
Abstract
Objective
To analyze the association of mast cells found on supraglottic biopsy of pediatric patients with common aerodigestive diseases.
Study Design
Cross-sectional study.
Setting
Tertiary care children’s hospital.
Methods
A total of 461 pediatric patients undergoing otolaryngology aerodigestive procedures provided consent between 2014 and 2019, and biopsies of the supraglottic larynx were collected at the time of their surgery. Pathologists reviewed biopsies for the presence and number of mast cells per high-power field. The patients’ electronic health records were reviewed for relevant demographic data and clinical diagnoses present at the time of biopsy. Multivariate logistic regression was used to assess the relationship of mast cells with odds of aerodigestive disease.
Results
Patients with mast cells in their biopsy had significantly higher odds of asthma (odds ratio [OR], 2.02; 95% CI, 1.17-3.46), gastroesophageal reflux disease (OR, 2.36; 95% CI, 1.47-3.77), laryngomalacia (OR, 2.98; 95% CI, 1.80-4.94), laryngeal anomalies (OR, 2.32; 95% CI, 1.52-3.55), and obstructive sleep apnea (OR, 2.16; 95% CI, 1.35-3.45). When mast cells were evaluated as a continuous variable, there was a nonlinear relationship between increasing mast cell count and odds of disease.
Conclusions
Mast cells are known to be associated with inflammatory conditions, though little is known about their presence in laryngeal inflammation. Results from our study demonstrate an association between mast cells in the pediatric larynx and asthma, gastroesophageal reflux disease, laryngomalacia, laryngeal anomalies, and obstructive sleep apnea. Our study also showed a nonlinear relationship between number of mast cells and odds of disease diagnosis.
Keywords
Mast cells are critical in the body’s response to allergic reactions through IgE cross-linking, which leads to cellular degranulation and release of inflammatory mediators. Recent studies have shown that mast cells have effects beyond atopic disorders through an IgE-independent mechanism without degranulation. This mast cell activity, induced by immune and nonimmune factors, may contribute to the development of an array of inflammatory disorders, such as inflammatory arthritis, asthma, coronary artery disease, and chronic dermatitis. 1 Mast cells can be found throughout the body, especially in the airway mucosal lining and digestive system mucosa. They have been implicated in respiratory disorders such as asthma and nasal rhinitis, 2 as well as digestive disorders such as eosinophilic esophagitis, 3 esophageal reflux, 4 and irritable bowel syndrome. 5
The larynx serves as a crucial anatomic connection between the respiratory and digestive tracts, and it is a frequent location of pathology in patients with aerodigestive disease. One previous study documented the presence of mast cells in the supraglottic larynx; however, this study assessed biopsies from asymptomatic patients. 6 In 1 case study, the histology of patients with subglottic and bronchial stenosis demonstrated increased numbers of interstitial mast cells. 7 Mast cells have been implicated in respiratory, digestive, and global inflammatory disorders, but the role of mast cell inflammation within the larynx and subsequent aerodigestive pathology is poorly understood. Understanding the implications of mast cell inflammation within the airway could be important for consideration of therapy targeting mast cells and their inflammatory mediators. There have been no previous studies assessing the correlation of clinical disease with mast cell inflammation within the pediatric larynx.
The use of esophageal biopsy specimens by gastroenterologists in the care of children with aerodigestive disease has been well established and commonly helps guide clinical decision making. With this in mind, otolaryngologists and gastroenterologists at the Aerodigestive Clinic at Vanderbilt Children’s Hospital speculated that laryngeal biopsies may hold similar benefits in clinical decision making and understanding of aerodigestive pathology. Thus, otolaryngologists began collecting biopsy specimens during airway procedures on an array of patients with aerodigestive disease. This study analyzes the association of mast cells found on these supraglottic biopsies with common aerodigestive diseases to better understand the role of mast cell inflammation in the airway.
Methods
This retrospective study received approval by the Vanderbilt Institutional Review Board (exempt; 181455), with a waiver of informed consent granted. Pediatric patients undergoing otolaryngology aerodigestive procedures or airway evaluations were reviewed who had biopsies of the supraglottic larynx collected at the time of surgery between 2014 and 2019. A total of 461 patients were included in the study.
