
Abstract
Objective
To evaluate the efficacy of implementing a standardized multimodal perioperative pain management protocol in reducing opioid prescriptions following otolaryngologic surgery.
Study Design
Retrospective cohort study.
Setting
County hospital otolaryngology practice.
Methods
A perioperative pain management protocol was implemented in adults undergoing otolaryngologic surgery. This protocol included preoperative patient education and a postoperative multimodal pain regimen stratified by pain level: mild, intermediate, and high. Opioid prescriptions were compared between patient cohorts before and after protocol implementation. Patients in the pain protocol were surveyed regarding pain levels and opioid use.
Results
We analyzed 210 patients (105 preprotocol and 105 postprotocol). Mean ± SD morphine milligram equivalents (MMEs) prescribed decreased from 132.5 ± 117.8 to 53.6 ± 63.9 (P < .05) following protocol implementation. Mean MMEs prescribed significantly decreased (P < .05) for each procedure pain tier: mild (107.4 to 40.5), intermediate (112.8 to 48.1), and high (240.4 to 105.0). Mean MMEs prescribed significantly decreased (P < .05) for each procedure type: endocrine (105.6 to 44.4), facial plastics (225.0 to 50.0), general (160.9 to 105.7), head and neck oncology (138.6 to 77.1), laryngology (53.8 to 12.5), otology (77.5 to 42.9), rhinology (142.2 to 44.4), and trauma (288.0 to 24.5). Protocol patients reported a mean 1-week postoperative pain score of 3.4, used opioids for a mean 3.1 days, and used only 39% of their prescribed opioids.
Conclusion
Preoperative counseling and standardization of a multimodal perioperative pain regimen for otolaryngology procedures can effectively lower amount of opioid prescriptions while maintaining low levels of postoperative pain.
The United States is amidst an opioid use crisis, responsible for >115 deaths daily. 1 The opioid epidemic imposes a significant cost on society, responsible for an estimated $8.4 billion in health care expenditures per year. 2 As prescribers of opioids, surgeons play a significant role in the widespread use of opioids, responsible for the second-highest amount of opioid prescriptions (37% of prescriptions), behind only pain specialists (49%). 3 In otolaryngologic surgery, 1 of every 17 patients prescribed opioids postoperatively will become a long-term opioid user. 4 Within otolaryngology there is currently a lack of standardization of practice for perioperative pain management, and this large variability contributes to significant overprescribing of opioid medications.5,6
Recently published clinical practice guidelines from the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) have provided clear actionable statements in an effort to curtail opioid prescriptions in otolaryngology. 7 Among these recommended strategies are preoperative patient counseling, multimodal treatment plans, and the tailoring of postoperative prescriptions based on procedure-specific level of anticipated pain. 7 A recent state-of-the-art review of opioid use in otolaryngology similarly delineated a perioperative pain management protocol, stratifying surgical procedures by pain level. 8 Our institution recently adopted a perioperative pain management protocol based on these recommendations. In this study, we assess the efficacy of implementing a standardized evidence-based perioperative pain management protocol across a comprehensive otolaryngology practice.
Methods
Study Design and Inclusion/Exclusion Criteria
We performed a retrospective cohort study comparing patients undergoing otolaryngologic surgery prior to and following implementation of a standardized perioperative pain management protocol (pre- vs postprotocol). The pain protocol was implemented in calendar year 2019 as part of an institutional quality improvement project. The postprotocol cohort underwent surgery between January 1, 2019, and December 31, 2019. For comparison, we used a historic preprotocol cohort that underwent surgery between January 1, 2018, and December 31, 2018. Patients in the preprotocol cohort were selected from a listing of 2018 surgical cases, matched by age and sex to a postprotocol patient.
All patients underwent surgery at a single county hospital, performed by 1 of 5 authors (L.L., K.S., A.M., M.S., M.A.). Patients were included if they were >18 years in age and undergoing an otolaryngology procedure. Inpatient and outpatient procedures were included in this study. Patients did not participate in the pain protocol if they had a history of chronic pain, long-term opioid use, or allergy to any medication in the protocol. Patients with preexisting liver disease were not prescribed acetaminophen and thus did not participate in the protocol. Patients with a history of seizures were not prescribed tramadol and were thus excluded from the protocol. Patients were excluded if they did not complete the postoperative questionnaire.
Perioperative Pain Protocol
At the preoperative visit, patients underwent counseling regarding expectations for postoperative pain, anticipated regimen of pain meds, potential adverse effects of analgesic medications, and proper storage and disposal options for unused opioids. A document summarizing these preoperative counseling points was reviewed in-person and provided to patients to take home (Supplemental Document 1, available online). Patient counseling was performed by 1 of the 5 authors (L.L., K.S., A.M., M.S., M.A.) as part of the standard preoperative visit.
