
Abstract
Objective
Acute mastoiditis is commonly attributed to infection. Rarely do clinicians encounter cases that do not respond to traditional antibiotics or surgical management. The goal of this study was to systematically review the literature to characterize diseases masquerading as acute infectious mastoiditis.
Data Sources
PubMed, Embase, and Scopus.
Review Methods
A systematic review was performed to identify all publications that reported on diseases with presentations mimicking acute mastoiditis, defined as postauricular redness, swelling, and tenderness. We included clinical prospective studies, retrospective studies, and case series/reports. Exclusion criteria included non-English articles, letters/commentaries, abstracts, and review articles.
Results
Out of 3339 results, 35 studies met final inclusion criteria. In children, 11 diseases were reported to mimic mastoiditis, including solid tumors, hematologic diseases, and autoimmune/inflammatory diseases. The most common disease in children was Langerhans cell histiocytosis, followed by rhabdomyosarcoma and acute myelogenous leukemia. In adults, 8 additional diseases were reported. The most common disease in adults was squamous cell carcinoma, followed by nasopharyngeal carcinoma and Langerhans cell histiocytosis. Presenting symptoms are reviewed, as well as characteristic radiographic, laboratory, and intraoperative features that may assist with diagnosis. A diagnostic algorithm for atypical cases of acute mastoiditis is proposed.
Conclusion
A small but significant group of diseases in children and adults can mimic acute mastoiditis. In such cases, history and examination alone may be insufficient to reach a diagnosis, and further investigation may be necessary. Otolaryngologists should always be mindful of the possibility that noninfectious pathologies may present with a constellation of symptoms similar to mastoiditis.
Acute mastoiditis (AM) is a suppurative infection of the mastoid air cells and most commonly results as a complication of acute otitis media. 1 Early symptoms include fever, otalgia, and otorrhea. As infection and inflammation spread, the breakdown of bony septae leads to coalescent mastoiditis with postauricular erythema, swelling, and tenderness. Diagnosis of AM is clinical, and widely accepted criteria include the presence of these aforementioned examination findings. 2
Most cases of AM can be attributed to infectious causes. However, otolaryngologists may be challenged by atypical cases that do not respond to antibiotics or surgical debridement. Scattered reports in the literature have shown that noninfectious diseases may present with a constellation of findings similar to those of a “hot” mastoid. In 2020, Beghdad et al described a 3-year-old girl presenting with fever, retroauricular swelling, facial weakness, and otorrhea who was originally diagnosed with AM. She was later found to have embryonal rhabdomyosarcoma (RMS) during mastoidectomy. 3 In a 4-year-old boy presenting with 2 months of postauricular swelling and otorrhea, mastoidectomy was performed for presumed mastoiditis; intraoperatively, a pale yellow mass was found filling his mastoid cavity and eroding into the bony sigmoid sinus plate. This fleshy mass was biopsied and found to be liposarcoma. 4 In adults as well, postauricular erythema, swelling, and tenderness can all be the presenting signs for a variety of noninfectious diseases. Failure to consider these alternatives may delay proper diagnosis and treatment.
Currently, the literature lacks consolidated data on the identity or frequency of reports on diseases that mimic AM. The purpose of this systematic review was to identify and organize such diseases into an organizational framework; review unique clinical, diagnostic, and intraoperative features; and provide a diagnostic algorithm to guide clinicians when presented with atypical cases.
Materials and Methods
This study was exempt by the Mount Sinai Program Institutional Review Board. We performed a systematic review according to PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses). 5 In consultation with an expert librarian, a database search was performed in PubMed, Embase, and Scopus with MeSH terms (“mastoiditis” OR “mastoiditides” OR “otomastoiditis”) without limits on date or language. These keywords were chosen and connected with the Boolean term “OR” to maintain broad criteria. The goal of this search was to identify all publications that reported on diseases with clinical presentations that mimicked AM, defined as postauricular erythema, swelling, and tenderness. The search algorithm is presented in Appendix A (available online).
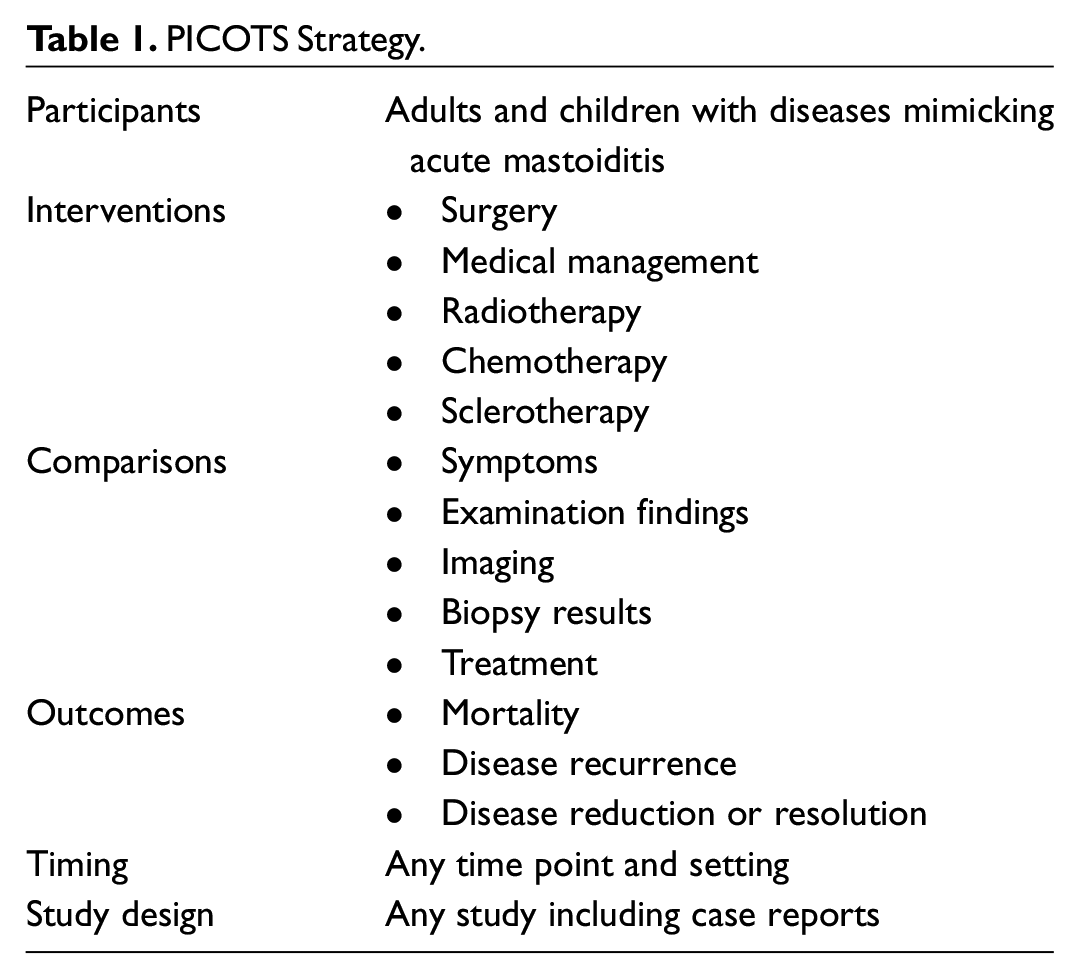
We included clinical prospective and retrospective studies, experimental research, and case series/reports. Studies were excluded if they reported on diseases limited to “radiographic mastoiditis” without physical examination features or on cholesteatoma, where frequent overlaps were anticipated. We excluded letters/commentaries and review articles. Two authors independently performed the initial review of the literature. Full-text articles were obtained for (1) abstracts that met inclusion criteria, (2) abstracts that did not provide sufficient information to make a screening decision, and (3) abstracts with reviewer disagreement. A description of the PICOTS strategy (participants, interventions, comparisons, outcomes, timing, and study design) relevant to this review is presented in Table 1 . All authors approved the final data set.