In each patient, biopsies were taken from the superior aspect of the arytenoid—specifically, the soft tissue overlying the corniculate cartilage—with a 3-mm laryngeal biopsy cup. This biopsy location was based on arytenoid mucosal exposure to swallowed and inhaled antigens across the larynx. One biopsy from each of the 461 patients was reviewed for the presence and number of mast cells per high-power field. Early in the study period, mast cells were counted per their characteristics on hematoxylin and eosin stain. Later in the study period, CD117 staining was employed at the discretion of the pathologist to identify mast cells with higher accuracy. If patients had multiple biopsies, their most recent biopsy was selected for inclusion in the study because oftentimes, there was more clinical information on patients at the time of most recent biopsy, which could help us better understand their underlying pathology.
Electronic health records were reviewed for relevant demographic data, medications, comorbidities, feeding method, surgical history, and clinical diagnoses present at the time of biopsy. These diagnoses were gathered per their ICD-10 diagnoses (International Classification of Diseases, Tenth Revision) in the electronic health record prior to the time of biopsy, as well as findings documented in the operation note.
When laryngeal anatomy was assessed, the distinction among normal anatomy, deep notch, and laryngeal cleft incorporated anatomic findings and known status of swallowing function provided by a preoperative videofluoroscopic swallow study. In patients with a normal swallow, a gap between the arytenoids that may have approached the level of the true vocal folds was termed a “deep notch.” In contrast, the same gap in a patient with an abnormal swallow was termed a “laryngeal cleft.” A right-angle laryngeal probe was used to assess the interarytenoid anatomy, placing the bend of the probe against the base of the interarytenoid notch and then determining the “depth” based on the pointed end of the probe. While no standard grading scale was used in these assessments, a probe tip pointing to the false vocal fold was clearly “normal,” while a probe depth pointing to the true vocal fold was clearly “deep” or indicative of a cleft.
Disease prevalence in patients with and without mast cells in their biopsies was compared with Fisher’s exact test Supplemental Appendix (available online). Any disease with a significantly higher prevalence (P < .05) in patients with mast cells in their biopsies was selected for statistical analysis.
Multivariate logistic regression models were made to assess the association between mast cells and the disease diagnoses that were significantly more prevalent in patients with mast cells in their biopsies. These models adjusted for age, sex, prematurity, tube feeding, and medications at the time of biopsy. One set of models assessed odds of disease diagnoses in patients with mast cells present versus absent in biopsies. A second set of models assessed odds of disease diagnoses with mast cells as a continuous variable.
Results
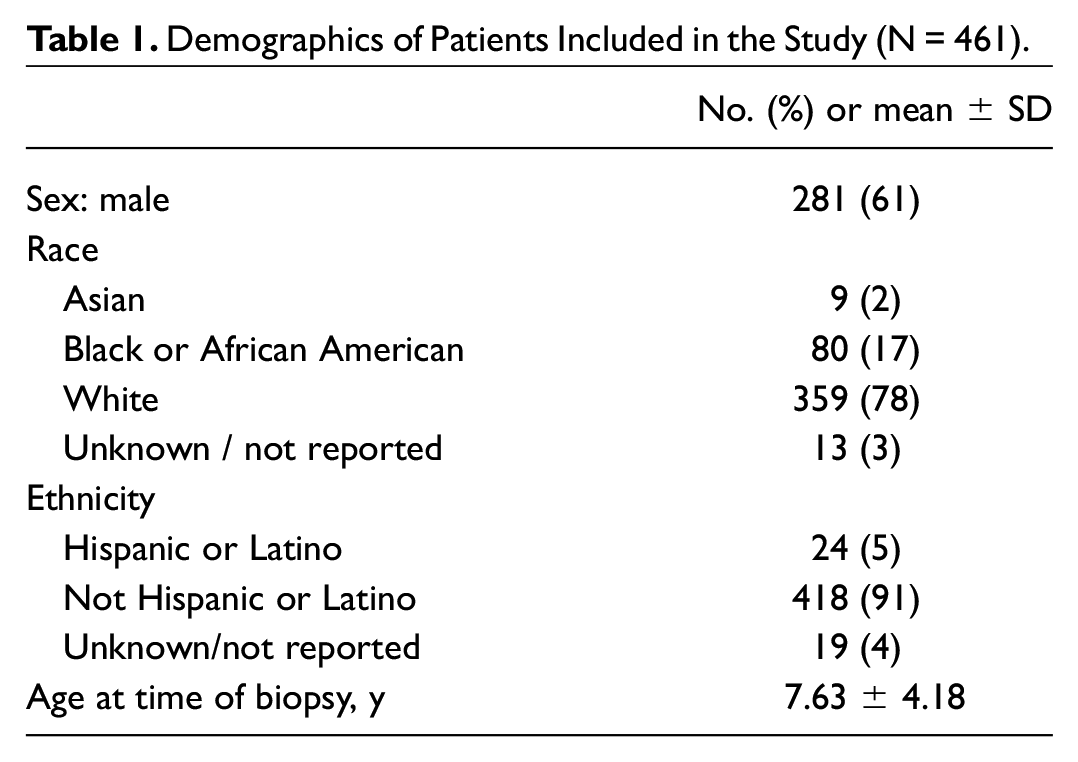
A total of 461 patients and their biopsies were evaluated. These patients ranged from to 3 weeks old to 18 years. There was a higher percentage of males than females included. Demographics of the patients are detailed in Table 1 .
