
Abstract
Objective
The only hypoglossal nerve stimulation (HNS) device available for US clinical use is implanted through 3 incisions. A recently proposed 2-incision modification moved the respiratory sensing lead from the fifth to the second intercostal space to eliminate the third lower chest incision. This study compared perioperative data and therapeutic outcomes between the techniques.
Study Design
Noninferiority cohort analysis of a retrospective and prospective registry study.
Setting
Tertiary care and community surgical centers.
Methods
Patients with obstructive sleep apnea underwent HNS implantation via a modified 2-incision technique (I2). A cohort previously implanted via the standard 3-incision technique (I3) were 1:1 propensity score matched for a noninferiority analysis of postoperative outcomes.
Results
There were 404 I3 patients and 223 I2 patients across 6 participating centers. Operative time decreased from 128.7 minutes (95% CI, 124.5-132.9) in I3 patients to 86.6 minutes (95% CI, 83.7-97.6) in I2 patients (P < .001). Postoperative sleep study data were available for 76 I2 patients who were matched to I3 patients. The change in apnea-hypopnea index between the cohorts was statistically noninferior (a priori noninferiority margin: 7.5 events/h; mean difference, 1.51 [97.5% CI upper bound, 5.86]). There were no significant differences between the cohorts for baseline characteristics, perioperative adverse event rates, or change in Epworth Sleepiness Score (P > .05).
Conclusion
In a multicenter registry, a 2-incision implant technique for a commercially available HNS device had a statistically noninferior therapeutic efficacy profile when compared with the standard 3-incision approach. The 2-incision technique is safe and effective for HNS implantation.
Keywords
Hypoglossal nerve stimulation (HNS) therapy is a novel treatment option for patients with moderate to severe obstructive sleep apnea (OSA) who are unable to effectively use positive airway pressure therapy. 1 Long-term results of the only commercially available HNS device approved by the Food and Drug Administration have demonstrated low perioperative risk and substantial therapy efficacy in >1000 patients.1,2
The standard HNS surgical technique uses 3 incisions, 1 for each implant component, including a lower chest incision for placement of a respiratory sensing lead in the fifth intercostal space. 3 A 2-incision (I2) modified surgical technique was initially explored by 1 author (M.W.), with subsequent adoption, modification, and standardization by a group of surgeons. 4 The modified technique places the respiratory sensing lead transpectorally in the second intercostal space deep to the implantable pulse generator (IPG), eliminating the morbidity of the third lower chest incision. Our group hypothesized that elimination of the third incision and its associated dissection time would decrease operative time without compromising device function, as robust respiratory sensor waveforms are still obtained in this new location. Here we detail perioperative and therapeutic outcomes in a cohort of patients implanted via the I2 technique as compared with the 3-incision (I3) technique, demonstrating that it is faster, has a noninferior therapeutic efficacy profile, and has no statistically significant differences in perioperative adverse event rates.
Methods
Participants
The ADHERE registry (Adherence and Outcome of Upper Airway Stimulation for OSA International Registry) is a multicenter prospective and retrospective international registry of patients with OSA who undergo HNS implantation as part of routine clinical care. It was approved by the ethics committee or institutional review board at each participating center and registered with ClinicalTrials.gov (NCT02907398). Multiple prior publications of ADHERE registry patients who underwent the standard I3 technique have documented HNS safety and efficacy.2,5,6
HNS System
The HNS system (Inspire Medical Systems Inc) consists of 3 components: a stimulating electrode placed on the medial division of the hypoglossal nerve, an IPG, and a respiratory sensing lead placed between the internal and external intercostal muscles. The IPG stimulates select tongue and suprahyoid muscles to protrude the tongue at end expiration, thereby dilating the pharyngeal airway at multiple levels.
