
Abstract
Objective
To examine postoperative opioid-prescribing patterns following otologic surgery.
Study Design
Retrospective population-based descriptive study.
Setting
All hospitals in the Canadian province of Ontario.
Methods
Of all patients with advanced ear surgery between July 1, 2012, and March 31, 2019, 7 cohorts were constructed: tympanoplasty with or without ossiculoplasty (n = 7812), atticotomy/limited mastoidectomy (n = 1371), mastoidectomy (n = 3717), semicircular canal occlusion (SCO; n = 179), stapedectomy (n = 2735), bone-implanted hearing aid insertion (n = 280), and cochlear implant (n = 2169). Prescriptions filled for narcotics postoperatively were calculated per morphine milligram equivalent (MME) opioid dose. Multivariable regression was used to determine predictors of higher opioid doses.
Results
The mean ± SD MMEs prescribed were as follows: tympanoplasty with or without ossiculoplasty, 246.77 ± 1380.78; atticotomy/limited mastoidectomy, 283.32 ± 956.10; mastoidectomy, 280.56 ± 1018.50; SCO, 328.61 ± 1090.86; stapedectomy, 164.64 ± 657.18; bone-implanted hearing aid insertion, 326.11 ± 1054.66; and cochlear implant, 200.87 ± 639.93. SCO (odds ratio [OR], 1.69 [95% CI, 1.16-2.48]) and mastoidectomy (OR, 1.50 [95% CI, 1.36-1.66]) were associated with higher opioid doses than tympanoplasty-ossiculoplasty. Asthma (OR, 1.24 [95% CI, 1.12-1.38]), chronic obstructive pulmonary disease (OR, 1.29 [95% CI, 1.12-1.47]), myocardial infarction (OR, 1.33 [95% CI, 1.05-1.68]), diabetes (OR, 1.22 [95% CI, 1.08-1.39]), and substance-related and addictive disorders (OR, 2.59 [95% CI, 1.67-4.00]) were associated with higher opioid doses prescribed. Overall MME prescribed by year demonstrates a sharp drop from 2017-2018 to 2018-2019.
Conclusion
This large comprehensive population study provides insight into the prescribing patterns following otologic surgery. The large amounts prescribed and substantial variation require further study to determine barriers that limit good opioid-prescribing stewardship in the postoperative period.
Acute pain following traumatic tissue injuries is generally limited in duration and associated with temporal reductions in intensity. 1 Opioid therapy is a common treatment option for postoperative acute pain. According to Health Quality Ontario, nearly 2 million people filled an opioid prescription in 2015-2016. 2 An estimated 13% of Canadians used prescription opioids in 2015, with approximately 2.2% acknowledging opioid abuse. 3 According to a national report, >9000 Canadians died from apparent opioid-related harms from January 2016 to June 2018. 4 While the reasons underlying the current opioid epidemic are multifactorial, one contributing factor that needs more attention is perioperative prescribing patterns. Although opioids may be necessary to provide patients with adequate pain relief, excessive postoperative opioid prescribing has been associated with increased risks of new long-term opioid use, drug diversion, and the development of opioid use disorder. 5
While otologists routinely manage postoperative pain, limited evidence exists to guide prescribing. The individual variations in pain tolerance along with the range of surgical procedures in otology make it difficult to understand systemic patterns in opioid prescriptions. Recent otologic studies indicate patterns of overprescriptions with patients consuming <50% of prescribed opioids.6-8 However, these studies are limited by small sample sizes, compromising their generalizability. The objective of this study is to understand longitudinal province-wide variations in opioid prescriptions following otologic procedures. This study is the first to use a comprehensive data set from the Canadian province of Ontario through the Narcotics Monitoring System (NMS) database to evaluate trends of prescribing patterns in common otologic procedures with detailed patient characteristics of opioid users, including demographics, geographic regions, and comorbidities.
Methods
Institutional Review Board
This study was approved by the Research Ethics Board of Queen’s University Health Sciences and Affiliated Teaching Hospitals (project 6025803).
Participants
Ontario is the largest province in Canada, with a population of >14 million residents in 2019, representing 38.8% of the Canadian population. 9 The Ontario NMS captures information on all prescriptions for controlled medications prescribed and dispensed from outpatient pharmacies in the province, regardless of payer. Pharmacist data entry into the NMS is mandatory for all controlled substances. 10 We identified 18,263 patients who underwent specific otologic surgical procedures between July 1, 2012, and March 31, 2019, based on Ontario Health Insurance Plan (OHIP) surgical billing codes (Supplemental Table S1, available online). Initial cohorts were tympanoplasty, ossiculoplasty, atticotomy, cortical mastoidectomy, mastoidectomy, endolymphatic sac shunt/decompression, semicircular canal occlusion (SCO), stapedectomy, bone-implanted hearing aid insertion (BAHA), and cochlear implant (CI). Cohorts with small sample sizes were combined by surgical similarities. The endolymphatic sac shunt/decompression cohort was excluded due to the small sample size and the inability to combine with another cohort. The index date for each cohort was the date of the first surgery. Patients were excluded from the cohorts if they had missing age and sex, resided outside of Ontario, and had lapses in their OHIP coverage within a 1-year period of the index date.