Demographics of Patients Included in the Study (N = 461).
The median number of mast cells in patient biopsies was 1 per high-power field (interquartile range, 0-2). Mast cell count distribution was right skewed ( Figure 1 ). There was a significantly higher prevalence of 5 diseases in patients with mast cells in their biopsy: asthma, gastroesophageal reflux (GERD), obstructive sleep apnea (OSA), laryngomalacia, and laryngeal anomalies ( Table 2 ). Laryngeal anomalies include laryngeal cleft, deep laryngeal notch, laryngomalacia, and laryngeal stenosis.
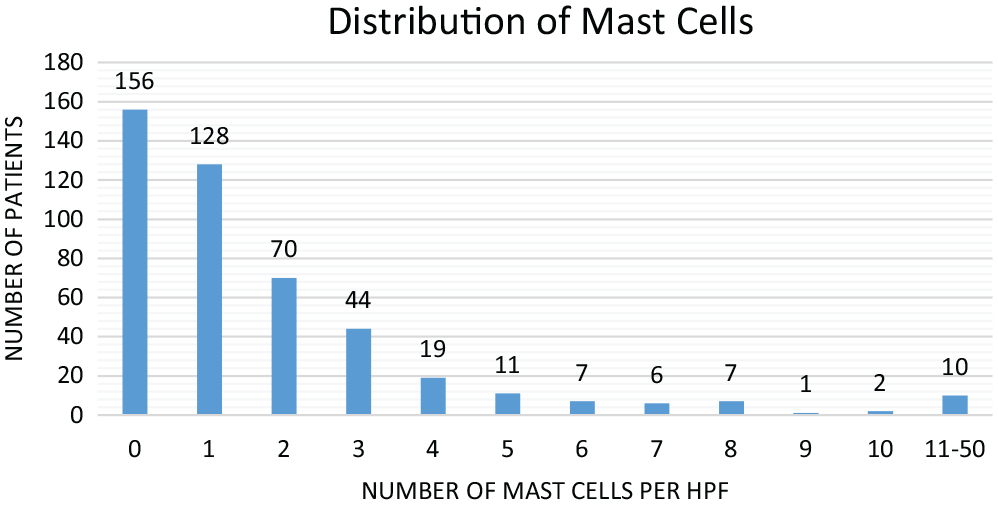
Distribution of mast cells in biopsies had a right-skewed distribution. HPF, high-power field.
Disease Prevalence Between Patients With and Without Mast Cells in Their Laryngeal Biopsies. a
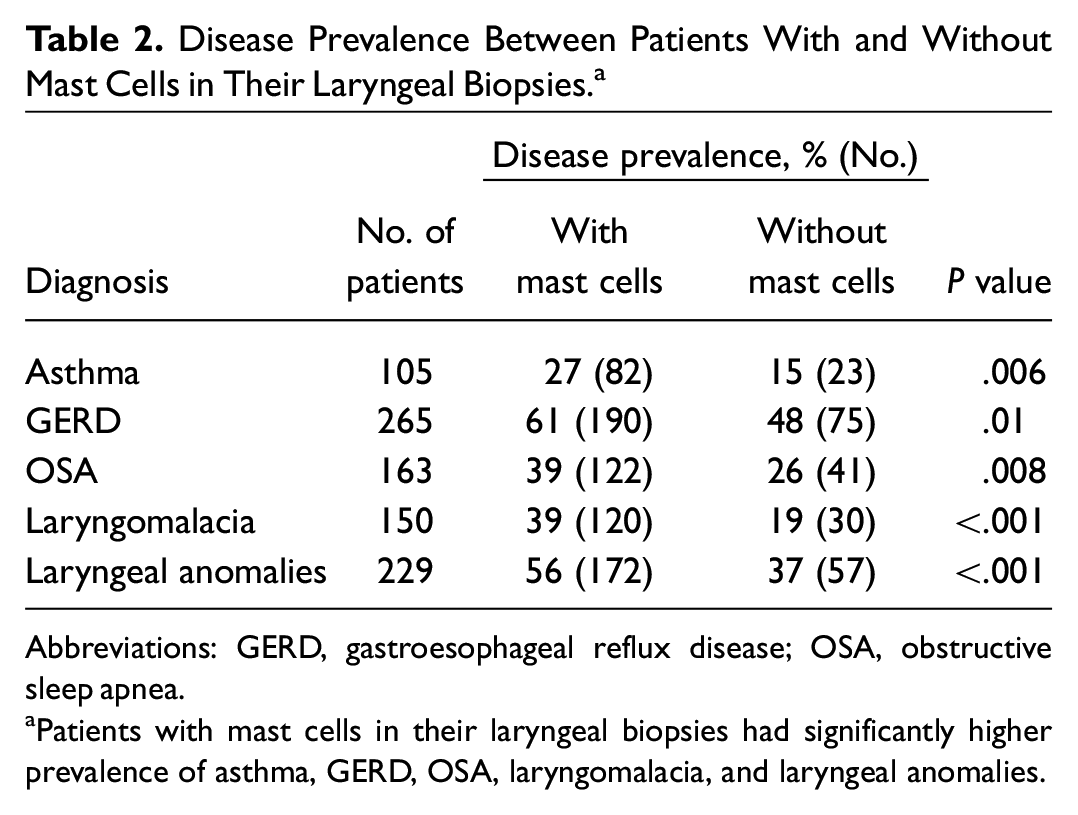
Abbreviations: GERD, gastroesophageal reflux disease; OSA, obstructive sleep apnea.