Standard I3 Implant Technique
The standard implant technique calls for 3 incisions, generally on the right side: a cervical neck incision for placement of the stimulation electrode on the hypoglossal nerve, a chest incision for placement of the IPG over the pectoralis major muscle in a subcutaneous pocket, and a third incision in the lower lateral chest for placement of the respiratory sensing lead in the fifth intercostal space in the interfascial plane between the internal and external intercostal muscles. The stimulating and sensing leads are tunneled subcutaneously to the IPG pocket. 3
I2 Modified Implant Technique
The I2 implant technique places the stimulation electrode on the hypoglossal nerve in the standard fashion. A detailed procedural description and surgical atlas have been published. 4 The IPG incision is made directly over the second intercostal space, 2 to 3 cm from the sternal margin, to protect against dissection and injury of the pectoralis minor muscle and the medial and lateral pectoral nerves. After formation of the standard IPG pocket over the pectoralis major muscle, the muscle is bluntly dissected to provide access to the second intercostal space. The external intercostal muscle transitions into a thin and fibrous anterior intercostal membrane medially at the sternal margin, so placement of the respiratory sensor medial to lateral ensures that muscle tissue will be present to help anchor the lead in the interfascial plane between the intercostal muscles. Only the stimulation lead requires subcutaneous tunneling to the IPG pocket.
Study Protocol and Timeline
Qualified participants meeting implant criteria underwent HNS device implantation as part of routine clinical care at 1 of the 6 participating sites. All study surgeons had substantial experience with the I3 implant technique prior to adoption of the I2 technique.
The HNS device was activated 1 month after implantation. Participants gradually increased therapy stimulation amplitude to permit accommodation to therapy over time until subjective benefits were perceived. Between 2 and 6 months postoperatively, either an in-laboratory titration polysomnography (PSG) was conducted to optimize and assess therapy efficacy, or a home sleep apnea test (HSAT) was used to assess efficacy at the patient’s current therapy amplitude. Peripheral arterial tomography was considered an acceptable form of HSAT.
ADHERE registry data relating to baseline demographics, clinical history, perioperative experience, and postoperative outcomes were collected after patients provided informed consent. Data were collected prospectively or retrospectively depending on what point a patient was at in the standard clinical care pathway at the time of study enrollment.
Data Analysis
Variable Definitions
The main independent variable was the implantation technique (I3 or I2) used by the operating surgeon. Secondary independent variables used for propensity score matching included baseline body mass index, apnea-hypopnea index (AHI), age, sex, and type of sleep study.
The primary dependent variable was the postoperative AHI. AHIs represented the whole-night average number of respiratory events per hour extracted from the baseline preoperative sleep study and the first postoperative sleep study with HNS therapy for each patient (whether an in-laboratory titration PSG or an HSAT).
Secondary outcomes included operative time, perioperative adverse events, and Epworth Sleepiness Score (ESS). Operative time was defined as the time, in minutes, from the first skin incision until the beginning of wound closure. Perioperative adverse events were divided into major and minor categories. Adverse events were classified as major if they were life-threatening or resulted in postoperative hospitalization, persistent or significant disability/incapacity, permanent impairment of a body function, permanent damage to a body structure, medical or surgical intervention, or death. The ESS is a 24-point patient questionnaire rating sleepiness symptoms, which was collected from patient surveys completed at the preoperative consultation and the last one available postoperatively.
Propensity Score Matching
Patient body mass index, preoperative AHI, age, and sex have been associated with HNS outcomes.2,6,7 Patients from the I2 cohort were therefore propensity score matched on a 1:1 basis with patients within the I3 cohort according to the aforementioned factors, as well as baseline and posttitration sleep study type, to control for confounders of subjective and objective therapy outcomes.
Statistical Analysis
Statistical analyses were designed to test the primary hypothesis that the AHI outcomes of the I2 cohort were noninferior to those of the I3 cohort. Power calculations for noninferiority testing were completed a priori on the basis of existing I3 data in the ADHERE registry, demonstrating a standard deviation of 14.7 events/h for change in AHI from baseline with HNS therapy. With an α of 0.05, power of 80%, and an a priori noninferiority threshold of 7.5 events/h, it was calculated that each cohort required at least 73 patients to test for noninferiority.
Student’s t test, the Wilcoxon rank sum test, and the chi-square test were used to evaluate for demographic and other dependent variable differences between the cohorts, with statistical significance inferred at a P value <.05. All statistical tests were completed in the R statistical programming language (version 4.0.2). 8 Baseline variables are presented in mean ± SD (95% CI) for outcome variables.