Data Sources
Administrative data sets housed at ICES (formerly the Institute for Clinical Evaluative Sciences) were used to obtain the data for this study. ICES is an independent nonprofit research organization funded by the Ontario Ministry of Health and the Ministry of Long-term Care, whose data holdings include all health care–related events for the population of Ontario. The Registered Persons Database (RPDB) is a repository of demographic information for residents of Ontario who are eligible for the OHIP. The RPDB contains information on health card number, date of birth, sex, address, and deceased date. Personal identifying information in the RPDB is removed, and each unique health number is converted into an anonymous unique identifier, the ICES Key Number. The OHIP database contains data on the diagnosis and fee-for-service claims submitted by physicians and paid by the universal health care system. The Canadian Institute for Health Information’s Discharge Abstract Database and Same Day Surgery data contain information on all inpatient and day surgery visits, respectively, abstracted from hospital records for patient diagnoses and procedures. We identified opioid prescription characteristics in the NMS, which captures information regarding all opioids dispensed from all retail pharmacies regardless of payer. These data sets were linked via unique encoded identifiers and analyzed at ICES.
Analyses
Summary statistics were generated for sociodemographic details (age, sex, and neighborhood income quintiles) and comorbidities prior to first surgery: asthma, chronic obstructive pulmonary disease (COPD), hypertension, congestive heart failure, stroke, myocardial infarction, diabetes, dementia, rheumatoid arthritis, and substance-related and addictive disorder ( Table 1 ). Age breakdown and frequency by place of residence can be found in Supplemental Table S2 (available online).
Demographics and General Health Characteristics of Patients With Specified Advanced Ear Surgery. a
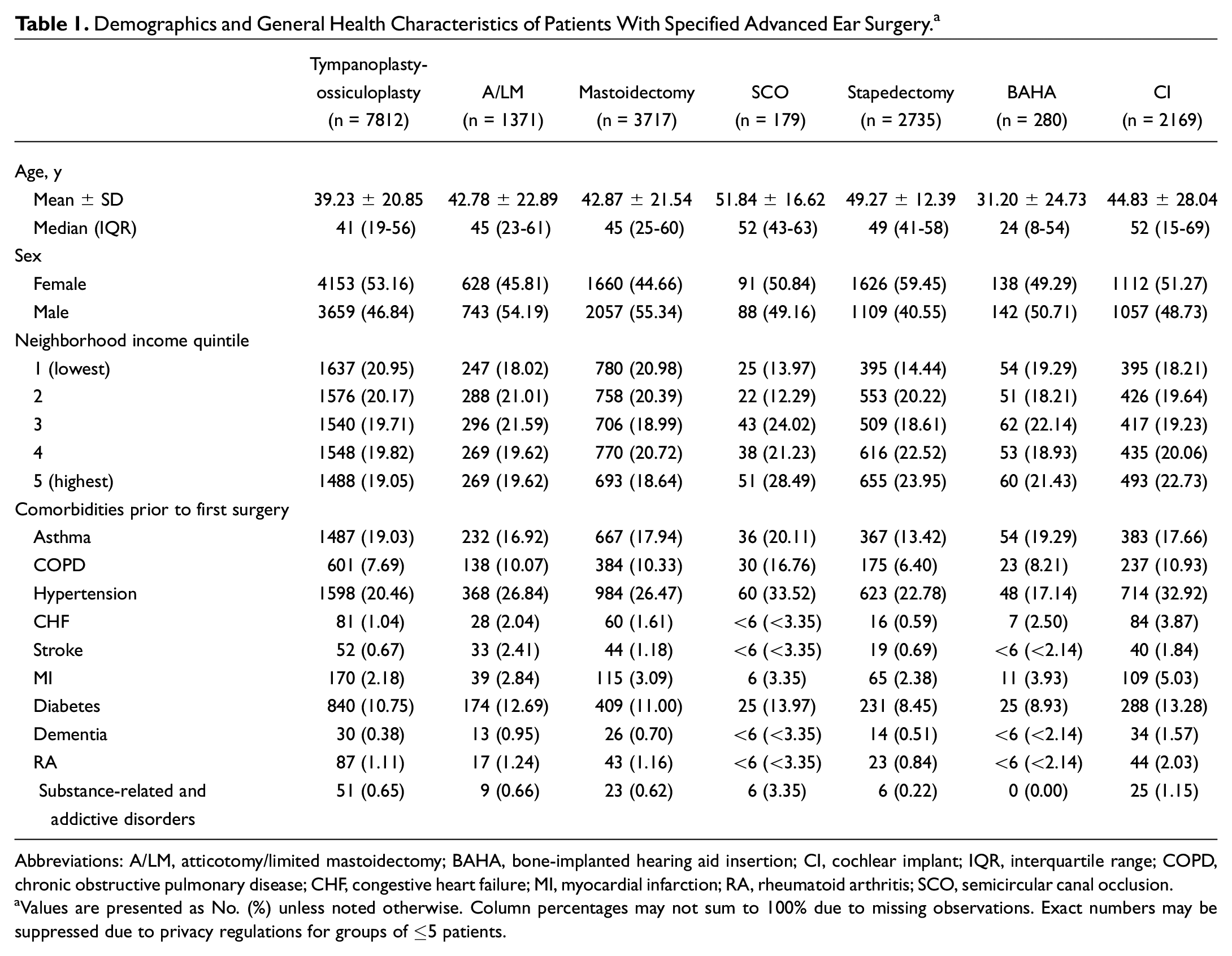
Abbreviations: A/LM, atticotomy/limited mastoidectomy; BAHA, bone-implanted hearing aid insertion; CI, cochlear implant; IQR, interquartile range; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; MI, myocardial infarction; RA, rheumatoid arthritis; SCO, semicircular canal occlusion.
Values are presented as No. (%) unless noted otherwise. Column percentages may not sum to 100% due to missing observations. Exact numbers may be suppressed due to privacy regulations for groups of ≤5 patients.