Patients with mast cells in their laryngeal biopsies had significantly higher prevalence of asthma, GERD, OSA, laryngomalacia, and laryngeal anomalies.
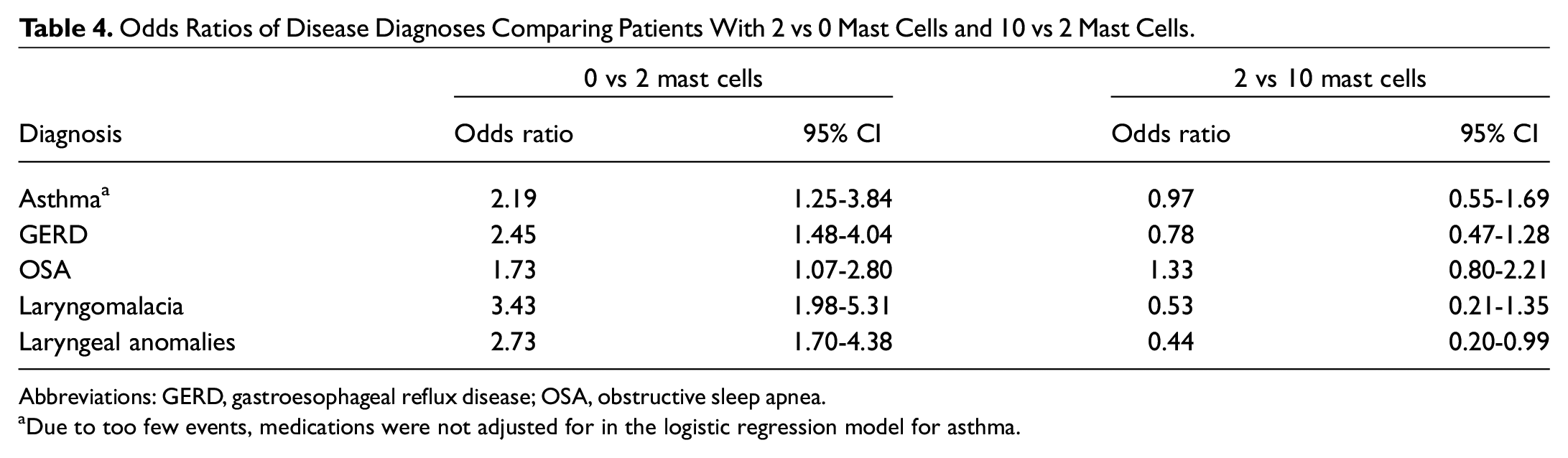
When logistic regression models were made for these 5 disease diagnoses, patients with mast cells present in their biopsies were at significantly higher odds of asthma, GERD, OSA, laryngomalacia, and laryngeal anomalies ( Table 3 ). When logistic regression analysis was made for assessing odds of disease diagnosis with mast cell as a continuous variable ( Figure 2 ), graphs demonstrate a nonlinear relationship between the number of mast cells and odds of disease diagnoses. Table 4 depicts this relationship numerically, comparing odds of disease diagnoses in patients with 2 mast cells per high-power field versus 0 and odds of disease diagnoses in patients with 10 mast cells versus 2.