Results
A pool of 404 I3 patients enrolled in the ADHERE registry was available across all 6 participating centers. The first I2 implant occurred in September 2019 (M.W.), with subsequent adoption by other surgeons between January and March 2020. No surgeon returned to the I3 technique for any patient after transitioning to the I2 technique. At the time of statistical analysis, 223 patients had undergone I2 HNS implantation and enrolled in the ADHERE database across the 6 centers, with 6-month AHI outcome data available from 76 patients, who were propensity score matched for comparison of postoperative outcomes with 76 I3 patients. There were no significant differences between the matched cohorts in baseline characteristics ( Table 1 ) or the combination of pre- and postoperative sleep study type ( Table 2 ). HSAT was used for postoperative assessment in 51.3% and 46.0% of the matched I3 and I2 cohorts, respectively, with no significant difference in the distribution of sleep study type (P = .63).
Baseline Characteristics of Matched Individuals in the 3- and 2-Incision Surgical Technique Cohorts.
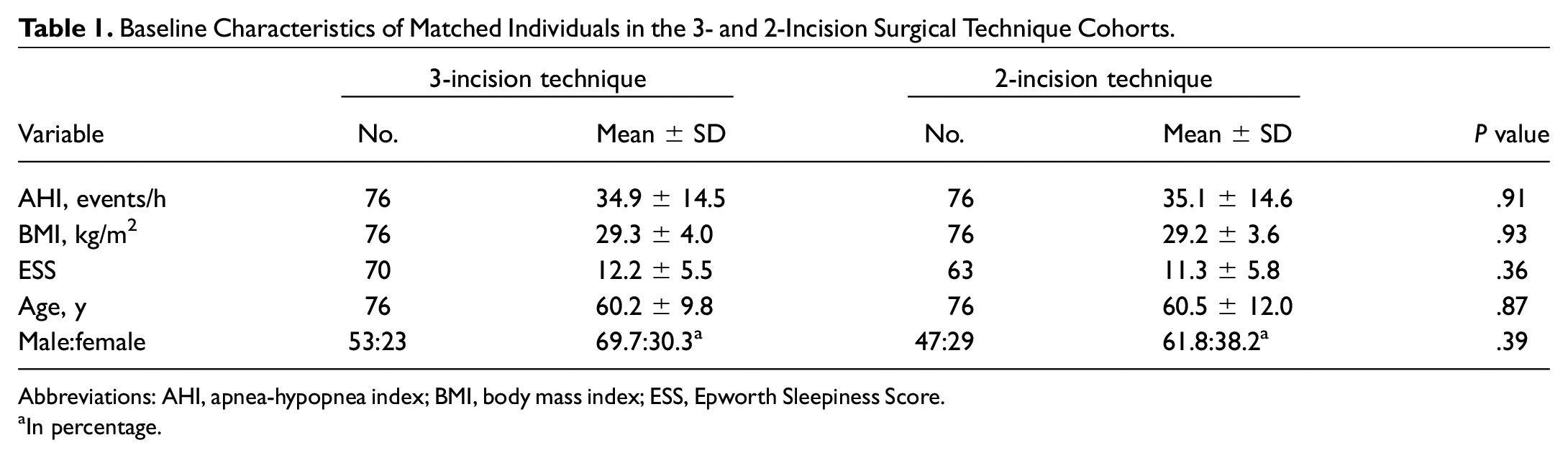
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; ESS, Epworth Sleepiness Score.
In percentage.
