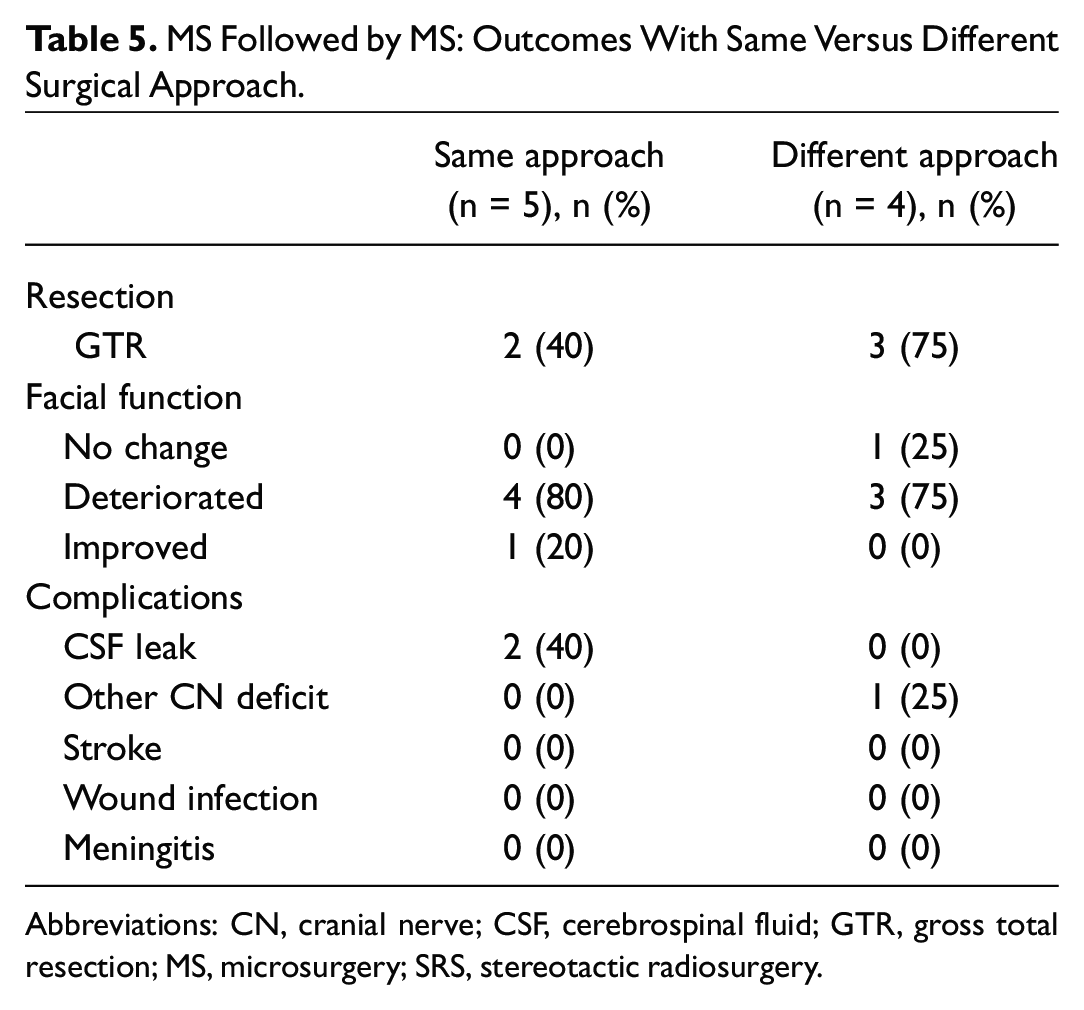
Abbreviations: CN, cranial nerve; CSF, cerebrospinal fluid; GTR, gross total resection; MS, microsurgery; SRS, stereotactic radiosurgery.
SRS Followed by MS
A total of 7 patients underwent SRS followed by MS. The median interval between interventions was 42 months (mean 41.4 months). For most patients, the decision to undergo MS was made in the context of progressive tumor growth over the course of several years. Four of 7 patients noted facial numbness in the context of tumor growth, and 1 had facial spasms.
