
Abstract
Objective
This study summarizes the anatomical features of the superior laryngeal nerve in Chinese to enable the rapid location of the superior laryngeal nerve during an operation.
Study Design
Retrospective analysis of anatomical data.
Setting
Hangzhou First People’s Hospital Affiliated to Nanjing Medical University.
Methods
A total of 71 embalmed human cadavers (132 heminecks) were examined over 3 months. The length and diameter of the internal and external branches of the superior laryngeal nerve and their relationships with different landmarks were recorded.
Results
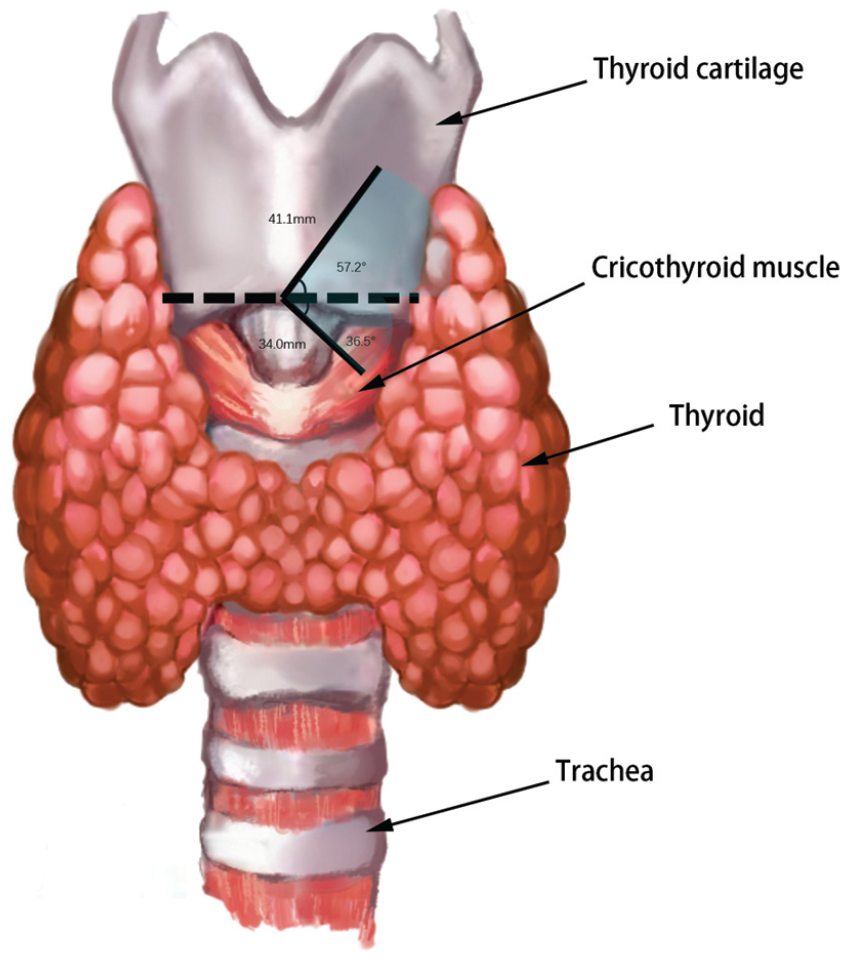
The total length of the internal branch of the superior laryngeal nerve was 23.4 ± 6.9 mm. The length of the external branch of the superior laryngeal nerve was 47.7 ± 11.0 mm. Considering the midpoint of the lower edge of the thyroid cartilage as the starting point and using that edge as a horizontal line, when the entry point is above that line, the external branch of the superior laryngeal nerve can be found within 41.1 mm and at an angle of 57.2°. When the entry point is below the lower edge of the thyroid cartilage, the external branch of the superior laryngeal nerve can be found within 34.0 mm and at an angle of 36.5°.
Conclusion
The superior laryngeal nerve in Chinese people has distinct anatomical characteristics. This article provides a new method of quickly locating the external branch of the superior laryngeal nerve during the operation, which can reduce the probability of damaging the external branch of the superior laryngeal nerve.
