
Abstract
Objective
Over the last decade there has been a trend toward observation for small nongrowing vestibular schwannoma (VS). Even without tumor growth, patients commonly experience ipsilateral hearing decline, and hearing rehabilitation remains challenging. This study analyzes hearing and speech performance outcomes after cochlear implantation (CI) in observed VS.
Study Design
Retrospective review.
Setting
Tertiary referral center.
Methods
Chart review was used to include patients with observed VS who had undergone ipsilateral CI, pre- and postimplantation audiometry, and speech performance. Tumor size pre- and postimplantation was measured with volumetric analysis.
Results
Seven patients with ipsilateral VS and CI were identified. Preimplantation tumor volume was 0.11 to 1.02 cm3. Five subjects were implanted with a straight electrode and two with a perimodiolar electrode. The average preimplant pure tone average was 91.3 dB (range, 80-117 dB) and 61.2 dB (range, 12-118 dB) for the implanted and nonimplanted ears, respectively. In all subjects with at least 1 year of listening experience (n = 6), consonant-nucleus-consonant word scores improved at 6 months and 1 year in the CI-alone and bimodal listening conditions. AzBio scores in quiet also improved at 6 months and 1 year. Of subjects with serial pre- and postoperative magnetic resonance imaging, volumetric analysis demonstrated no tumor growth.
Conclusion
Our results demonstrate that CI is a successful option for subjects with small nongrowing VS. All subjects had improved performance postimplantation. VS may continue to be observed with serial magnetic resonance imaging given increasing conditionality among CI manufacturers and ability to assess cerebellopontine angle extension despite implant artifact.
Keywords
Vestibular schwannoma (VS) is a benign nerve sheath tumor arising from the inferior or superior vestibular nerves. Management of VS may include surgical resection, stereotactic radiation, and observation with serial imaging. Over the last 2 decades, refinements in microsurgical technique and reduced tolerance for posttreatment cranial neuropathy have led many providers to opt for more conservative treatment strategies. 1 There has been a trend toward subtotal and near-total resection to reduce the risk of facial nerve dysfunction in surgical patients, and a greater proportion of patients are undergoing a period of initial observation to determine tumor growth trajectory.2-4
The majority of patients with a VS are symptomatic, with many experiencing hearing impairment on the affected side. 5 Even in patients who demonstrate minimal or no change in tumor size on serial magnetic resonance imaging (MRI), ipsilateral hearing may decline with time, particularly when hearing loss is present at diagnosis.5,6 Hearing rehabilitation in the presence of VS remains challenging, particularly in patients with unilateral severe to profound hearing loss. Historically, options for rehabilitating single-sided deafness (SSD) have been limited to bone-anchored hearing implant or a hearing aid that routes sound to the contralateral ear (contralateral routing of signals). In July 2019 cochlear implantation was approved by the US Food and Drug Administration (FDA) for treatment of SSD, which has in turn helped broaden access to implantation for patients with VS and ipsilateral hearing loss.
Cochlear implantation has been shown to be significantly beneficial for patients with SSD through improved speech understanding in complex environments, sound localization, and quality of life.7,8 Multiple studies have also demonstrated improved speech recognition after ipsilateral CI in SSD, superior to untreated or rerouting amplification.8-10
Multiple studies have shown improved speech performance following CI in patients with VS, although these studies were limited to patients who received radiation therapy or prior microsurgical resection.11-13 To date no studies have exclusively analyzed speech performance outcomes after ipsilateral CI in patients with untreated VS. In addition, CI in the setting of ipsilateral VS, a retrocochlear pathology, is performed outside the current FDA criteria for implantation. The purpose of this study is to describe speech performance outcomes in patients at our institution who have undergone CI in the setting of nongrowing VS and secondarily to evaluate the feasibility and utility of MRI volumetric analysis to follow tumor size before and after CI.
Methods
Following Vanderbilt University Institutional Review Board approval (181441), retrospective chart review was used to identify a cohort of adult patients with a diagnosis of VS who, at the time of analysis, had been managed with observation alone. Further chart review was used to identify those who had also undergone ipsilateral CI without prior surgical resection or stereotactic radiation. Seven patients met these inclusion criteria. Exclusion criteria included contralateral CI and prior surgical resection or radiation.
Retrospective chart review was used to identify demographic information, electrode type, audiometric performance, pre- and postoperative speech performance outcomes, tumor size, and number of pre- and postoperative MRI studies. Postimplantation outcomes were recorded at 1, 3, 6, and 12 months.
