
Abstract
Objectives
Plunging ranula is a pseudocyst of saliva extravasated from the sublingual gland (SLG) to the submandibular space. This is treated by transoral excision of the SLG or transcervical cyst excision that might differently affect surgical morbidity and recurrence. This study compared the clinical outcomes of complete vs partial excision of the SLG for plunging ranula.
Study Design
A nonrandomized comparative study.
Setting
Academic medical center.
Methods
This study included 42 patients with plunging ranula who underwent complete or partial excision of the SLG with the evacuation of cystic content. Two surgical methods of complete or partial SLG resection were alternatively allocated to consecutive patients without randomization. The primary outcome was a postoperative recurrence. Secondary outcomes were operation time and complications.
Results
Complete and partial excision of the SLG was performed in 22 and 20 patients, respectively, without injury to the Wharton’s duct or the lingual nerve. Postoperative complications in 42 patients were minor with temporary events: hematoma, 1 (5%); tongue numbness, 2 (5%); dysgeusia, 4 (9%); and dysphagia, 2 (5%), which did not differ between patients with complete and partial excision of the SLG (P > .1). However, recurrence occurred in only 5 of 20 patients with partial SLG excision but none of 22 patients with complete SLG excision for a median follow-up of 36 months.
Conclusions
Complete SLG excision is preferred over partial SLG excision to treat plunging ranula for reducing postsurgical risks of complications and recurrence.
Plunging ranula is a pseudocyst of saliva extravasated from the sublingual gland (SLG) to the sublingual and submandibular spaces through the defect of the mylohyoid muscle. 1 Ranula contains mucous collection in a pseudocyst within the fascial planes in the floor of mouth. 2 Ranula is developed commonly by injury to the duct of the SLG, causing it to rupture and saliva to leak into the connective tissues under the floor of mouth. 3 Plunging (cervical) ranula is typically found as a bulging cystic lesion in the submandibular area and the upper neck by mucus collection extending below the mylohyoid muscle. 3 Ectopic SLG or congenital dehiscence in the mylohyoid muscle may cause the occurrence of plunging ranula. 4
Plunging ranula causes facial and neck disfigurement on cosmetically sensitive areas, which leads to the need for treatment. Plunging ranula has been treated with surgery or nonsurgical sclerotherapy via OK-432 or other sclerosing agents. 5 Surgery is recognized as the primary modality to treat plunging ranula. 5 Different surgical methods of treating plunging ranula have been described. 6 In an online survey of 220 members of the American Head and Neck Society, the majority (80%) preferred ranula excision, with or without the SLG excision, via a transoral, cervical, or combined approach. 7 Only 27 (12%) respondents performed the SLG excision with the evacuation of ranula. 7 A recent meta-analysis recommended transoral resection of the SLG as the primary surgical procedure for plunging ranula because of the fewer complications and the lower recurrence rate as compared with the transcervical approach. 5
Ranula has no true epithelial lining in the cyst, only mucus collection along the fascial planes under the mouth floor. Excision of ranula might be unnecessary to treat oral or plunging ranula. Most recent studies have endorsed transoral complete excision of the affected SLG with simple evacuation of ranula pseudocyst. The SLG is composed of approximately 5% of whole oral salivary secretion. 8 The volume of SLG is considerable, and its complete excision might lead to increased complication rates and operation time during blunt dissection from surrounding important anatomic structures. Minimally invasive gland-preserving conservative surgery has been popularized to treat benign parotid tumors. 9 Partial parotidectomy or extracapsular dissection may allow for the reduction of postoperative complications and the preservation of salivary secretary function without compromising local control. 10 Therefore, a hypothesis may be as follows: partial excision of the SLG is more effective to treat plunging ranula in terms of reduced operation time and surgical morbidity but with no increased recurrence rate when compared with complete excision of the SLG. This study compared the clinical outcomes of complete vs partial excision of the SLG for plunging ranula.
