
Abstract
Objective
To compare outcomes after tracheostomy between children from Spanish- and English-speaking families.
Study Design
Prospective cohort study.
Setting
Tertiary care children’s hospital.
Methods
All children <18 years of age who had a tracheostomy placed between 2014 and 2020 were included. Comorbidities and postsurgical outcomes were compared between (1) children whose families preferred speaking Spanish or identified as Hispanic/Latino and (2) children from English-language or non-Hispanic families.
Results
A total of 339 children met inclusion, with 11% (37/339) from families identifying Spanish as their primary language and 33% (112/339) identifying as Hispanic. Spanish-speaking families were more likely to have tracheostomy-dependent children with cardiac conditions (65% vs 42%, P = .008) and high complexity (72% vs 49%, P = .007). Outcomes were similar regardless of language preference, with 45% (153/339) still tracheostomy dependent, 28% (94/339) decannulated, and 6.8% (23/339) deceased at a median follow-up of 1.77 years (interquartile range, 0.65-3.43). Severe neurocognitive disabilities were similar between Spanish- and English-language families (P > .05). Spanish language was not associated with times to decannulation or death in univariate or multiple regression models. A sensitivity analysis of self-identified Hispanic or Latino patients did not show significant differences for time to decannulation, death, or neurocognitive disability rates (P > .05).
Conclusion
Spanish language and Hispanic ethnicity appear to have minimal impact on pediatric tracheostomy outcomes.
Children from non-English-speaking families face increased health disparities as compared with those from English-speaking households. 1 Limited English proficiency results in decreased access to medical care even when controlling for socioeconomic factors, health status, race, and ethnicity. 2 The most recent estimate from US Census data suggests that 60 million Americans >5 years old speak a language other than English at home, with Spanish representing the majority. 3 A growing population of patients with limited English proficiency faces potential health care barriers that lead to miscommunication 4 and poorer outcomes.5,6
Spanish-speaking patients present unique challenges in pediatric otolaryngology. Families speaking Spanish feel less satisfied with various aspects of care as compared with English-speaking families. 7 Hispanic patients have poorer outcomes for frequent ear infections 8 and cochlear implantation 9 and are less likely to be diagnosed with common pediatric otolaryngologic conditions. 10 In-person Spanish interpreters may positively influence some of these issues, 11 but understanding how language and ethnicity affect otolaryngology care in the Spanish-speaking community is necessary.
To date, the relationship between preferred language and pediatric tracheostomy outcomes has been unexplored. Tracheostomy-dependent children with community health disparities encounter longer hospitalization lengths and total costs regardless of medical complexity. 12 Some of these discharge obstacles could be language related, similar to those identified in discharges and readmissions after adenotonsillectomy.13,14 As a result, recognizing barriers in the Spanish-speaking community may provide institutions with targets for tracheostomy-based quality improvement initiatives. The primary objective of this study is to determine if language and ethnicity influence index admission outcomes after pediatric tracheostomy in Spanish-speaking families. Secondary objectives assessed key clinical milestones, such as decannulation and mortality, with the relationship between these metrics and Hispanic ethnicity. We hypothesized that tracheostomy-dependent children with Spanish-speaking caregivers would have poorer outcomes as compared with those speaking English.
Methods
A prospective cohort study of all children who underwent tracheostomy between January 1, 2014, and June 30, 2020, was initially performed as a quality improvement project. Review of these data was approved by the University of Texas Southwestern Medical Center Institutional Review Board (STU-2019-1103). The Children’s Health Airway Management Program (CHAMP) prospectively enrolls children in a registry within the electronic medical record upon tracheostomy placement. The database, maintained by CHAMP, is checked monthly for accuracy and follows each child until decannulation, adulthood (21 years old), or death. Only patients who underwent tracheostomy at Children’s Medical Center Dallas were included. Revision procedures or tracheostomies placed at outside institutions were excluded. Children’s Medical Center Dallas is a tertiary children’s hospital in North Texas that serves a large Spanish-speaking and Hispanic population. Patients and providers have access to 24/7 in-person Spanish-language interpreters and remote video interpretation services to supplement live interpreter services. Also, patients are provided translated versions of all information and documentation available to patients and their families. Furthermore, many of the staff members are certified bilingual and can communicate with families during their hospitalization, ambulatory visits, or telephone communications. This provides outstanding access to written and verbal communication for Spanish-speaking families.