The prescribed total morphine milligram equivalent (MME) was calculated with the 2017 Canadian “Guideline for Opioid Therapy and Chronic Noncancer Pain” conversion table. 11 This conversion was used to normalize the different narcotics to allow comparison (eg, morphine, 1 mg = 1 MME; oxycodone, 1 mg = 1.5 MME). The mean with standard deviation and median with interquartile range were calculated for total postoperative MME dose in milligrams ( Table 2 ). Frequencies of medications prescribed were calculated within 2 months prior to surgery and within 1 month postsurgery (Supplemental Table S3, available online). For predictors of higher opioid prescriptions, multivariable logistic regression was used, with the total postoperative MME dose outcome defined as >135 vs ≤135 mg (ie, the median MME dose from all patients who were given postoperative opioid prescriptions; Table 3 ). LHIN (Local Health Integration Network) regions were anonymized and compared with a randomly selected region. Type of first surgery was compared with tympanoplasty-ossiculoplasty. Statistical significance was reached if P < .05. All analyses were performed at ICES with the SAS Enterprise Guide 7.15 (SAS Institute).
Pain Medication Outcomes of Patients With Specified Advanced Ear Surgery.
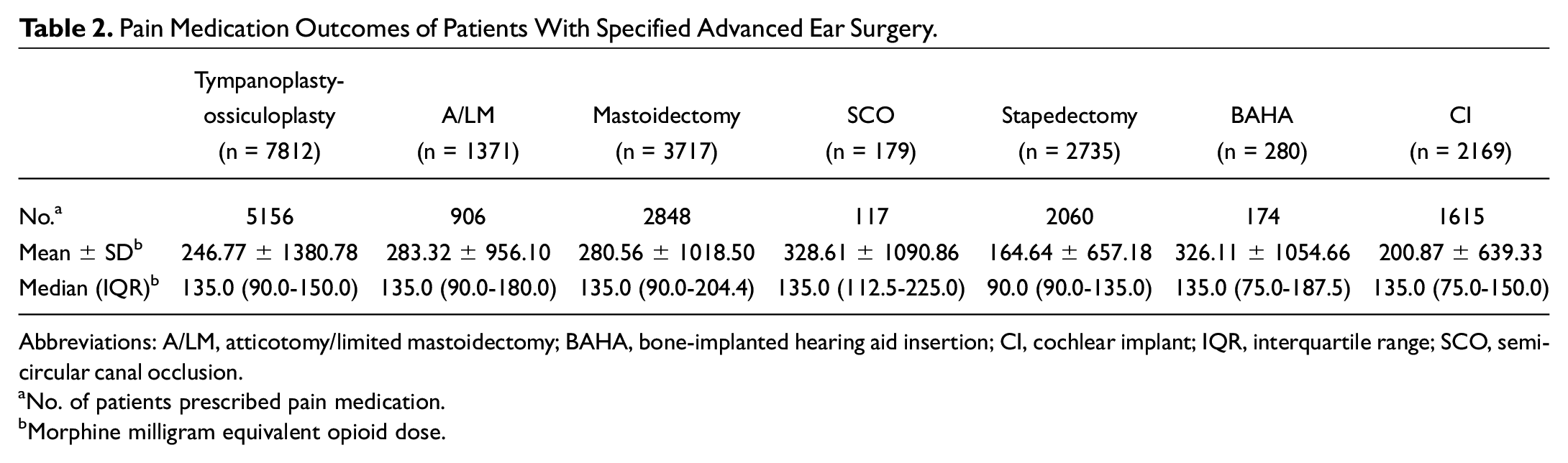
Abbreviations: A/LM, atticotomy/limited mastoidectomy; BAHA, bone-implanted hearing aid insertion; CI, cochlear implant; IQR, interquartile range; SCO, semicircular canal occlusion.
No. of patients prescribed pain medication.
Morphine milligram equivalent opioid dose.