PICOTS Strategy.
Assessment of Bias
Studies were anticipated to involve nonrandomized studies without control groups (ie, case reports and series); therefore, publication bias was assessed via the Quality Assessment Tool (National Institutes of Health). 6
Data Collection
Bibliometric data were obtained on study title, country, publication year, publication journal, and study design. Level of evidence was determined per standard definitions. 7 Specific data collected from each article were as follows: diagnosis, number of subjects, age, symptoms, length of symptoms, examination features, laboratory and imaging findings, biopsy and immunohistochemistry (IHC) results, intraoperative findings, treatment, and outcomes.
Quantitative Synthesis
A quantitative synthesis was performed with pooled samples to compare diagnostic and treatment approaches to mastoiditis mimickers. Given the heterogeneity of studies and diseases, a standard meta-analysis was not feasible for comparing studies with paired samples and a weighted average.
Results
Search Results
Our original search provided 3339 unique results; 3201 were excluded after screening. In total, 103 full-text articles were excluded after review, and 35 articles met final inclusion criteria ( Figure 1 ). There was a significant risk of bias for studies in this review (Appendix B, available online). In total, 34 studies were level 4 evidence, and 1 was level 3 evidence. Articles originated from 13 countries, and the most common were the United States, Greece, and China.
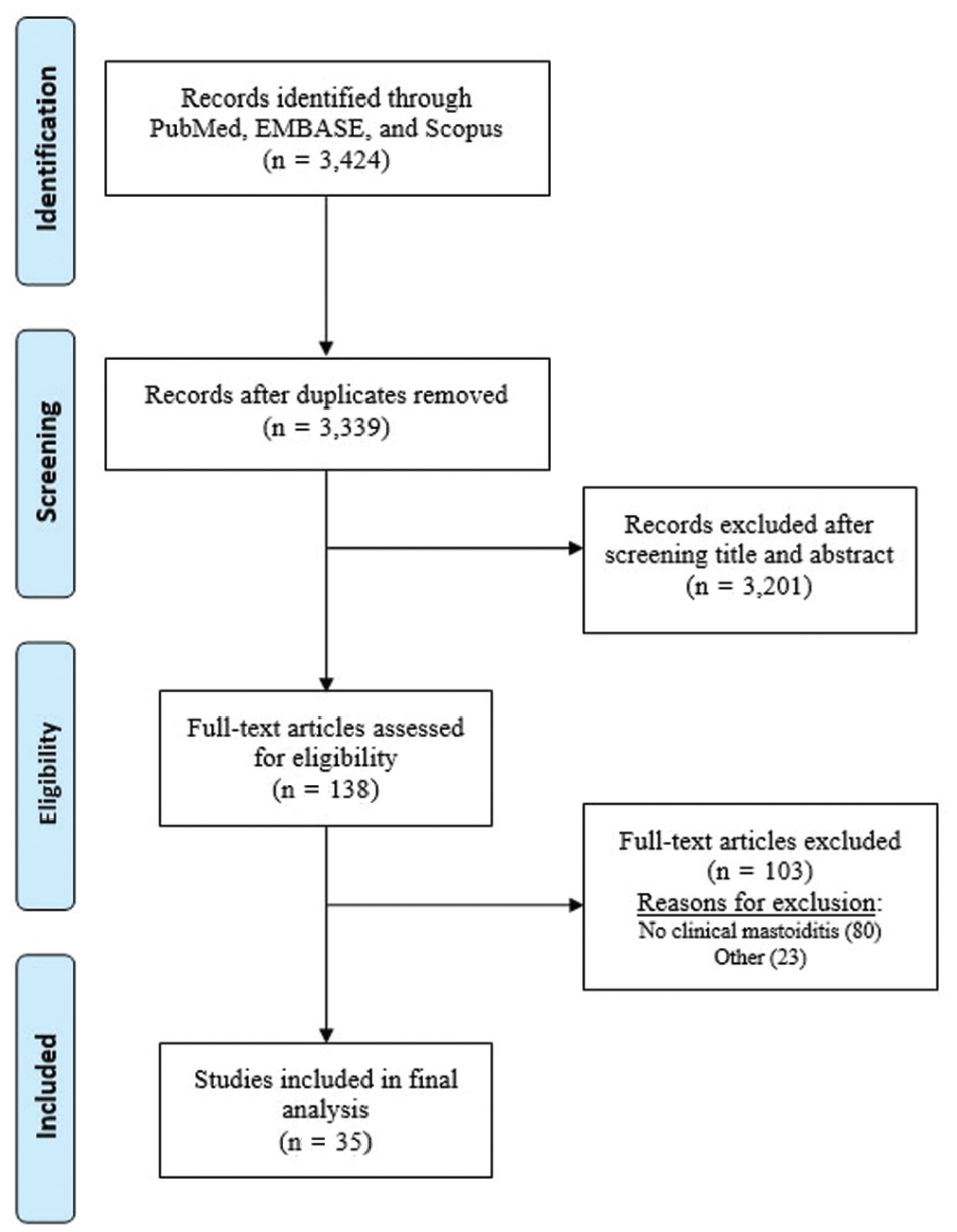
Disposition of preferred reporting items for this systematic review.
Mastoiditis Mimickers
Twenty-three publications were based on a pooled total of 24 children (<18 years old) with diseases mimicking AM ( Table 2 ).3,4,8-28 Age ranged from 10 weeks to 16 years with a male predominance (14 males, 8 females, 2 not reported). In total, 11 unique diseases were cited: acute myelogenous leukemia (AML), angiosarcoma, cranial fasciitis, Ewing sarcoma, Kawasaki disease, Langerhans cell histiocytosis (LCH), liposarcoma, melanoma, non-Hodgkin B- and T-cell lymphoma (NHL), and RMS. The most common diseases in children were LCH (n = 7), RMS (n = 4), and AML (n = 3).
Diseases in Children Mimicking Acute Mastoiditis.