The primary outcome compared index admission metrics between children from families with Spanish-language preference and those who preferred English. Children from families speaking languages other than English or Spanish were excluded. Secondary outcomes compared key postsurgical clinical metrics at latest follow-up between language preference groups and assessed the impact of Hispanic ethnicity. Language or ethnic designations were self-selected by the primary caregivers. The following demographics were identified: age at tracheostomy (months), sex (male/female), race (American Indian, Asian, Black or African American, other, White), ethnicity (Hispanic or Latino/non–Hispanic or Latino), preferred language (English/Spanish), gestational age (weeks), birth weight (kilograms), perinatal complications (yes/no), percentage poverty by zip code, and expected payer (Medicaid/private).
Metrics recorded from the index admission were as follows: primary indication for tracheostomy (respiratory failure, airway obstruction, secretion control); complex case, defined as total parental nutrition, a history of sepsis, or major cardiac surgery (yes/no); and weight at tracheostomy (kilograms). CHAMP also monitors accidental tracheostomy decannulation (yes/no) and other tracheostomy-related complications (yes/no). Tracheostomy-related complications are identified by ICD-10-CM terminology (hemorrhage, infection, malfunction, and unspecified; International Classification of Diseases, 10th Revision, Clinical Modification). Tracheostomy infection includes granulation tissue and stomal irritation, while malfunction comprises stenosis attributed to tracheostomy tube and false tract placement. An unspecified tracheostomy-related complication consists of mucus plugging and accidental decannulation.
Key morbidity diagnoses were conditions that were present on admission or during the index stay. These were based on ICD-10-CM coding schemes: short gestation <37 weeks (P07), congenital malformations (Q00-Q99), complications of birth (P02), sepsis of newborn (P36), maternal complications of pregnancy (P01), respiratory distress syndrome of newborn (P22), birth hypoxia (P20-P21), sepsis (A40-A41), cardiac conditions (I00-I99), chronic respiratory disease (P27, J96.1), and unintentional injuries (V01-X59).
Index discharge information was as follows: total length of stay (days), posttracheostomy length of stay (days), disposition (home, short-term rehabilitation facility, in-hospital mortality), mechanical ventilation at discharge (yes/no), 30-day all-cause readmission (yes/no), readmission cause (tracheostomy related, disease related, other), and time to first follow-up appointment (days).
Key posttracheostomy outcomes included status (alive with tracheostomy, decannulated, deceased, lost to follow-up), ventilatory requirement (yes/no), and severe neurocognitive disability (yes/no). Neurocognitive disability was defined as severe if a child could not be educated among peers in a traditional classroom setting (eg, global developmental delay).15,16
Continuous data are presented as medians with interquartile range (IQR). Categorical data are presented as counts with percentage. The univariate analysis used 2-sample Wilcoxon rank sum (Mann-Whitney) tests for continuous variables and the Pearson χ2 test for categorical variables. Median time to decannulation and death was determined and used to compare differences between groups with a log-rank test of equality. Relationships were explored through parametric survival analysis (Weibull distribution). The model was created with forward stepwise regression to determine which variables were significantly associated with time to decannulation or death. Variables where P > .05 were removed until the final model was determined. Language and ethnicity were added to the model to see if they significantly influenced the time to death or decannulation while controlling for other covariates. The model’s fit was determined with visual inspection and is presented in tabular form.
All analyses were performed with Stata 17 (StataCorp). Statistical significance was set to P < .05. This study adhered to STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology) for observational studies. 17 Data were collected and managed via REDCap tools (Research Electronic Data Capture) hosted at the University of Texas Southwestern Medical Center.18,19 To account for multiple comparisons, priority is given to the analysis of language and Hispanic ethnicity and less to any secondary findings of significance. Missing values are handled by listwise deletion.
