
Abstract
Objective
To evaluate the predictive utility of the Hospital Frailty Risk Score (HFRS), a stratification tool based on the ICD-10 (International Classification of Disease, Tenth Revision), and other risk factors for 30-day readmissions and mortality in a nationally representative cohort.
Study Design
Retrospective database review.
Setting
Nationwide Readmissions Database (2017).
Methods
Patients with head and neck cancer who underwent major surgical procedures were identified from the 2017 Nationwide Readmissions Database, representing 116 medical centers nationwide. Bivariate and multivariable logistic regression methods were used to identify factors associated with unplanned 30-day readmission, 30-day readmission mortality, and increased length of hospital stay.
Results
A total of 14,420 patients underwent major head and neck cancer surgery. Unplanned readmission occurred in 11% of patients. The most common reasons for unplanned readmission were procedural complications (26.5%), sepsis (7.3%), and respiratory failure (3.9%). Elevated frailty index (HFRS ≥5) was identified in 22% of patients. Frailty was associated with higher 30-day readmission rates (18.0% vs 9.5%, P < .01), which held on multivariate modeling (odds ratio [OR], 1.59 [95% CI, 1.37-1.85]). Frail patients spent more days in the hospital (8.2 vs 6.8, P = .02) and incurred more charges across hospital stays ($275,000 vs $188,000, P < .01). Patients >75 years old (OR, 1.26 [1.03-1.55]) and patients with electrolyte abnormalities (OR, 1.25 [1.07-1.46] were significantly more likely to be readmitted.
Conclusion
In this head and neck cancer surgical population, HFRS significantly predicted unplanned readmission. HFRS is a potential risk stratification tool and should be compared with other methods and explored in other cancer populations. Beyond the challenge of identifying at-risk patients, future work should explore potential interventions aimed at mitigating readmission.
Unplanned hospital readmissions represent a significant economic burden, with Medicare costs totaling nearly $15 billion annually for this expense alone.1,2 Emphasis on efficiency of health care delivery and increased quality improvement interventions have called attention to minimize this annual cost.
In head and neck cancer surgery in particular, the associated morbidity of the underlying procedure can result in higher rates of postoperative complications in comparison with other surgical procedures. While economic costs are important, patient health and outcomes are paramount; therefore, a considerable push to identify high-risk patients exists. Such risk stratification can help inform clinicians of patients who require more intense preoperative risk profile optimization and addressing of existing comorbidities. We sought to evaluate the predictive utility of elevated frailty index on readmissions secondary to head and neck procedures, as determined by the Hospital Frailty Risk Score (HFRS), a stratification tool based on the ICD-10 (International Classification of Disease, Tenth Revision). 3
Prior literature examining rates of readmission in otolaryngology found that patient-specific factors drive most variability in readmission incidence, with wound complications and comorbidities specifically increasing such incidence.4-10 While ample attention has been focused on identifying and associating patient-level comorbidity factors, less attention has been focused on the more holistic patient picture and, correspondingly, the role of frailty in head and neck procedure–related readmissions and outcomes. Frailty, classically associated with age, represents a state of the body in which there exists a decreased physiologic reserve and capacity to respond to stressors (eg, major surgery).11-13 However, because no standardized definition for frailty exists, studying it can be challenging. Recent work has characterized the role of frailty by proxy of several frailty indices and found varying associations between frailty and mortality, in-hospital death, length of stay, and readmission rates.11,14 A relationship appears to exist between frailty and such outcomes; however, further research is needed to better characterize the exact nature of this association. Herein, we conducted a study to investigate the role of an elevated frailty index and other risk factors on incidence of short-term readmissions, economic costs, and causes of readmission in a nationally representative subset of patients with head and neck cancer.