At the time of revision surgery, 6 patients underwent a translabyrinthine approach and 1 an RS approach. GTR was achieved in 3 patients (43%). In the operative reports reviewed, salvage MS was described as more difficult than usual, with lack of the normal tissue planes or “sticky” planes. Nonetheless, only 2 of 7 patients had a deterioration of their facial nerve function. The first patient went from HB grade 2 to grade 4, and the other had a HB grade of 6. There were no reports of trigeminal nerve deficits or facial spasms. In the patient who had facial spasms prior to surgery, these resolved postoperatively. One patient had a postoperative CSF leak.
SRS Followed by SRS
A total of 7 patients underwent SRS twice in the context of tumor growth. The largest tumor dimension (median) prior to the first intervention was 22 mm (range 3-28 mm). The median interval between interventions was 60 months (mean 49.8 months). The median duration of follow-up was 34 months. The margin dose of the second SRS was between 10 and 12 Gy.
No patient in this group developed facial weakness. One patient developed a new trigeminal nerve deficit (sensory), and 1 patient reported intermittent facial spams (treated with Botox). Only 1 patient continues to have serviceable hearing. Furthermore, 1 patient developed hydrocephalus after the second dose of SRS, which required ventriculo-peritoneal shunt placement. He presented with worsening headaches 10 months after the second dose of SRS, and the diagnosis was made.
A total of 6 patients required more than 2 interventions: 5 patients underwent 3 interventions, and 1 underwent 4 interventions over a 20-year period. No patient had malignant pathology. The median duration of follow-up in this group since the last intervention is 32.5 months (range 15-65 months).
Discussion
The current study reviewed our institutional experience with salvage resection and radiosurgery following failed primary treatment for VS. In general, tumor control rates from both primary MS and SRS are excellent. 11 However, both modalities have the potential for treatment failures, and second procedures of any kind present unique challenges.
Failures After Surgery
Recurrent disease after MS complete resection is rare.1-3 It can occur as late as 10 or more years following resection 12 and is the reason why prolonged surveillance is encouraged. Monitoring is also required for residual disease, whether left behind intentionally or not. Less-than-total tumor resection may be used when there is a significant risk of injury to neural structures and has been encouraged by several groups,4-10 including our own. We attempted to identify factors that would encourage immediate SRS versus observation for residual tumor and noted that younger age was not a factor, nor was size of residual. However, when reviewing the progress notes, rapid tumor enlargement prior to initial surgery seemed to drive decision making, as did preoperative tumor size. In general, we observe the residual tumor when possible, which allows for tumor collapse to its most compact volume and for additional tumor death. It also allows for facial or other cranial nerve recovery, although we do not consider facial paresis a contraindication for SRS.
Reports of SRS after resection have revealed excellent tumor control rates, in the range of approximately 95%. 13 A recent systematic review demonstrated that tumor control rates after surgery and subsequent SRS were 93.9%, with low associated morbidity. 14 Facial weakness following adjuvant SRS is rare. In older outcomes from the late 1980s, in which higher doses of radiation were used, rates of facial nerve function deterioration after SRS and previous surgery were as high as 23%. 15 However, with current SRS doses, used since the mid-1990s, new facial weakness is extremely uncommon. Brokinkel et al 16 reviewed 6 studies of MS followed by SRS comprising a total of 159 patients. They found that 82.8% of patients maintained a facial function of HB 1 to 2 after surgery, which subsequently stayed stable in 94% of those patients after SRS. Furthermore, 17 patients showed progressive recovery of facial nerve function as compared with the immediate postoperative period, suggesting that SRS does not preclude the expected recovery of facial paresis in the context of an intact nerve. This was confirmed in our patient series. Even in cases of macrocystic regrowth, we still consider SRS, as in our experience, cystic tumors respond even better to SRS.
