
Abstract
Objective
To measure the craniovertebral angle during tonsillectomy, assess the interrater reliability of our methodology, and investigate the correlations of the Rapid Upper Limb Assessment and the craniovertebral angle to quantify ergonomic risk.
Study Design
Prospective, observational study.
Setting
Tertiary care pediatric institution.
Methods
Neck posture was evaluated for 92 images with 7 surgeons. Lateral images of the surgeon were captured every minute in a standardized method. Images were assessed by 3 raters, measuring the craniovertebral angle, defined as the angle between a horizontal line through the C7 vertebrae and another line through C7 and the tragus of the ear. Interrater reliability of the craniovertebral angle was evaluated using the κ statistic. Per prior publications, reports of neck pain were frequent when the craniovertebral angle value was <50°; thus, we defined an abnormal posture if the craniovertebral angle was <50°.
Results
Mean (SD) craniovertebral angle during tonsillectomy was 26.0° (11.3°). One hundred percent of procedures had at least 1 assessment of abnormal posture. The lowest interrater reliability was 0.77 (CI: 0.67-0.87). Rapid Upper Limb Assessment and craniovertebral angle (CA) correlation was −0.12 (P = .27) and, therefore, null.
Conclusion
Poor posture during tonsillectomy places otolaryngologists at intraoperative ergonomic risk. The craniovertebral angle is a predictor of future neck pain, and a pathologic neck position during tonsillectomy was identified. Given the high interrater reliability, our approach to assessing intraoperative surgical ergonomics was validated. Overall, RULA and the CA are not a substitute for one another but complementary.
The goal of ergonomics is to create a work environment that enables the worker to complete their job efficiently and safely. Sustained poor posture may lead to musculoskeletal (MSK) conditions resulting in injury, time off work, and added costs. From 2009 to 2011, 33.2% of the population reported having MSK conditions with an associated increase in the number of physician office visits and use of prescription medications. 1 Accordingly, during the same study period, an average of 20.8 prescriptions were filled per person for these MSK complaints. 1 Overall, the economic impact of these conditions is substantial—estimated as being close to $212 billion in 2009 to 2011. 1
MSK injuries are particularly relevant to surgeons, as approximately one-third of their time at work is spent in the operating room. 2 In a survey of otolaryngologists, 97% of participants reported experiencing MSK symptoms during their career. 3 Poor surgical ergonomics related to repetition results in over half of days off work being caused by overexertion and overuse.4-7 The high work posture stress load in surgeons, which leads to poor surgical ergonomics, has been attributed to the high prevalence of static work postures during operative cases. 8 Specific to otolaryngology, surgical intervention in the oral cavity can require abnormal neck posture, resulting in a compromise in surgical ergonomics. It has been established that a forward head position (FHP) can lead to a shift in the center of gravity, with the upper body drifting backward and creating ergonomic risk that can result in injury. 9 As a compensation to upper body drift, both hips typically tilt forward, and in this way, FHP not only can be the source of neck pain but can also cause back pain. 9
Rates of musculoskeletal disorders in surgeons, and otolaryngologists specifically, have been increasingly reported in the literature.2,4,10 Using the Rapid Upper Limb Assessment (RULA), our group has previously established that tonsillectomy places the surgeon at higher ergonomic risk, particularly in the neck and trunk regions. 11 With such a great prevalence of ergonomic risk, there is a need to mitigate at-risk posture in the operating room (OR) through interventions. While the RULA and the Rapid Entire Body Assessment (REBA) provide rapid evaluation of ergonomic positioning during surgery, these measures often lack granularity. To assess the impact of ergonomic interventions, more precise quantification methods are needed.