Methods and Materials
Data Source and Study Population
The Nationwide Readmissions Database (NRD) is a nationally representative longitudinal database developed and maintained by the Healthcare Cost and Utilization Project, a joint project among federal, state, and industry stakeholders and sponsored by the Agency for Healthcare Research and Quality. 15 The database covers 59.7% of all inpatient admissions in the United States, capturing demographic, clinical, and nonclinical variables from various community, public, and academic medical centers across 28 state inpatient databases. Patient- and hospital-level variables included age, sex, income quartile, insurance type, urban vs rural location, state residency, hospital ownership, hospital bed size, and hospital teaching status. Reason for readmission was defined by the associated primary ICD-10 diagnosis code at the time of rehospitalization. Primary outcomes in this study were 30-day readmission rate, with secondary outcomes of interest being 30-day mortality, reasons for readmission, costs of total hospitalizations, length of hospitalization stay, and patient/hospital-level risk factors for readmission. Reasons for readmission were determined according to the first listed ICD-10 code for associated diagnosis. This study was deemed exempt from the University of California–San Diego Institutional Review Board, as the NRD is publicly available with deidentified patient information.
All adults (age ≥18 years) who were alive at the time of discharge and had valid length of stays between January and November 2017 were included in the study. Patients were identified first as having a head and neck–related oncologic diagnosis via ICD-10 diagnosis codes and second as having a major head and neck procedure via ICD-10 Procedure Coding System codes (Supplemental Table S1, available online). Only unplanned readmissions were considered events of interest per a corresponding indicator variable present in the database. Patients had unique identifiers that allowed tracking across different hospitals within the same state by utilizing state inpatient databases, although cross-state itinerant patients could not be assigned the same unique identifier.
A patient’s frailty status was determined at the time of hospitalization for the procedure per the ICD-10 codes. Each patient’s frailty risk score was calculated and used for placement into a low-risk group (score <5) or a high-risk group (score ≥5) with appropriate score assignments per Gilbert et al 3 (Supplementary Table S2, available online).
Statistical Analysis
Baseline demographic and clinical characteristics were compared with Pearson’s chi-square test and Student’s t test for categorical and continuous variables, respectively. Our unit of observation was any patient index event, defined as any valid admission where the patient primarily underwent a major head and neck procedure and was discharged alive. Cumulative incidence functions were used to represent rates of readmission and mortality within 30 days of index admission. For readmission, patients were censored if they had a planned readmission, and for mortality, patients were censored if they had any readmission event and were discharged alive. Multivariable logistic mixed effect regression models were used to assess the association between covariables of interest and our primary study endpoint of readmission following initial hospitalization. This approach allowed us to account for clustering of patients within hospital facilities as well as repeated admissions within a single patient. Negative binomial multivariable regression was used to model length of stay as an outcome of interest. All statistical analysis was performed with R version 4.03 (R Foundation for Statistical Computing), with 2-sided P values <.05 considered the threshold for statistical significance.
Results
Patient Characteristics
A total of 14,420 patients with cancer underwent a major head and neck surgical procedure from January to November 2017. In total, 3172 (22.0%) patients were determined to be frail. When compared with the nonfrail population, the frail patients were significantly more likely to be older, have Medicare, be in a lower-income quartile, and incur higher charges with a longer length of stay on readmission ( Table 1 ). Furthermore, frail patients had higher baseline Charlson comorbidity scores (≥2) than nonfrail patients (63.0% vs 44.3%, P < .01). Frail patients were less likely than nonfrail patients to present with oral cavity cancers (56.4% vs 73.7%, P < .01) and more likely to present with laryngeal cancer (32.2% vs 19.3%, P < .01). There were no significant differences noted for rural location of practice.
Patient and Hospital Characteristics.