Methods
A comparative study was conducted of patients with plunging ranula between 2010 and 2018. Inclusion criteria were transoral complete or partial excision of the SLG with the evacuation of cystic content for plunging ranula. Exclusion criteria were cystic metastasis of malignancies, other cystic benign diseases (eg, lymphatic malformation), previous surgery or sclerotherapy, no agreement on surgical treatment, or inappropriate information and follow-up <2 years. The lesions were localized by contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI), and the cystic fluid was aspirated to be differentially diagnosed ( Figure 1 ).11,12 Two surgical methods of complete or partial SLG resection were alternatively allocated to consecutive patients without randomization and blinding (masking). This was not determined by the size or location of plunging ranula or the age or sex of the patient. The study was reviewed and approved by the institutional ethics committee and all patients provided written informed consent. Intra- and postoperative findings were recorded. The patients were regularly followed to monitor postoperative recurrence with physical examination and intermittent imaging study of CT or MRI.
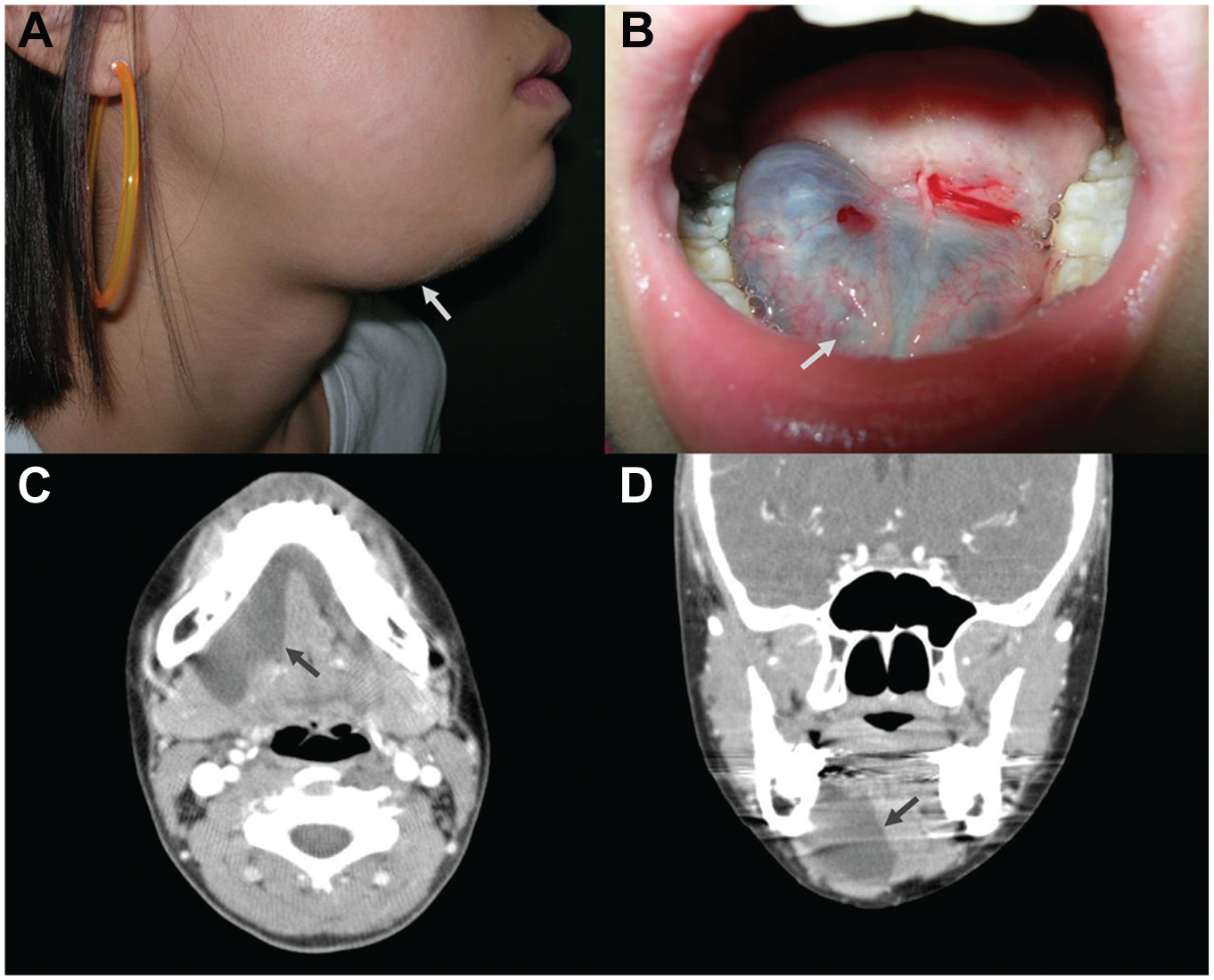
A case of plunging ranula. (A, B) A bulging cystic mass in the right submandibular region and the floor of mouth. (C, D) A nonenhancing cystic lesion in the sublingual and submandibular spaces.