Objective and more precise quantification, specifically of the high-risk neck region, can be obtained through utilization of the craniovertebral angle (CA). The CA measures FHP, and Ruivo et al 12 showed that cases with FHP associated with neck pain had a CA <50°. Lower CA values confer higher ergonomic risk, and those who consistently maintain CA values less than 50° have been shown to be at risk for neck pain, temporomandibular disorders, and cervicogenic headaches.12,13 In addition, in another study, patients with tension headaches showed a smaller CA (mean angle 45.3°± 7.6°) than healthy control subjects (mean angle 54.1°± 6.3°). 13 A study of spinal surgeons found that the CA remained <25° for each participating subject during the entirety of the procedure. 9 Given the importance of surgical ergonomics on physician quality of life, productivity, and career length, the aim of our study was to measure the CA during tonsillectomy, validate the interrater reliability of our methodology, and investigate the correlations of RULA and CA to quantify ergonomic risk during tonsillectomy. The authors hypothesized that during tonsillectomy, otolaryngologists assume at-risk CA values, which can be reliably quantified intraoperatively. Given this study’s small scale, it is a pilot study that provides suggestive conclusions in using this method for future large-scale ergonomic studies.
Methods
Participants
All resident and attending otolaryngologists at a tertiary, academic children’s hospital were recruited voluntarily and invited to participate in intraoperative assessment. This study was approved by the institutional review board at Nationwide Children’s Hospital (STUDY00000359).
Data Collection
A prospective, observational study was completed by 3 research associates over a 4-week period. The 3 reviewers comprised 2 postbaccalaureate research associates and 1 research fellow who had completed otolaryngology residency. All were trained in measurement of CA by 1 member of the research team with expertise in ergonomics research. CA was quantified by collecting lateral images of the surgeon while performing the intervention (tonsillectomy). Participants were instructed to perform the procedure in a standard fashion. No efforts were made to normalize chair height, bed height, Mayo stand positioning, or other variables, as our intent was to assess CA reliability between raters and validity with RULA. Images were captured at a standardized distance of 8.75 feet, and height was adjusted to include head, neck, and upper back of the surgeon in a sagittal plane. One image was captured, using a tripod with a built-in level, each minute during the intervention for the duration of the procedure. Representative images were captured with some variability in CA throughout the procedure. By capturing random photos continuously, the objective was to avoid bias and record the surgeon in normal positioning. Surgeon identifier, level of training, date of surgery, technique for tonsillectomy, and length of the procedure were recorded. A total of 92 images during 11 procedures were obtained. Neck posture was evaluated by measuring the CA; images that demonstrated lateral tilt of the head were excluded (10 images).
CA was defined as the angle between a horizontal line through the C7 vertebrae and another line that begins at C7 and traverses the tragus of the ear ( Figure 1 ). As a CA of <50° correlates with neck pain, temporomandibular disorders, and cervicogenic headaches, we defined an abnormal posture if the CA was <50° ( Figure 2 ).12,13 The consistency of a measure is reported through reliability, and in this study, interrater reliability of CA was assessed for 3 raters using the κ statistic (35 images). Images were assigned by the primary author and then reviewed independently by each reviewer to determine interrater reliability. High interrater reliability was established; the lowest κ observed between the 3 raters was 0.77 (CI: 0.67-0.87).