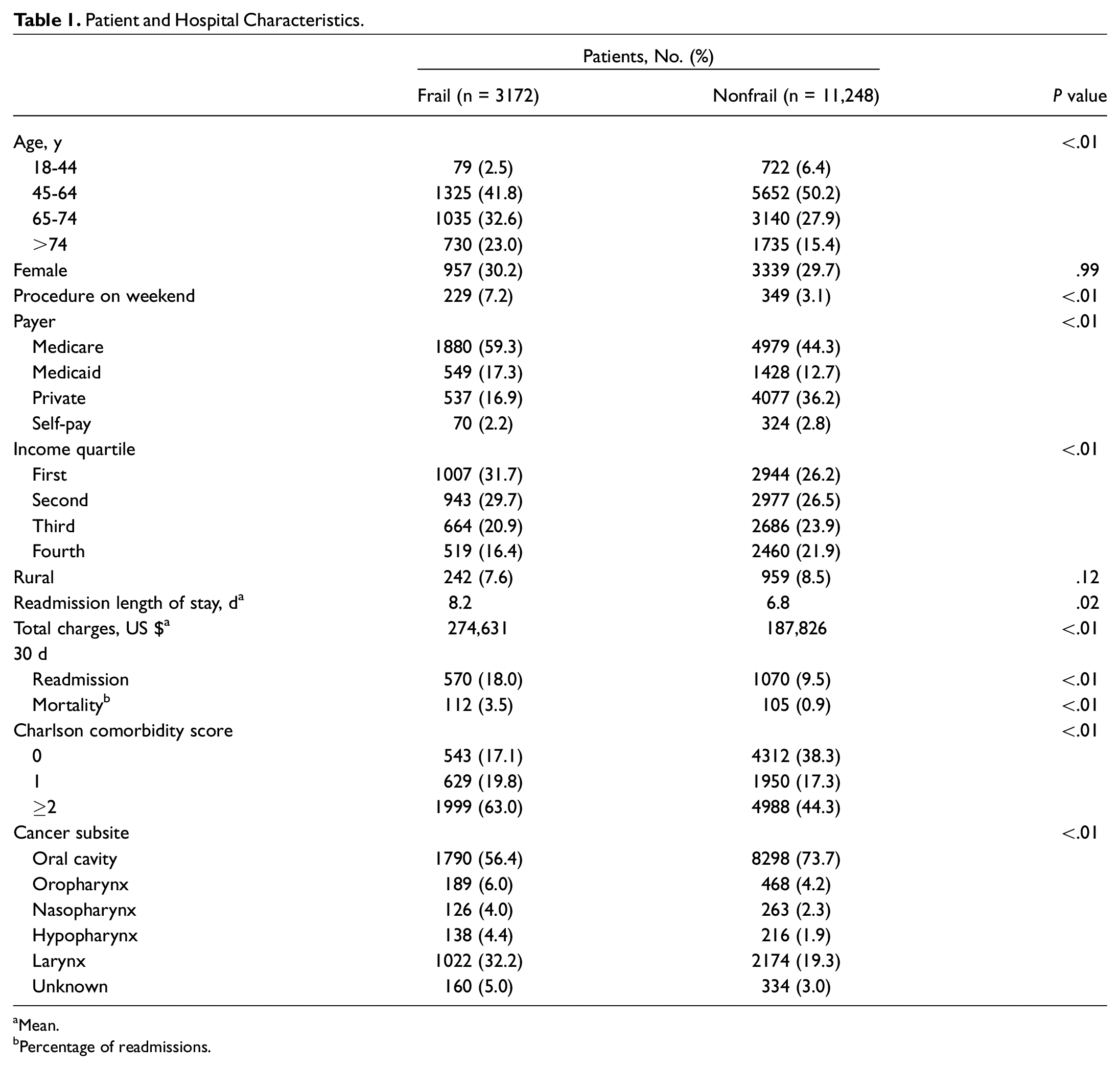
Mean.
Percentage of readmissions.
Readmission Rates
For frail patients, the most common reasons for readmissions were intraoperative and postprocedural complications (including wound infections; 21.2%), sepsis (8.9%), and respiratory failure (8.1%). Nonfrail patients were most often readmitted for intraoperative and postprocedural complications (29.3%), sepsis (6.5%), and pneumonitis (2.9%; Table 2 ).