The perioperative pain protocol ( Table 1 ) stratified surgical procedures by pain level: mild, intermediate, and high. According to the pain tier of the procedure, patients received a standardized pre- and postoperative regimen of analgesic medications. On the day of surgery in the preoperative area, all patients received a preoperative dose of 1000 mg of acetaminophen and 600 mg of gabapentin. Both medications were administered orally with a sip of water 20 to 30 minutes prior to induction of general anesthesia. Given the wide variation of procedure types in this study, the utilization of local anesthesia was left to the discretion of the surgeon. Similarly, intraoperative anesthesia regimen was left to the discretion of the anesthesiologist.
Perioperative Pain Management Protocol by Procedure Level of Pain.
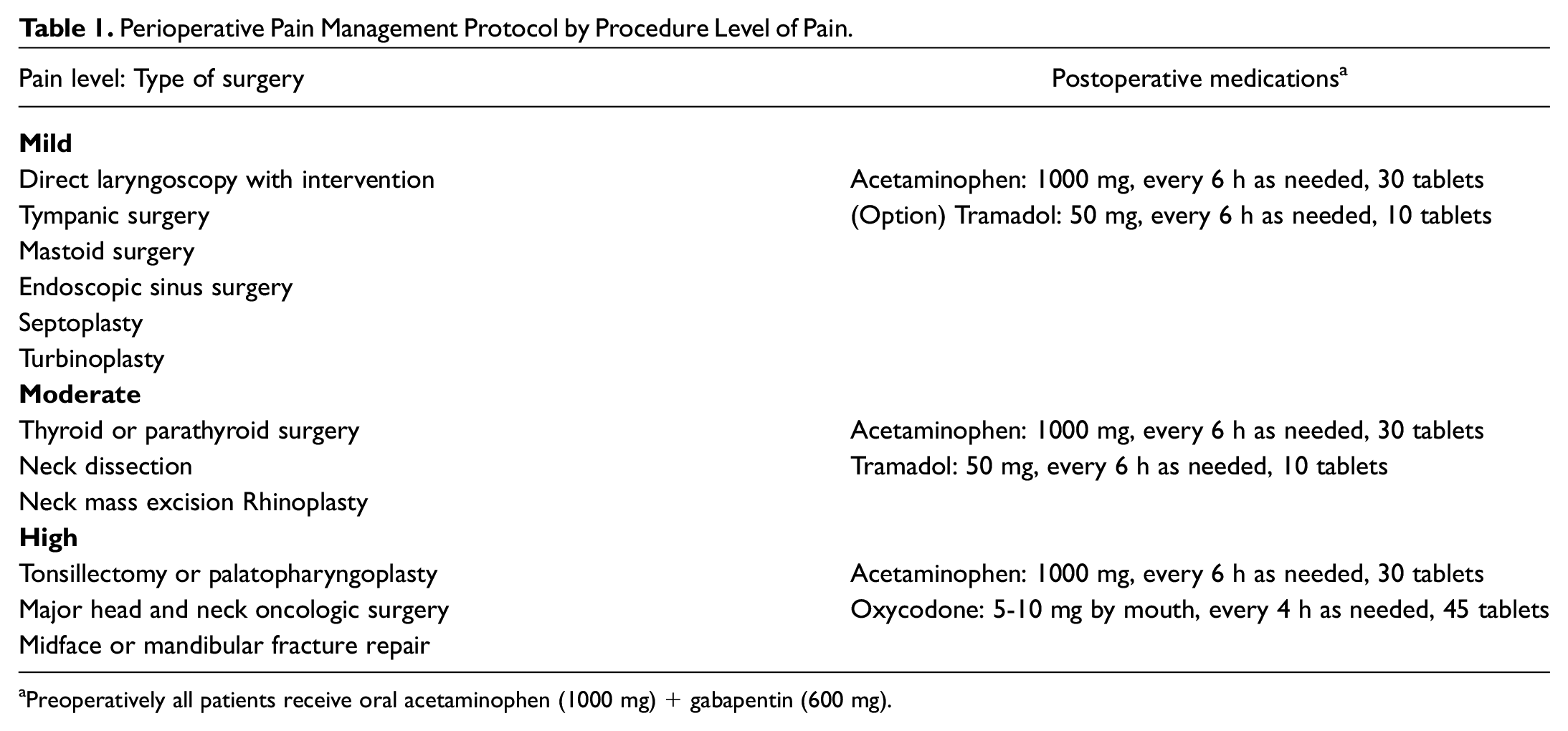
Preoperatively all patients receive oral acetaminophen (1000 mg) + gabapentin (600 mg).