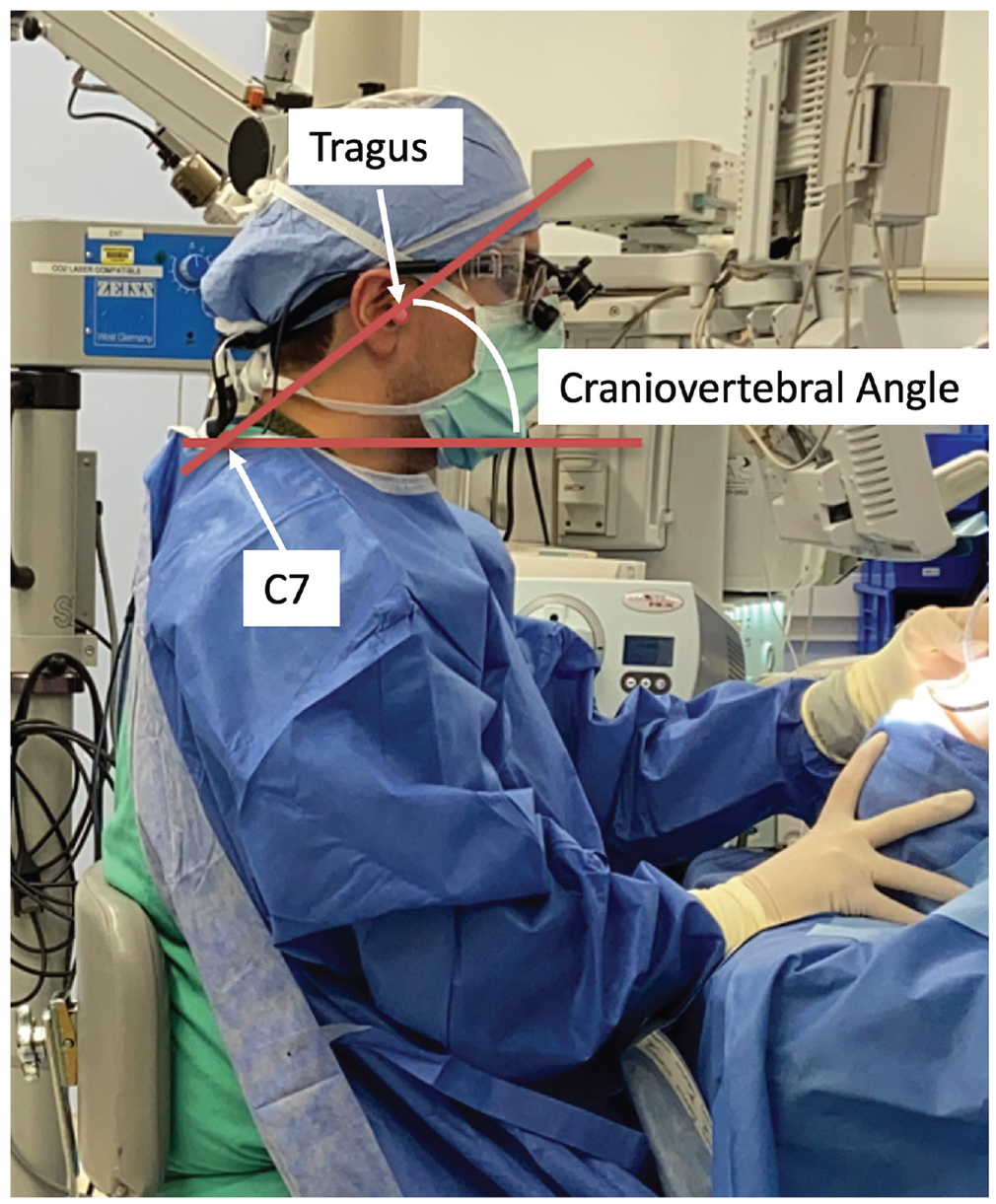
Example of craniovertebral angle.