Odds Ratios of Disease Diagnoses in Patients With vs Without Mast Cells.
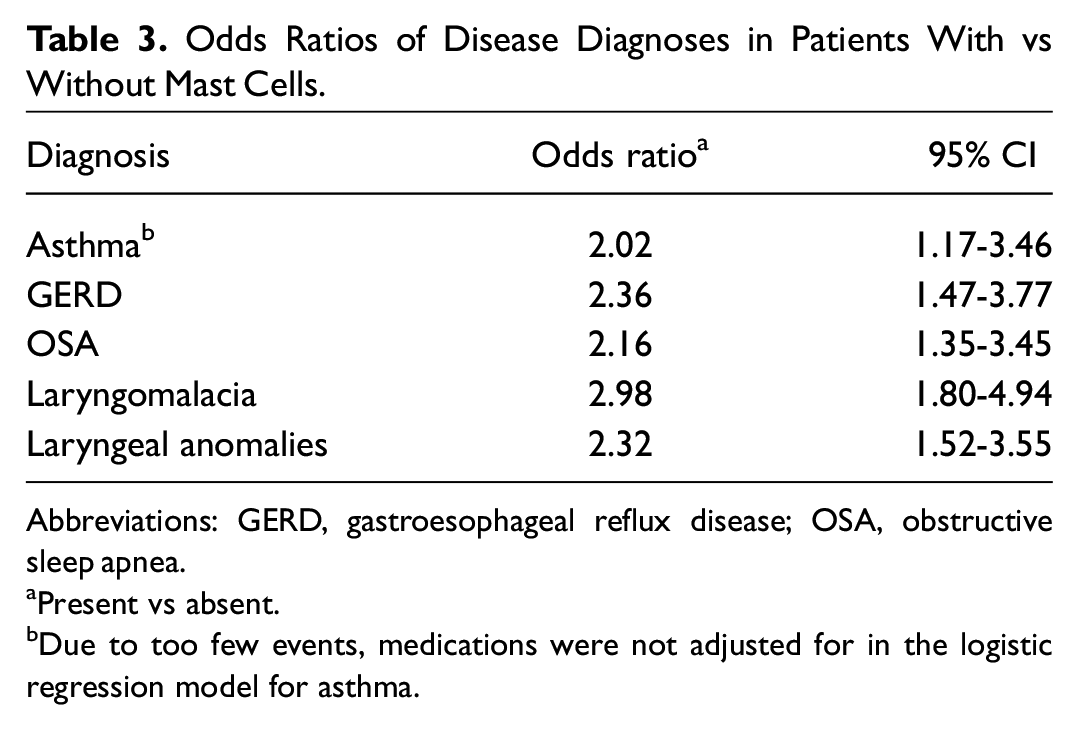
Abbreviations: GERD, gastroesophageal reflux disease; OSA, obstructive sleep apnea.
Present vs absent.
Due to too few events, medications were not adjusted for in the logistic regression model for asthma.