The postoperative regimens prescribed were as follows:
Mild pain procedures: direct laryngoscopy, otologic surgery, endoscopic sinus surgery, septoplasty; 30 tablets of 650-mg acetaminophen with an optional prescription at the provider’s discretion of 10 tablets of 50-mg tramadol
Intermediate pain procedures: thyroidectomy, parathyroidectomy, neck dissections, open septorhinoplasty; 30 tablets of 650-mg acetaminophen and 10 tablets of 50-mg tramadol
Severe pain procedures: tonsillectomy, palatopharyngoplasty, major oncologic surgery, facial fracture repair; 30 tablets of 650-mg acetaminophen and 45 tablets of 5-mg oxycodone
All analgesic medications were recommended to be taken on an as-needed basis. Although patients requiring an inpatient stay postoperatively were prescribed the same regimen while in the hospital, medications taken as an inpatient were not counted toward overall opioid consumption. Upon discharge, inpatients were prescribed the same amounts, doses, and regimen of analgesics listed in Table 1 . All patients in this protocol were instructed to avoid use of NSAIDs (nonsteroidal anti-inflammatory drugs) after surgery. All patients were provided standardized written instructions regarding dosing and timing for each prescribed medication at the time of discharge (Supplemental Document 2, available online).
Postoperative surveys were completed by patients at the clinic visit 1 week following surgery (Supplemental Document 3, available online). This survey was collected as part of an institutional quality improvement project rather than for research purposes. Versions of the survey were available in English, Spanish, and Vietnamese. The mean pain level over the first week was assessed by the Wong-Baker FACES Pain Rating Scale, a pictonumeric scale by which patients rate their pain levels from 0 to 10. 9 This survey also asked patients to self-report severity of medication-related adverse effects (none, mild, moderate, or severe), duration of analgesic medication use, amount of opioids taken as a percentage and an absolute number, and whether any analgesic medication refill was requested.
Data Collection and Analysis