Baseline and Postoperative Sleep Study Combinations in the Matched 3- and 2-Incision Surgical Technique Cohorts. a
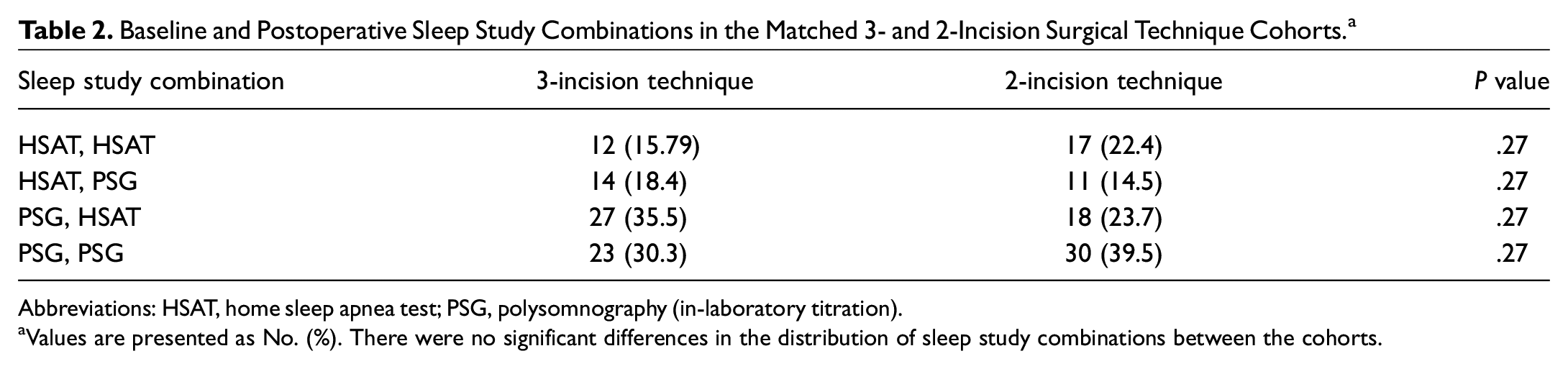
Abbreviations: HSAT, home sleep apnea test; PSG, polysomnography (in-laboratory titration).
Values are presented as No. (%). There were no significant differences in the distribution of sleep study combinations between the cohorts.
Mean operative time decreased from 128.7 minutes (95% CI, 124.5-132.9) across all I3 patients to 86.6 minutes (95% CI, 83.7-97.6) across all I2 patients (P < .001; Figure 1 , Table 3 ). There was no significant difference in perioperative adverse event rates between the cohorts (P > .05). The 2 major adverse events in the I2 cohort were pneumothorax and postoperative bradycardia resulting in overnight hospitalization for observation in separate patients. Mean operative time reduced from 102.3 minutes (95% CI, 95.2-109.3) to 84.5 minutes (95% CI, 78.0-90.9; P < .001) between the last 10 I3 and I2 patients, respectively, for each surgeon. There was a significant difference in operative time between the entire I3 cohort and the last 10 I3 patients for each surgeon (P < .001) but not for the I2 cohort.
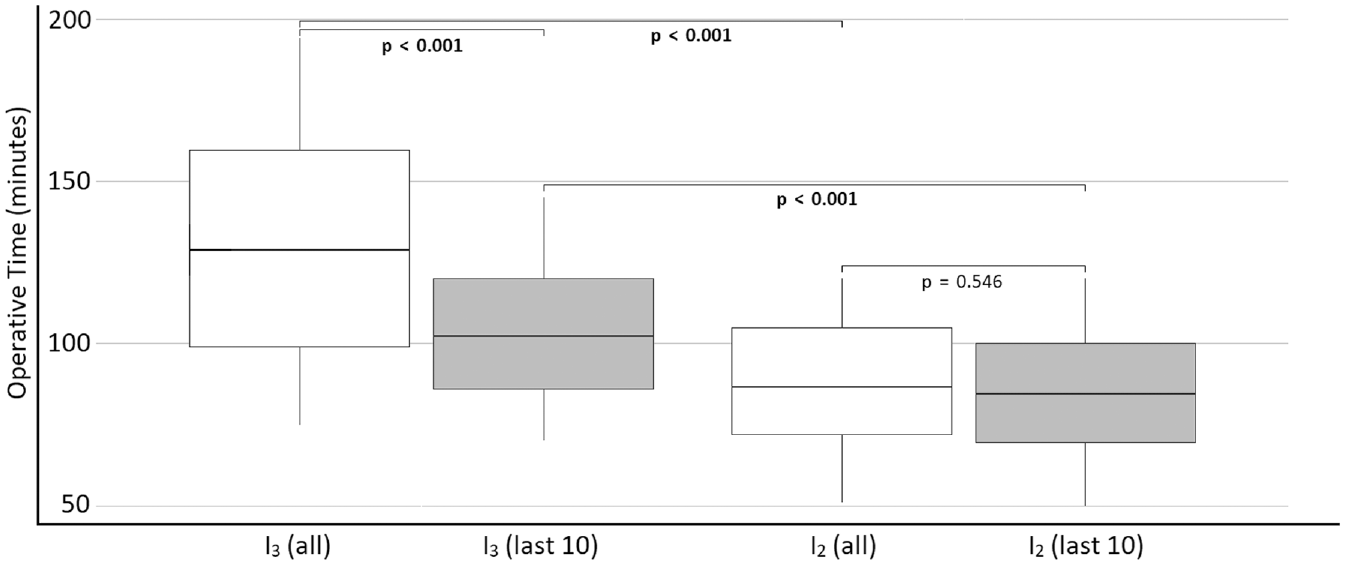
Operative time decreased from 128.7 to 86.6 minutes across the 3- to 2-incision patients, respectively (P < .001). It decreased from 102.3 to 84.5 minutes in the last 10 patients for each surgeon (P < .001). Data are depicted as median (line), interquartile range (box), and 5-95% of the total distribution (whiskers). I2, 2-incision; I3, 3-incision.