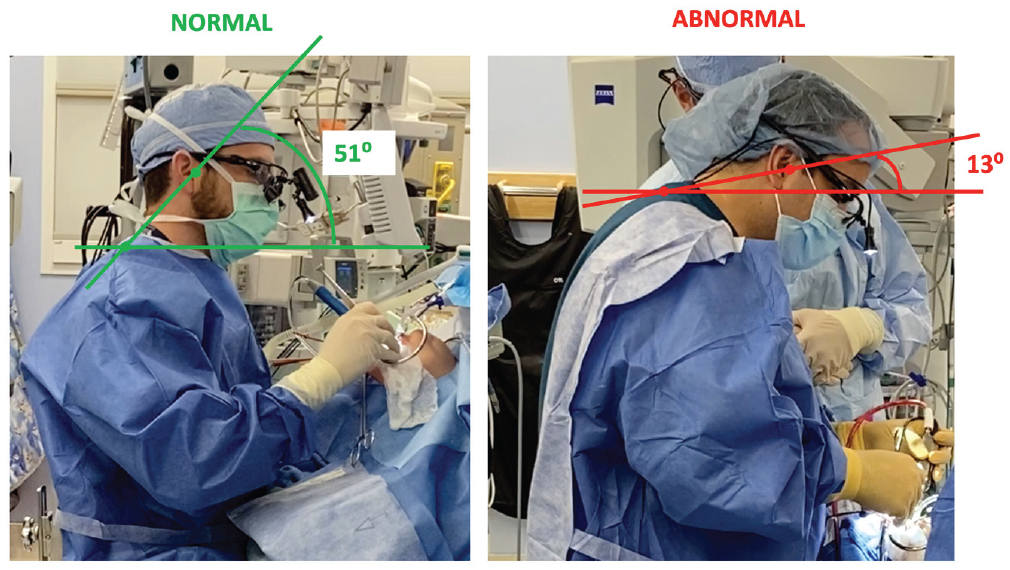
Normal vs abnormal craniovertebral angles.
Images were then quantified using RULA. RULA is a validated, objective assessment of ergonomic risk for sustained postures.14,15 RULA evaluates arm, wrist, neck, trunk, and leg positioning, along with the duration and force of postures. Scores range from 1 to 7 with a score of 1 to 2 representing an acceptable posture, 3 to 4 necessitating further investigation as change may be needed, 5 to 6 justifying further investigation to implement a change soon, and 7 requiring immediate investigation and implementation of changes.
Statistical Analysis
The CA and RULA were described with means and standard deviations. Thresholds for these assessments (CA <50° and RULA <3) were summarized with proportions. Correlation between the continuous CA and RULA was assessed using the Pearson correlation coefficient. Finally, we evaluated the relationship between surgeon and procedure characteristics using a mixed-effects linear regression model with a random intercept for each procedure. All analyses were performed in SAS Enterprise Guide Version 8.1 (SAS Institute), and statistical significance was evaluated using an α of .05.
Results
CA Reflects At-Risk Posture During Tonsillectomy
Seven surgeons (3 resident surgeons, 4 attending surgeons) were evaluated during tonsillectomy (N = 11). Ninety-two images were obtained, yet those that contained a lateral tilt of the head or were taken when the surgeon was not actively operating were excluded, thus resulting in 82 eligible images. CA mean (SD) of each subject ranged from 13.5° to 36.3° (4.8° to 11.9°). The mean (SD) CA across all samples was 26.0° (11.3°), within the range of abnormal posture that was defined as a CA <50°. Only 5% (n = 4) of images had negligible risk with CA ≥50°. Of the 11 tonsillectomies, 1 procedure had 43% (3 of 7) images with favorable (not at-risk) CA angles. One procedure had 10% (1 of 10) images captured with favorable CA, and the remaining 9 procedures had 0% (0 of 3-12 images/surgery) with favorable CA angles, which overall represents poor CA throughout most procedures.
CA Correlates With the Neck, Trunk, and Leg Scores of RULA
The mean (SD) RULA was 3.2 (0.6), and only 1% (n = 1) of images had scores that represented an acceptable posture ( Figure 3 ). The mean (SD) RULA wrist/arm score was 3.5 (0.7), and the mean (SD) RULA neck, trunk, and leg score was 2.8 (1.2).