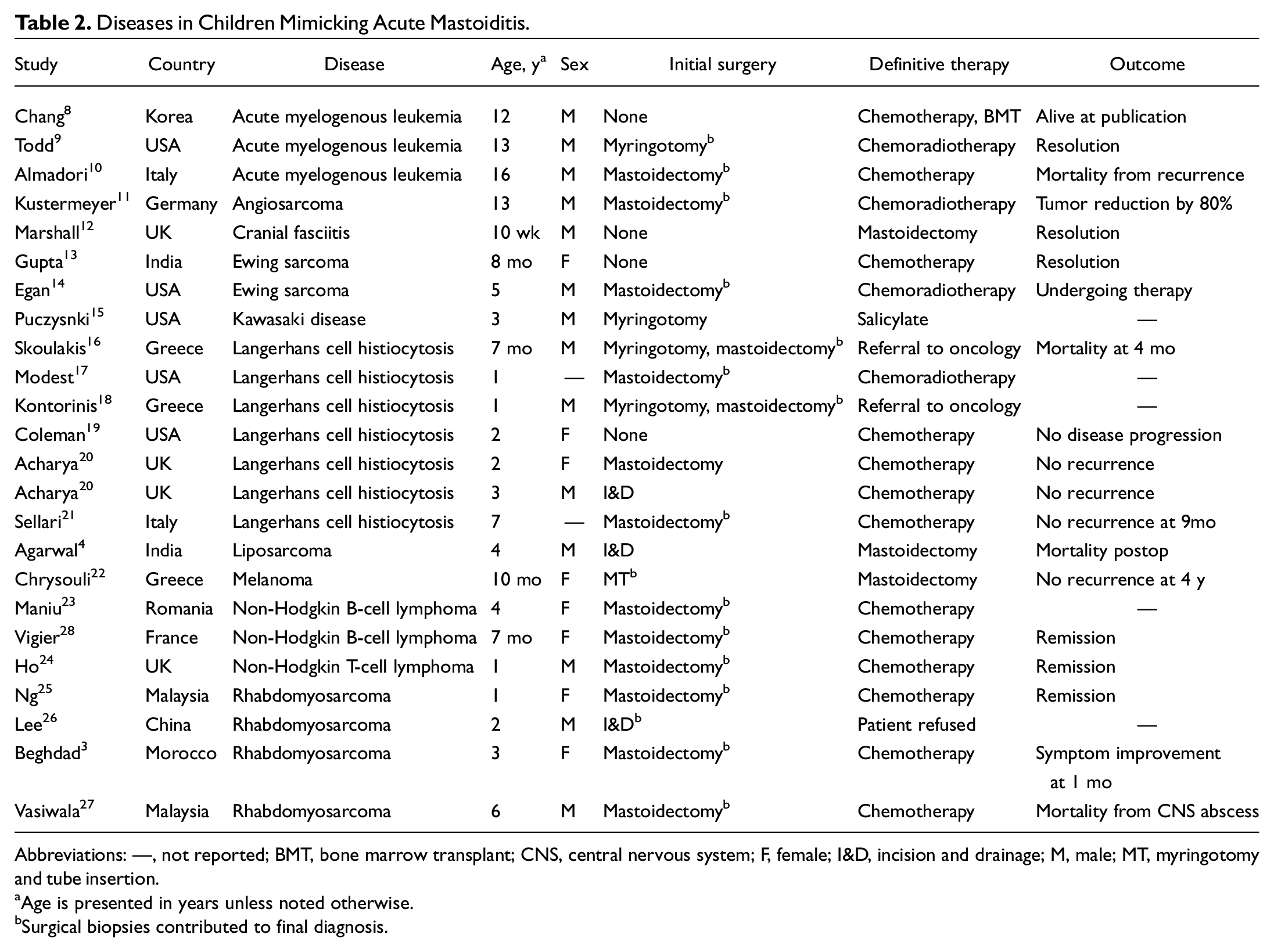
Abbreviations: —, not reported; BMT, bone marrow transplant; CNS, central nervous system; F, female; I&D, incision and drainage; M, male; MT, myringotomy and tube insertion.
Age is presented in years unless noted otherwise.
Surgical biopsies contributed to final diagnosis.
Fourteen studies comprised an additional 16 adults with diseases mimicking AM ( Table 3 ).8,17,28-40 Two studies included children and adults.8,17 Age ranged from 18 to 88 years with a male predominance (9 males, 6 females, 1 not reported). In total, 8 diseases were cited in adults: AML, aneurysmal bone cyst, fibromatosis, granulomatosis with polyangiitis (GPA), LCH, nasopharyngeal carcinoma (NPC), NHL, and squamous cell carcinoma (SCC). The most common diseases in adults were SCC and NPC (n = 3 for both).
Diseases in Adults Mimicking Acute Mastoiditis.
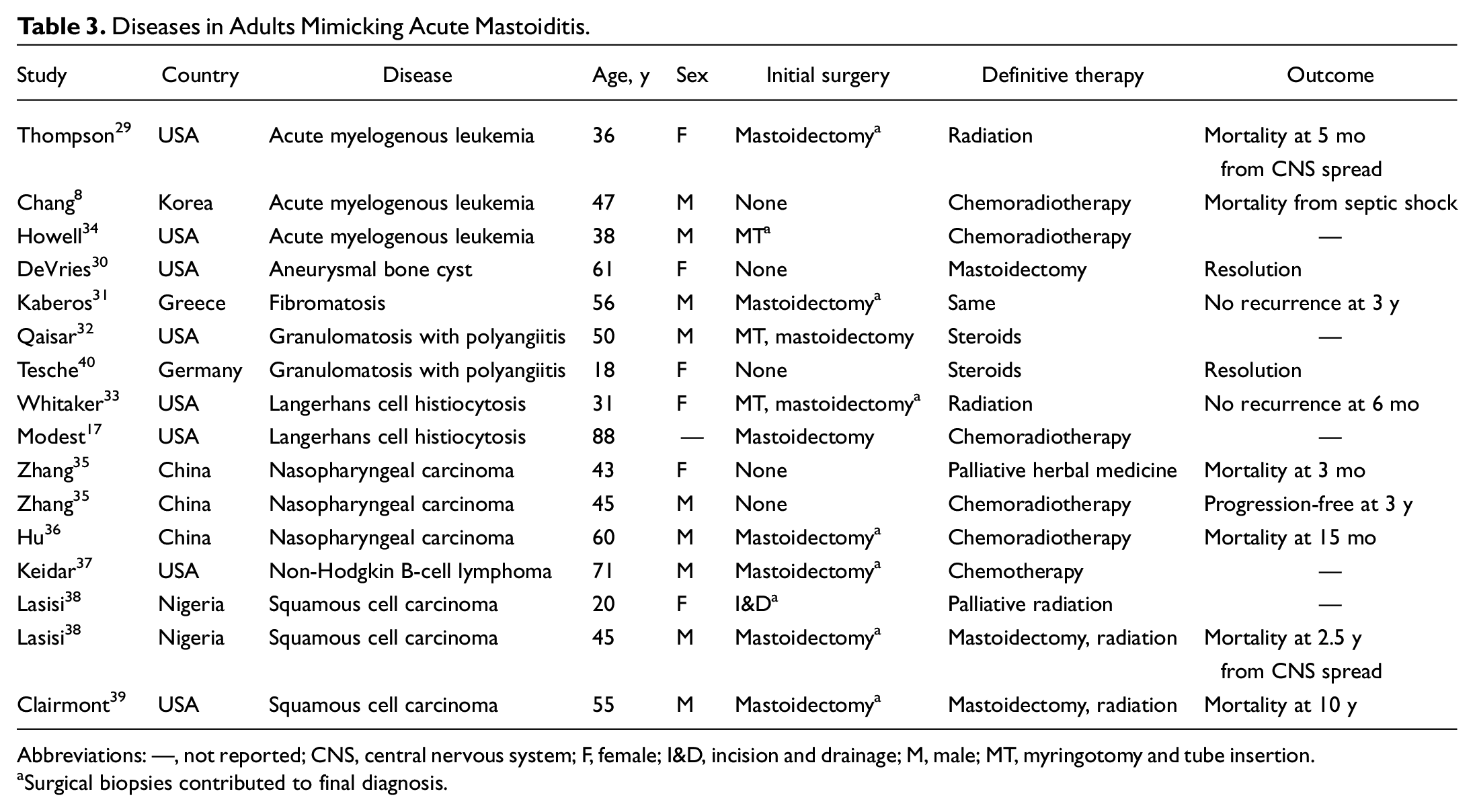
Abbreviations: —, not reported; CNS, central nervous system; F, female; I&D, incision and drainage; M, male; MT, myringotomy and tube insertion.