Data collected for all patients consisted of the following: demographics, comorbidities, type of surgery, length of hospitalization, and any relevant medical complications. Patients in the postprotocol cohort were also surveyed regarding adverse effects, analgesic use duration, amount of opioid medication use, and need for additional prescriptions of pain medication. The electronic medical record was reviewed for any opioid medication refills within the first 30 days after surgery. Additionally, the CURES database was queried for each study patient to capture any additional refills of opioid medications within the 30-day postoperative period at other health care sites.
All opioid quantities were converted to morphine milligram equivalents (MMEs) for analysis. All statistical analysis was performed in SPSS (IBM). Opioid prescription amounts were compared between the pre- and postprotocol cohorts, and additional analyses were performed comparing cohorts by each pain tier and procedure subtype. The Student t test was used to compare cohorts, with a P value <.05 indicating a significant difference.
Institutional Review Board
This study protocol was approved by the Santa Clara Valley Medical Center’s Institutional Review Board (19-006).
Results
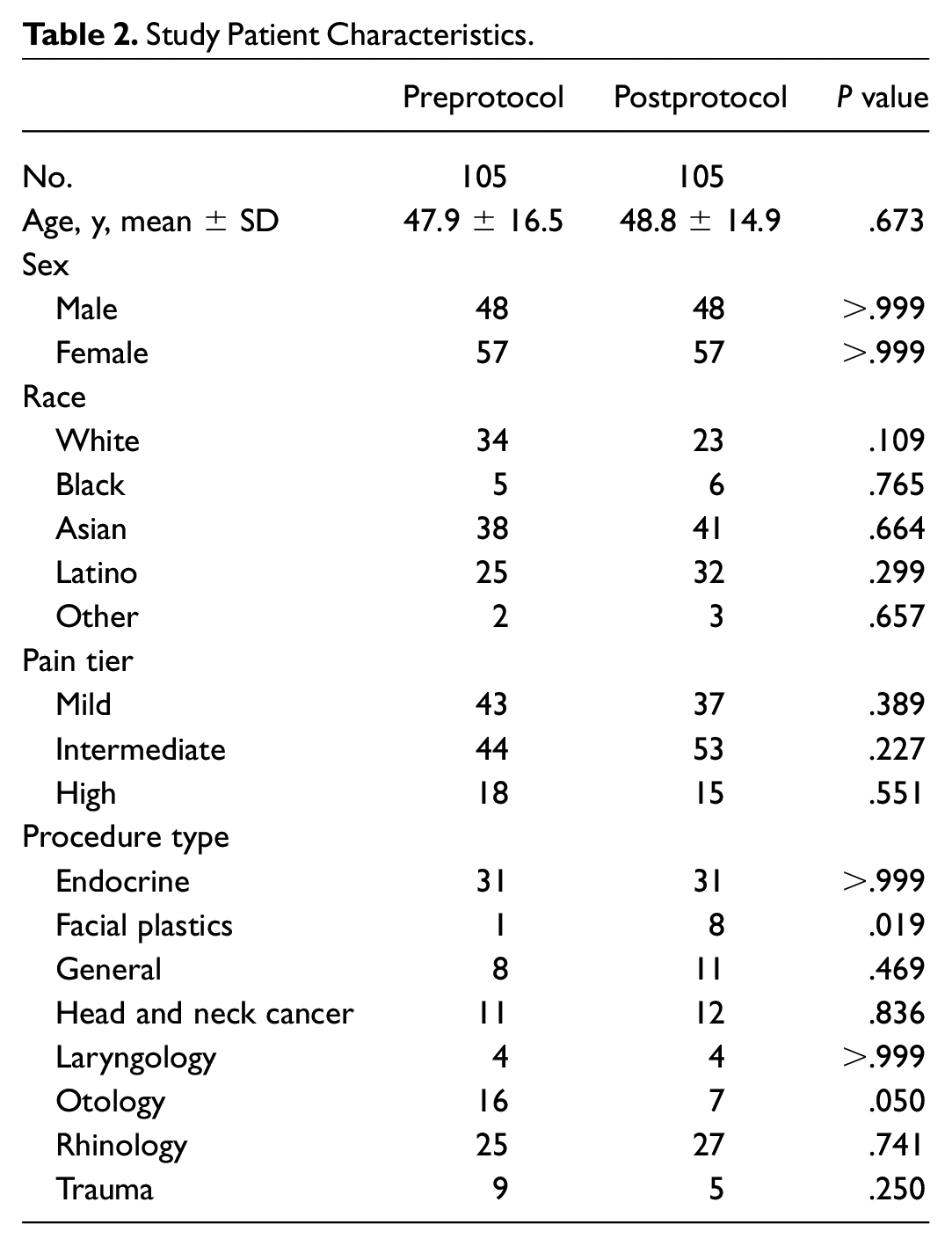
An overall 216 patients were included in this study. Six postprotocol patients had incomplete postoperative surveys and were thus excluded from the study. Analysis was ultimately performed for 105 patients in the preprotocol cohort and 105 in the postprotocol cohort. Demographic characteristics between the cohorts were not significantly different. Demographics and distribution of surgery by pain level and procedure type are described in Table 2 .
Study Patient Characteristics.
Mean ± SD MMEs prescribed decreased from 132.5 ± 117.8 to 53.6 ± 63.9 (P < .05) following protocol implementation. Mean MMEs prescribed significantly decreased (P < .05) for each procedure pain tier: mild (107.4 to 40.5), intermediate (112.8 to 48.1), and high (240.4 to 105.0; Figure 1 ).
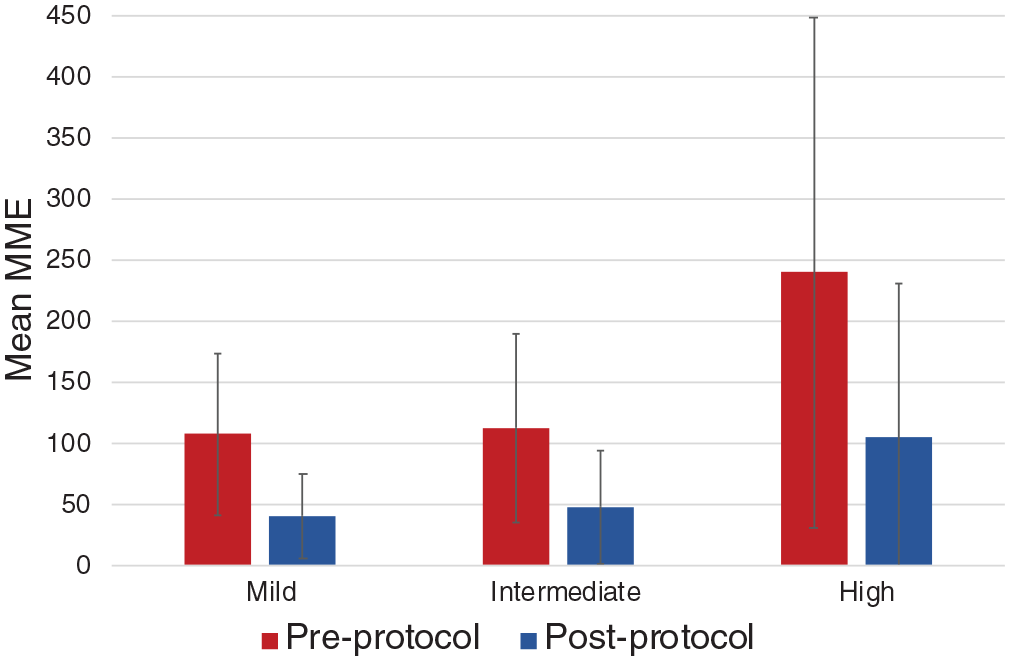
Comparison of prescribed opioid amounts before and after protocol implementation, sorted by procedure pain tier. Error bars represent standard deviation. MME, morphine milligram equivalent .