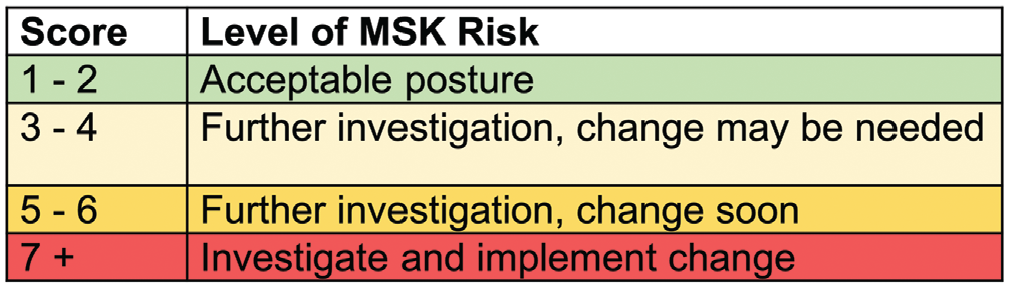
Level of musculoskeletal (MSK) risk based on final Rapid Upper Limb Assessment score. 15
RULA neck, trunk, and leg score was moderately correlated with CA (r = -0.46, P < .0001) ( Figure 4 ). However, as CA improved, the RULA wrist/arm score worsened (r = 0.29, P = .01). Due to the paradoxical improvement in the neck, trunk, and leg score with worsening in the wrist/arm score, the overall RULA and CA correlation was null (r = −0.12, P = .27).
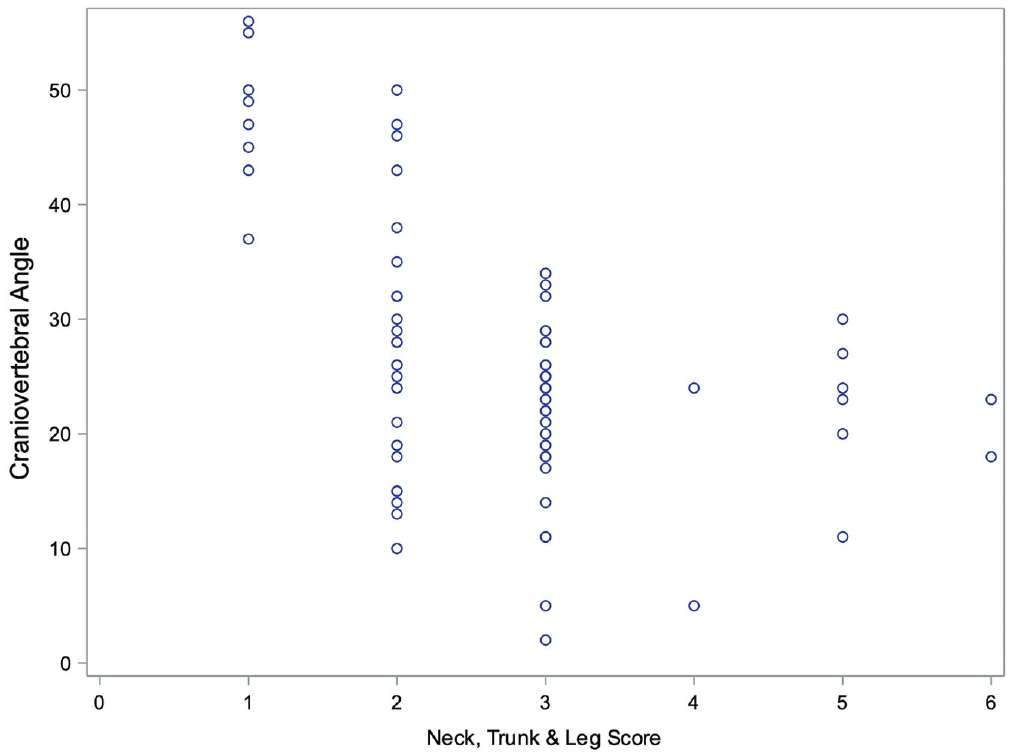
Scatterplot of craniovertebral angle and Rapid Upper Limb Assessment neck, trunk, and leg score.
In considering other variables in our data ( Figure 5 ), CA does vary by physician training level. Attendings were found to have poorer CA than residents (CA difference = 10.4, P = .05). No effect was observed with surgical technique (P = .78) and length of surgery (P = .47).