Surgical biopsies contributed to final diagnosis.
Fever and Leukocytosis
In total, 7 of 13 children (53.8%) with temperature data presented with fevers. Febrile diseases included Kawasaki disease, 15 LCH,18,20,21 RMS,25-27 and NHL. 28 Among children with white blood cell counts, most demonstrated leukocytosis (84.6%, 11/13). Diseases presenting with leukocytosis included AML, 10 cranial fasciitis, 12 Ewing sarcoma,13,14 Kawasaki disease, 15 LCH,18,19,21 NHL,24,28 and RMS. 26 Two of 6 adults with temperature data presented with fevers (33.3%, 2/6). Both had SCC. 38 All 4 adults with white blood cell levels presented with normal counts.28,31,32,37 Five diseases did not present with fever or leukocytosis: aneurysmal bone cyst, AML, fibromatosis, liposarcoma, and melanoma.
Otoscopy and Facial Nerve Findings
In children, 17 of 23 studies cited positive external auditory canal findings, representing 7 diseases (AML, Ewing sarcoma, Kawasaki disease, NHL, liposarcoma, melanoma, RMS). The most common otoscopy findings were otorrhea (33.3%, 8/24), canal granulation (21.7%, 5/23), and eardrum erythema/swelling (17.4%, 4/23). Other findings were canal swelling (13%, 3/23), stenosis (8.7%, 2/23), and effusion (8.7%, 2/23). Polypoidal canal tissue was described exclusively with RMS. In adults, 12 of 14 studies noted positive external auditory canal findings, representing all 8 diseases. The most common otoscopy finding was canal swelling (40%, 6/15), followed by otorrhea (26.7%, 4/15), stenosis (20%, 3/15), and effusion (13.3%, 2/15). Eardrum erythema/swelling was unique to GPA, and fleshy canal tissue was unique to SCC.
In total, 11 children representing 5 diseases presented with facial weakness or paralysis. Diseases in children included RMS, Ewing sarcoma, NHL, AML, and eosinophilic granuloma. Six adults representing 5 diseases also presented with facial palsy or paralysis: NPC, GPA, AML, SCC, and LCH.
Audiometric Findings
Eight studies examined audiometric testing in children. The type of hearing loss was classified as conductive in the majority of cases (62.5%, 5/8). Conductive hearing loss diseases included AML, 10 Ewing sarcoma, 14 Kawasaki disease, 15 LCH, 19 and NHL. 23 Two studies did not specify the type of hearing loss, and 1 study reported normal hearing. No study indicated the degree of hearing loss. Six studies conducted audiometric testing in adults. Three adults experienced conductive hearing loss (LCH17,33 and SCC 38 ), 1 experienced mixed hearing loss (aneurysmal bone cyst 29 ), and the remaining 2 were unspecified. No study indicated the degree of hearing loss.
Surgical Interventions and Intraoperative Appearance
Twenty children (83.3%, 20/24) underwent surgical intervention: mastoidectomy (n = 14), myringotomy (n = 2), myringotomy with mastoidectomy (n = 2), incision and drainage (n = 1), and myringotomy with tympanostomy tube insertion (n = 1). Intraoperative biopsies contributed to a definitive diagnosis in most children (80%, 16/20); the majority (85%, 17/20) continued on to require definitive treatment with a nonsurgical modality ( Table 2 ).
Eleven adults (68.8%, 11/16) underwent surgical intervention: mastoidectomy (n = 7), tympanostomy tube insertion with mastoidectomy (n = 2), tympanostomy tube insertion alone (n = 1), and incision and drainage (n = 1). Intraoperative biopsies contributed to diagnosis for 9 of 11 adult patients (81.8%). The majority of surgical adults (81.8%, 9/11) required subsequent definitive treatment via a nonsurgical modality ( Table 3 ).
Gross intraoperative findings were described for 13 diseases. Six diseases were characterized by unique texture: AML was described as rubbery, 9 gelatinous,10,18 and necrotic 28 ; RMS as fleshy/polypoidal25,27; NPC as granular and friable 36 ; fibromatosis as soft 31 ; SCC as keratinous 38 ; and cranial fasciitis as “thickened” with “moth-eaten” bone. 12 Colors were attributed to 4 diseases: liposarcoma as “pale-yellow,” 4 melanoma as “cuttlefish ink–colored,” LCH as a friable “reddish” mass,16,21,33 and eosinophilic granuloma as “milk-like.” 20 Purulence was associated with Ewing sarcoma and NHL.14,23,24
Laboratory Features and IHC
Unique laboratory features are presented in Table 4 . Five diseases presented with elevated erythrocyte sedimentation rate or C-reactive protein: cranial fasciitis, 12 NHL,28,37 Ewing sarcoma, 14 Kawasaki disease, 15 and LCH.16,18,19,33 AML presented with thrombocytopenia, 10 Ewing sarcoma and NHL with elevated lactate dehydrogenase,14,37 and GPA with elevated antineutrophil cytoplasmic antibody (c-ANCA) and protease 3 antibody levels.32,40 IHC findings are also presented in Table 4 .