Under general anesthesia, the mouth of each patient was opened with the Denhardt mouth gag, and the tongue was retracted to the opposite side. An incision was made with a Bovie electrode and fine-needle tip along the sulcus between the mobile tongue and the floor of mouth. Local lidocaine injection was not used along the incision and in the wound. The SLG was dissected with the incision site and retracted anteriorly. The distal part and opening of the Wharton’s duct were first identified and carefully dissected posteriorly to the hilum without injury. The lingual nerve was also identified and carefully preserved. All parts of the SLG on the affected side were removed in the complete excision group, while in the partial excision group, the part of the SLG with extension to plunging ranula was removed with preservation of the other remaining SLG. After complete or partial SLG resection, the mylohyoid muscle defect causing plunging ranula was widened, and the cystic content of ranula was evacuated. After partial SLG excision, the cut end of the remaining gland was cauterized without any sealants or suture ligations, leaving the unclosed mouth incision connected. The wound was cleaned, irrigated, and hemostasized. The incision was closed with absorbable sutures, and the midportion of the incision remained unclosed to spill wound fluid into the oral cavity. No drain was inserted. The submandibular and sublingual area was compressed cranially and removed the next morning. The patient received prophylactic administration of oral antibiotics for 5 days after surgery.
Any complications were checked during the hospital stay and at outpatient visits. Subjective pain sensation was checked during the hospital stay with a visual analog scale (VAS) with a 10-cm line (low to high). The patients were regularly followed for 1 week, 1 month, and thereafter every 6 months at outpatient clinics with physical examination and intermittent imaging studies of CT or MRI.
The primary outcome was postoperative recurrence. Secondary outcomes were operation time and complications. Continuous variables were expressed as mean and standard deviation and categorical data as number and percentage. Statistical differences between the complete and partial SLG excision groups were calculated with the Mann-Whitney U test (continuous variables) or the Fisher’s exact test (categorical variables). All tests were 2-tailed, and statistical significance was P < .05 per SPSS 22.0 statistical software (SPSS Inc).
Results
Fifty-three cases of plunging ranula were initially accessed, but 7 were excluded due to primary nonsurgical sclerotherapy ( Figure 2 ). Forty-six patients underwent complete (n = 24) or partial (n = 22) SLG excision with the evacuation of cystic fluid on the affected side. Four patients were lost to follow-up within 2 years. Finally, 42 patients were involved in the final analyses: 22 with complete SLG excision and 20 with partial. Twenty-one (50%) patients were men and 21 (50%) were women, with a mean age of 19 years: sex distribution and mean age did not differ between the groups (P > .1; Table 1 ). No patients in either group had an injury to the Wharton’s duct or the lingual nerve. Operation time and blood loss did not differ between the groups (P > .1).