Top 10 Reasons for Readmission for All, Frail, and Nonfrail Patients. a
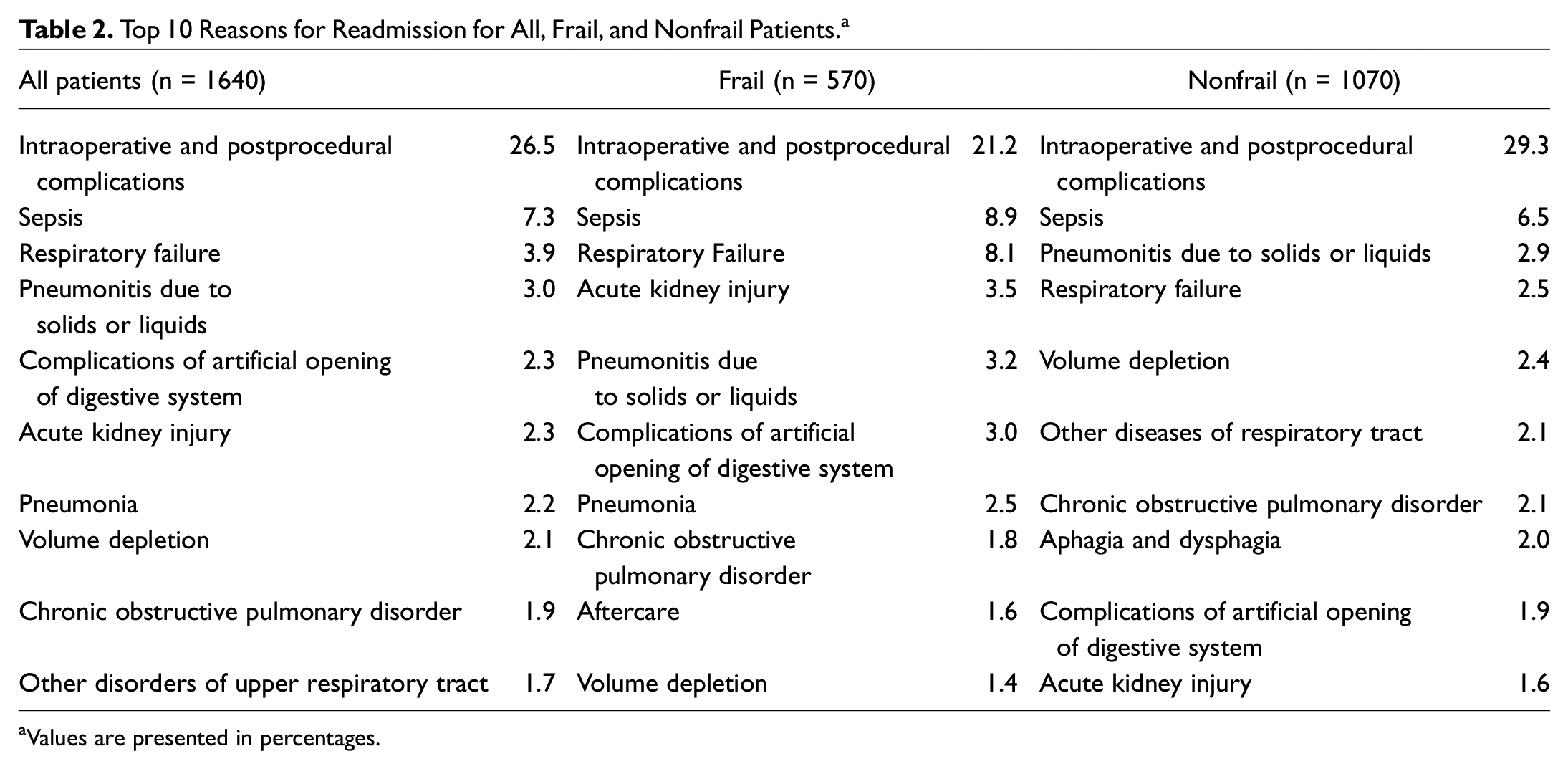
Values are presented in percentages.
Overall, the unplanned 30-day readmission rate was 11.3%. Patients who were frail and underwent major head and neck surgery were more likely to be readmitted within 30 days than nonfrail patients (18.0% vs 9.5%, P < .01; Figure 1 ). Within the first 10 days following discharge, frail patients were significantly more likely to be readmitted than nonfrail patients (5.3% vs 3.0%, P < .01).