Diseases With Characteristic Laboratory and IHC Features. a
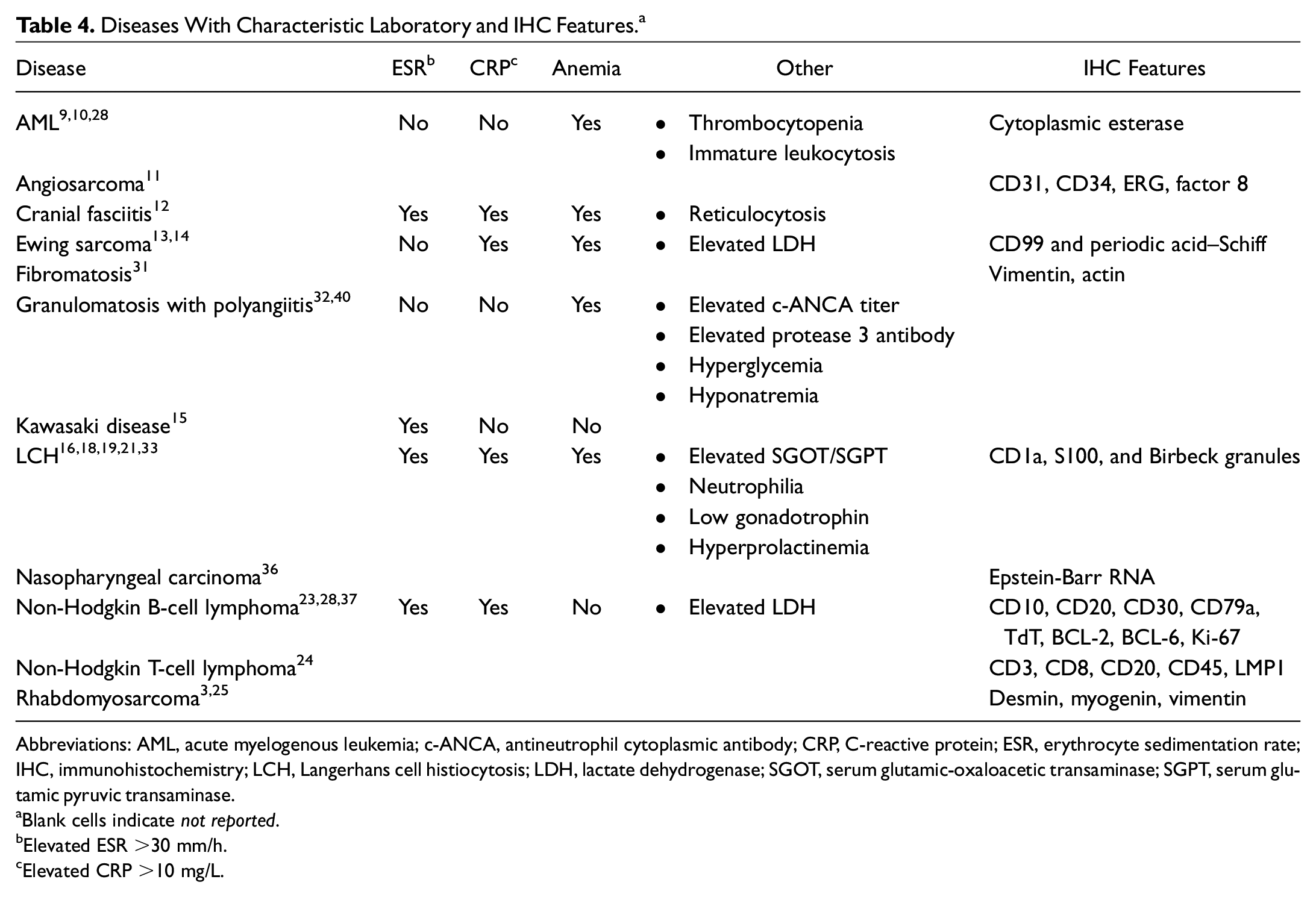
Abbreviations: AML, acute myelogenous leukemia; c-ANCA, antineutrophil cytoplasmic antibody; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IHC, immunohistochemistry; LCH, Langerhans cell histiocytosis; LDH, lactate dehydrogenase; SGOT, serum glutamic-oxaloacetic transaminase; SGPT, serum glutamic pyruvic transaminase.
Blank cells indicate not reported.
Elevated ESR >30 mm/h.
Elevated CRP >10 mg/L.
Time Course
Twenty-seven studies cited the length of time from symptom onset to presentation, with a range from 3 days (cranial fasciitis 12 ) to 4 years (SCC 38 ). A visual representation of symptomatic period prior to presentation is shown in Figure 2 .
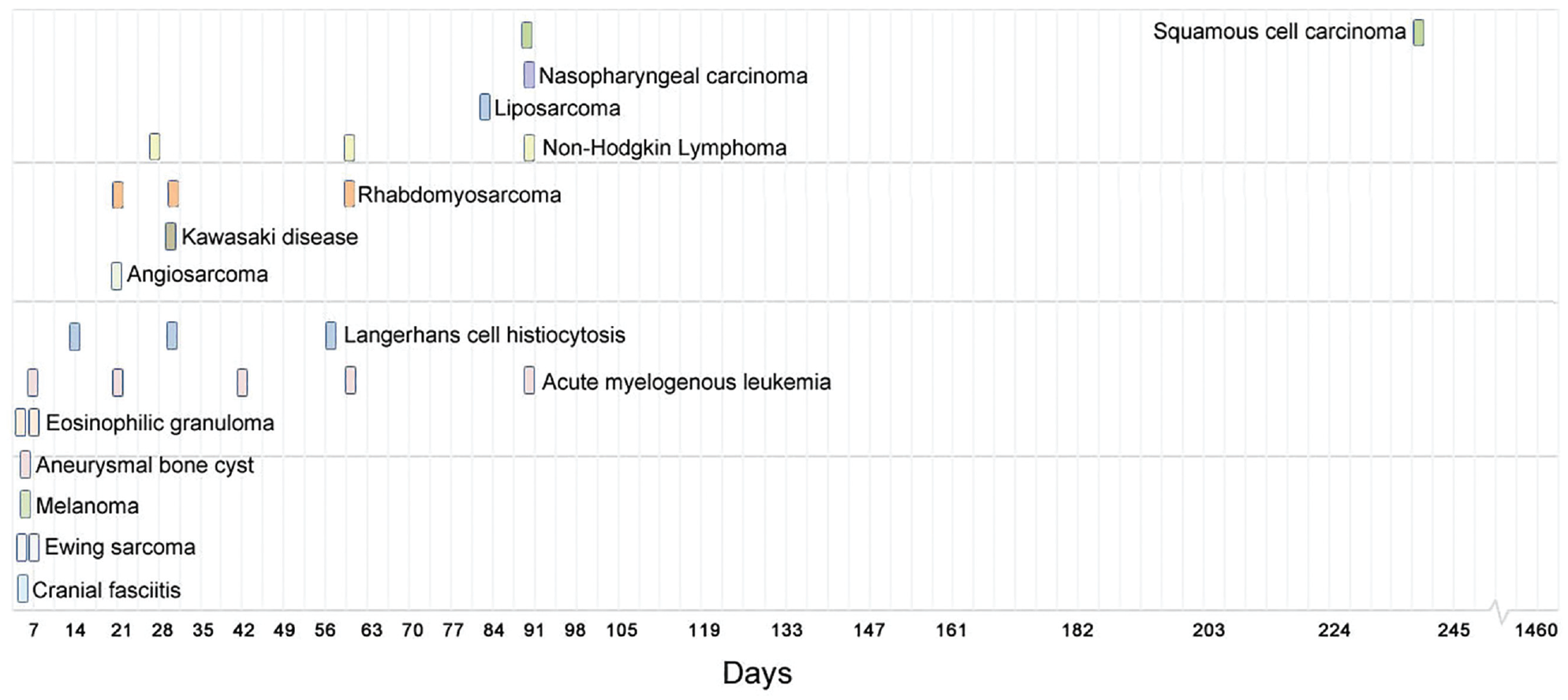
Time course of mastoiditis mimickers. Visual representation of time from symptom onset to initial presentation for diseases mimicking mastoiditis.