Perioperative Outcomes Among All 3- and 2-Incision Surgical Technique Cohorts. a
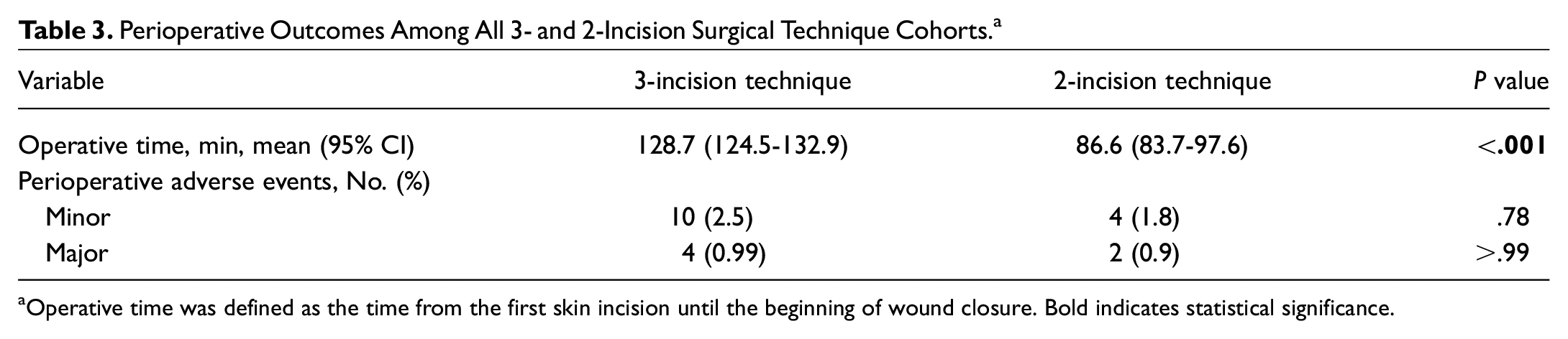
Operative time was defined as the time from the first skin incision until the beginning of wound closure. Bold indicates statistical significance.
Among patients matched for comparison of postoperative outcomes, the mean decrease in AHI was 20.1 events/h (95% CI, 16.2-24.0) in the I3 cohort and 18.6 events/h (95% CI, 15.1-22.1) in the I2 cohort ( Table 4 ), with a statistically noninferior mean difference (1.5 events/h) between them (97.5% CI upper bound, 5.9 events/h; P < .05; Figure 2 ). The mean decrease in ESS between the I3 (4.26 [95% CI, 2.64-5.89]) and I2 (2.7 [95% CI, 1.17-4.23]) cohorts was not significantly different (P > .05). Mean nightly therapy usage was greater in the I2 cohort (7.1 h/night [95% CI, 6.6-7.6]) than the I3 cohort (6.2 h/night [95% CI, 5.7-6.6]; P < .01).