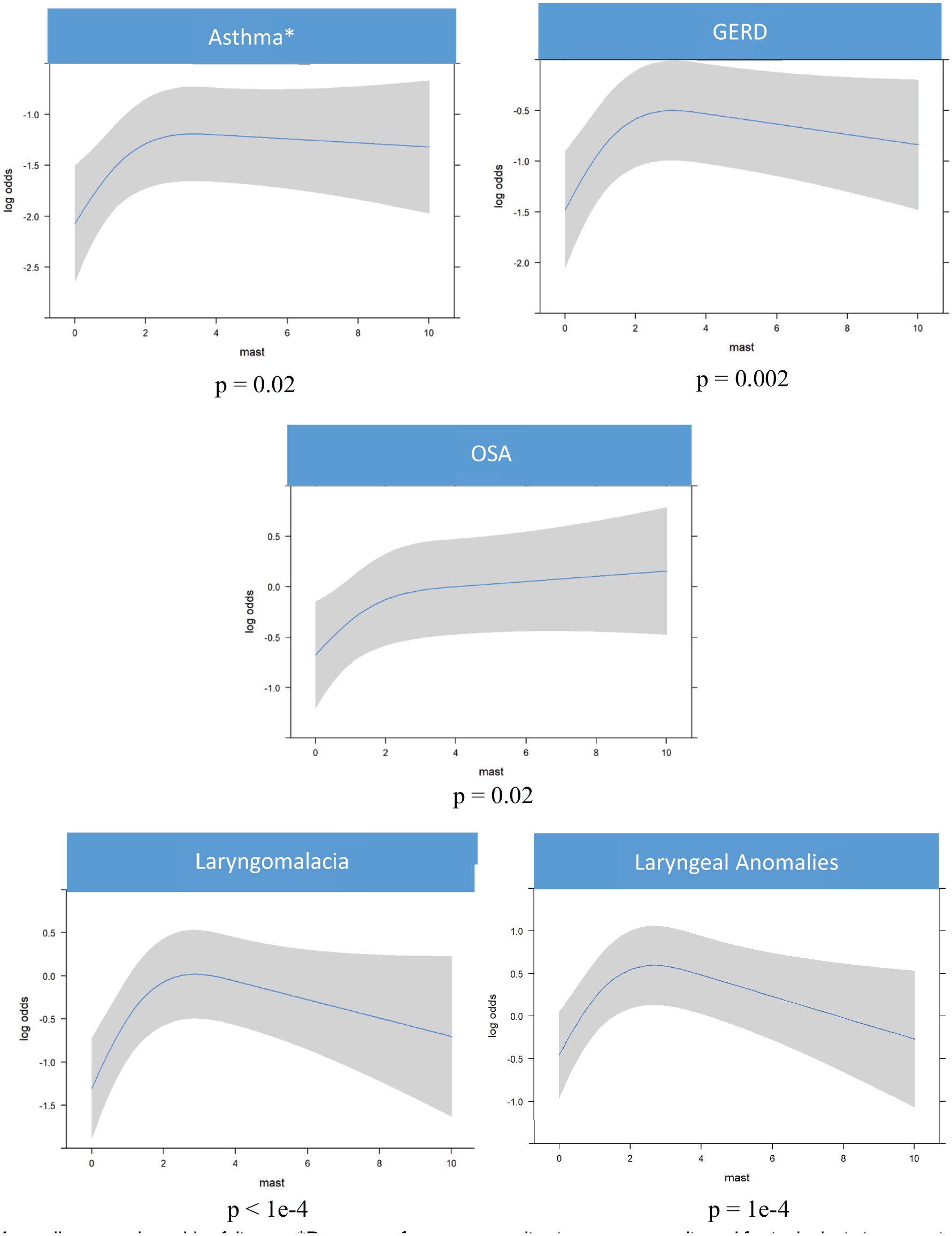
Mast cell count vs log odds of disease. *Due to too few events, medications were not adjusted for in the logistic regression model for asthma. GERD, gastroesophageal reflux disease; OSA, obstructive sleep apnea.
Odds Ratios of Disease Diagnoses Comparing Patients With 2 vs 0 Mast Cells and 10 vs 2 Mast Cells.
Abbreviations: GERD, gastroesophageal reflux disease; OSA, obstructive sleep apnea.
Due to too few events, medications were not adjusted for in the logistic regression model for asthma.
Discussion
The investigation of mast cells in pediatric laryngeal biopsies is a novel concept, so there are no established criteria for pathologic numbers of mast cells. This study helps elucidate the distribution of mast cells found within the pediatric larynx and its clinical significance. Our results indicate that mast cells in the supraglottic larynx have a significant association with asthma, GERD, OSA, laryngomalacia, and laryngeal anomalies. Patients are at significantly higher odds of having these diseases when mast cells are present; however, the true relationship between odds of disease and mast cell count remains unclear. All 5 diseases demonstrate a nonlinear relationship with increasing mast cell count. Odds of asthma, GERD, and OSA appear relatively stable beyond 2 or 3 mast cells per high-power field. This may indicate that impact of mast cell inflammation in these disorders is not dose dependent. Laryngomalacia and laryngeal anomalies have an unexpected decrease in odds as mast cell count increases. However, due to few specimens with high mast cell counts, the odds ratios at high mast cell counts do not reach statistical significance. Ideally, this study serves as the basis of future investigations to determine certain cellular thresholds for laryngeal diagnoses.