Factors Affecting Likelihood of Higher Opioid Prescription in Perioperative Period. a
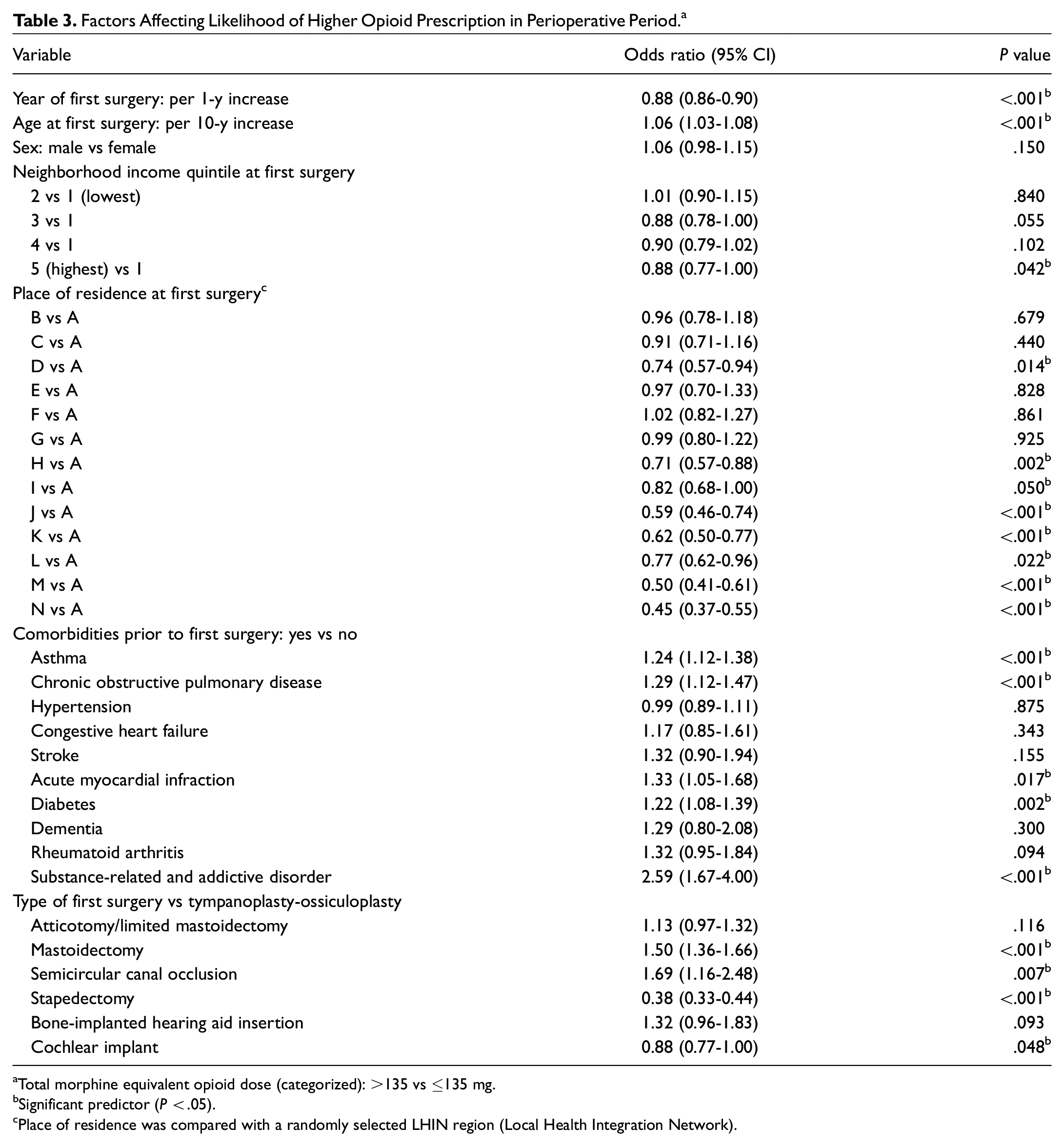
Total morphine equivalent opioid dose (categorized): >135 vs ≤135 mg.
Significant predictor (P < .05).
Place of residence was compared with a randomly selected LHIN region (Local Health Integration Network).
Results
Cohort Characteristics
We identified 18,263 patients who underwent otologic surgery between 2012 and 2019. Separate cohorts were created for each advanced otologic surgical procedure, including tympanoplasty-ossiculoplasty (n = 7812), atticotomy/limited mastoidectomy (n = 1371), mastoidectomy (n = 3717), SCO (n = 179), stapedectomy (n = 2735), BAHA (n = 280), and CI (n = 2169). The median age ranged from 24 years (Q1-Q3, 8-54) for the BAHA cohort to 52 years (15-69) for the CI cohort. In the total sociodemographic cohort, 9408 (51.51%) patients were female; 3709 (20.31%) were in the highest income quintile; 120 (0.66%) had substance-related and addictive disorders prior to surgery; and 4395 (24.07%) experienced hypertension before surgery. Of all the comorbidities reported prior to the first surgery, hypertension was the most common health condition, followed by asthma, diabetes, and COPD. Regional variations based on LHIN for total MME opioid prescribed were identified, with the largest variation seen in mastoidectomy cohort ( Figure 1 ).
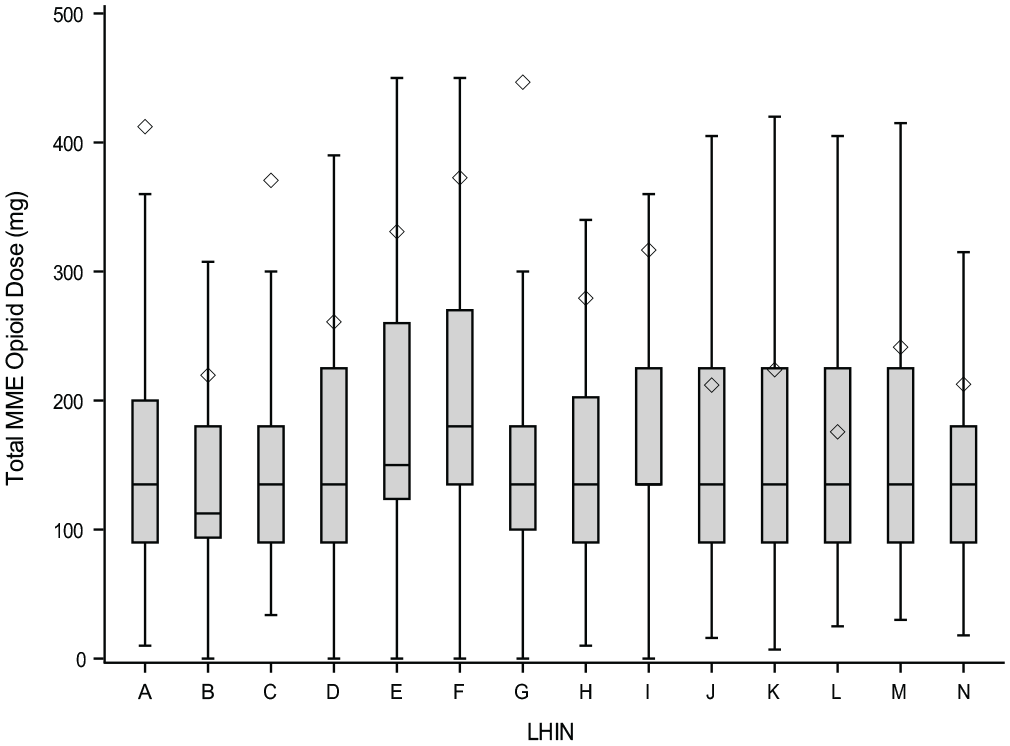
Total morphine milligram equivalent (MME) opioid prescribed for mastoidectomy cohort based on place of residence. The Q1-Q3 and median are represented by the box and line; the mean is represented by the diamond; and the 95% CI is represented by the error bars. LHIN, Local Health Integration Network.