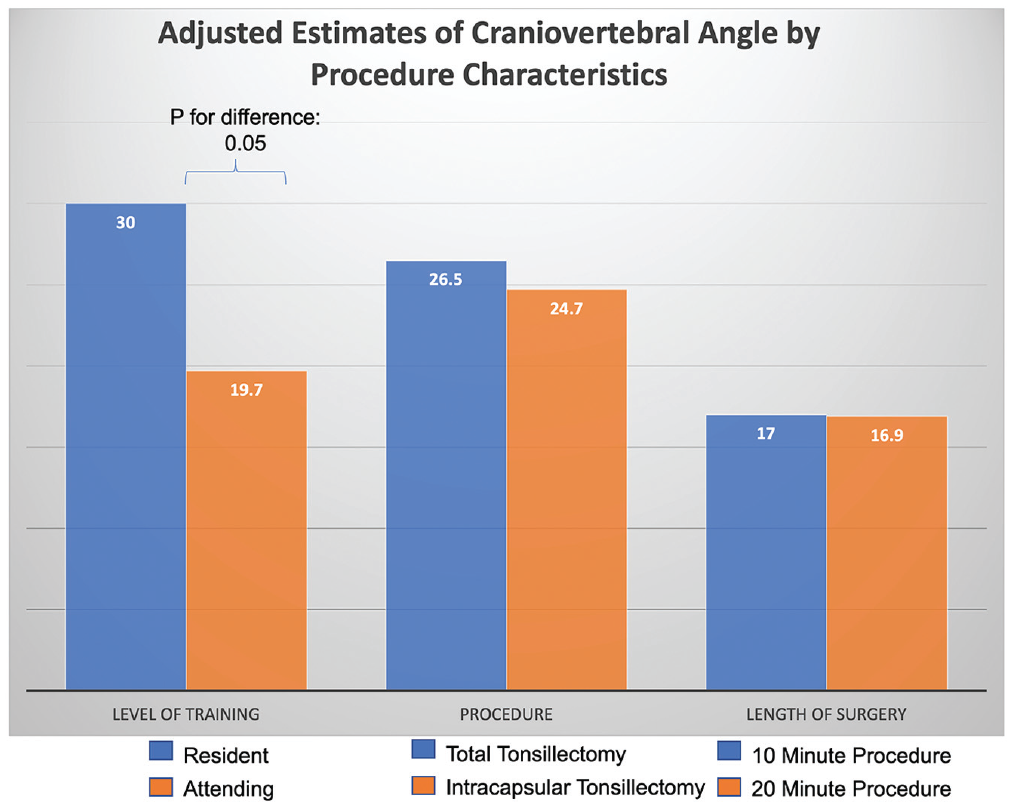
Craniovertebral angle and procedure characteristics. CA, Craniovertebral angle.
Discussion
Surgical ergonomics has been shown to have a strong effect on career longevity, rate of work-related injuries, and productivity. The CA is an important predictor of neck pain and injury through its ability to measure FHP. As the FHP increases, so too does the load exerted on the spine by the head. In the current study, a pathologic neck position during tonsillectomy was identified, with all of the procedures having at least 1 assessment of abnormal CA posture. This implies that surgeons are subjecting themselves to greater ergonomic risk throughout the day, especially during tonsillectomies. It should be noted that there are advantages to using the CA, for the CA has a wide range of possible values and is not category based like RULA. In this way, the CA allows us to detect changes over time that are potentially a result of interventions. Overall, RULA and the CA are not a substitute for one another but complementary.
To further establish the consistency of CA, we investigated the interrater reliability of CA measurements and found this to be high. In addition, in assessing the validity of CA as a predictor of MSK injury, the 82 images of CA values were evaluated with RULA scores of ergonomic risk. Using CA and RULA to assess ergonomics, we observed that just 5% of surgeons had negligible risk using the CA and 1% had acceptable posture using RULA. This suggests that CA can be used in future studies to objectively quantify surgical ergonomics, as well as monitor the effect of intraoperative interventions designed to mitigate ergonomic risk. In our cohort, the average CA value of 26.0° was far below the acceptable range, reinforcing our prior findings that even common, short procedures for otolaryngologists pose significant ergonomic risk.