Volumetric analysis was measured with the institutional radiology platform IMPAX (AGFA Healthcare). Slice-by-slice manual segmentation of the tumor was performed to determine tumor volume and maximum linear dimension. Lack of tumor growth was confirmed on least 2 preoperative MRI scans where available in the electronic medical record.
All testing was completed with recorded stimuli at 60 dB SPL, presented via a single loud speaker at 0° azimuth 1 m from the listener. Monosyllabic word recognition performance was assessed with one 50-item list of the consonant-nucleus-consonant (CNC) test. 14 An AzBio sentence recognition test was used to assess speech recognition in noise. 15 Preoperatively, all patients were tested with each hearing aid alone as well as with bilateral hearing aids. All hearing aids had been verified to match to NAL-NL2 target audibility for speech at 60 dB SPL.
Results
Seven patients met final inclusion criteria. Demographic information is listed in Table 1 . Patients were implanted with all 3 manufacturers: Advanced Bionics, MED-EL, and Cochlear. Full electrode insertion was achieved in all patients. Preimplantation tumor volume ranged from 0.11 to 1.02 cm3. Five subjects were implanted with a straight electrode and 2 with a perimodiolar electrode. One patient had bilateral vestibular schwannoma associated with neurofibromatosis 2 (NF2). None of the patients had tumor extension into the cochlea or vestibule, while 2 had extension into the cerebellopontine angle. The mean preimplantation pure tone average was 91.3 dB (range, 80-117 dB) and 61.2 dB (range, 12-118 dB) for the implanted and nonimplant ears, respectively. One patient had bilateral profound hearing loss with unmeasurable preoperative pure tone average.
Patient Demographics.
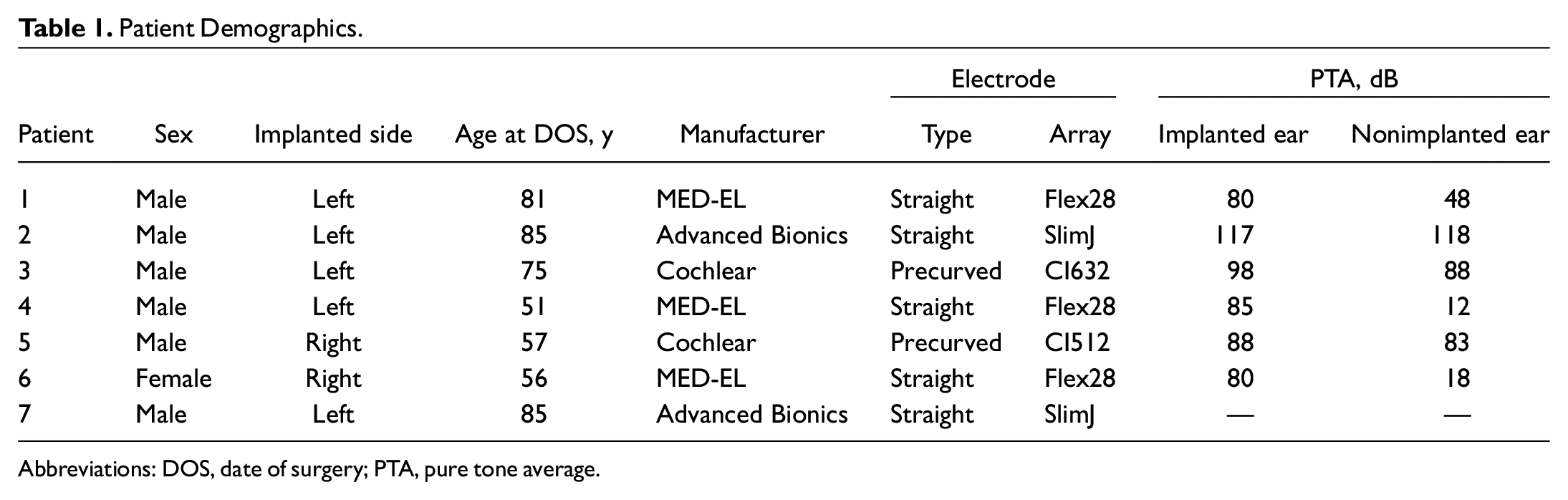
Abbreviations: DOS, date of surgery; PTA, pure tone average.