Results
A total of 339 children underwent tracheostomy during the study period. The median age at tracheostomy was 6.9 months (IQR, 4.0-46.3) and 54% were male (183/339). Children from Spanish-speaking families represented 11% (37/339) of the population, while 33.0% of children were Hispanic or Latino (112/339). The racial distribution was as follows: 3.0% Asian (10/339), 31% Black or African American (106/339), 54% White (196/339), 2.1% >1 race (7/339), and 5.6% unknown/not reported (19/339). Among families who prefer to speak Spanish, 89% identified as White (33/37). The median gestational age was 36 weeks (IQR, 28-39); the median birthweight was 2.4 kg (IQR, 1.1-3.1); and 58% (194/339) had a complication of birth or delivery. Most children (77%, 259/339) used Medicaid as their primary payer, and the median percentage poverty by zip code was 14.9% (IQR, 8.3%-23.9%). Baseline characteristics were similar between those who preferred to speak Spanish and English except for the proportion of Hispanic patients (100% vs 25%, P < .001) and White patients (89% vs 54%, P = .001; Table 1 ).
Demographics of Children With Tracheostomies by Language. a
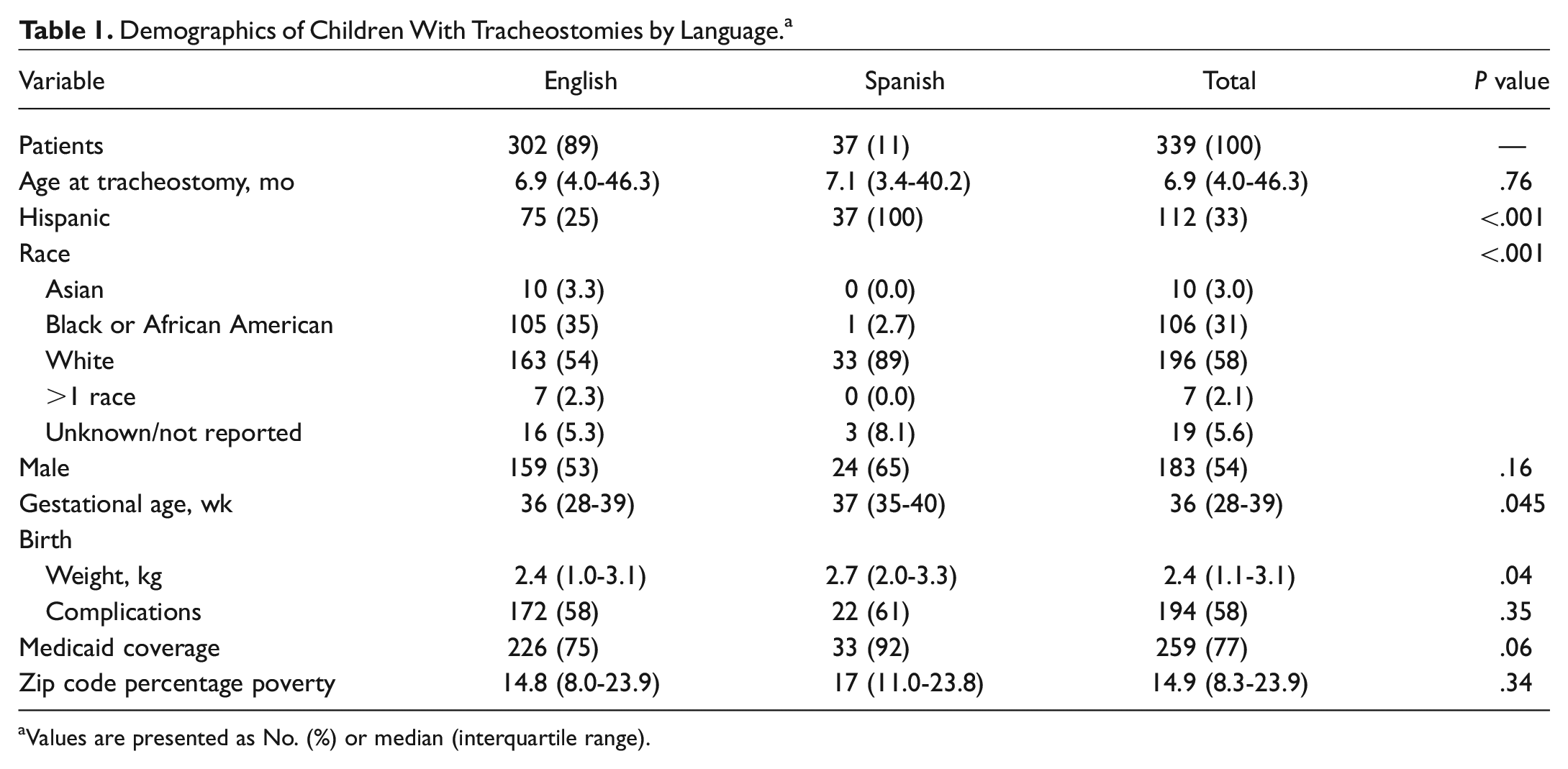
Values are presented as No. (%) or median (interquartile range).
