
Abstract

We have read the article entitled “Periprosthetic Leakage in Tracheoesophageal Prosthesis: Proposal of a Standardized Therapeutic Algorithm.” 1 We acknowledge the authors for the systematic management of the patient with laryngectomy and voice prosthesis (VP). To date, there was no similar article through this approach, highlighting the importance of a systematic approach in the management of late complications and advocating for a multidisciplinary unit formed by otolaryngologists and speech therapists. 2
There is controversy regarding the factors that could influence the duration of the VP and the causes of periprosthetic leakage, 3 some of which are discussed in this article. 1 Apart from individual predisposition, various factors have been discussed in the literature. 3 A direct correlation between the incidence of severe fistula enlargement and reflux disease, confirmed by impedance-pH monitoring, has been demonstrated in several studies.3,4 These patients have a 2.3-fold higher risk of tracheoesophageal fistula enlargement, and the risk of fistula enlargement is correlated with the reflux severity. Improvement of fistulas and VP duration has been shown in patients with antireflux treatment.2,3 For this reason, prophylactic treatment with proton pump inhibitors associated with alginate may be justified in all patients with periprosthetic leakage or substantial fistula enlargement.2-4 With these findings, we wish to point out some aspects that we consider of capital importance in the comprehensive management of patients with periprosthetic leakage.
First, the study of Parrilla et al 1 lacks a detailed explanation in its methodology about the evaluation of possible reflux or the presence of antireflux therapeutic measures, being able to represent a source of biases. Given previous evidence, our working group proposes a small modification to the algorithm, including the evaluation of a reflux or antireflux treatment regimen. Second, given evidence regarding their effectiveness and cost reduction,2,5 our working group advocates for the routine use of specific VPs with a double esophageal flange or with large esophageal and tracheal flanges in case of periprosthetic leaks ( Figure 1 ).
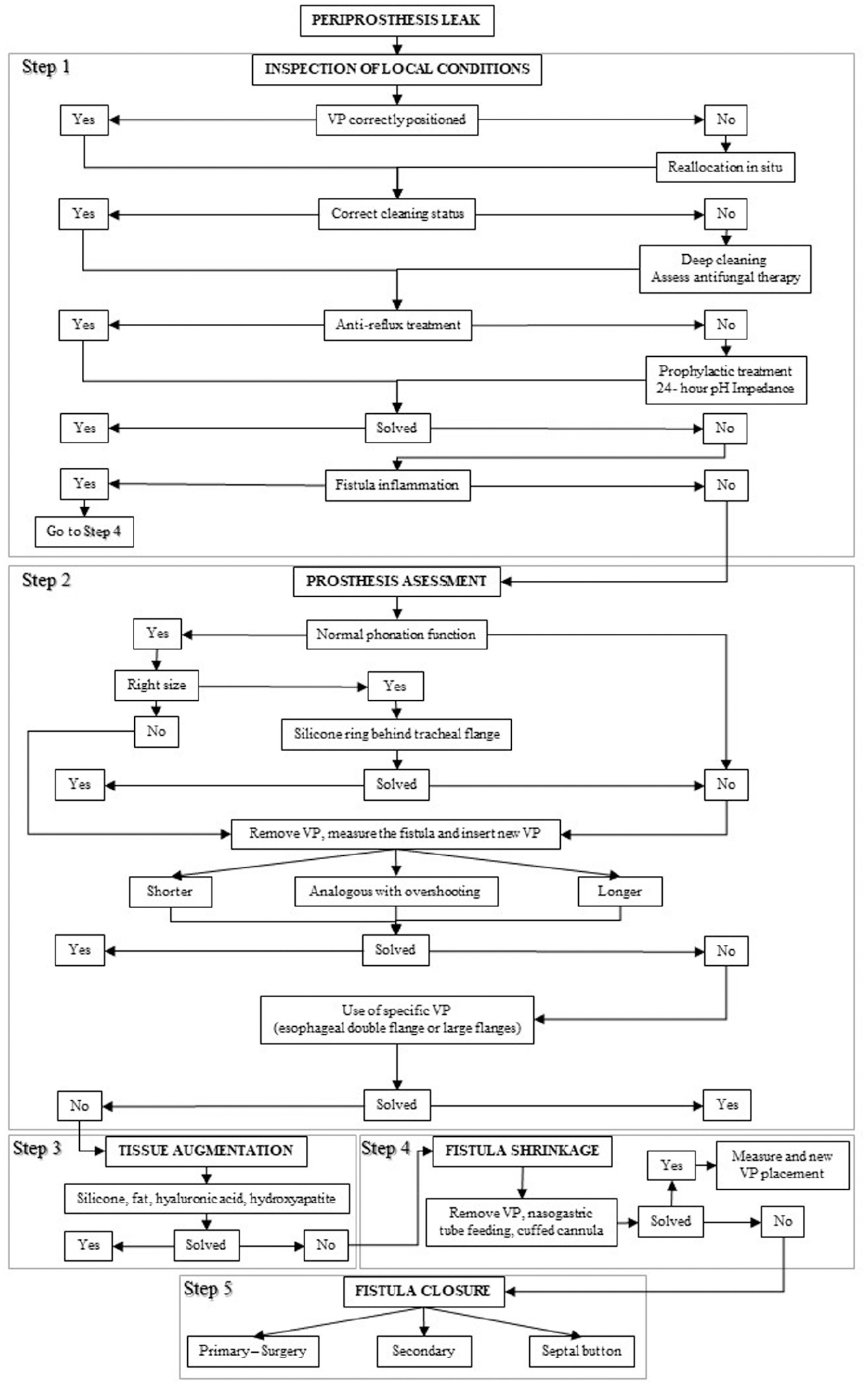
Modification of the protocol for the management of periprosthetic leaks proposed by Parrilla et al. 1 VP, voice prosthesis.
The management of the patient with laryngectomy and VP use is complex and requires a multidisciplinary and systematic approach by professionals with experience in the field to reduce replacements and complications. The evolution of these patients is heterogeneous and highly changeable over time. The new algorithm proposed implements aspects such as the treatment of reflux or the routine use specific VPs.