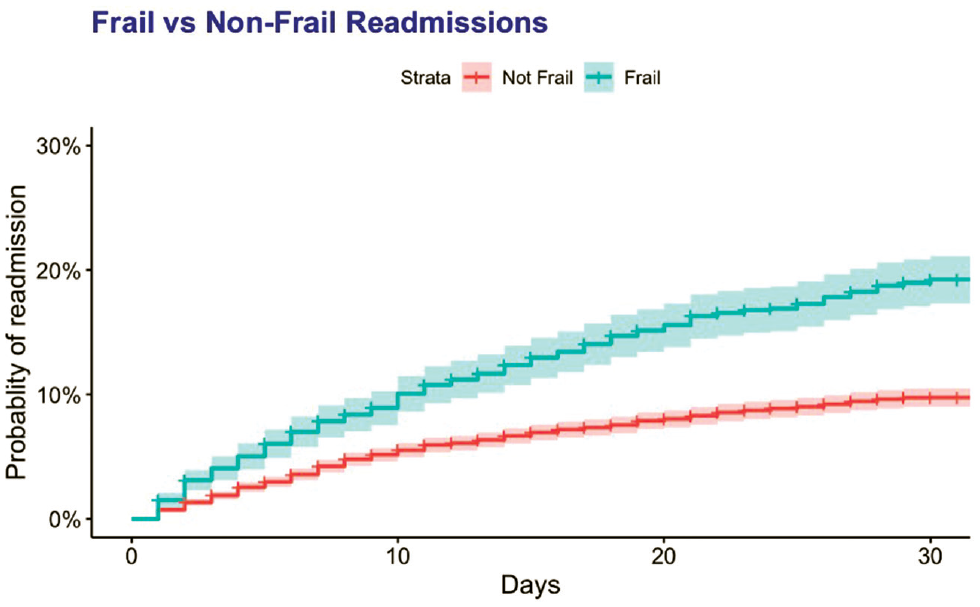
Thirty-day readmission cumulative incidence function comparing frail and nonfrail patients. Shaded region indicates 95% CI.
On multivariable analysis, frailty was associated with an increased risk of readmission (odds ratio [OR], 1.59 [95% CI, 1.37-1.85]; Table 3 ). In addition to smoking, the 5 most common comorbidities were included in the multivariable model. Among these, only electrolyte disturbance was a significant predictor for readmission (1.25 [1.07-1.46]). When compared with the age reference group (45-64 years), younger age (18-44 years) and older age (>75 years) were significant predictors for readmission. The only other significant associations with rate of 30-day readmissions were having commercial insurance (0.76 [0.63-0.92]) and being female (0.86 [0.75-0.97]), both of which decreased the risk of readmission. As compared with the reference site (oral cavity cancer), all other head and neck cancer subsites were significant for readmission (OR range, 1.63-2.29), with hypopharynx cancer being the most robust predictor of 30-day readmission (2.29 [1.73-3.01]).
Patient Characteristics Associated With the Risk of Unplanned Readmission, Death Upon Readmission, and Increased LOS at Rehospitalization Among All Patients.