Table 2 compares the key mortality-related diagnoses and other index hospitalization data. Spanish-speaking families were more likely to have tracheostomy-dependent children with cardiac conditions (65% vs 42%, P = .008) and patient complexity (72% vs 49%, P = .007). Families of Spanish-language preference were less likely to have maternal complications (11% vs 29%, P = .02). All other conditions were statistically similar between language groups.
Index Hospitalization Characteristics of Children With Tracheostomies by Language. a
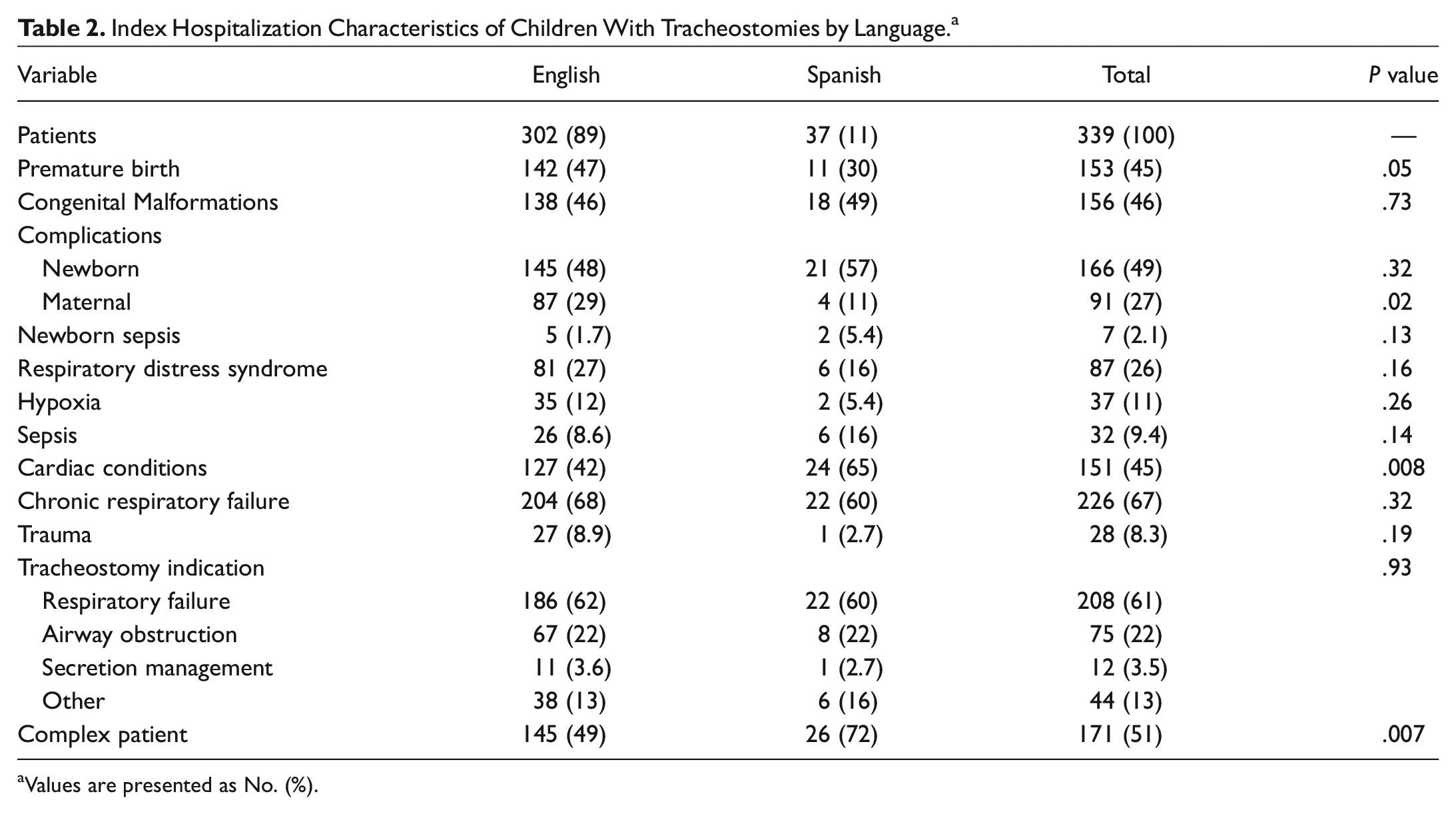
Values are presented as No. (%).