Mean MMEs prescribed significantly decreased (P < .05) for each procedure type: endocrine (105.6 to 44.4), facial plastics (225.0 to 50.0), general (160.9 to 105.7), head and neck oncology (138.6 to 77.1), laryngology (53.8 to 12.5), otology (77.5 to 42.9), rhinology (14.2.2 to 44.4), and trauma (288.0 to 24.5; Figure 2 ).
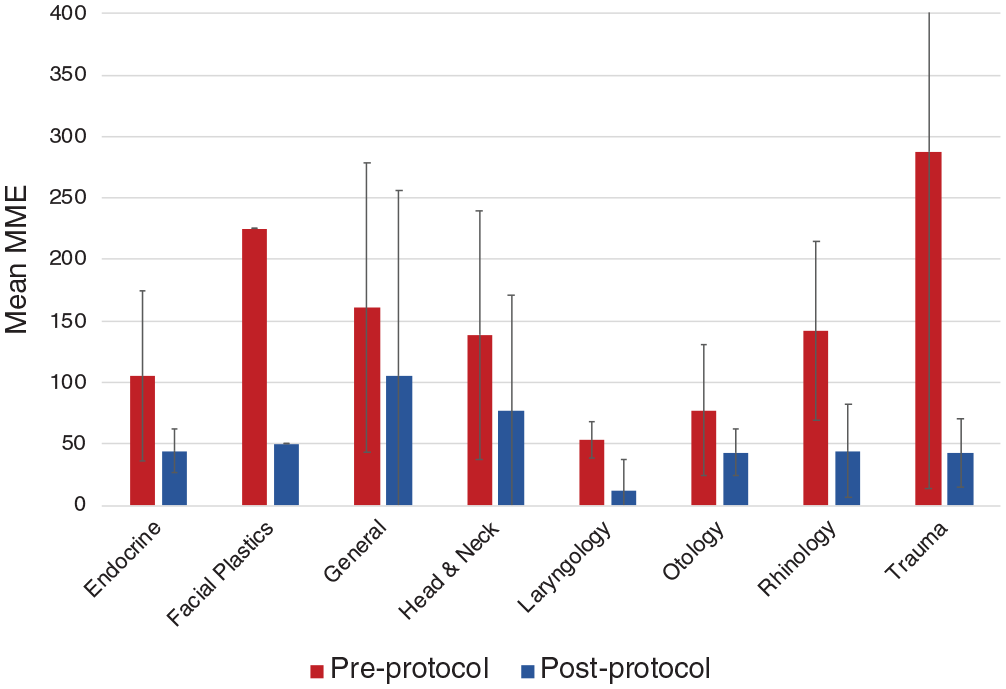
Comparison of prescribed opioid amounts before and after protocol implementation, sorted by procedure type. Error bars represent standard deviation. MME, morphine milligram equivalent.
For patients undergoing the pain protocol, the mean 1-week postoperative pain score was 3.4. Pain scores reported by postprotocol patients are shown in Figure 3 . By pain tier, mean 1-week pain scores were 3.7 ± 2.8 for the mild pain tier, 3.0 ± 2.7 for the intermediate, and 3.9 ± 3.2 for the high. By procedure type, mean 1-week pain scores were as follows: 3.4 ± 2.9 for endocrine, 3.6 ± 2.5 for facial plastics, 3.8 ± 3.7 for general, 4.4 ± 2.6 for head and neck cancer, 4.7 ± 1.8 for laryngology, 3.4 ± 3.6 for otology, 4.4 ± 3.2 for rhinology, and 3.5 ± 3.8 for trauma cases.