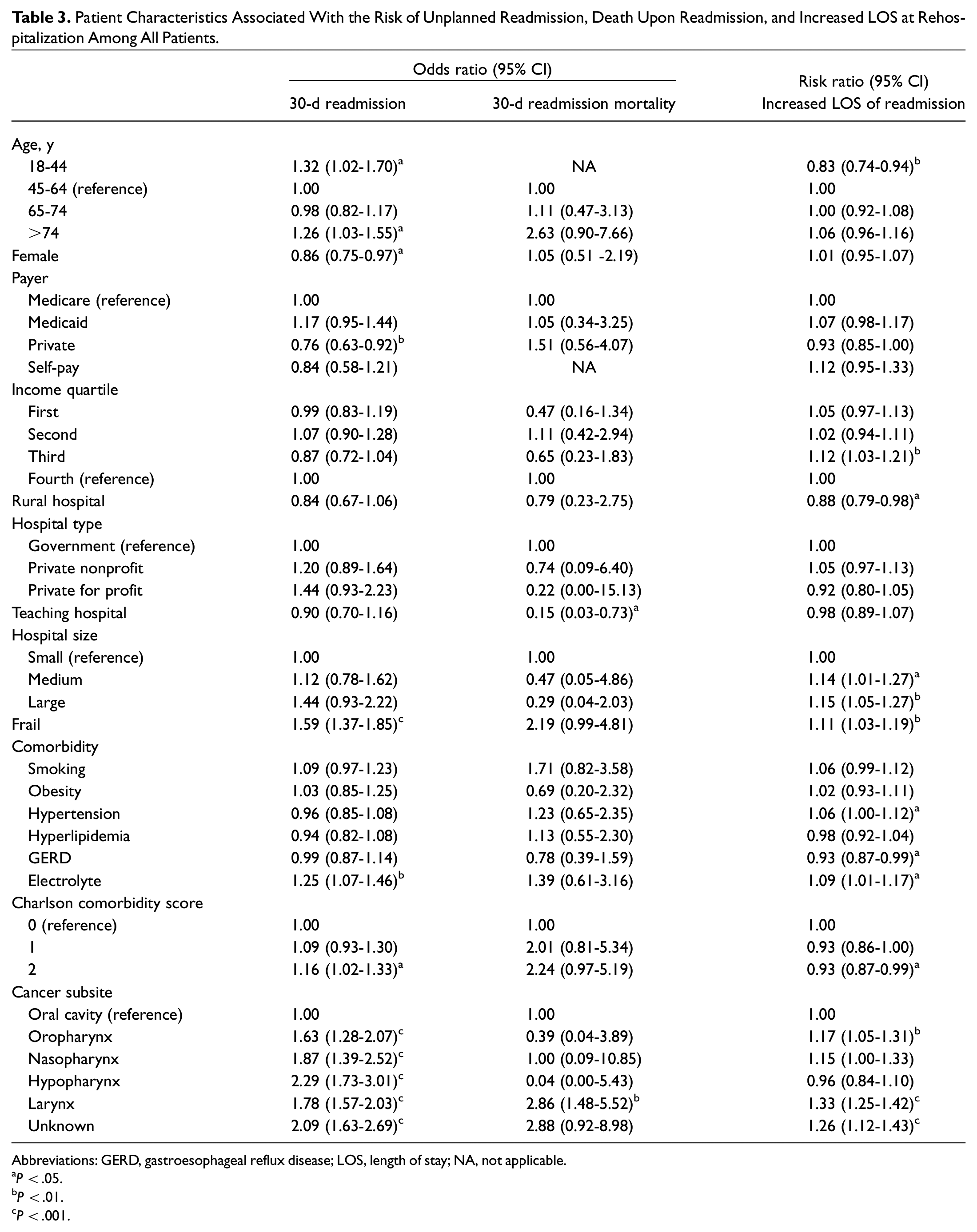
Abbreviations: GERD, gastroesophageal reflux disease; LOS, length of stay; NA, not applicable.
P < .05.
P < .01.
P < .001.
Mortality
Among patients who were readmitted, frail patients were significantly more likely to experience 30-day mortality (3.5% vs 0.9%, P < .01; Figure 2 ). On multivariable analysis, frailty did not significantly predict 30-day mortality (OR, 2.19 [95% CI, 0.99-4.81]). Among cancer subsites, only larynx cancer (2.86 [1.48-5.52]) was a significant predictor of 30-day inpatient readmission mortality. Furthermore, readmission at a teaching hospital had a protective association as compared with a nonteaching hospital (0.15 [0.03-0.73]).