Discussion
Historically, AM occurred in up to 20% of patients with acute otitis media, and many cases required surgery. 41 With the widespread adoption of vaccinations and antibiotics, the frequency of acute infectious mastoiditis has dropped precipitously to about 0.004% of individuals. 42 As infections decrease, patients with classic mastoiditis findings may have a relatively greater chance of harboring atypical pathologies. In fact, increasing reports have shown that noninfectious diseases may have clinical presentations similar to those of AM. Many of these patients may experience misdiagnosis, unnecessary procedures, and delayed treatment. To the best of our knowledge, there has been no consolidated report to date of such pathologies. In this review, we sought to fill this gap in knowledge by identifying and organizing atypical pathologies and describing the unique laboratory, radiographic, and intraoperative features that may assist with diagnosis.
Solid Tumors
Sarcomas
Sarcomas are a family of rare benign tumors arising from bone and soft tissue. This review identified Ewing sarcoma, RMS, angiosarcoma, fibromatosis, and liposarcoma.
Ewing sarcoma was reported in 2 children. Time from symptom onset to presentation was short, ranging from 3 to 7 days. Laboratory findings characteristic of this disease include leukocytosis, elevated inflammatory markers, and increased lactate dehydrogenase, all which were present in this review ( Table 4 ). On histology, Ewing sarcoma has the appearance of a small round cell tumor that stains positive for PAS and CD99. 43 One child with available IHC data in this review was CD99+. These markers, with elevated inflammatory markers and a young age, may help narrow this disease on a differential. One child underwent cortical mastoidectomy for presumed infection prior to diagnosis, and both children underwent definitive chemotherapy.13,14
RMS was identified in 4 children. RMS is the most common soft tissue sarcoma in children and accounts for 3% of all pediatric tumors. 44 The head and neck is the most common site. All 4 cases underwent surgical intervention for presumed mastoiditis, and intraoperative descriptors included “fleshy” and “polypoidal.” This unique appearance may help differentiate RMS from other sarcomas. Biopsy results included the presence of sarcoma cells with positive staining for desmin and vimentin. Treatment typically involves surgical resection, radiation, or chemotherapy; 3 children in this review underwent definitive chemotherapy. 45
Angiosarcoma was reported in 1 child. Angiosarcomas represent <1% of all sarcomas. Angiosarcoma occurs almost exclusively in young males. 46 Unique to angiosarcoma is high vascularity on angiography, as seen in the 13-year-old boy in this review. This radiographic finding, with age and sex, may differentiate angiosarcoma. The boy in this review underwent mastoidectomy, with biopsy results showing kaposiform hemangioendothelioma with spindle cell patterns. Surface markers included CD31, CD34, and vascular endothelial marker (ERG). Treatment of angiosarcoma is typically a combination of surgery, radiotherapy, or chemotherapy. The subject in this review underwent definitive chemotherapy with adjuvant radiation. 47
Fibromatosis was reported in 1 adult. Fibromatosis, or desmoid tumors, are benign, locally aggressive tumors derived from fibrous overgrowths of dermal and subcutaneous tissue. They occur in the head and neck in 10% of cases and are more common in Caucasians and females. 48 Presentation is similar to other soft tissue sarcomas and typically involves a slowly growing, painless mass. Treatment involves surgery with or without radiation. The patient in this review underwent mastoidectomy with subtotal removal of disease and no recurrence at 3-year follow-up. 48
Liposarcoma was reported in 1 child. Liposarcoma accounts for 20% of soft tissue sarcomas and is the most common sarcoma worldwide. 49 It is more common in males. In this review, a 4-year-old boy with liposarcoma localized to the mastoid presented after superinfection mimicked mastoiditis. After multiple failed antibiotics, he underwent mastoidectomy, where a yellow fleshy mass was discovered. Histologic examination confirmed lipoblastic activity in a myxoid background. Surgical excision is the mainstay of treatment for liposarcoma, and prognosis is excellent, with a 5-year survival rate >75%. 50 The boy in this review who underwent mastoidectomy, however, died in the immediate postoperative period due to acute respiratory failure unrelated to the surgery.
Cutaneous Malignancies
Three cases of SCC were identified. Temporal bone SCC is commonly detected between the fifth and seventh decades of life, and symptoms are hearing loss, otalgia, otorrhea, and facial weakness. 51 A unique feature for patients in this review was the presence of palpable cervical lymphadenopathy from nodal metastasis and fleshy granulation tissue in the external auditory canal. Two cases of SCC masquerading as mastoiditis had concurrent dural and intracranial invasion. Surgery, with or without radiation, remains the mainstay of treatment. Two patients in this review underwent lateral temporal bone resections, and the third underwent incision and drainage; all 3 subsequently received radiotherapy. Prognosis is favorable for T1 and T2 cancers; however, 2-year overall survival drops to about 50% for T3 and 7% for T4. 52 Two of 3 patients died from their disease by publication.
Melanoma was reported in 1 girl who was 10 months old. She was initially treated with intravenous antibiotics and ventilation tubes for otorrhea, mastoid erythema, and mastoid inflammation. She subsequently underwent mastoidectomy where diagnosis of melanoma was confirmed. Unique to this disease was the intraoperative appearance of black, “cuttlefish ink–colored” tissue. Further history revealed that the girl’s mother died from melanoma when the girl was 3 months old; therefore, her melanoma likely represented fetal metastasis. Her disease underwent spontaneous regression, and she remained disease free at 4-year follow-up. 22
Nasopharyngeal Carcinoma
NPC was identified in 3 adults. NPC is the most common neoplasm of the nasopharynx and endemic to East Asia, where up to 25 per 100,000 individuals are diagnosed annually. 53 Older age and male sex are additional risk factors. 54 Two of 3 patients in this review were male, and all were middle-aged and East Asian. Among mastoiditis mimickers, sex and ethnicity may be important to consider. Cervical lymph node involvement and distant metastases were present in all 3 patients. To this end, the spread of NPC to the mastoid may portend a higher disease stage and worse prognosis. First-line treatment is radiation 55 : 2 subjects underwent chemoradiation and the third underwent palliative herbal therapy. Overall survival is poor for stage 3 and 4 diseases, with a median survival of 31 months. 56 All 3 cases in this review were classified as stage 3, and only 1 patient was alive at the time of publication.
Cranial Fasciitis
Cranial fasciitis was reported in 1 child. Cranial fasciitis is a rare benign tumor of fibroblast origin that occurs almost exclusively in children with a male predominance. 57 The boy in this review was 10 weeks old and presented with 3 days of postauricular swelling with a palpable, nontender mastoid mass. He was initially treated with antibiotics, followed by myringotomy and mastoidectomy for presumed mastoiditis. Intraoperatively, underlying bone was “moth-eaten.” Biopsy results demonstrated spindle cells positive for myosin and CD68, consistent with a myofibroblastic origin and cranial fasciitis. Treatment for cranial fasciitis typically involves surgical excision; the patient in this case remained disease free at 6 weeks postoperatively.