Six-Month Outcomes in the Matched 3- and 2-Incision Surgical Technique Cohorts. a
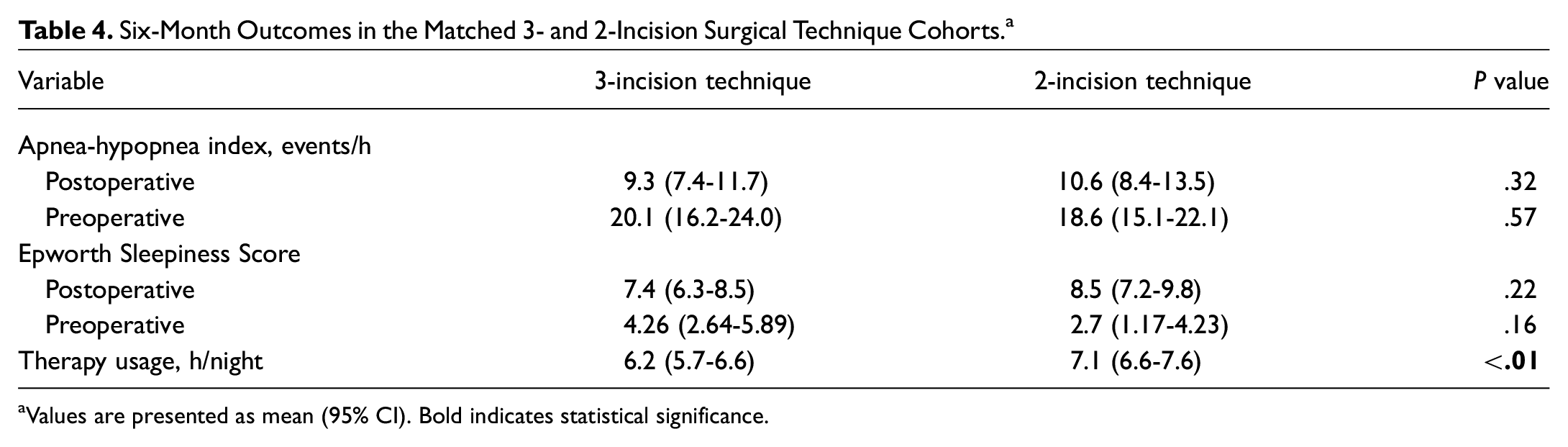
Values are presented as mean (95% CI). Bold indicates statistical significance.

The mean difference in apnea-hypopnea index change (1.51 events/h [diamond]; 97.5% CI upper bound, 5.86 [line]) between the matched surgical cohorts was noninferior (P < .05; equivalence threshold of 7.5 events/h [green area]).
Discussion
This study demonstrated that the I2 technique for HNS device implantation has no significant differences in safety as compared with the I3 technique and has a noninferior therapeutic efficacy profile. Moreover, I2 patients completed surgery 42.1 minutes faster on average than I3 patients and utilized therapy to a greater degree.
HNS AHI outcomes were statistically noninferior between the groups, as expected. The stimulation electrode is placed on the same division of the hypoglossal nerve as in the I3 technique, and validation of appropriate nerve activation and respiratory sensing is a standard component of both intraoperative protocols. We previously reported that respiratory waveforms in the I2 technique initially have greater amplitude than what is typically observed with sensing lead placement in the fifth intercostal space. 4 The HNS automatic gain control dampens this to the expected smooth peaks and valleys within a few minutes during implant validation. In all other aspects, the HNS therapy operation appears identical between the techniques.
I2 patients completed surgery substantially faster than I3. Notably, we found that the operative time of each surgeon’s last 10 I3 patients was also significantly lower than that for the entire I3 cohort. We hypothesize that the difference in the I3 group is due to evolution of the standard surgical technique over time, 3 as well as individual procedural efficiencies achieved by each surgeon. The difference in operative times between the I3 and I2 cohorts most likely arises from the elimination of a third incision and 1 of the 2 lead-tunneling procedures. Although not captured by the reported operative time, all surgeons noted additional time savings during wound closure in the operating room, as the I2 technique requires closure of only 2 incisions instead of 3. Importantly, there were no reports of adverse perioperative events related to pectoralis major muscle dissection, including hematoma, infection, or postoperative weakness suggestive of medial or lateral pectoral nerve injury. The I2 technique requires blunt dissection of the pectoralis major muscle that is not a component of the standard I3 technique. Muscle dissection is technically easy and rapid through cold, blunt dissection, with any bleeding controlled by bipolar electrocautery to minimize the risk of pectoral nerve injury. The reasons for greater therapy utilization in the I2 cohort are not clear but are more likely related to refinements in therapy adjustment protocols over time that better emphasize patient comfort than they are to differences in operative technique.