All patients had improved CNC monosyllabic word recognition following implantation in the CI-alone listening condition ( Table 2 ). Individual trajectories in CNC word score improvement are presented in Figure 1 . The mean preimplantation CNC word score was 6% (range, 0%-22%) and by 6 months improved to 55% (range, 39%-72%; n = 5). At 12 months, patients demonstrated stable improvement with an average CNC monosyllabic word score of 55% in the CI-alone listening condition (range, 36%-88%; n = 6). Average improvement in CNC word score preimplantation to 12 months postimplantation was 49% (range, 24%-88%). One patient did not have 12-month postoperative scores available due to lack of follow-up; this individual did have an improvement of 32% in CNC word score at 1 month in the CI-alone listening condition. Two patients had CNC word scores available in the binaural condition and showed improvements of 20% and 66% at 12 months postimplantation.
Percentage Correct Pre- and Postoperative Consonant-Nucleus-Consonant Word Scores. a
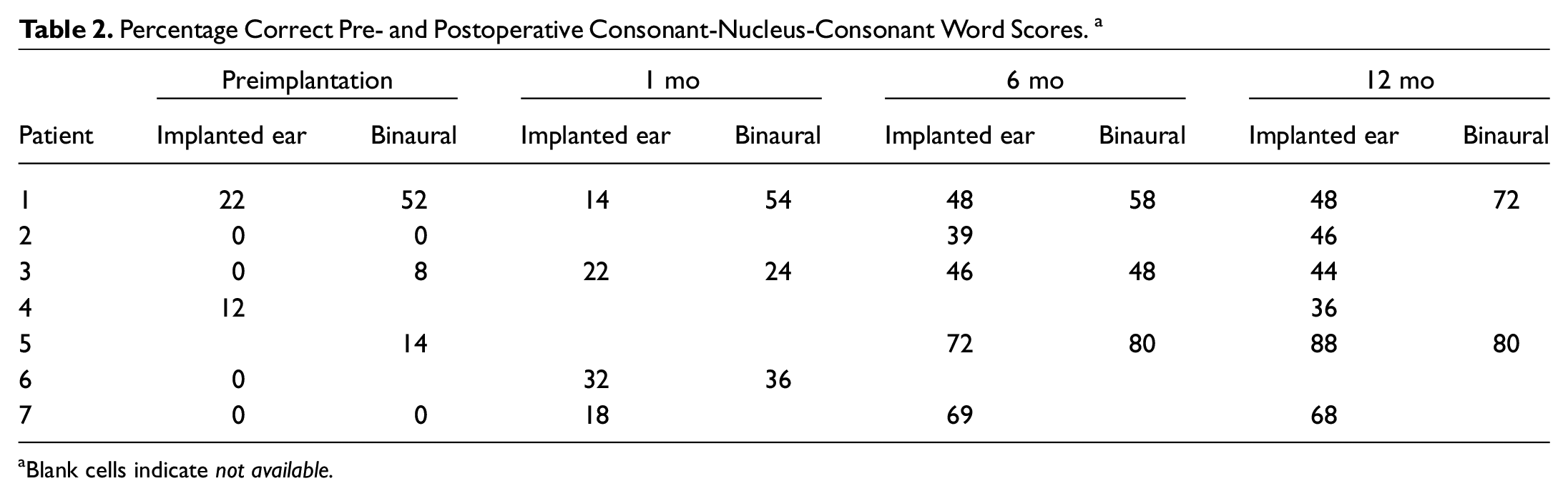
Blank cells indicate not available.