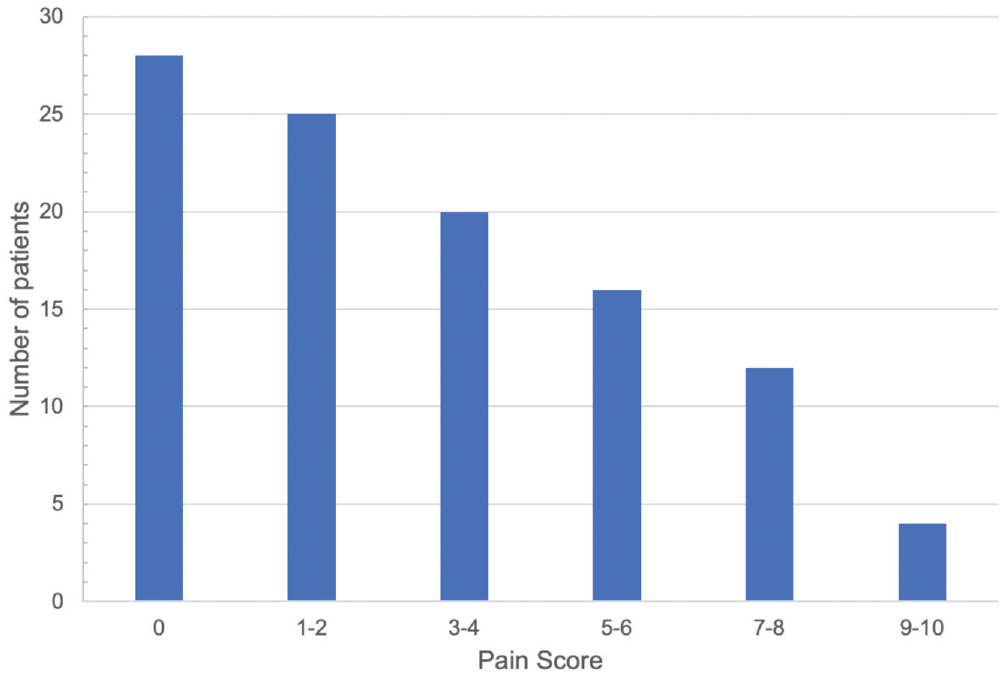
Pain scores reported by patients after protocol implementation.
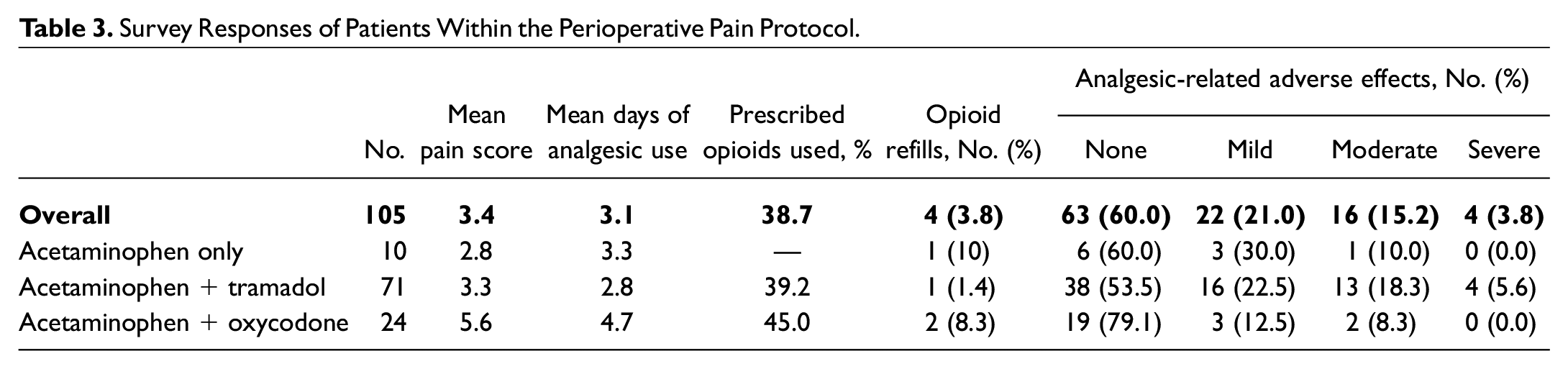
Survey responses of patients within the perioperative pain protocol are listed in Table 3 . Among 105 postprotocol patients, 24 (22.9%) were prescribed acetaminophen only, 71 (67.7%) acetaminophen and tramadol, and 10 (9.5%) acetaminophen and oxycodone. Overall patients used analgesic pain medications for a mean 3.1 days postoperatively. Postprotocol patients reported using 38.7% of their prescribed opioids. Medication-related adverse effects were reported as none in 63 (60.0%), mild in 22 (21.0%), moderate in 16 (15.2%), and severe in 4 (3.8%). Patients prescribed acetaminophen and tramadol had higher rates of mild, moderate, and severe adverse effects as compared with patients prescribed acetaminophen and oxycodone. There was no significant difference in number of opioid refill requests between pre- and postprotocol patients (3 vs 4, P = .20).