In recent years, the incidence of thyroid cancer has been increasing both in China and worldwide. 1 As it is the first choice for the treatment of thyroid cancer, the incidence of thyroid cancer surgery has increased dramatically. Many surgeons think that thyroid surgery is very simple, but many complex problems can occur during the operation that can reduce the patient’s quality of life. For example, injury to the recurrent laryngeal nerve (RLN) leads to vocal cord paralysis and asphyxia. Parathyroid gland injury causes limb convulsion, requiring lifelong calcium supplementation. 2 With the widespread use of intraoperative nerve monitoring (IONM) and nanocarbon, the incidence of damage to the RLN and parathyroid gland during thyroid surgery has been substantially reduced.3-5 However, many surgeons still refer to the superior laryngeal nerve (SLN) as “the neglected nerve,” owing to the fact that the rate of damage to the SLN remains as high as 58%. 6 Many reports have confirmed that IONM can be used to help protect the external branch of the superior laryngeal nerve (EBSLN).7-9 However, this technique is not always applicable. Even if it can be applied, it is better to locate the nerve directly. Many studies have explained the physiological anatomy of the SLN and its relationship with important structures.7,10-12 These studies have tried to provide markers that can be used to locate the SLN quickly and reliably during an operation by summarizing the characteristics of the SLN. However, there are still many reports showing that it is very difficult to accurately locate and adequately protect nerves. The difficulties mentioned in the reports include accidental injuries during surgery,13,14 the inability to find the nerves, and the need to use electrical stimulation to identify the nerves.8,12,14 Although some reports have stated that an injury to the SLN injury has a minimal effect on the voice, 15 most scholars have described the relationships between the SLN and the surrounding structures ( Figure 1 ), which play important roles in the protection of the SLN. These studies have reported various relationships among the SLN and the superior thyroid artery (STA),15,16 the sternothyroid muscle,16,17 the carotid arteries,15,16,18,19 and the inferior pharyngeal constrictor muscle (IPC). 15 There are still many contradictory views and unsolved problems in these reports. All the above reports lack relevant information about the Chinese population. This study was performed to summarize the anatomical characteristics of the SLN in the Chinese population to provide a basis for the rapid identification of the location of the EBSLN during an operation.
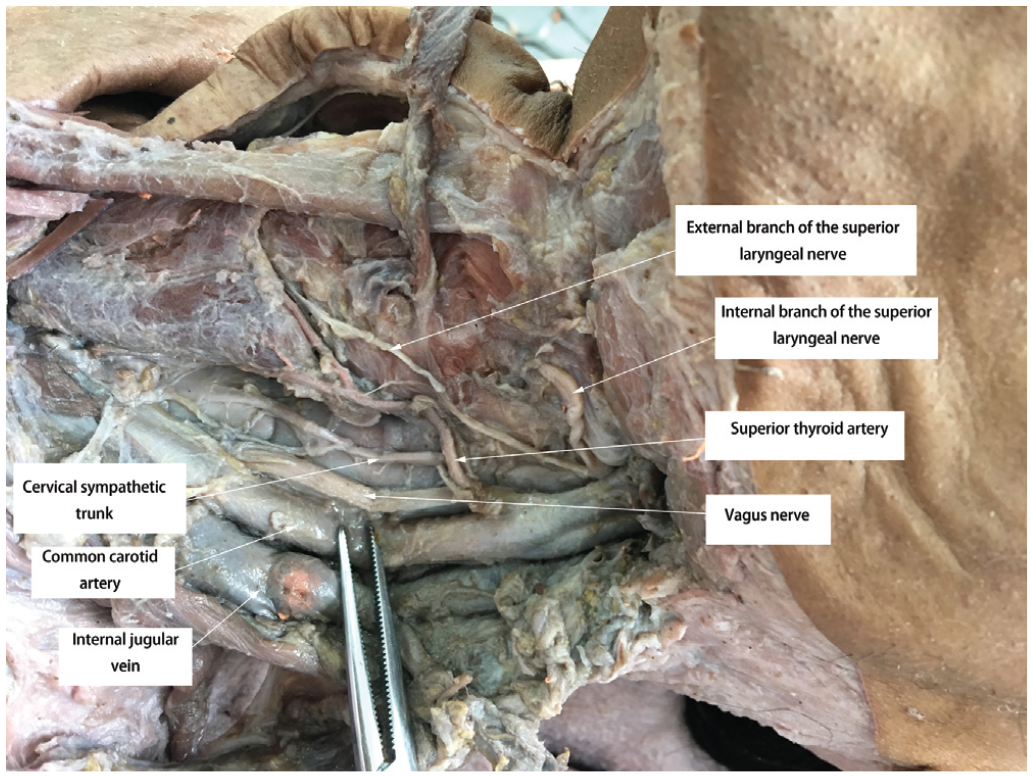
The superior laryngeal nerve and the surrounding structures.