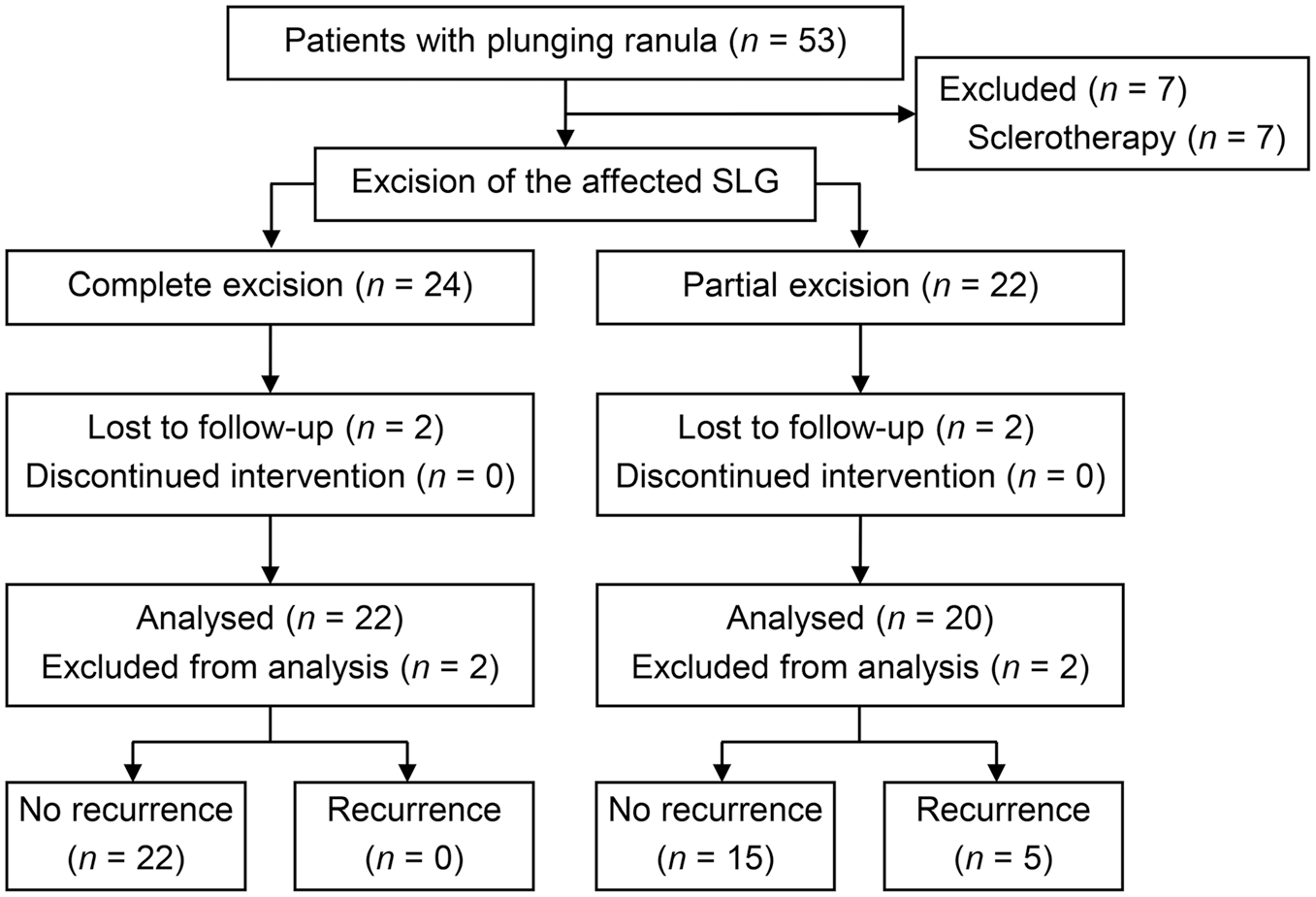
Flowchart of the study cohort with complete vs partial excision of the sublingual gland (SLG) with the evacuation of cystic content for plunging ranula.