Survey Responses of Patients Within the Perioperative Pain Protocol.
Discussion
Surgeons play a significant role in the exacerbation of the current opioid epidemic, as diversion of leftover opioids is a major contributor to opioids circulating in the community.10-12 One study of ambulatory otolaryngology surgery in a 23-hospital health care system found that >75% of patients were in possession of excess opioids after the acute postoperative period. 13 In this study, we demonstrate that a standardized, multimodal, and tiered approach to perioperative pain management can effectively reduce the amount of opioid prescriptions in the postoperative setting. This protocol is in accordance with recent AAO-HNS practice guidelines, 7 which emphasized appropriate stratification of pain levels by procedure type to determine perioperative prescribing practices. A 10-point rating scale is used in which patients consider 1 to 4 low or mild pain, 5 or 6 moderate, and 7 to 10 severe.14,15 Within this protocol, patients undergoing procedures across all anticipated pain tiers are still able to achieve relatively mild levels of pain (<4.0). Establishing and validating strategies such as those in this study provides an important step toward curtailing the amount of community opioids attributable to surgeon prescription while still providing adequate analgesia to postsurgical patients.
The pain management protocol in this study synthesizes findings across many other studies within otolaryngology, demonstrating that successful opioid reduction requires intervention across several phases of the perioperative timeline. Additionally, while numerous subspecialty-specific studies have had similar success in multimodal analgesia approaches, such as endoscopic sinus surgery, 16 facial plastic surgery, 17 thyroid surgery,18,19 and head and neck cancer and reconstructive surgery, 20 our institutional experience demonstrates that similar success can be seen when implementing a multimodal pain protocol across an entire otolaryngology department or general otolaryngology practice.
This study highlights the importance of preoperative counseling regarding opioid side effects and addictive potential, a strategy also recommended by recent AAO-HNS clinical guidelines. 7 A study of adults coping with opioid addiction demonstrated a significant association between clinician counseling and reduced craving and opioid use in the subsequent week. 21 In rhinoplasty surgery, a small study assessing the effect of preoperative counseling and standardization of opioid prescribing found that this protocol reduced postoperative opioid consumption. 17 Similarly, in a prospective study of endocrine surgery, patient education within a standardized postoperative pain protocol resulted in a very low rate of postoperative opioid use (6.1%) while maintaining a 94.6% satisfaction rate. 21
On the day of surgery, multimodal analgesia approaches with standardized opioid protocols can be successful in limiting opioid prescriptions.6,16-20,22,23 Preoperative administration of multimodal analgesia can be effective at limiting acute postoperative pain. A study of patients undergoing head and neck cancer resection with free flap reconstruction demonstrated that preoperative celecoxib, tramadol, and gabapentin resulted in significantly fewer opioids in the postanesthesia care unit. 20 The AAO-HNS guidelines now recommend nonopioid multimodal alternatives as first-line therapy following otolaryngologic surgery.7,24 A systematic review found that gabapentin was effective in reducing opioid consumption and postoperative pain following tonsillectomy, thyroidectomy, and nasal surgery. 25 There are also increasing data that NSAIDs, which were not investigated in this study, prescribed postoperatively as part of a multimodal regimen can be effective at managing pain and decreasing opioid consumption in otolaryngologic surgery without increasing bleeding risk.20,24,26
The pain protocol in this study utilized tramadol as an alternative to traditional opioids. Tramadol is a unique opioid that is thought to act through 2 mechanisms: (1) agonist effect on μ-opioid and k-opioid receptors and (2) inhibition of norepinephrine and serotonin reuptake, which is thought to potentiate antinociceptive effects. 27 Tramadol is a less potent opioid with one-tenth of the MME value, 28 which has made it a popular alternative option in pain management, as its lower potency may be associated with a lower side effect profile and abuse potential as compared with traditional opioids. 29 However, broad prescribing of tramadol should be undertaken with caution as it poses unique risks, such as seizures and serotonin syndrome. 30 As such, caution should certainly be taken in patients with a history of seizures or those taking other serotonergic medications such as selective serotonin reuptake inhibitors and tricyclic antidepressants. Tramadol may in fact have a higher adverse effect profile than expected, as our study shows that patients prescribed tramadol with acetaminophen had higher rates of adverse effects than patients prescribed oxycodone with acetaminophen. Given how patients in this study were surveyed, these data are limited by patients’ subjective ratings of adverse effects, and additional information regarding specific adverse effects experienced was not able to be determined. Furthermore, there are conflicting reports regarding the abuse potential of tramadol. 30 Prescribing tramadol for an acute pain episode may be associated with increased risk of persistent opioid use versus other short-acting opioids. 31 While our study demonstrates that integration of tramadol in a perioperative pain management strategy can significantly lower the amount of opioids prescribed, further study is warranted to assess the safety and efficacy of tramadol against traditional opioids and nonopioid analgesics in the acute postoperative and long-term settings.