Materials and Methods
General Information
This study was approved by the institutional review board of the Hangzhou First People’s Hospital Affiliated to Nanjing Medical University. A total of 71 embalmed human cadavers (132 heminecks) from Zhejiang University School of Medicine and Wenzhou Medical University, Wenzhou, Zhejiang, China, were examined over 3 months. Among the cadavers, 67 left SLNs (50.8%) and 65 right SLNs (49.2%) were observed. There were 101 males (76.5%) and 31 females (23.5%). The necks included in the study were intact and undamaged.
Statistical Methods
We used SPSS 22.0 (SPSS, Inc) to analyze the different parameters. Continuous variables are expressed as the means ± SDs, and categorical variables are expressed as numbers and percentages. We used nonparametric tests or t tests to analyze the data. In our study, P < .05 was considered statistically significant.
Result
Neck Length and Length of the Thyroid
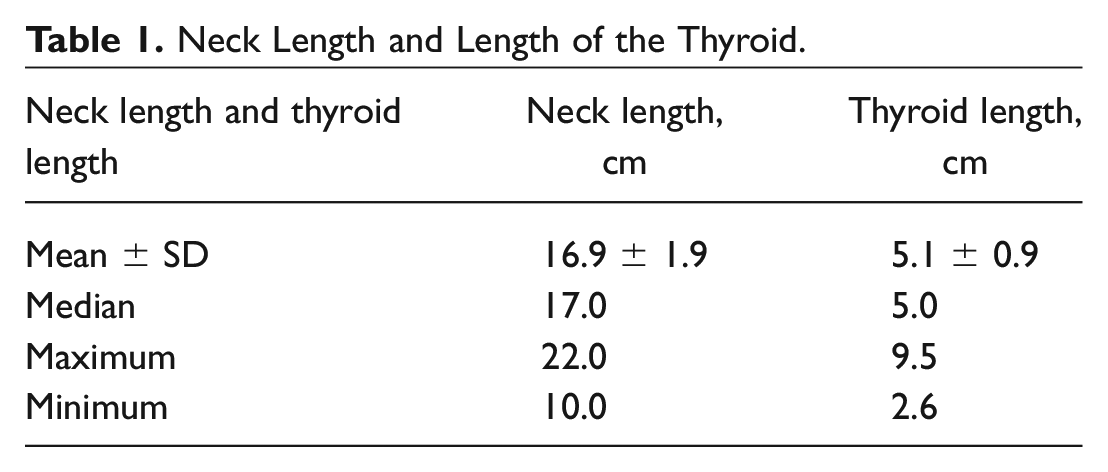
We measured the length of the neck and the length of the thyroid on 132 heminecks. The length of the neck was measured from the mastoid part of the temporal bone to the sternoclavicular joint, and the length of the thyroid was measured as the longest distance from the upper pole to the lower pole. The average neck length was 16.9 ± 1.9 cm. The neck was longer in men than in women (P < .000). There was no difference with regard to side (P = .234). The average thyroid length was 5.1 ± 0.9 cm. There was no difference based on sex (P = .275) or side (P = .102) ( Table 1 ).