The mechanism of mast cell inflammation within the larynx is uncertain, but there are known mast cell inflammatory pathways and mediators that may contribute to airway pathology. Mast cells have profibrotic capabilities via production of proteases, cytokines (especially IL-4 and IL-13), chemokines, and growth factors, which promote fibroblast activity directly or indirectly through activation of additional inflammatory cells, such as T cells, B cells, and neutrophils. Clinically, mast cells have been found in high numbers of various fibrotic lung disorders, such as idiopathic pulmonary fibrosis, chronic hypersensitivity pneumonitis, and sarcoidosis. These mast cells have also had lower numbers of granules and increased tryptase release, suggesting that they may be more active, degranulating more frequently. 8 The number of mast cells found on bronchial alveolar lavage correlates with pulmonary fibrotic disease severity in multiple studies.9-11 In the upper airway, fibroblast dysregulation has recently been implicated in the pathology of idiopathic subglottic stenosis. 12 It is possible that mast cell activation contributes to the inflammatory cascade that orchestrates development of subglottic stenosis and other upper airway pathology. In addition to their promotion of fibrosis, mast cell inflammatory pathways promote edema and cytotoxicity, resulting in physiologic insult.
Mast cells in the distal airway are known to be integral in the pathogenesis of asthma. Previous studies have documented increased numbers of mast cells in smooth muscle and mucous glands of asthmatic airways as compared with the airways of controls.13,14 In pediatric patients, children with frequent severe exacerbations of asthma had higher levels of submucosal and airway smooth muscle mast cells. The number of mast cells in patients with asthma was lower when compared with nonasthmatic controls, but this may be due to the increased degranulation in the former. 15 There are many potential ways that mast cells in airway tissue may contribute to the pathogenesis of asthma—for instance, through influencing mucous gland hyperplasia, mucous gland hypersecretion, and degranulation effects on epithelium. 16 It is hypothesized that mast cells positioned in bronchial epithelium are well suited to propagating an allergenic response to aeroallergens due to their location at the interface of body and environment. 17 Our results have shown that patients with mast cells within the supraglottic larynx are at higher odds of asthma. It is not clear if this could be an extension of inflammation into adjacent tissue as a result of asthmatic reactions or if this reflects that laryngeal tissue is independently primed for mast cell inflammation in patients with asthma.
In comparison with asthma, mast cells do not have a well-demonstrated link to OSA in previously published literature. However, systemic inflammation is a pivotal area of investigation in OSA pathophysiology and its associated morbidity. It is theorized that episodes of hypoxia in patients with OSA may result in increased production of reactive oxygen species and inflammatory cascades, which may contribute to development of cardiovascular disease. 18 In pediatric patients with OSA and sleep-disordered breathing, studies have found significantly elevated levels of serum C-reactive protein, suggestive of a systemic inflammatory state.19,20 Furthermore, a meta-analysis revealed a significant reduction in serum C-reactive protein after adenotonsillectomy in obese and nonobese patients with OSA. 21 However, these previous studies have not made connections between this systemic inflammatory cascade and mast cells inflammation specifically. There may also be a more localized element of increased inflammation within the airway of children with OSA. Studies have shown increased proinflammatory cytokines, TNF-alpha, and IL-6 and highly proliferative T cells in OSA-derived tonsil tissue, as well as increased leukocytes in the uvular mucosa of patients with OSA.22,23 Neither study investigated the presence of mast cells within tonsillar tissue, but our results may indicate an association between mast cells and the inflammatory milieu of OSA due to the increased odds of OSA in patients with mast cells in their biopsies.
The gastrointestinal pathway has been implicated in several disease processes affected by underlying mast cells, including the pathogenesis of esophageal reflux. Patients with nonerosive esophageal reflux have significantly higher levels of mast cells in esophageal mucosa when compared with asymptomatic controls. Additionally, the percentage of degranulated mast cells is significantly higher in patients with esophageal reflux, suggesting that mast cells contribute to the pathogenesis of nonerosive esophageal reflux. 4 Intraepithelial esophageal mast cells may also be useful in understanding the differing pathogenesis and diagnosis of reflux chest pain syndrome versus other phenotypes of esophageal reflux. 24
The association between laryngeal mast cells and GERD demonstrated in our study may be related to extraesophageal manifestations of acid reflux. When acid refluxes into the larynx, oropharynx, and/or nasopharynx, it is considered laryngopharyngeal reflux disease. Although the role of laryngopharyngeal reflux disease is not well understood, it is thought to influence the development of aerodigestive diseases such as laryngomalacia, chronic cough, chronic croup, and recurrent respiratory papillomatosis. It is not clear if reflux is a cause of laryngomalacia or simply presents concurrently. 25 However, there is an 80% to 100% correlation between laryngomalacia and reflux when diagnosed with pH manometry, and patients on acid suppression have had significant improvement of symptoms caused by laryngomalacia.26,27 If mast cell inflammation is related to extraesophageal reflux, this may help explain the association between laryngomalacia/laryngeal anomalies and laryngeal mast cells in our study. Previous investigation of the laryngeal histopathology in patients with laryngomalacia has found intraepithelial eosinophils, basal cell hyperplasia, and intraepithelial inflammatory cell migration, which are all evident in the esophageal mucosa of patients with esophageal reflux. 28 No previous studies have identified an association between mast cell inflammation within the larynx and laryngomalacia.