Comparison of Complete vs Partial Excision of the Sublingual Gland. a
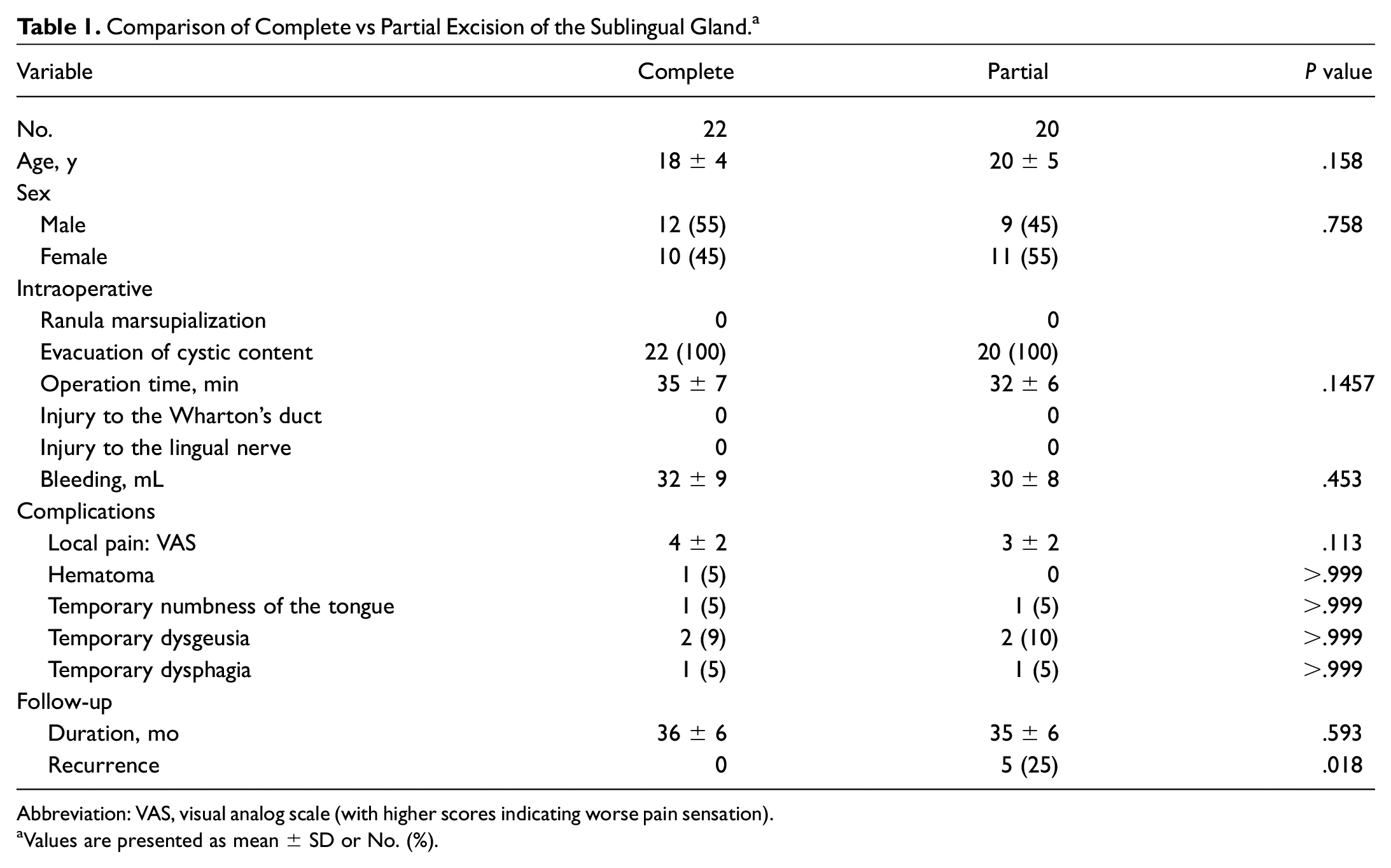
Abbreviation: VAS, visual analog scale (with higher scores indicating worse pain sensation).
Values are presented as mean ± SD or No. (%).
Postoperatively, the mean VAS score of subjective pain sensation was 4, which did not differ between the groups (P = .113). Postoperative complications in 42 patients were minor with temporary events: hematoma, 1 (5%); tongue numbness, 2 (5%); dysgeusia, 4 (9%); and dysphagia, 2 (5%), which did not differ between patients with complete and partial excision of the SLG (P > .1). Numbness, dysgeusia, and dysphagia were defined as symptoms that persisted significantly for >10 days after surgery. However, neurologic complications spontaneously resolved within the first postoperative month. For a median follow-up of 36 months, recurrence occurred in 5 of 20 patients with partial SLG excision but none of 22 patients with complete SLG excision (P = .018). All recurrent cases occurred within the first postoperative year but none thereafter. The patients with recurrence underwent complete excision of the remnant SLG on the affected side and experienced no further recurrence afterward.