Neck Length and Length of the Thyroid.
Internal Branch of the Superior Laryngeal Nerve
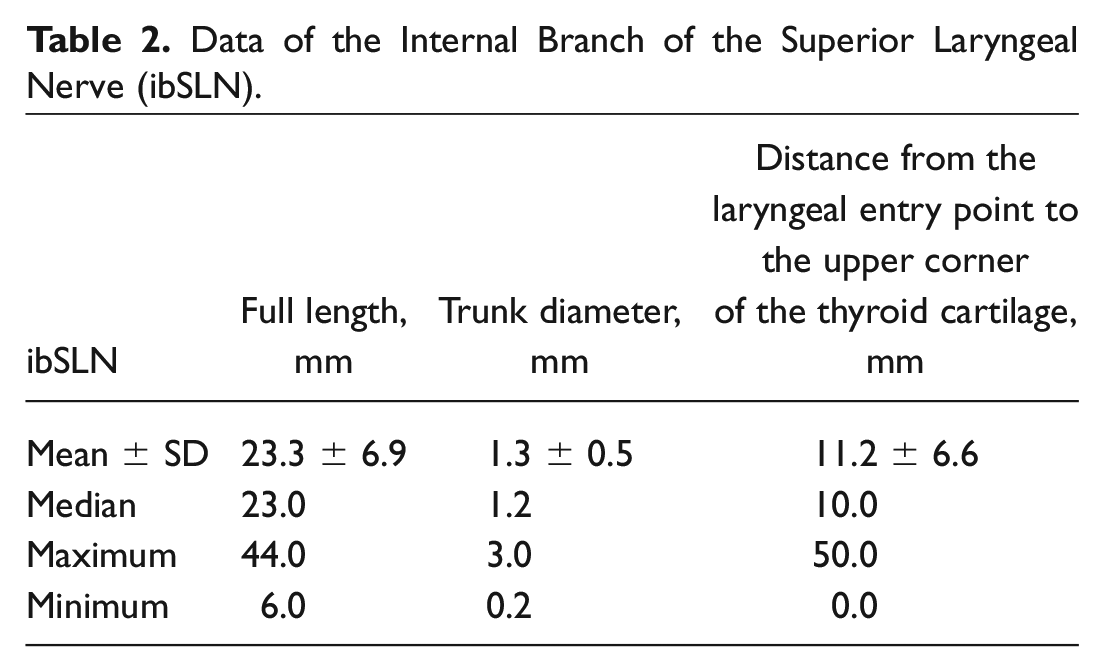
In this study, we finely dissected the anterolateral region of the neck and measured the total length of the internal branch of the superior laryngeal nerve (ibSLN). The mean length (1 case had missing data) was 23.4 ± 6.9 mm. The length of the ibSLN was longer in men than in women (P = .018). There was no difference with regard to side (P = .365). The diameter of the trunk was 1.3 ± 0.5 mm. There was no difference based on sex (P = .245) or side (P = .554). The mean value of the distance from the entry point into the larynx to the upper corner of the thyroid cartilage was 11.2 ± 6.6 mm ( Table 2 ). There were 39 cases (29.6%) of no bifurcation in the ibSLN, 80 cases (60.6%) of 1 bifurcation, 7 cases (5.3%) of 2 bifurcations, 4 cases (3.0%) of 3 bifurcations, and 2 cases (1.5%) of 4 bifurcations ( Figure 2 ). The ibSLN entry points were all in the thyrohyoid membrane.
Data of the Internal Branch of the Superior Laryngeal Nerve (ibSLN).
Branches of the internal branch of the superior laryngeal nerve (ibSLN).