Patterns in Opioid Prescription
Of the 18,263 patients, 12,876 (70.50%) received opioids, while 5387 (29.50%) have no records of opioid prescription in the NMS database. The mean ± SD MMEs prescribed were as follows: tympanoplasty with or without ossiculoplasty, 246.77 ± 1380.78; atticotomy/limited mastoidectomy, 283.32 ± 956.10; mastoidectomy, 280.56 ± 1018.50; SCO, 328.61 ± 1090.86; stapedectomy, 164.64 ± 657.18; BAHA, 326.11 ± 1054.66; and CI, 200.87 ± 639.93 ( Figure 2 ). The median (interquartile range) MME prescribed was as follows: tympanoplasty with or without ossiculoplasty, 135.0 (90.0-150.0); atticotomy/limited mastoidectomy, 135.0 (90.0-180.0); mastoidectomy, 135.0 (90.0-204.4); SCO, 135.0 (112.5-225.0); stapedectomy, 90.0 (90.0-135.0); BAHA, 135.0 (75.0-187.5); and CI, 135.0 (75.0-150.0). Opioids included codeine, oxycodone, buprenorphine, hydromorphone, morphine, and methadone. Other medications were benzodiazepines and medical tetrahydrocannabinol (Supplemental Table S3, available online). Less than 11% of the patients were using opioids before surgery ( Figure 3 ). Immediate-release codeine was the most common opioid used in all cohorts preoperatively except for SCO, with oxycodone being the most common. In addition, <6% of the patients were users of other medications before surgery except for SCO group, with 7.26% of patient outcomes for benzodiazepines. Buprenorphine was the least commonly prescribed opioid at a frequency of <4% for all surgical procedures. Mean MME opioid dose prescribed after otologic surgery by fiscal year shows a decline from 2012-2013 (ie, July 2012–March 2013) to 2018-2019 (ie, April 2018–March 2019) with a sharp drop from 2017-2018 (ie, April 2017–March 2018) to 2018-2019 (ie, April 2018–March 2019; Figure 4 ).
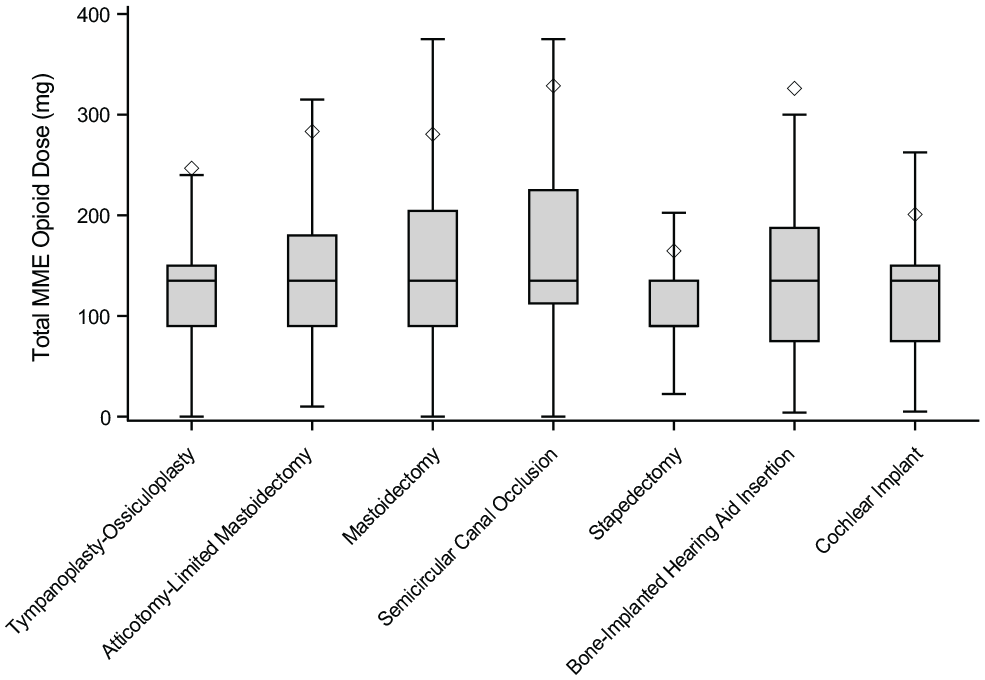
Total morphine milligram equivalent (MME) prescribed for all cohorts. The Q1-Q3 and median are represented by the box and line; the mean is represented by the diamond; and the 95% CI is represented by the error bars.