Aneurysmal Bone Cyst
Aneurysmal bone cyst was reported in 1 adult. This is a benign osseous lesion characterized by fibrous tissue enclosing blood-filled cavities. Incidence is <1 per 100,000 people per year. Temporal bone involvement is rare and limited to case reports. 30 The patient in this review was a 61-year-old woman who presented with 4 days of mastoid swelling, tenderness, and canal edema. After failure with antibiotics, she underwent mastoidectomy with resolution of disease at 6-month follow-up.
Hematologic Malignancies
AML was the third-most common mastoiditis mimicker in children and adults. AML comprises a group of cancers caused by clonal proliferation of myeloid progenitor cells. Leukemic infiltration of skin and soft tissue occurs in 13% of cases 58 and manifests as erythematous-violaceous nodules. When localized around the mastoid, these cutaneous lesions can mimic the appearance of AM. Laboratory workup may show anemia, neutropenia, and thrombocytopenia; anemia and thrombocytopenia were found in patients in this review ( Table 4 ). Three patients with AML underwent mastoidectomy for presumed infection, and histologic features included positive cytoplasmic esterase staining on IHC, 29 eosinophilic cells with bilobed nuclei, 9 and blast cells. 10 Overall prognosis of AML is poor with a 5-year survival rate of 15%. 59 In this review, both adults with AML died from disease; 2 of 3 children were alive at publication.
LCH is known as the “mimicker of malignancy and infection” 60 and was the most common disease in this review to mimic mastoiditis. LCH is caused by clonal proliferation of Langerhans cells originating from bone marrow. 61 LCH has an incidence of 5 per million individuals and most commonly presents between the ages of 1 and 3 years. 62 The average age of children in this review was 2.1 years. Bony involvement occurs in the majority of patients and is associated with painful raised papules. Skin involvement occurs in 40% of patients and has the appearance of an eczematous rash. 63 Bony and soft tissue involvement of the temporal bone can mimic the appearance of AM. Disease course is subacute with slow progression, over the course of weeks to 2 months ( Figure 2 ). Among diseases mimicking mastoiditis, LCH presented with the most distinct radiographic features, such as “lytic” and “punched out” lesions throughout the temporal bone.
Of 9 patients in this review, 7 underwent mastoidectomy prior to their diagnosis of LCH. Although not curative, surgical intervention was helpful in reaching the diagnosis, with biopsies revealing Langerhans cells and Birbeck granules, as well as markers CD1a, S100, and CD207. Survival rates are excellent, at almost 100% in children with low-risk subtypes. Consistent with the literature, the majority of children and adults in this review (88.9%, 8/9) survived after treatment with surgical enucleation, radiation, and/or chemotherapy.
NHL was identified in 3 children and 1 adult. NHL encompasses a variety of lymphocytic neoplasms originating from lymph tissue. NHL accounts for 4% of new cancer diagnoses each year, and incidence increases with age. 64 In our review NHL involving the mastoid followed a subacute course, with patients experiencing symptoms over the course of several months prior to diagnosis ( Figure 2 ). A laboratory feature unique to NHL was elevated lactate dehydrogenase from high cell turnover. All 4 patients underwent mastoidectomy for presumed infection. Surgical pathology supported the diagnosis of NHL with the presence of B- and T-cell surface markers ( Table 4 ). A combination of chemotherapy, radiation, and bone marrow transplant is the mainstay of treatment, and all patients in this review underwent definitive chemotherapy. Two children were in remission; follow-up data for the other 2 subjects were not presented.
Autoimmune/Inflammatory
Kawasaki disease was reported in 1 child. Kawasaki disease is a childhood disease characterized by vasculitis of medium-sized arteries. Cardiac involvement leads to mortality in 1% of cases. 65 Unlike other noninfectious mastoiditis mimickers, Kawasaki disease is associated with fever and leukocytosis; the 3-year-old boy in this review presented with a fever to 104 °F and leukocytosis. Another characteristic unique to Kawasaki was the presence of an elevated erythrocyte sedimentation rate. The patient in this review underwent myringotomy for presumed mastoiditis; however, after pathologic samples showed lymphoid tissue with reactive germinal centers, surgery was aborted and salicylate therapy initiated.
GPA was reported in 2 adults. GPA is a rheumatologic disorder characterized by small and medium vessel vasculitis. Prevalence is 3 per 100,000 individuals. 66 Mastoid involvement can lead to destructive granulomatous lesions and otitis media, as seen in these patients. Unique to GPA is the number of organ systems involved, particularly the lungs; on imaging, patients in this review demonstrated masses in both lungs in addition to mastoid involvement. Defining features also included the presence of c-ANCA, protease 3 antibody, and elevated erythrocyte sedimentation rate and C-reactive protein. One patient in this review initially underwent myringotomy, tympanostomy tube placement, and mastoidectomy for presumed AM; however, after lung biopsy confirmed GPA, definitive treatment was switched to steroids, which resolved symptoms.
Diagnostic Algorithm
A variety of diseases can share the phenotype of AM. As organized here, this can be broadly categorized into solid tumors, hematologic malignancies, and autoimmune/inflammatory diseases. We propose a diagnostic algorithm to narrow down this broad differential ( Figure 3 ). This algorithm may serve as a useful first step for organization but is by no means a definitive guide and is limited by the reporting bias inherent to the studies in this review. The importance of a thorough history cannot be overstated, particularly with attention to demographics, cancer history, and length of symptoms prior to presentation. The next factor to consider is age: several diseases were reported exclusively in children, such as Ewing sarcoma, Kawasaki disease, and RMS; others were associated with adults, such as NPC and SCC.