External Branch of the Superior Laryngeal Nerve
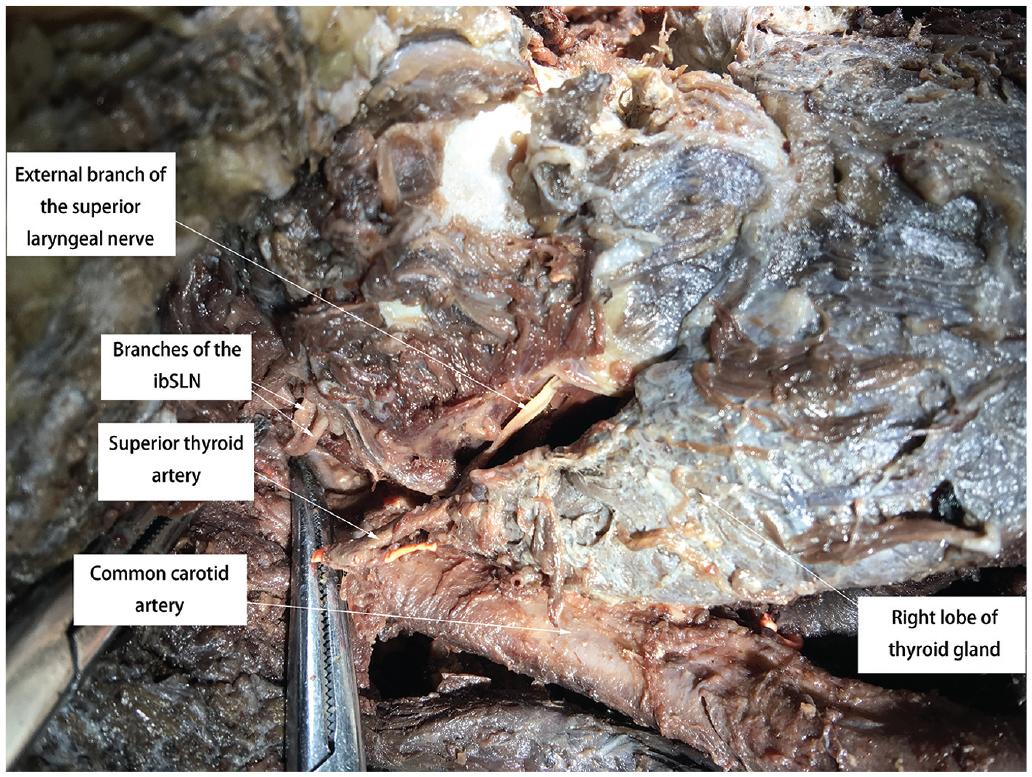
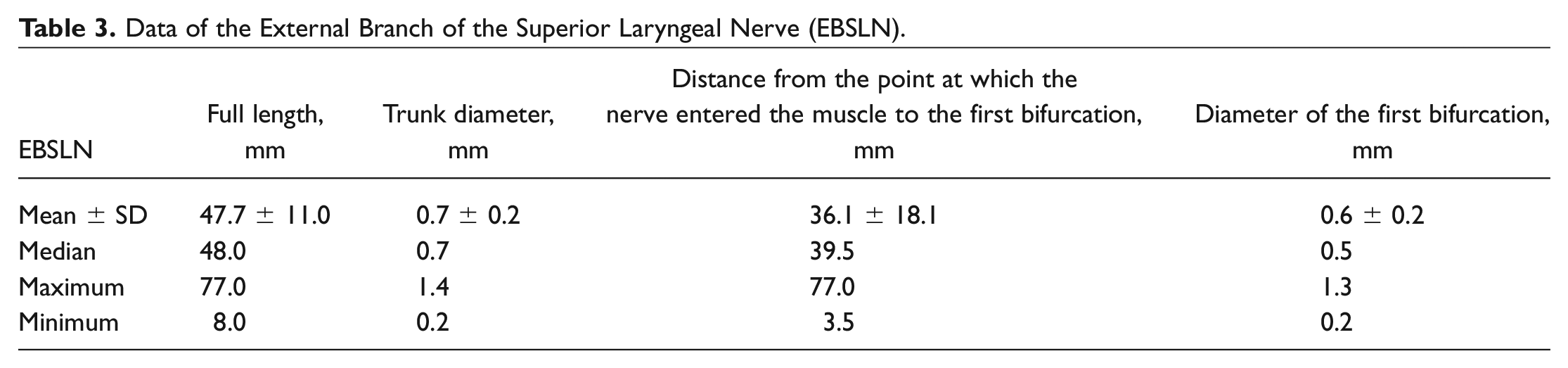
We measured 132 EBSLNs in this study. The mean total length was 47.7 ± 11.0 mm. The EBSLN was longer in men than in women (P < .000). There was no difference with regard to side (P = .538). The average trunk diameter was 0.7 ± 0.2 mm. There was no difference based on sex (P = .152) or side (P = .359). The average distance from the point at which the nerve entered the muscle to the first bifurcation was 36.1 ± 18.1 mm. The mean diameter of the first bifurcation was 0.6 ± 0.2 mm ( Table 3 ). The number of bifurcations was between 0 and 5. There were 2 cases (1.5%) of no bifurcations, 81 cases of 1 bifurcation (61.4%), 33 cases of 2 bifurcations (25.0%), 8 cases of 3 bifurcations (6.1%), 5 cases of 4 bifurcations (3.8%), and 3 cases of 5 bifurcations (2.3%) ( Figure 3 ). There were 2 cases (1.5%) of the EBSLN and STA having no points of intersection and 79 cases (59.9%) of the EBSLN crossing behind the STA. There were 50 cases (37.9%) of the EBSLN interweaving with the STA and 1 case (0.8%) of the EBSLN crossing in front of the STA. There were 110 cases (83.3%) of the EBSLN running along the surface of the IPC and 20 cases (15.2%) of the EBSLN penetrating the IPC. There was 1 case (0.8%) of the EBSLN penetrating the IPC, exiting the IPC, and then entering the larynx and 1 case (0.8%) of the EBSLN penetrating the IPC and then reentering the cricothyroid muscle. There was a total of 23 cases (17.4%) of the EBSLN entering the larynx at the cricothyroid muscle and 109 cases (82.6%) of the EBSLN entering the larynx at the IPC.
Data of the External Branch of the Superior Laryngeal Nerve (EBSLN).
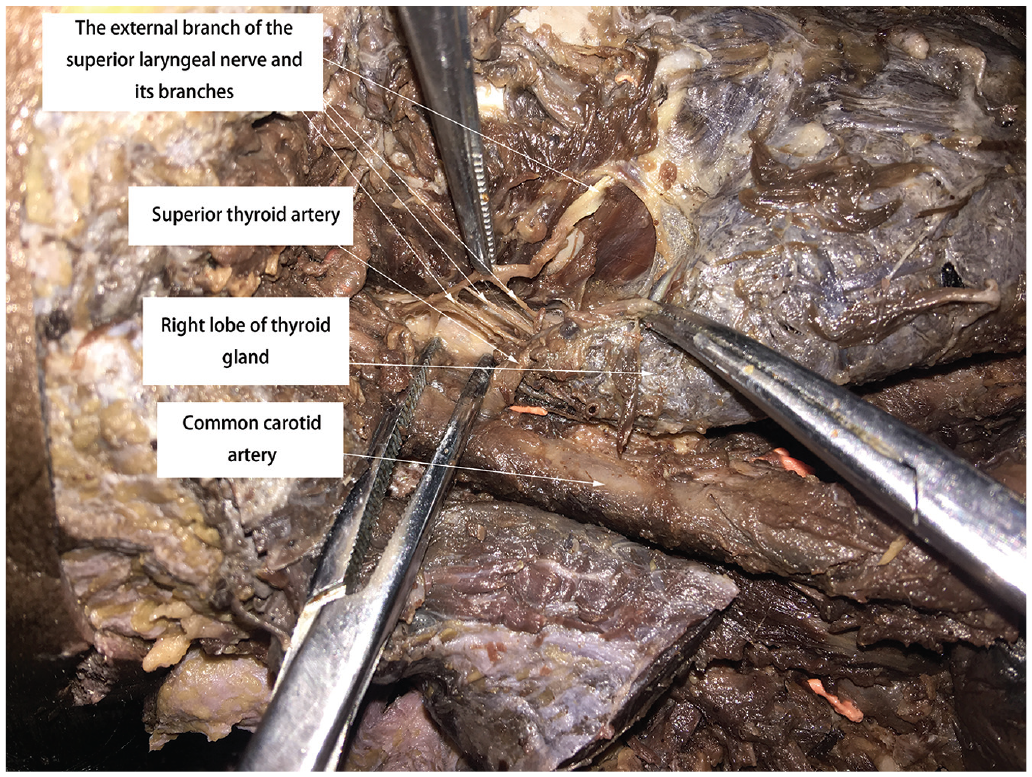
The external branch of the superior laryngeal nerve and its branches.