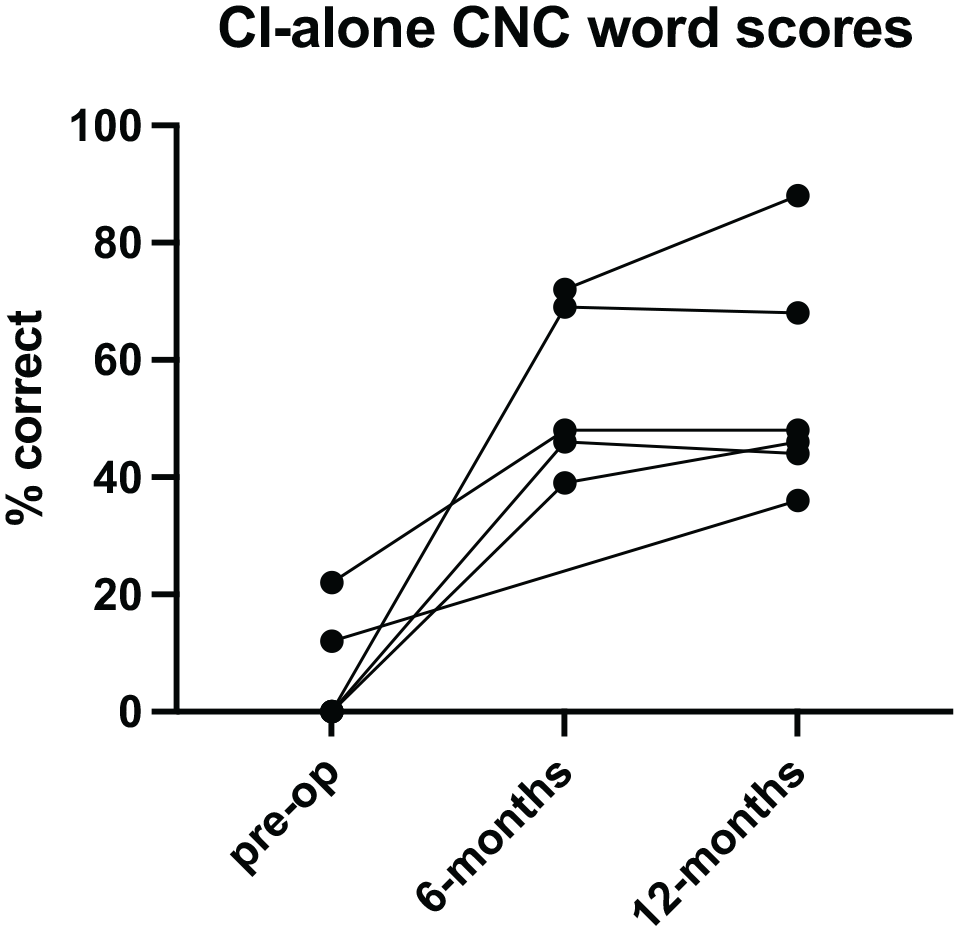
Cochlear implantation–alone consonant-nucleus-consonant word scores.
Patients demonstrated similar improvement in AzBio scores in quiet ( Table 3 ). Individual trajectories in AzBio score improvement are presented in Figure 2 . Mean 6-month performance in AzBio sentences in quiet improved to 56% (range, 40%-86%; n = 5) from 9% preimplantation in the CI-alone listening condition (range, 0%-33%; n = 7). Patients exhibited stable improvement at 12 months, with a mean performance of 56% (range, 44%-87%; n = 6) and an average improvement of 45% when compared with preimplantation testing (range, 23%-80%; n = 6). The 2 patients who were tested in the binaural listening condition at 12 months had improvement of 38% and 48%.
Percentage Correct Pre- and Postoperative AzBio Sentence Scores in Quiet.
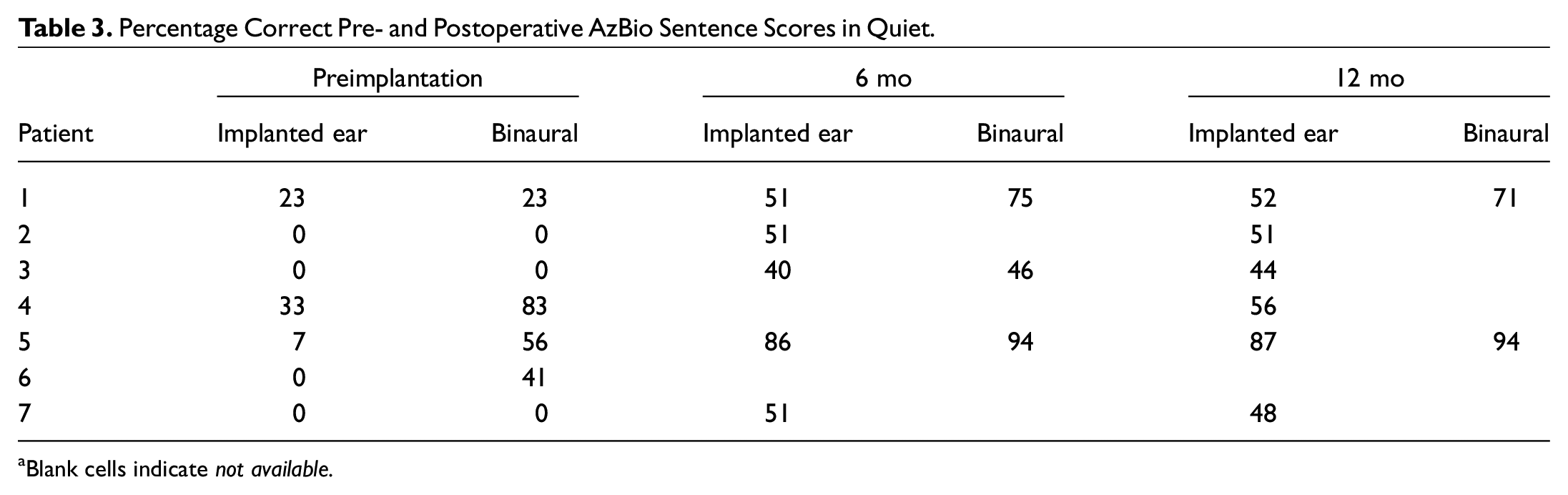
Blank cells indicate not available.