Discussion
This study showed the lowest complications and recurrence from SLG excision with the simple evacuation of cystic fluid. The complications were minor and spontaneously resolved within the first postoperative month. The operation time and surgical complications were comparable between patients with complete and partial excision of the SLG. Postsurgical recurrence occurred only after partial excision of the affected SLG but not after complete excision. Therefore, the results might deny the null hypothesis that partial excision of the SLG is effective to treat plunging ranula in terms of reduced operation time and surgical morbidity but no increased recurrence rate when compared with complete excision of the SLG. Accordingly, this study suggests that complete excision of the SLG rather than partial excision is recommended to treat plunging ranula.
Plunging ranula has been treated by ≥10 methods with different morbidity and cure rates.5,6 An early literature review showed the highest success rates of treating plunging ranula when the SLG was removed: 96% in SLG excision alone; 95% in SLG plus ranula excision; 95% in SLG plus submandibular gland (SMG) excision; and 92% in SLG, SMG, and ranula excision. 6 Ranula excision alone, SMG plus ranula excision, marsupialization, and incision and drainage had the lowest success rates: 38%, 55%, 38%, and 4%, respectively. 6 Sclerotherapy with OK-432 intracystic injection had a 59% success rate. 6 Therefore, removal of the affected SLG is recommended for the effective treatment for plunging ranula. 6 A recent meta-analysis from 39 clinical studies with evidence level 4 compared the outcomes of treatment for oral and plunging ranulas. 5 When 3 treatment methods for plunging ranula were categorized, transoral excision of the SLG showed the highest cure rate (98.9%; 95% CI, 97.4%-99.8%) when compared with transcervical excision of the SLG and ranula (91.5%; 95% CI, 80.0%-98.4%) and intracystic injection of OK-432 (65.6%; 95% CI, 39.0%-87.8%). 5 In terms of postoperative complications, hematoma and nerve dysfunction were less common after transoral SLG excision than after transcervical SLG excision, although statistical significance did not differ because of the inconsistent description or high heterogeneity (I2 > 60%) of the studies. 5 The findings were consistent with those of the present study showing no recurrence and minor complications of transoral complete SLG excision.
The SLG is located in the complicated anatomy structures among the floor of mouth, mandible, and mylohyoid muscle. 13 The surrounding structures include the lingual nerve, the Wharton’s duct, the sublingual and submental arteries and veins, branches of the hypoglossal nerve, the submandibular ganglion, and extrinsic tongue muscles. 13 Despite the smallest major salivary gland, the SLG contributes to approximately 5% of whole oral salivary secretion. 8 Complete excision of the unilateral SLG may require a considerable mean operation time of 75 minutes when transorally treating plunging ranula, according to a previous report. 14 The procedure may involve injury to structures adjacent to the SLG, particularly the Wharton’s duct and the lingual nerve. 13 These might be reduced by excision of only some part of the SLG that appeared to cause plunging ranula. However, the present study failed to show any advantage of partial over complete SLG excision in terms of operation time and complication rates. Instead, the remnant SLG tissues caused no sealing of the leak through which mucus extravasated and mucus recollection in the previous ranula pocket below the mylohyoid muscle. Therefore, the present and recent studies have advocated for full resection of the SLG to prevent recurrence.14-17
Complete excision of the affected SLG was safe and reliable without major complications and recurrence. The follow-up period in this study was too short to identify the complete recurrence rate after surgery, yet it might be sufficient to observe most relapse cases because of the occurrences within 1 year. This is the first study to compare 2 surgical procedures of complete vs partial SLG excision in treating plunging ranula. However, nonrandomization and no blinding in treatment allocation might have caused bias that hindered reliable outcomes. The lack of a sample size calculation may also make it difficult to generalize the results of this study. Nonetheless, useful conclusions might be provided by the present study—that is, the sequential allocation of complete and partial SLG excision was adopted because of the relative rarity of the disease entity and small number of patients.
Conclusions
This study compared the clinical outcomes of complete vs partial excision of the affected SLG in the treatment of plunging ranula. Operation time and complication rates were comparable between the surgical procedures with the simple evacuation of cystic content. However, partial SLG excision showed a 25% relapse rate, but complete SLG excision had no relapse. Therefore, complete excision of the SLG is recommended to treat plunging ranula for reducing postsurgical risks of complications and recurrence.