The EBSLN has a different relationship with the superior thyroid, and the classification criteria are based on the standards in Cernea et al. 20 In our study, the EBSLN crossed the superior thyroid vessels within >1 cm of the upper pole of the thyroid gland (type I in the Cernea classification) in 43 patients (32.6%), within 0 cm and 1 cm in 84 patients (63.6%) (type IIa in the Cernea classification), and within <0 cm in 5 patients (3.8%) (type IIb in the Cernea classification).
Relationship Between the Entrance Point of the EBSLN and the Midpoint of the Lower Margin of the Thyroid Cartilage
This study provides an innovative method of quickly locating the EBSLN. We set the line between the midpoint of the lower margin of the thyroid cartilage and the point of nerve entry into the laryngeal muscle as the hypotenuse. One side adjacent to the right angle in the triangle was formed by the line between the intersection of the vertical line passing through the entry point of nerve into the laryngeal muscle and the horizontal line passing through the midpoint of the lower edge of the thyroid cartilage and the entry point of the nerve into the laryngeal muscle. The other adjacent side was formed by the line between the point of the intersection of the vertical line passing through the entry point of nerve into the laryngeal muscle and the horizontal line passing through the midpoint of the lower edge of the thyroid cartilage and the midpoint of the lower edge of the thyroid cartilage.
When the EBSLN entry point was above the horizontal line formed by the lower margin of the thyroid cartilage, the angle between the line connecting the EBSLN entry point and the midpoint of the lower edge of the thyroid cartilage and the horizontal line passing through the midpoint of the lower margin of the thyroid cartilage was between 12.5° and 77.5°. The average value of the angle was 28.2 ± 13.0°, the 5th percentile was 13.7°, and the 95th percentile was 57.2°. The distance from the entry point of the EBSLN to the midpoint of the lower margin of the thyroid cartilage was between 18.0 mm and 42.0 mm. The average length was 30.7 ± 6.8 mm, the 5th percentile was 18.9 mm, and the 95th percentile was 41.1 mm.
When the EBSLN entry point was below the horizontal line of the lower margin of the thyroid cartilage, the angle between the line connecting the EBSLN entry point and the midpoint of the inferior margin of the thyroid cartilage and the horizontal line passing through the midpoint of the lower margin of the thyroid cartilage was between 0.0° and 51.0°. The average value of the angle was 5.7 ± 12.5°, the 5th percentile was 0.0°, and the 95th percentile was 36.5°. The distance from the entry point of the EBSLN to the midpoint of the lower margin of the thyroid cartilage was between 10.0 mm and 35.0 mm. The average length was 23.8 ± 5.9 mm, the 5th percentile was 13.9 mm, and the 95th percentile was 34.0 mm.