Revision surgery is a feasible option for both recurrent and residual VS, although SRS is the most employed approach. It may be necessary if there is compression of the brainstem or in patients who strongly prefer surgery. Another indication for revision MS is intractable trigeminal neuralgia, which may improve after nerve decompression. In revision surgery, we will always look for evidence of vascular compression. In our cohort, patients who underwent repeat surgery rather than SRS were younger, more symptomatic, and had larger tumors at the time of consideration of second intervention. Most patients did recover to HB grades of 2 or 3. In terms of surgical approach, there is no consensus on the best approach for repeat MS. Some groups will advocate using the same approach, 17 whereas others suggest that an alternate approach may allow dissection in healthy tissue devoid of scarring.18,19 Although our patient numbers were too small to perform meaningful statistical analysis, we favor a different approach for revision MS, to enter an untouched surgical field and avoid scarred tissue planes related to previous surgery.
Failures After Irradiation
SRS is known for high rates of tumor control. Overall, the need for further intervention following GKS in particular is approximately 3% to 5%. 20 However, given the increasing number of tumors treated with SRS, a certain number of failures do occur and can be addressed with resection or reirradiation.
It is important not to confuse treatment failure with the known tumor expansion that occurs initially after SRS. Nagano et al 21 described a transient expansion in as many as 75% of patients. It is believed that an initial volume increase is a common phenomenon and will usually be followed by regression as time passes. 21 Neurological deficits are not always consequences of tumor growth but may be a result of the radiation itself. These types of injuries may occur anywhere from 3 to 24 months after SRS. During this time, rather than resorting to salvage surgery, a course of corticosteroids is recommended. Radiation-induced neuropathies are thought to resolve within 3 to 12 months in more than half of cases. 20 Intervention following SRS should occur only if there is sustained tumor growth on serial imaging, usually 2 or more MRIs or if a patient is symptomatic from mass effect. In our patients, the median duration between interventions was 42 months, and sustained growth was noted on several interval MRIs.
Centers who treat large volumes of VS will often report that salvage resection after SRS tends to be more difficult.20,22,23 However, these data are inconsistent. Wise et al 22 reviewed 37 patients who underwent salvage MS after SRS. At long-term follow-up, they found that 73% of patients had grade 1 or 2 HB scores. Overall, they concluded that to preserve facial function and prevent other complications, either near-total or subtotal resection was advisable. Our cohort consisted only of 7 patients, and GTR was achieved in 3 of the patients, which was intentional for the reasons outlined above. Less than GTR should be considered if necessary to preserve facial nerve function. This may involve simply leaving a small rim of the tumor on the facial nerve. However, certain situations may require a more aggressive approach, depending on the patient’s age, rate of regrowth, and tumor size.
Salvage SRS after previous treatment remains an option for a tumor that progresses after initial SRS. Although the number of patients reported in the current literature is small, the current evidence suggests high efficacy and low levels of toxicity. Most groups will advocate for waiting a minimum of 2 to 3 years before a treatment failure is confirmed, and this was the case in our cohort. Following this, the decision must be made between salvage MS and reirradiation. If there is any clinical or radiologic evidence of brainstem compression, MS is the preferred approach, if feasible. Patient age, comorbidities, and individual preferences may also play into the decision-making process. At the present time, there are 7 reports of reirradiation for VS management, comprising a total of 126 patients.24-30 The median marginal radiation dose for retreatment was between 11.5 and 13 Gy and was quite uniform across studies. Among our patients who underwent repeat SRS, none have required additional intervention after a median follow-up time of 34 months. No patient has worsened facial nerve function, although 1 patient developed facial spasms and 1 developed a new trigeminal nerve deficit after their second SRS. Much remains to be discovered regarding repeating SRS.
Limitations
One limitation in this study is that hearing outcomes are not reported in all groups. We did not put an emphasis on this information because more than half the cohort underwent a translabyrinthine approach to resection, either primarily or during salvage and because often, in a salvage situation, hearing outcomes are not necessarily part of the goals of care.
Conclusion
Management of VS is complex, and both MS and SRS have the potential for treatment failures. SRS may be considered following MS, especially in the context of tumor residual to ensure preservation of facial nerve function. Facial nerve outcomes are excellent, and SRS does not preclude recovery of postoperative weakness. Salvage MS following previous MS and SRS is an option, although it can be surgically challenging and is usually reserved for symptomatic patients with rapidly growing tumors. Finally, repeat SRS carries a low adverse event profile, although long-term follow-up is required. It should be considered in smaller tumors that are growing but asymptomatic.