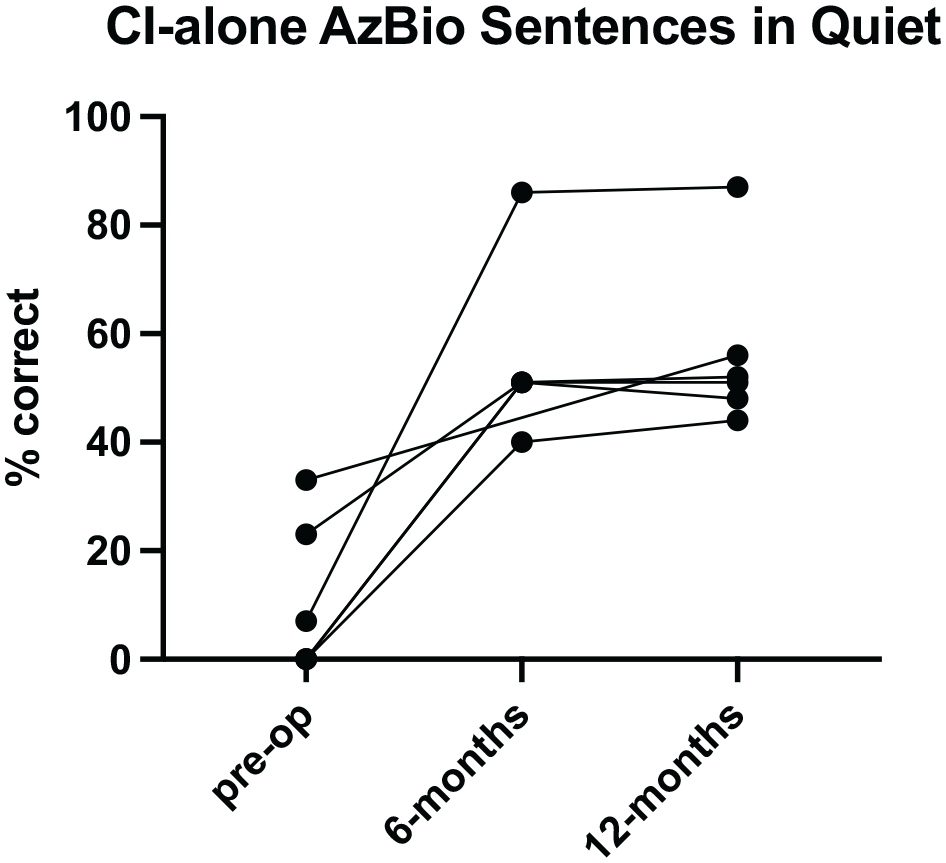
Cochlear implantation–alone AzBio sentences in quiet.
Lack of tumor growth was confirmed by at least 2 preimplantation MRI scans in 4 patients. One patient’s preoperative imaging was not stored in the electronic medical record imaging library and thus was not available for retrospective analysis. Patients were observed for a range of 2 months to 7 years at this institution prior to implantation. Of subjects with serial pre- and postimplantation MRI, volumetric analysis demonstrated lack of tumor growth ( Table 4 ). Length of imaging follow-up in these patients ranged from 1 to 3 years. Despite implant artifact, volumetric analysis remained feasible in surveillance of VS.