In assessing the correlation of CA and RULA, the RULA neck, trunk, and leg score and CA complement one another in indicating ergonomic risk, for as the CA increased or improved, RULA decreased, and therefore less ergonomic risk was present. There was also correlation in that as the CA improved, the RULA wrist/arm score became worse. This contradictory relationship between different components of RULA and CA ultimately resulted in no correlation between overall RULA and CA. Given that the RULA neck, trunk, and leg score measures FHP, which affects CA, it is unsurprising that a correlation exists between the 2 measures. The inverse correlation between the CA and RULA wrist/arm score may be explained by the need for more extreme positioning of the wrists and arms when trying to sustain a posture with less FHP. As future interventions are being considered, it would be beneficial to consider its implications on all parts of the body.
Attending surgeons were found to have a lower CA and therefore worse posture when compared to residents. With greater emphasis being placed on ergonomics research and training in recent years, our findings align with the hypothesis that younger generations are possibly taking greater effort to sustain better posture. Alternatively, a lower CA in attending surgeons can potentially be attributed to repetitive maintenance of poor posture over time in comparison to residents in early stages of their career. In addition, both total and intracapsular tonsillectomies were evaluated, but no significance was discovered between the two in regard to the CA. Since these techniques are similar to one another, it does align that surgeons sustain similar CA values during these procedures for required visualization. Finally, no difference was found between the CA and length of surgery. More research is needed for this finding, for we would hypothesize that a longer surgery would tire the surgeon, thus leading to a greater FHP and a smaller CA. While data were collected in this study at 1-minute intervals with photography, it may be interesting to evaluate more granular time points.
The strengths of this study are that a standardized approach was used to capture the images, thereby reducing errors related to data collection and assisting in the creation of a reliable assessment, as reflected by our high interrater reliability values. In addition, the utilization of the CA to assess ergonomic risk in pediatric otolaryngology was a novel application. However, our study is not without limitations. Intrinsic to the assessment tool, CA itself is limited in that it does not account for lateral head tilt—a position conferring greater ergonomic risk. In obtaining the representative images, the surgeons were aware that they were being photographed, which introduces observation bias and may have contributed to an overestimation of CA. In addition, since this study was completed at a single institution, there were a limited number of subjects, which may have reduced power. Furthermore, recruitment was voluntary, and in this way, bias was introduced because those who agreed to participate were likely more interested in ergonomics and an objective assessment of their intraoperative postures. Finally, the analyses evaluating CA differences by type of tonsillectomy, length of surgery, and start time were underpowered. It is unlikely that the type of tonsillectomy is associated with CA, but for the other characteristics, to achieve 80% power at an α of .05 under the conditions of this study, future work should include a sample size of 106 patients to demonstrate a statistically significant difference in CA.
There is a need for future work and interventions in order to decrease ergonomic risk for pediatric otolaryngologists. The authors selected tonsillectomy because, relative to myringotomy and tympanostomy tube placement, it was associated with greater ergonomic risk, yet future work will include other procedures. Furthermore, ergonomic training, added equipment, and other solutions may help decrease the prevalence of ergonomic risk.
Conclusion
In this pilot study, the authors’ findings suggest that a pathologic neck position is present during tonsillectomy. In addition, this method in measurement of the CA revealed high interrater reliability. There was a correlation between CA and RULA, but the overall correlation was null. Future studies in surgical ergonomics may use the authors’ method in measurement of CA and RULA.
Footnotes
This article was presented virtually at the AAO-HNSF 2020 Virtual Annual Meeting & OTO Experience, September 13 to October 25, 2020.