This study is the first to document and categorize the presence of mast cells in laryngeal mucosa, an important connection between the gastrointestinal and respiratory tract. Strengths of this study include the large sample size as well as the variety of diagnoses documented in the patients. This is the first study that aims to elucidate the implications of an inflamed larynx and cellular factors. This may aid future studies aiming to understand the role of laryngeal inflammation in airway reconstruction failure.
While medications such as cromolyn sodium, corticosteroids and targeted biologics have demonstrated clinical activity against mast cell–mediated disease in other populations, the data set that we present is neither designed nor powered to recommend or refute these treatments in children with elevated mast cell counts in laryngeal biopsies.
There are several limitations to our study and sampling methods. First, biopsies were reviewed by different pathologists and methods of mast cell identification, adding variability to the mast cell count. Additionally, our biopsies indicate a snapshot across a population of children with aerodigestive conditions. Some children with a single biopsy may go on to present disease not yet captured in our data collection. When multiple biopsies were available across time, using the most recent biopsy allowed us to know the most about the child and his or her conditions, and it gave us the opportunity to demonstrate the associations that treatments may have had on mast cell counts. The statistical models used to determine the odds ratio of disease in relation to mast cells controlled for medications taken at the time of biopsy. Furthermore, because biopsies were taken systematically from arytenoid mucosa and mast cell count was determined from 1 slide, there may be patients who have mast cell inflammation present in their larynx that was not captured by the biopsy, resulting in sampling error. We have partnered with our pediatric pathology team to make a more standardized process for future studies. To eliminate this variability of evaluation, future studies may investigate mast cell inflammation with mast cell tryptase to capture the active mast cells, to assess if they are more prominent in patients with more symptoms. It may be beneficial to assess the correlation of histologic mast cell inflammation with the gross appearance of the larynx in future studies. We are also currently evaluating the effect of eosinophil inflammation in this same population to assess the impact of different inflammatory cells.
Another limitation is that disease diagnoses were determined by documentation in the electronic health record at the time of biopsy, rather than by the gold standard of diagnosis. For example, children with GERD had received a clinical diagnosis of reflux, but this may not necessarily have been confirmed with impedance probe testing. While some patients diagnosed with asthma may have formal pulmonary function testing to confirm diagnoses, others were diagnosed by clinical presentation. Diagnosis of OSA was gathered from electronic health record documentation. Some patients may not have had a formal sleep study to confirm this diagnosis.
Although the sample size of the total study is relatively large, the small number of patients with high mast cells counts limits the reliability of the regression model at higher numbers. Last, because the design of this study was cross-sectional, it limits the ability to demonstrate more than an association between mast cells and the various disease diagnoses. Prospective studies are necessary to delineate the exact pathophysiologic mechanism and if there is a causative relationship between mast cells and these disease diagnoses.
Conclusion
The results from our study demonstrate a significant association between mast cells in the pediatric larynx and asthma, GERD, laryngomalacia, laryngeal anomalies, and OSA. Our study also showed a nonlinear relationship between the number of mast cells and the odds of asthma, GERD, laryngomalacia, and laryngeal anomalies, warranting further investigation of this relationship. Future prospective studies are necessary to delineate the pathophysiologic role of mast cells in the larynx within each of these disorders.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211055139 – Supplemental material for Clinical Significance of Mast Cells in the Supraglottic Larynx of Children With Aerodigestive Disease
Supplemental material, sj-docx-1-oto-10.1177_01945998211055139 for Clinical Significance of Mast Cells in the Supraglottic Larynx of Children With Aerodigestive Disease by Emily L. Mace, Shilin Zhao, Brittany Lipscomb, Christopher T. Wootten and Ryan H. Belcher in Otolaryngology–Head and Neck Surgery
Footnotes
This article was presented at the AAO-HNSF 2021 Annual Meeting & OTO Experience; October 3-6, 2021; Los Angeles, California.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.