Pre- and Postoperative Magnetic Resonance Imaging Volumetric Analysis. a
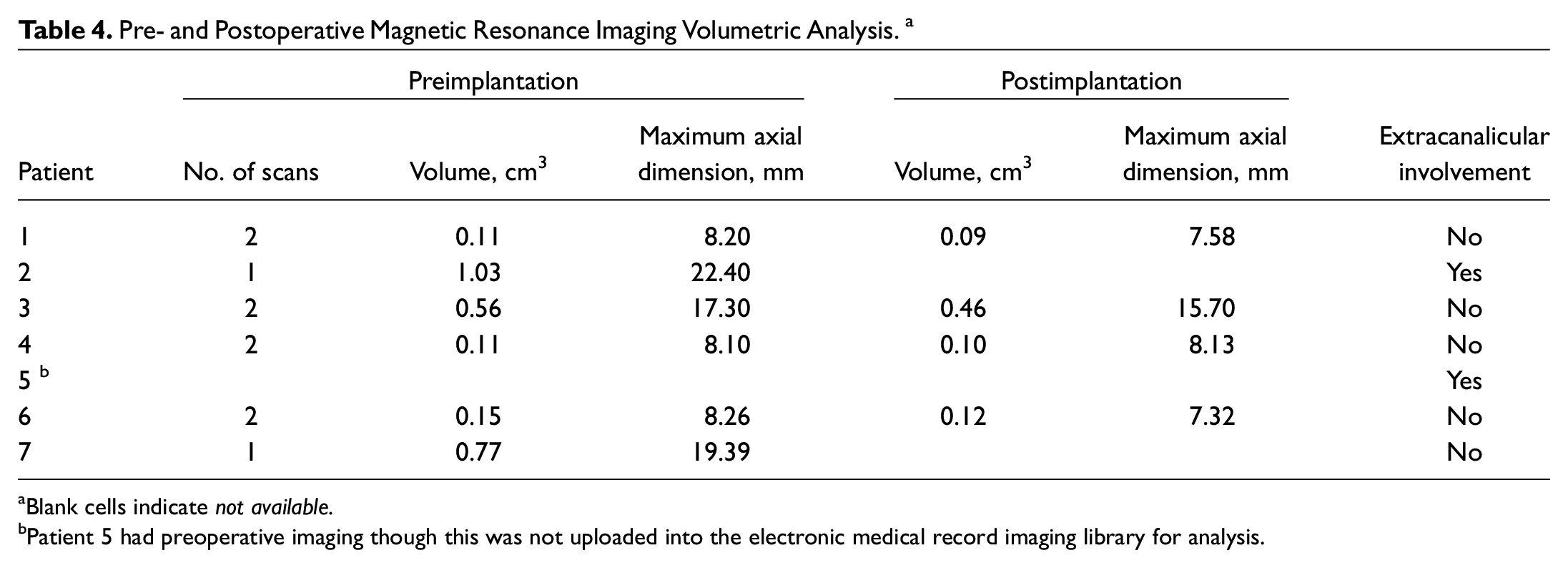
Blank cells indicate not available.
Patient 5 had preoperative imaging though this was not uploaded into the electronic medical record imaging library for analysis.
Discussion
Over recent decades the observed incidence of VS has increased considerably. Increased access to MRI and standardized protocols for asymmetric hearing loss have led to more frequent detection of small, incidentally diagnosed tumors.16,17 Over the past 2 decades, management of VS has shifted toward more conservative management. 1 The FDA’s approval of CI for treatment of SSD is currently exclusive of SSD in the setting of VS; however, there is a pressing need to better understand hearing rehabilitation options, including CI, for management of hearing loss in patients with untreated VS. In the present study we found that speech performance was consistently improved in patients with untreated VS meeting audiometric criteria for ipsilateral implantation.