Although the major and minor perioperative adverse event rates were not statistically different, 1 surgeon did experience an intraoperative pneumothorax on his 39th I2 implant and his 79th implant overall while operating at his local ambulatory surgery center. The surgeon observed air bubbles during interfascial pocket dissection prior to respiratory sensing lead placement, raising concern for pneumothorax. Postoperatively, the patient was hemodynamically stable and maintained normal blood oxygen saturation on supplemental nasal oxygen, but chest x-ray confirmed the presence of a large pneumothorax. The patient was subsequently transferred to the local hospital emergency department where a chest tube was placed by hospital staff. This was removed after a short hospitalization without further complication, and chest x-ray confirmed resolution of the pneumothorax. Having initially seen air bubbles during the interfascial plane dissection, the surgeon attributed the event to an unnecessary degree of dissection when creating a potential space for the respiratory sensing lead. He has subsequently modified his surgical technique to use a minimal amount of interfascial instrumentation, instead using the tip of the respiratory sensing lead to gently auto-dissect its own pocket. This was the only case of pneumothorax that he has experienced using either technique.
Another group recommended against placement of the respiratory sensing lead in a higher intercostal space after a single cadaveric dissection suggested thinner intercostal musculature and the absence of the innermost intercostal muscle in the more superior rib spaces. 9 It should be noted that these authors elected to dissect the third and fourth intercostal spaces lateral to the midclavicular line and deep to both pectoralis muscles. While we acknowledge that the intercostal musculature is typically thinner in the second intercostal space than in the fifth, we posit that our more superomedial dissection is likely safer than the proposed cadaveric modification. Our technique provides for a wider intercostal space and a shallower dissection more medially, as the pectoralis major muscle is thinner medially and the pectoralis minor muscle is in the lateral aspect of the wound. Cautious dissection of the external intercostal muscle layer, with a focus on placement of the respiratory sensing lead superficial to the internal intercostal muscle (instead of deep to an opaque layer of external intercostal muscle), provides for safe and effective surgery. Minimal instrumentation of the interfascial space further protects against inadvertent injury, as evidenced by our substantial volume of I2 implants with no significant difference in perioperative adverse event rates.
Several limitations of this study should be acknowledged. First, all participating surgeons had substantial experience with the I3 technique prior to transitioning to the I2 technique. It is possible that novice surgeons may have a greater risk of intraoperative complication or longer operative times than observed in our group. Nevertheless, all surgeons indicated that the I2 technique is technically easier than the I3 technique, with a shallower and more easily visualized intercostal space approach. We also feel that it is typically easier to monitor the actions of surgical assistants in the second intercostal space dissection and have observed a rapid grasp of the modified technique among our surgical trainees. Second, we used all-night AHI outcomes from postoperative titration PSG as well as HSATs where therapy settings were not adjusted. There are differences in the sensitivity for respiratory events between the testing modalities, 10 and it is possible that some patients in the PSG groups may have had significantly different all-night AHI outcomes if optimal HNS therapy voltages were identified earlier in the night. We controlled for this as best as possible by ensuring that there were no significant differences in the pre- and postoperative combination of sleep study type. Third, we were unable to quantify any difference in perioperative pain, as pain assessments are not collected in the ADHERE database. While we anecdotally thought that postoperative pain in the I2 cohort generally seemed less severe than in the I3 cohort, this observation could be biased, and formal perioperative pain comparisons between the techniques will require further study. Last, this study was powered to detect noninferiority in AHI change between the techniques. Statistical noninferiority in perioperative adverse event rates may be detectable only with a much larger sample size, as the incidence of adverse events in both cohorts is quite low. If a true difference exists, we suggest that surgeons balance this against the decreased intraoperative morbidity from elimination of a third incision and a second lead-tunneling procedure. Moreover, the decreased anesthesia time may benefit a patient population at increased risk for perioperative morbidity due to its underlying OSA. 11
This study documents the surgical outcomes of 6 experienced surgeons with HNS implantation via a modified I2 technique. Further studies are needed to assess outcomes in the wider surgical community. Nevertheless, our data suggest that the I2 technique can be easily adopted, providing patients receiving HNS therapy with faster operative times and an equivalent surgical risk and therapeutic efficacy profile.