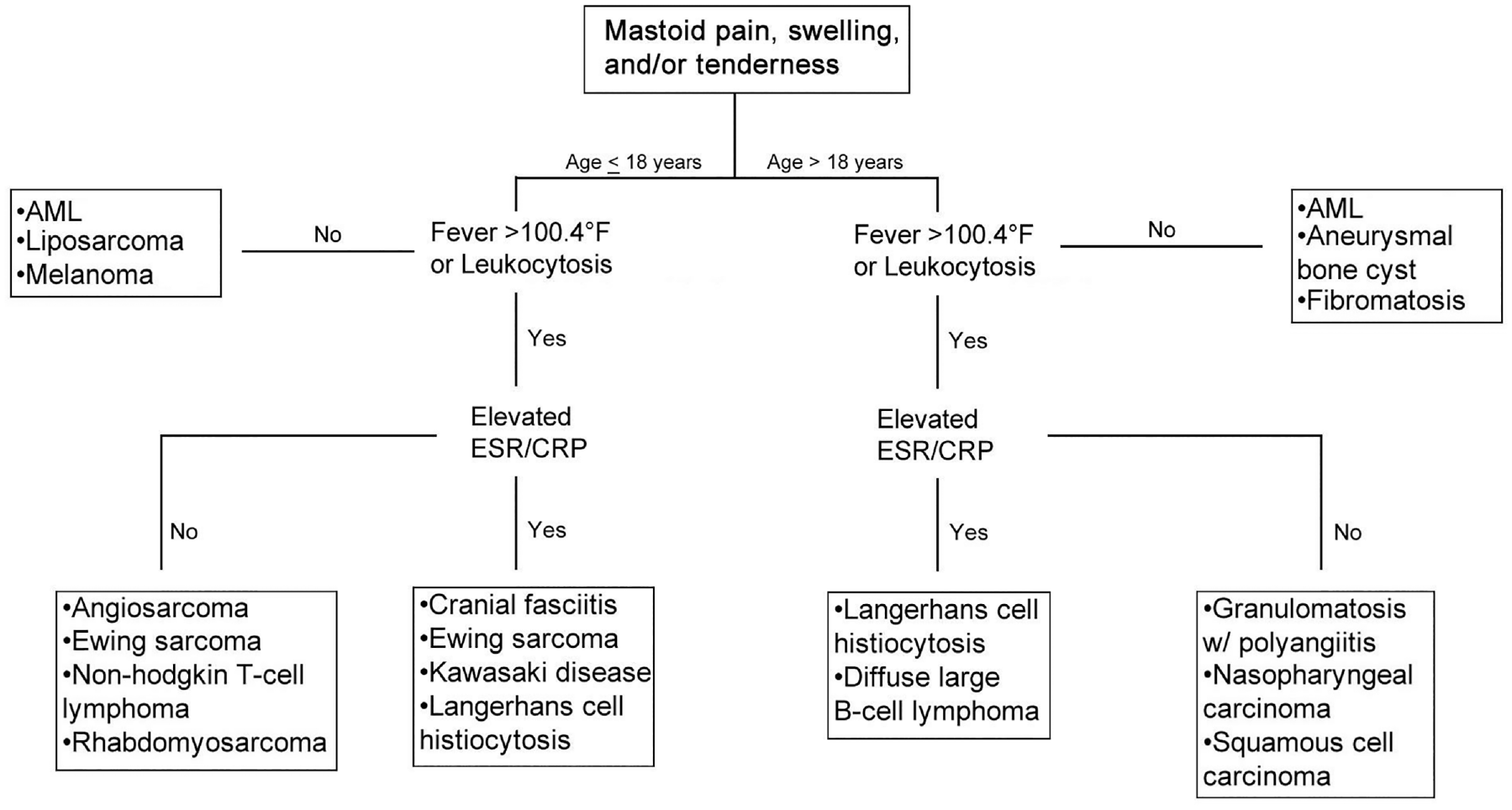
Algorithm for atypical presentations of mastoiditis. An algorithm for the diagnosis and treatment of noninfectious pathologies mimicking mastoiditis. AML, acute myelogenous leukemia; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
Diseases can be classified by the presence or absence of fever and leukocytosis. Fever and leukocytosis are common features of acute infectious mastoiditis, and their absence may suggest an atypical diagnosis. Afebrile diseases include AML, aneurysmal bone cyst, fibromatosis, liposarcoma, and melanoma. Of note, traditionally afebrile diseases may still present with fever or leukocytosis from superinfection. Otoscopy findings of the ear canal and eardrum were often positive but nonspecific, with the majority of patients demonstrating a combination of otorrhea, canal swelling/granulation, and eardrum pathology. Facial weakness and hearing loss were similarly nonspecific findings; however, they present more frequently than would be expected for routine mastoiditis. Therefore, the presence of facial weakness or hearing loss should raise the index of suspicion and warrant further investigation prior to surgical intervention.
Laboratory markers are useful for differentiating diseases. Inflammatory and autoimmune pathologies may present with elevated erythrocyte sedimentation rate and C-reactive protein. Diseases with high cell turnover, such as Ewing sarcoma and lymphoma, may present with elevated lactate dehydrogenase. Thrombocytopenia and anemia were unique to AML, and c-ANCA and protease 3 antibody were unique to GPA. Leukocytosis was frequently present; however, as mentioned earlier, this finding was often nonspecific and a by-product of reactionary inflammation or superinfection.
Imaging was noncontributory in most cases due to nonspecific findings. Only in specific circumstances was imaging helpful, as in “lytic, punched out” lesions with LCH, hypervascularity with angiosarcoma, or ground glass lung opacities with GPA. Computed tomography was the main imaging modality in most studies. Magnetic resonance imaging may better suggest the presence of atypical diseases and their unique characteristics.
Finally, once the decision to operate was made, histological and IHC features routinely assisted with diagnosis. Many diseases have unique pathologic and IHC profiles. In this review, 80% of children and adults who underwent surgery reached their diagnosis with the assistance of biopsies, underscoring the importance of this step. Nevertheless, when suspicious intraoperative findings are encountered, surgeons should maintain a low threshold to abort their procedure after biopsies are taken, because in many cases, definitive treatment entails a nonsurgical modality.
Limitations
This review has several important limitations. Studies were generally limited to case reports and series with a low level of evidence. Data from studies were also pooled and analyzed in a quantitative synthesis rather than meta-analysis. Inclusion of traditional cross-study analyses could not be performed given the limitations of existing data, bias, and heterogeneous study reporting. Finally, our search strategy was limited to diseases with clinical findings of AM. This excluded studies that reported on mimickers of “radiographic mastoiditis.” Cholesteatoma was also excluded, which certainly can mimic mastoiditis. Nevertheless, these were intentional design features to increase the clinical relevance and feasibility of this review.
Conclusion
A broad spectrum of noninfectious diseases can mimic the clinical and radiographic features of AM. In such cases, further investigation with attention to history, laboratory workup, imaging, and surgical pathology is critical. Otolaryngologists should always be mindful of the possibility that noninfectious diseases may present with a constellation of symptoms similar to mastoiditis and thus maintain an organizational framework for reaching a diagnosis.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211064190 – Supplemental material for A Review of Noninfectious Diseases Masquerading as Acute Mastoiditis
Supplemental material, sj-docx-1-oto-10.1177_01945998211064190 for A Review of Noninfectious Diseases Masquerading as Acute Mastoiditis by Kevin Wong, Annie E. Arrighi-Allisan, Caleb J. Fan, George B. Wanna, Maura K. Cosetti and Enrique R. Perez in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-2-oto-10.1177_01945998211064190 – Supplemental material for A Review of Noninfectious Diseases Masquerading as Acute Mastoiditis
Supplemental material, sj-docx-2-oto-10.1177_01945998211064190 for A Review of Noninfectious Diseases Masquerading as Acute Mastoiditis by Kevin Wong, Annie E. Arrighi-Allisan, Caleb J. Fan, George B. Wanna, Maura K. Cosetti and Enrique R. Perez in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
We thank Samantha Walsh, MLS, Levy Library, Icahn School of Medicine at Mount Sinai, for her assistance developing the search strategy.
This article was presented at the 2021 AAO-HNSF Annual Meeting & OTO Experience; October 3-6, 2021; Los Angeles, California.
Author Contribution
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.