Discharge outcomes were similar between the language preference groups ( Table 3 ). The median length of stay was 91 days (IQR, 43-160), and discharges to a short-term rehabilitation hospital occurred for 49% (166/339). Most were discharged on mechanical ventilation (72%, 234/339). The 30-day all-cause readmission rate was 19% (63/339), and 37% were related to the tracheostomy (23/63).
Discharge and Follow-up Data of Children With Tracheostomies by Language. a
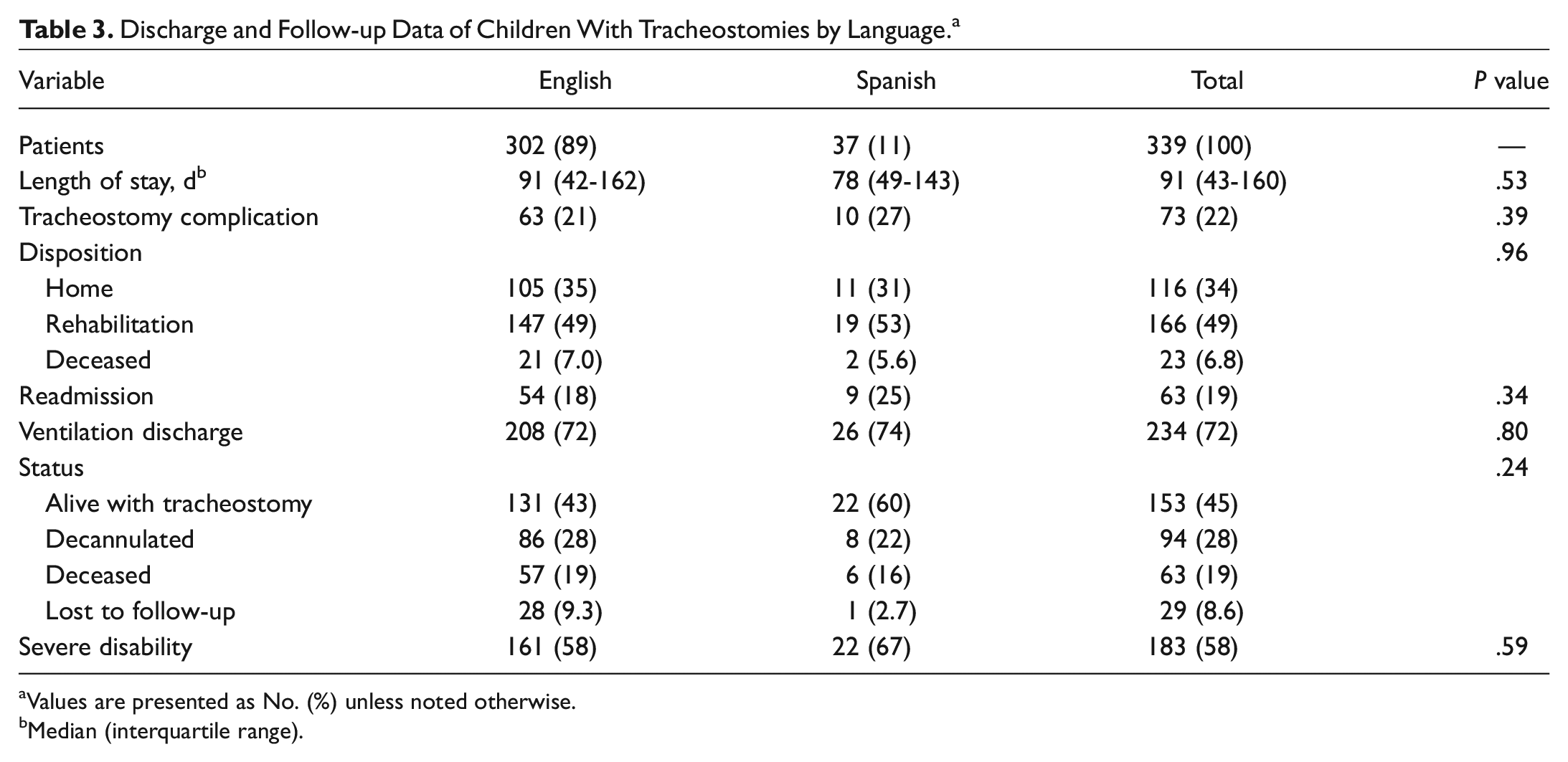
Values are presented as No. (%) unless noted otherwise.
Median (interquartile range).
No differences in key postsurgical outcomes were identified between groups at a median 1.77 years (IQR, 0.65-3.43) of follow-up. Specifically, 45% (153/339) still had a tracheostomy in place; 28% (94/339) were decannulated; and 19% (63/339) had died. Severe neurocognitive disabilities were diagnosed in 58% (183/339) of children. Twenty-nine patients were lost to follow-up. See Table 3 for complete comparisons.
Time to decannulation or death was similar between children from Spanish- and English-speaking families. The median time to decannulation was 1.40 years (IQR, 0.73-3.01) for Spanish speakers and 1.95 years (IQR, 0.71-3.30) for English speakers. The median time to death was 0.70 years (IQR, 0.16-1.89) for Spanish speakers vs 0.57 years (IQR, 0.15-1.66) for English speakers. A multiple parametric survival analysis identified mechanical ventilation at discharge, accidental