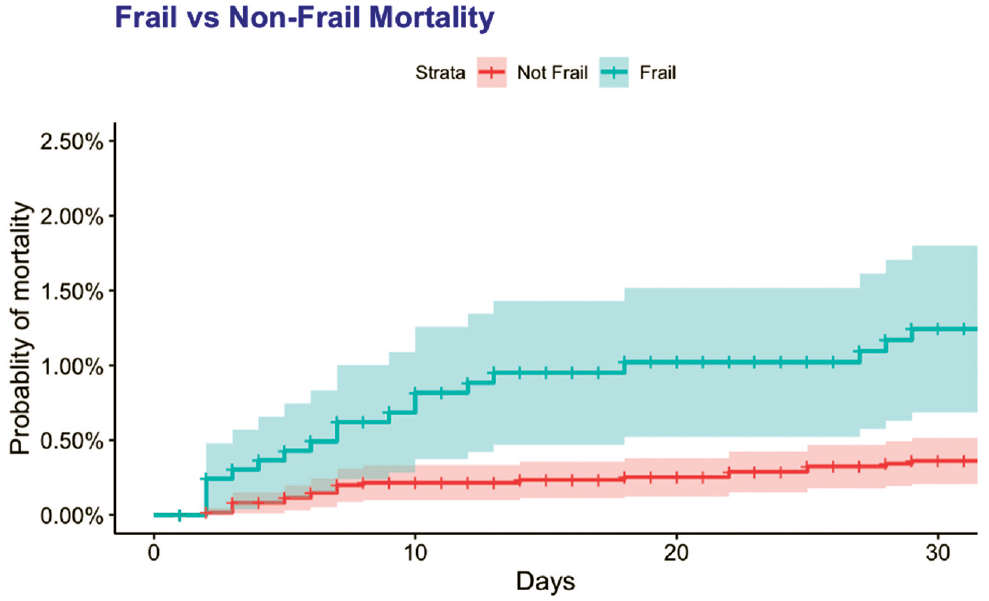
Thirty-day mortality cumulative incidence function comparing frail and nonfrail patients. Shaded region indicates 95% CI.
Length of Stay and Charges
When readmitted, frail patients tended to stay longer (8.2 vs 6.8 days, P < .01). On multivariable analysis, frailty was associated with an increased risk of longer length of stay (risk ratio, 1.11 [95% CI, 1.03-1.19]).
Among the most common comorbidities in our patient cohort, only electrolyte abnormality was a significant predictor of increased length of stay (OR, 1.09 [95% CI, 1.01-1.17]). When compared with oral cavity cancers, oropharynx (1.17 [1.05-1.31]), larynx (1.33 [1.25-1.42]), and an unknown site (1.26 [1.12-1.43]) were significant predictors of having an increased length of stay ( Table 3 ). Furthermore, of those readmitted, frail patients tend to incur more charges across their index admission and readmission combined ($274,631 vs $187,826, P < .01).
Discussion
As the number of head and neck cancer procedures increases annually, so too do associated comorbidities in tandem with growing primary care health concerns such as obesity and hypertension.16-18 Correspondingly, a need exists to identify and optimize patients undergoing such procedures such that harm is minimized and secondarily systemic burden and costs can be decreased by limiting readmissions. In our study examining the NRD, we found a 30-day readmission rate of 11.3% in patients undergoing major head and neck oncologic procedures. After integrating the HFRS risk stratification tool into our data set, we demonstrated that patients with an elevated frailty index (HFRS score ≥5) were significantly more likely to have 30-day readmissions than their nonfrail counterparts. These higher-frailty patients were significantly more likely to have longer hospitalizations and therefore incur greater costs across combined admissions. Furthermore, older patients, patients with electrolyte abnormalities, and patients with a non–oral cavity cancer subsite were more likely to necessitate postoperative readmissions following initial discharge, while patients with private insurance were slightly less likely to need readmission.
Frailty is increasingly being recognized as an important preoperative parameter that extends beyond age and provider assessment. Within geriatric oncology, frailty has become an increasingly important topic of interest as it can inform clinicians of patient health status, prognosis, and response to treatment. 19 However, despite its increasing prevalence and the American Geriatric Society guidelines recommending preoperative frailty assessment in all older patients, screening for frailty remains a limited practice.20,21 This clinical characteristic, when used in the correct setting, can help minimize adverse patient perioperative outcomes and limit readmission and hospital expenses in the grand scheme.