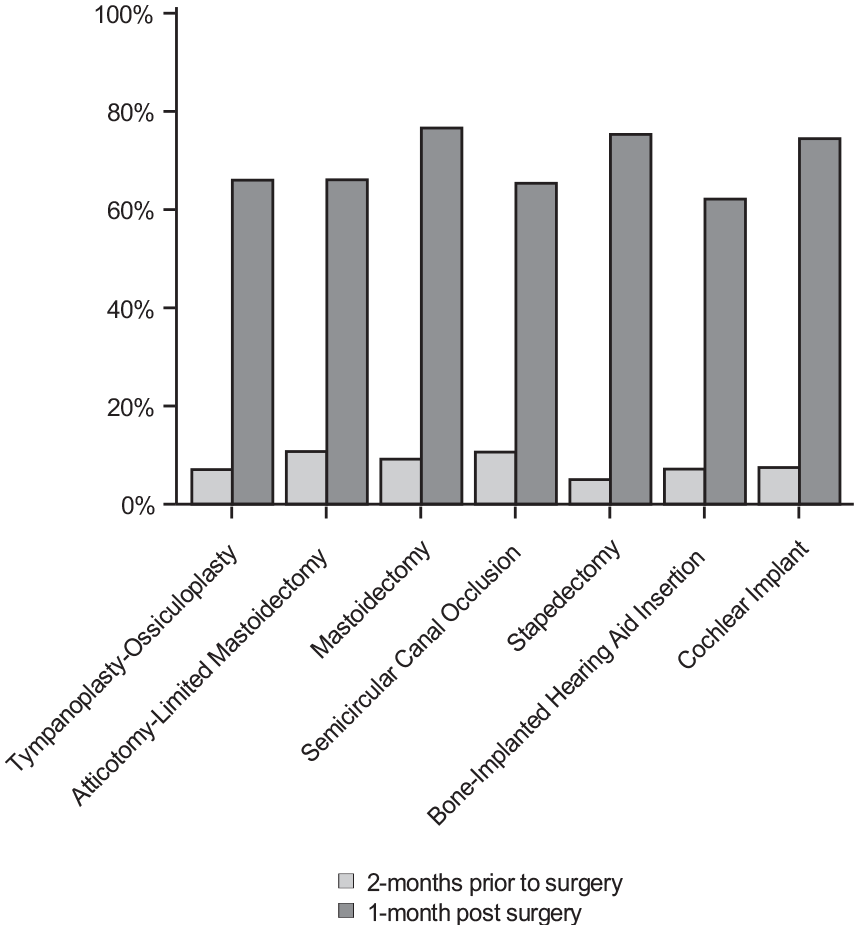
Percentage of patients who were prescribed pain medications in all cohorts 2 months prior to surgery and 1 month after.
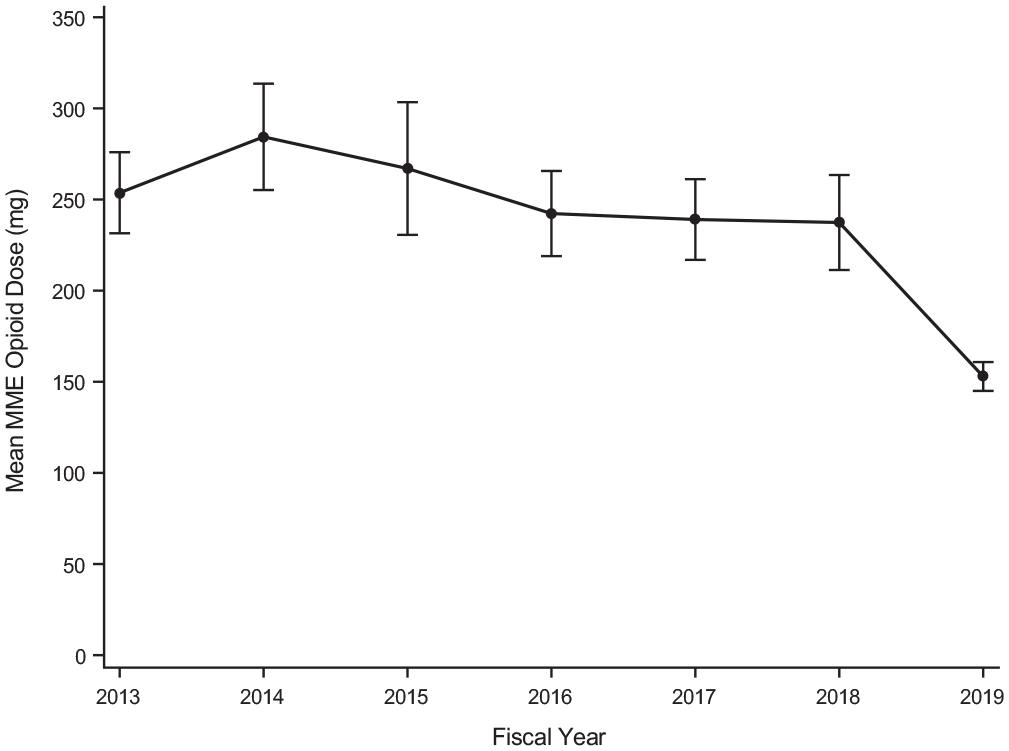
Mean (SE) morphine milligram equivalents (MMEs) prescribed following otologic surgery by fiscal year. Year is denoted on the x-axis, and aggregate MME is denoted on the y-axis (1 month postsurgery).