injury, and Medicaid payer as being significantly associated with time to decannulation. The variables of unknown/not reported race and a history of congenital malformations were significantly associated with time to death. Spanish language was not associated with times to decannulation or death in univariate or multiple regression models ( Tables 4 and 5 ).
Multiple Variable Parametric Survival Analysis of Decannulation Among Children With Tracheostomies.
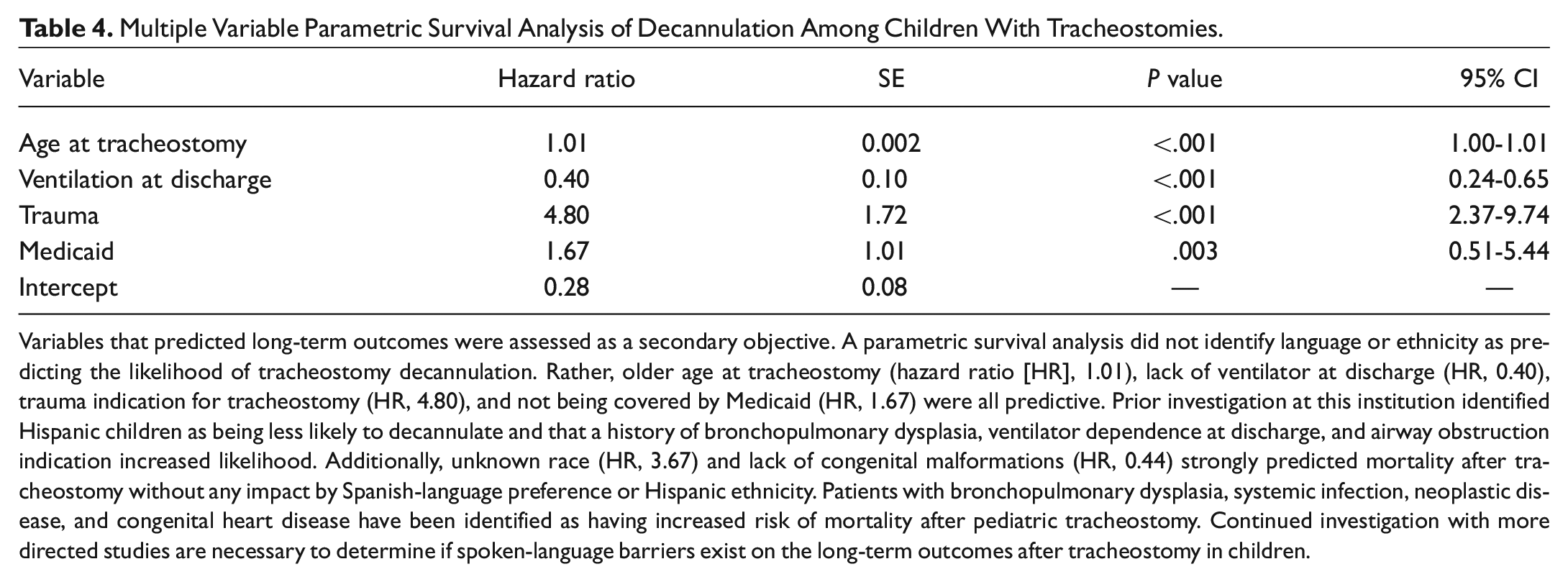
Variables that predicted long-term outcomes were assessed as a secondary objective. A parametric survival analysis did not identify language or ethnicity as predicting the likelihood of tracheostomy decannulation. Rather, older age at tracheostomy (hazard ratio [HR], 1.01), lack of ventilator at discharge (HR, 0.40), trauma indication for tracheostomy (HR, 4.80), and not being covered by Medicaid (HR, 1.67) were all predictive. Prior investigation at this institution identified Hispanic children as being less likely to decannulate and that a history of bronchopulmonary dysplasia, ventilator dependence at discharge, and airway obstruction indication increased likelihood. Additionally, unknown race (HR, 3.67) and lack of congenital malformations (HR, 0.44) strongly predicted mortality after tracheostomy without any impact by Spanish-language preference or Hispanic ethnicity. Patients with bronchopulmonary dysplasia, systemic infection, neoplastic disease, and congenital heart disease have been identified as having increased risk of mortality after pediatric tracheostomy. Continued investigation with more directed studies are necessary to determine if spoken-language barriers exist on the long-term outcomes after tracheostomy in children.
Multiple Variable Parametric Survival Analysis of Death Among Children With Tracheostomies.

A sensitivity analysis of self-identified Hispanic or Latino patients did not show significant differences for the primary outcomes or secondary outcomes of decannulation, death, or neurocognitive disability. Differences in proportions were present were for the following variables: gestational age, birth weight, and Medicaid payer. No cross-level interactions or effect modifiers were identified.
Discussion
This large cohort study of tracheostomy-dependent children identified similar rates of decannulation, mortality, and neurocognitive disability between Spanish- and English-speaking families. Although non-English-speaking families encounter a variety of poorer health outcomes,1,2,5,6 this is the first study examining potential barriers with regard to tracheostomy in children. Hispanic children also did not have differences in outcomes, which has been recognized for several other conditions in pediatric otolaryngology.8-10 This suggests that factors beyond spoken language, such as patient complexity 20 and socioeconomic status, 12 are stronger predictors of tracheostomy-related outcomes.