The present study is the first to evaluate HFRS-based frailty scoring utility in head and neck oncologic procedures, but it is just one piece of many in the existing body of literature supporting the premise of frailty as an important predictor of postoperative outcomes in otolaryngology. The results are mixed with different frailty measures, such as the modified frailty index (mFI), Johns Hopkins Adjusted Clinical Groups, and the Groningen Frailty Indicator. Bras et al found that the Groningen Frailty Indicator was not a predictor of complications after head and neck cancer surgery, though it did predict elderly patients who subjectively report a poorer postoperative recovery. 22 Abt et al demonstrated that mFI, while associated with postoperative complications, was not associated with unplanned readmissions or mortality. 23 Alternatively, in a single-institution analysis, Pitts et al noted higher mFI to increase odds of readmission. 14 Nieman et al showed that a higher Adjusted Clinical Groups score was associated with increased length of stay, incremental costs, postoperative complications, and mortality, though they did not comment on readmission risk. 24 The association between frailty and survival was shown to be independent of demographic variables in alternative cohorts, and the use of frailty helps add dimensionality to the analysis of the patient in a health system where access to care, race, and education/income have been linked to survival outcomes in head and neck cancer, yet actionable directions are few.25,26
While frailty indices have long been researched, few have actually been implemented directly into patient care. As a scoring tool dependent on the ICD-10, the HFRS can be integrated into existing electronic health record systems, giving health care providers an additional pathway to evaluate and risk stratify patients possibly in need of more intensive care or optimization. Potential avenues for intervention for patients classified “frail” per the HFRS can include earlier and more frequent pre- and postoperative visits, home monitoring of vitals, or even solicitation of patient-reported outcomes.
Strengths of this study include that it is a nationally representative multi-institution cohort derived from sites across the country. Furthermore, while comparable prior studies were unable to distinguish between planned and unplanned readmissions, 2017 NRD data allowed us to make such a distinction to more accurately categorize incidence of elective vs nonelective readmissions. However, because our study relies on observational large database patient data, it is prone to selection and misclassification bias. The HFRS scoring tool relies exclusively on ICD-10 diagnosis codes; therefore, accurate code assignments are a necessary prerequisite to proper risk stratification and subsequent assignment into frailty categories. In addition, mortality data from the NRD is derived from readmission-related hospitalization and not from index readmission or a postreadmission timeline; as such, the true mortality rate is likely underestimated in this study. Furthermore frailty assessment based on diagnosis clustering and coding may not adequately characterize the physical phenotype of frailty. We acknowledge that frailty is one of many components that can assist surgeons in accurately predicting patients at risk for readmissions, as there was some overlap in the reasons underlying readmissions between frail and nonfrail patients. We envision this frailty index being used preoperatively to risk stratify patients in need of greater clinical optimization, as ICD-10 diagnoses were presumably accrued in larger amounts in sicker patients with more protracted postoperative courses to be able to predict readmission risk. Last, this frailty index remains susceptible to the influences of delays in billing and coding associated with prior and current hospitalizations. Overall, frailty quantification as a screening tool ought to be cost-effective, quick, and efficient, which is where an ICD-10–based risk stratification tool such as the HFRS shines, though ultimately more granular attributes may be lost, such as physical phenotype and activities of daily living assessments.
Conclusion
Patients with an elevated frailty index were significantly more likely to experience 30-day readmissions and subsequently more likely to experience longer inpatient hospitalizations and incur greater expenses than nonfrail patients. HFRS represents a valuable stratification tool to help identify at-risk patients who can undergo preoperative optimization to minimize their probability of short-term rehospitalization. This functional status assessment represents an avenue for future quality improvement efforts aimed toward mitigating readmission.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211043489 – Supplemental material for Frailty Index as a Predictor of Readmission in Patients With Head and Neck Cancer
Supplemental material, sj-docx-1-oto-10.1177_01945998211043489 for Frailty Index as a Predictor of Readmission in Patients With Head and Neck Cancer by Rohith S. Voora, Alexander S. Qian, Nikhil V. Kotha, Edmund M. Qiao, Minhthy Meineke, James D. Murphy and Ryan K. Orosco in Otolaryngology–Head and Neck Surgery
Footnotes
This article was presented at the 2021 AAO-HNSF Annual Meeting & OTO Experience; October 3-6, 2021; Los Angeles, California.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.