Factors Influencing Higher Opioid Dose
In the multivariable logistic regression analysis for factors influencing higher opioid dose, year of surgery (per 1-year increase) was associated with lower dose outcome (odds ratio [OR], 0.88 [95% CI, 0.86-0.90]; P < .001). Increasing age at first surgery (per 10-year increase) was associated with higher dose (OR, 1.06 [95% CI, 1.03-1.08]; P < .001). Highest income quintile was associated with lower dose when compared with the lowest income quintile (OR, 0.88 [95% CI, 0.77-1.00]; P = .042). Of the 14 anonymized LHIN regions, 8 had statistically significant lower dose outcomes versus a randomly selected LHIN region. Of the comorbidities prior to first surgery, the following were associated with higher opioid dose prescribed: asthma (OR, 1.24 [95% CI, 1.12-1.38]; P < .001), COPD (OR, 1.29 [95% CI, 1.12-1.47]; P < .001), acute myocardial infraction (OR, 1.33 [95% CI, 1.05-1.68]; P = .017), diabetes (OR, 1.22 [95% CI, 1.08-1.39]; P = .002), and substance-related and addictive disorders (OR, 2.59 [95% CI, 1.67-4.00]; P < .001). When different types of otologic surgery were compared with tympanoplasty-ossiculoplasty, mastoidectomy (OR, 1.50 [95% CI, 1.36-1.66]; P < .001) and SCO (OR, 1.69 [95% CI, 1.16-2.48]; P = .007) were associated with higher opioid prescriptions. Stapedectomy (OR, 0.38 [95% CI, 0.33-0.44]; P < .001) and CI (OR, 0.88 [95% CI, 0.77-1.00]; P = .048) were associated with lower MME prescribed when compared with tympanoplasty-ossiculoplasty.
Discussion
Despite the increased awareness and knowledge pertaining to the risks of prescription opioids, there are minimal guidelines available for surgeons to guide safe prescribing practices. A recent specialty-specific guideline recommends that otolaryngologists–head and neck surgeons develop a multimodal treatment plan and limit opioid therapy to the lowest effective dose. 12 In addition, the guideline recommends nonopioid multimodal analgesia as a first-line therapy, screening for opioid use disorder risk factors, counseling around pain expectations, and discussion of opioid-related risks and resources for proper disposal of unused opioids. Ultimately, the dose and duration of prescription rely on clinical judgment and patient preferences.
Opioid Prescription in Otology/Neurotology
In this study, we found wide variability in MME doses dispensed postoperatively for advanced ear surgery, with average opioid prescriptions of 239.73 ± 1097.62 MME. These findings are higher than those reported in other otologic studies, possibly suggesting patterns of overprescriptions.6-8 The type and rate of prescriptions varied, with immediate-release codeine being the most common. Our findings show that SCO and mastoidectomy surgery is associated with higher opioid doses in comparison with middle ear surgery. Pain after skull base surgery is complex and more likely to include tissue dissection, which could contribute to the variability seen in these cohorts. 13 Similar mean MMEs were noted for BAHA and SCO despite differences in surgical complexity. However, median MMEs demonstrate a higher range for SCO than for BAHA, indicating more pain management after SCO surgery. Factors such as comorbidities, lack of standardization, and opioid prescriptions from other providers can influence MMEs prescribed irrespective of surgical approaches. In addition, extra MMEs were filled for tympanoplasty-ossiculoplasty than CI, which involves more tissue dissection. The CI surgical cohort encompasses a wide age range, including pediatrics and adolescents, who may be prescribed nonopioid pharmacotherapy for pain management to avoid opioid-related adverse events. 14 In the literature, one study found no statistically significant differences in opioid consumption among different otologic surgical procedures, whereas another study reported that patients who had postauricular incisions were prescribed more opioids (86.2 MMEs) as compared with those undergoing middle ear–type procedures.6,7 The inclusion of all patients with diverse characteristics, such as wide age range, previous opioid use, and comorbidities, can influence the variations.
Median opioid prescribed for many of the procedures was 135 MME, with the lowest median for stapedectomy at 90 MME. In a previous study, patient-reported pain control after otologic surgery was achieved for 75% with 12 pills (MME = 60 mg) and for 90% with 24 pills (MME = 135 mg). 6 Our findings are higher in comparison, indicating possible patterns of unnecessary prescriptions. In addition, opioid-naïve patients are at a higher risk for long-term use with associated increase in morbidity and mortality. 15 Our study indicates a large change in postoperative opioid medication dispensed for all cohorts when compared with preoperative opioid prescriptions. This demonstrates that the prescriptions filled after the surgery date were for postoperative pain control rather than regular opioid use by the patients. Although our data do not contain information on the usage of the opioids, an increasing amount of literature suggests that <50% of prescribed opioids are used after otologic surgery. 8 The fate of these unused prescription opioids remains unclear and can lead to nonmedical usage of drugs.