Existing studies of CI outcomes in VS are limited in number and sample size, particularly with respect to patients with untreated VS. The majority of studies focus on patients who have received prior SRS or microsurgical resection. Bartindale et al reported a systematic review of 15 studies, which included 45 patients with radiated, excised, or observed VS. All patients in this review, including those with observed (untreated) VS, demonstrated improvement in speech discrimination score (average improvement from 30% to 54%), which did not appear to be influenced by prior treatment. 12 Urban et al described improved sentence scores in 7 patients with ipsilateral implantation who were either observed (n = 2) or underwent previous radiation (n = 5); however, only postoperative data were reported. 11
Although the literature citing outcomes of ipsilateral CI in observed VS is limited, previous studies have noted the success of CI in patients with NF2. These reports have shown improved postoperative speech outcomes.18-20 Borsetto et al conducted a systematic review of 50 patients from 12 studies comparing speech performance outcomes following CI in observed (n = 21) versus radiated (n = 29) VS, largely in patients with NF2. This study showed similar improvements in pure tone average and speech discrimination between the groups. 21 This review included 5 patients with sporadic ipsilateral disease, 2 of whom were observed. Given the predilection to bilateral VS in NF2, these studies are useful when considering cochlear implantation in the challenging setting of hearing rehabilitation in the patient with NF2.
Tumor Surveillance
In a recent study, Lees et al showed that a majority of VS tumors demonstrate early growth (68%) within the first years of diagnosis, defined as at least a 20% increase in size on volumetric analysis. 22 A smaller proportion (4%-8%) may exhibit delayed growth up to 11 years after diagnosis. 23 These findings highlight the importance of early and long-term surveillance of tumor size, which must be considered prior to CI.
Historically there have been challenges with surveillance imaging of VS in the setting of prior CI due to implant artifact. For CI to be considered a reasonable and safe method for hearing rehabilitation, one must be able to thoroughly evaluate the internal auditory canal (IAC) on MRI. These challenges have been mitigated with advancements in implant and imaging technology in recent years. Since 2019, all FDA-approved receiver-stimulators are now manufactured to be MRI conditional to 3.0 T without a head wrap. Todt et al showed that it is possible to evaluate the IAC and utilize surveillance MRI in patients after VS resection with 3.0-T MRI sequencing, particularly with optimal positioning of the receiver-stimulator to minimize the effect of artifact. 24 All patients in this study were implanted with a Cochlear 512 electrode. Walton et al analyzed 76 MRI scans from 13 subjects with NF2 and found that analysis of the ipsilateral cerebellopontine angle and IAC was unaffected in 85% of scans and subjectively severely impaired (classified as “view obscured”) in just 2% of scans. 25
Treatment Postimplantation
An additional scenario meriting discussion is the postimplantation patient who ultimately requires radiation for treatment of growing and/or symptomatic VS. While imaging to observe tumor size and extension may be feasible, more detailed stereotactic radiation planning can be more difficult due to implant artifact. There are no data regarding outcomes in this small patient population, and further investigation may be warranted.
For similar reasons, some patients may undergo surgery to resect VS after implantation. If surgery is needed, some data suggest that the implant may be used for intraoperative auditory brainstem response and neural response imaging for cochlear nerve monitoring. This technique has been suggested to best preserve the cochlear nerve during tumor resection for continued successful implant use.26,27
The present report is unique in reviewing hearing outcomes only in patients with observed VS. Our findings have bolstered our confidence in the feasibility of serial imaging for patients with VS and ipsilateral CI. Furthermore, hearing outcomes in this patient population have been favorable. As our length of follow-up and experience with this strategy continue to grow, we hope to refine our algorithms for the selection of appropriate candidates and to better characterize the long-term outcomes (and potential pitfalls) of this approach.
There are several limitations to consider in interpreting and applying the results from this study. The primary limitation is the sample size due to the few patients with small stable VS who have undergone CI. In addition, many of these patients were recently implanted, and the data reflect early postoperative hearing outcomes. Finally, due to various health care system and patient factors, the COVID-19 pandemic affected follow-up audiology and clinic visits and thus the volume of postimplantation data that were available. As return visits increase and longer-term outcomes are collected, we expect to gain a more refined understanding of the longer-term benefits and disadvantages of this promising treatment strategy.
Conclusion
Our results indicate that CI is a successful option for subjects with a small nongrowing VS. All subjects had improved performance postoperatively. VS may continue to be observed with serial MRI given increasing MRI conditionality among many CI manufacturers and its ability to adequately assess cerebellopontine angle extension despite implant artifact. Given the higher incidence of VS diagnosis, growing trends toward observation, and excellent CI outcomes presented here, we anticipate utilizing CI for hearing rehabilitation in an increasing number of patients in the future.
Footnotes
This article was presented for the AAO-HNSF 2020 Virtual Annual Meeting & OTO Experience; September 13–October 25, 2020.