The results of this study suggest that there is much work to be done to optimize opioid prescriptions, as patients reported utilizing only 39% of prescribed opioids even with a standardized protocol in place. As awareness of the opioid epidemic continues to increase among providers and patients and as analgesic alternatives are developed and validated, the necessity of opioid prescriptions in otolaryngology may continue to diminish. A recent randomized multicenter study of endoscopic sinus surgery demonstrated that the mean consumption of opioid tablets was <2 and that the majority of patients were able to control pain adequately with a regimen of acetaminophen and ibuprofen. 26 In rhinoplasty surgery, an average of 6 or 7 opioid pills are consumed postoperatively when prescribed with acetaminophen and ibuprofen. 17 Further study is certainly needed to determine the appropriate level of opioids to prescribe that reduces excess but is still able to sufficiently control postoperative pain.
This study has several limitations. This study was retrospective, introducing potential recall bias as the data relied on self-reported patient information. It was not blinded to the clinicians, potentially introducing bias in management and assessment of pain for these patients. The generalizability of this study is limited as patients with a history of chronic pain and opioid use did not participate, excluding a population that may be at higher risk for inadequate pain control and potential opioid abuse. The use of local anesthesia was not standardized, which may have affected postoperative pain levels and medication use in a manner that this study was not able to measure. Intraoperative anesthesia was not standardized and instead left to the discretion of the anesthesiologist, potentially introducing significant variability into the patient experience as it related to postoperative pain. Secondary outcome data for preprotocol patients were limited, as they were not assessed for their pain levels, medication-related side effects, duration of analgesic use, and amount of opioids consumed; thus, the effect of the protocol implementation on these metrics cannot be evaluated. The use of a historic cohort as a control group also introduces potential effects of temporal changes in practice unrelated to the implementation of this protocol. Further studies are certainly warranted to determine the best analgesia-prescribing practices, tailored to procedural and patient characteristics. Nonetheless, this study demonstrates that implementation of a perioperative pain protocol can significantly reduce amount of postoperative opioid prescriptions.
Conclusion
Implementation of a standardized perioperative pain management protocol can effectively reduce the amount of opioid prescriptions while maintaining low levels of postoperative pain. Further studies are needed to refine and optimize postoperative analgesic prescribing practices.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211071116 – Supplemental material for Implementation of a Standardized Perioperative Pain Management Protocol to Reduce Opioid Prescriptions in Otolaryngologic Surgery
Supplemental material, sj-docx-1-oto-10.1177_01945998211071116 for Implementation of a Standardized Perioperative Pain Management Protocol to Reduce Opioid Prescriptions in Otolaryngologic Surgery by Michael T. Chang, M. Lauren Lalakea, Kimberly Shepard, Micah Saste, Amanda Munoz and Misha Amoils in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-3-oto-10.1177_01945998211071116 – Supplemental material for Implementation of a Standardized Perioperative Pain Management Protocol to Reduce Opioid Prescriptions in Otolaryngologic Surgery
Supplemental material, sj-docx-3-oto-10.1177_01945998211071116 for Implementation of a Standardized Perioperative Pain Management Protocol to Reduce Opioid Prescriptions in Otolaryngologic Surgery by Michael T. Chang, M. Lauren Lalakea, Kimberly Shepard, Micah Saste, Amanda Munoz and Misha Amoils in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-pdf-2-oto-10.1177_01945998211071116 – Supplemental material for Implementation of a Standardized Perioperative Pain Management Protocol to Reduce Opioid Prescriptions in Otolaryngologic Surgery
Supplemental material, sj-pdf-2-oto-10.1177_01945998211071116 for Implementation of a Standardized Perioperative Pain Management Protocol to Reduce Opioid Prescriptions in Otolaryngologic Surgery by Michael T. Chang, M. Lauren Lalakea, Kimberly Shepard, Micah Saste, Amanda Munoz and Misha Amoils in Otolaryngology–Head and Neck Surgery
Footnotes
This article was presented at the AAO-HNSF Annual Meeting & OTO Experience; October 4, 2021; Los Angeles, California.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.