Opioid Prescription by Socioeconomic and Geographic Data
The opioid epidemic has disproportionately affected low-income communities in Canada. 16 In bivariate analysis, highest income quintile was associated with lower dose outcome as compared with the lowest income quintile. This finding is consistent with an American study showing that increasing income is associated with smaller doses of opioids in comparison with the lowest income brackets. 17 These income-level disparities in a public health care database increase the risk of opioid-related harms and may be influenced by provider perceptions and patient-specific factors. 16
Regarding the influence of age in higher opioid dose prescriptions, our data suggest that increasing age at first surgery (per 10-year increase) was associated with higher opioid dose prescribed. This contrasts with the American study that showed younger patients receiving more opioids. 17 Patients aged <18 years were excluded in that study, whereas our findings include all ages. Pediatric patients are less likely than older patients to be prescribed opioids postoperatively. Opioid prescribing in children is influenced by assessment of opioid harm, family preferences, and effective nonopioid regimen. 18
Our data show variations in opioid prescriptions based on the place of residence. LHINs were historically the health authorities responsible for regional administration of public health care services in Ontario. The regions were anonymized to protect identity. Out of the 14 LHIN regions, 8 had statistically significant lower dose outcomes versus a randomly selected region. This demonstrates significant variability within the province. A recent Canadian study examining opioid prescription postotologic surgery noted variations in surgical techniques through questionnaires that were filled by Canadian surgeons. 19 The study showed a transcanal approach for stapedotomy (62%), transcanal and endaural for tympanoplasty (31% and 38%), endaural and endoscopic for small cholesteatoma (36% and 29%), and postauricular for extensive cholesteatoma (93%). 19 Therefore, it would be difficult to predict factors that determine regional variability, such as number of surgeons, surgical approaches, and availability of resources within each region. Additionally, the mean values are higher for the mastoidectomy cohort than the median and third quartile boundary, suggesting a positive skew of the data. Possible explanations would be confounding prescriptions from other providers in the time frame, lack of guidance in postoperative pain management, and patient-related factors, including previous opioid use. It is possible that these outliers may be contributing to the higher mean values noted. When Canadian otologists’ perspectives are considered, opioids are more commonly prescribed in Canada than Austria, with surgeons reporting low confidence in postoperative pain management. 19 This with our findings makes it more relevant to highlight opioid stewardship among Canadian otologists.
Opioid Prescriptions and Comorbidities
Of the comorbidities analyzed prior to first surgery, asthma, COPD, acute myocardial infraction, diabetes, and substance-related and addictive disorders were associated with higher opioid doses prescribed. Patient related factors such as younger age, lower income, and specific comorbidities (diabetes, heart failure, and pulmonary disease) are associated with higher risks of prolonged opioid use. 20 Furthermore, alcohol and substance abuse disorders increase the risk of new persistent opioid use in opioid-naïve patients, regardless of surgical procedures. 21 These patient-specific factors and comorbidities are important considerations for surgeons when tailoring postoperative pain management.
Opioid Prescription by Year
Finally, our findings show that the amount of opioids prescribed decreased sharply in the most recent years of the study (2018-2019). This finding reveals a similar trend to a nationwide otologic study conducted in the United States. 17 This downward trend could reflect the increasing national dialogue to control the opioid epidemic. In several other surgical fields, sufficient postoperative pain control with NSAIDs (nonsteroidal anti-inflammatory drugs) has shown to be comparable or even superior to opioids in randomized studies and meta-analyses.22,23 Most otologic surgery studied comprises outpatient procedures with mild to moderate postoperative pain scores for ≤4 days.12,24 There are opportunities to treat postoperative pain through a multimodal approach with emphasis on nonopioid pharmacotherapy such as NSAIDs and acetaminophen as first-line agents.23,25
Strengths and Limitations
Our study has several strengths. The comprehensive single-payer health services databases available in Ontario allowed for an objective population-based measure with large sample sizes. Linkage of the data set with the NMS provided detailed information of medications dispensed for all cohorts. Previous studies on opioid-prescribing patterns within the specialty were not designed to characterize frequency and dose of opioid initiation at a population level with linked health administrative databases. There are limitations to our study that are intrinsic to administrative data. Given the complexity of narcotic prescriptions, summary statistics on the number of pills and exact durations are not able to be delineated. Historical dispensing data may not reflect evolving opioid-prescribing patterns. Since the NMS captures all opioids dispensed, our data may be influenced by other confounding sources, such as prescriptions from additional providers, variations in postoperative pain management among otologists, and patient-specific factors (eg, pain tolerance, comorbidities, and previous opioid use).
Conclusion
The opioid epidemic continues to be an ongoing issue in Canada, and prescription opioid abuse plays a significant role. Although the proportion of people being prescribed opioids decreased from 2013 to 2018 in Canada, the dosage and duration of therapy among people starting opioids remained relatively stable. 26 A growing body of literature indicates overprescribing in surgical specialties.27-29 Our findings provide insights into the prescribing patterns of opioids in Ontario for common otologic surgical procedures with large variations and specific factors that influence higher opioid prescriptions. Otologic surgery is generally expected to have mild to moderate postoperative pain for 2 to 4 days, 12 and postoperative analgesic regimens should reflect the amount of predicted pain. Therefore, improvements to safe prescribing could be achieved by focusing on preoperative counseling regarding expected pain, identification of risk factors for opioid use disorder, and multimodal pain management with nonopioid analgesia to control short-term pain and minimize the adverse effects of opioids.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211045364 – Supplemental material for Opioid Prescriptions Following Otologic Surgery: A Population-Based Study
Supplemental material, sj-docx-1-oto-10.1177_01945998211045364 for Opioid Prescriptions Following Otologic Surgery: A Population-Based Study by Keshinisuthan Kirubalingam, Paul Nguyen, Gregory Klar, Joanna M. Dion, Robert J. Campbell and Jason Atkins Beyea in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
We thank IQVIA Solutions Canada Inc for use of its Drug Information Database. The data set was cut at ICES Queen’s. Data set creation and data analysis were performed at ICES Queen’s by Dr Paul Nguyen.
This article was given as an oral presentation at the Annual Research Grand Rounds, Otolaryngology–Head and Neck Surgery, Queen’s University, March 24, 2021, and at the Charles Sorbie Faculty Research Day, Department of Surgery, Queen’s University, April 9, 2021.
Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information and the Ontario Ministry of Health. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data resources; no endorsement is intended or should be inferred.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.