The relationship between non-English-speaking patients and health disparities has drawn interest. For a number of patients, nonfinancial barriers to care include language, culture, and logistical challenges, such as inconvenient appointment times or inadequate transportation. 21 Offering access to medical interpreters, improving cultural competency, and providing convenient family-centered care have been suggested as ways to address these disparities. 1 In a systematic review of children with special health care needs, limited proficiency in English was independently associated with poorer patient outcomes and quality. 22 Similar findings were unable to be reproduced in the results shown here, which may reflect a commitment to these patient-centered approaches at this institution. Despite the many challenges of caring for this vulnerable population, the outcomes appear largely uninfluenced by language or ethnicity, suggesting that systematic biases and barriers have not marginalized the care of children with a tracheostomy. A commitment to improving the safety and quality of care for children with a tracheostomy likely contributes significantly to this observation. CHAMP was developed to address the many recognized poor outcomes among this vulnerable population of children. A multidisciplinary team of providers implemented several operational and clinical measures that have been recently described to improve outcomes for tracheostomy-dependent children. 23
Communication issues have been a focus in prior otolaryngology studies assessing non-English patients. For example, poor communication with non-English-speaking patients has resulted in increased emergency department visits after adenotonsillectomy.13,14 Lack of information retention, reluctance to contact providers, and difficulty accessing interpretation services are contributory factors. 14 The use of written discharge instructions in a native language has been preferred by Spanish-speaking families and can mitigate a potential source of caregiver dissatisfaction. 24 It appears that some health disparities can arise from miscommunication secondary to proficiency in a non–English language preference. As a center that offers outstanding access to interpretation and translation services, the results from this cohort may underestimate this effect.
Baseline characteristics of children requiring tracheostomy were largely similar between language groups. Spanish-speaking families were more likely to have tracheostomy-dependent children with cardiac conditions and high case complexity. Notably, families of Spanish-language preference had fewer maternal complications. It is unclear why this pattern of comorbidities was seen in our cohort, but it deserves further investigation. Perhaps the frequency of ambulatory and acute care encounters among children with complex cases, left unexplored in this study, implies a more robust network of providers and greater access to mitigate adverse outcomes. Additionally, favorable perinatal characteristics among Hispanic children have been referred to as the “Hispanic paradox.” 25 This phenomenon suggests that despite disparities with respect to education, insurance, prenatal care, and socioeconomic status, birth outcomes remain encouraging. Self-selection of the healthiest immigrants, protective cultural factors, and strong social supports in the community have been offered as explanations.25-27 A lower rate of prematurity and higher birthweight would explain more favorable outcomes in this Hispanic cohort. The extent to which these factors are related to ethnicity, at least among pediatric patients undergoing tracheostomy, remains an important area to explore. Future studies that investigate tracheostomy outcomes within the Hispanic community will help provide continued recognition of potential disparities.
Socioeconomic factors were unexplored in these results. Children from non–English language families are more likely to reside in low-income housholds. 1 Community disadvantage has been associated with differences in hospitalization length and costs after pediatric tracheostomy placement regardless of medical complexity. 12 The influence of socioeconomic forces in pediatric otolaryngology is gaining tremendous interest, 28 and a commitment to addressing these factors for pediatric tracheostomy patients is necessary. The current results suggest that among a cohort of children with a tracheostomy and high medical complexity, health disparities by language or ethnicity may have a modest influence on outcomes.
There are several limitations to this study. First, this represents a single-institution experience from a large urban children’s hospital. Centers performing pediatric tracheostomies in geographically and demographically unique regions may encounter dissimilar findings. Second, the frequency with which Children’s Medical Center Dallas cares for Hispanic and Spanish-speaking children in the North Texas community could mitigate certain health disparities. A robust system of translated materials, available interpreters, and Spanish-speaking providers improves the efficiency of care and could underestimate outcome disparities. Third, language preference is determined on caregiver-selected response and not reflective of language proficiency. Spanish language preference may reflect considerable variations in ability to read, speak, and understand English, which could overestimate the similarities between the groups of children.
Conclusion
Clinical outcomes after tracheostomy in this prospective cohort does not appear to be significantly affected by Spanish-language preference or Hispanic ethnicity. While these patient characteristics have been identified as a detriment to care in other areas, it has a more modest role in tracheostomy-dependent children. Further work from other institutions will be beneficial to compare outcomes for this vulnerable population based on language preference. The overall complexity of these patients likely introduces the biggest contribution to outcomes. Nonetheless, a continued dedication to quality improvement among tracheostomy-dependent children will be essential to identifying and addressing language-related barriers.
Footnotes
This article was presented at the AAO-HNSF Annual Meeting & OTO Experience; October 5, 2021; Los Angeles, California.
Authors’ Note
Romaine F. Johnson, associate editor of the journal, had no role in the editorial review or decision to publish this article.