Discussion
The length of the ibSLN was reported to be 21 to 84.9 (44.9 ± 1.0 mm) by Furlan et al, 17 64 ± 1.2 mm by Lang et al, 21 and 57.2 ± 7.7 mm by Kiray et al. 22 The diameter of the ibSLN was reported to be 2.1 ± 0.2 mm by Kiray et al 22 and 1.8 to 2.0 mm by Stephens et al. 23 The length and diameter of the ibSLN in those reports are almost twice those measured in our data, which we think is due to ethnic differences and different starting and ending points of measurement.
Paraskevas et al 24 found that the ibSLN was divided into 3 branches in 72.2% of cases and into 2 branches in 27.8% of cases. We believe that the small sample size used by the previous authors and ethnic differences may be responsible for these differences.
The diameter of the EBSLN is usually approximately 0.8 mm. 9 Our results are similar to those in a previous report. The length of the EBSLN was reported to be 99.7 mm by Lang et al, 21 62.6 mm by Furlan et al, 17 and between 5 and 7 cm by Espinoza et al. 25 Our results were slightly different from the above results, which may be related to measurement errors.
Cernea et al 20 described 3 relationships between the EBSLN, the STA, and the upper pole of the thyroid gland. In type I (60%), the EBSLN crosses over the STA more than 1 cm above the upper pole of the thyroid. In type IIa (17%), the EBSLN crosses over the STA less than 1 cm above the upper pole of the thyroid. In type IIb (20%), the EBSLN crosses the cross the STA below the upper pole of the thyroid. Cheruiyot et al 26 reported that in Chinese populations, type I accounted for 29.0%, type IIa accounted for 52.2%, and type IIb accounted for 18.8%. Cha et al 10 also found that in Chinese populations, type I accounted for 27.6%, type IIa accounted for 51.7%, and type IIb accounted for 20.7%. In our research, type I accounted for 32.6%, type IIa accounted for 63.6%, and type IIb accounted for 3.8%, which was similar to the previous proportions.
There are many classification methods for the anatomical relationship between the EBSLN and the IPC, and the proposed classification by Friedman et al 27 is generally accepted. In type 1, the EBSLN runs its entire course superficial to the IPC, while in type 2, the EBSLN penetrates the lower fibers of the IPC. In type 3, the EBSLN runs beneath the IPC fibers. This study showed that there were some problems in this classification method because the classification boundary between type 2 and type 3 was not sufficiently accurate. Therefore, we only considered 2 types in our comparison: in the first type, the EBSLN ran along the surface of the IPC, while in the second type, the EBSLN ran deep into the IPC at any point along its trajectory. A systematic review and meta-analysis by Cheruiyot et al 26 also reported that the EBSLN runs superficial to the IPC in cadaveric studies in 87.7% of the cases; in Asian populations, that value was 83.6%, which was similar to our finding of 83.3%.
The EBSLN has a varying anatomical relationship to the STA, but most authors have reported that the EBSLN passes medial to the STA.28-30 In our study, the EBSLN passed through the medial side of the STA in 59.9% of the cases, which was consistent with the finding of the above study.
Due to the vulnerability of the EBSLN, many surgeons have proposed landmarks to avoid damage. Aina and Hisham 31 reported dissection from the inside of the upper pole of the thyroid to expose the EBSLN instead of using the landmark proposed by Cernea et al. 20 Moosman and DeWeese 29 described a “sternothyroid–laryngeal triangle” bounded by the sternothyroid muscle superiorly, the inferior constrictor and cricothyroid muscles medially, and the superior pole of the thyroid inferiorly, within which the EBSLN could be found. It is difficult for surgeons, especially young surgeons, to find the EBSLN with the above methods. There is relatively large variability in the placement of the landmarks. Our research proposes a new method to find the entry point of the EBSLN: the point where the EBSLN enters the laryngeal muscle is in a bilaterally symmetrical circular area at the midpoint of the lower edge of the thyroid cartilage. The upper boundary of the area is a straight line; this line is centered on the midpoint of the lower edge of the thyroid cartilage, 41.1 mm as the radius, and the upward intersection angle with the horizontal line is 57.2 degrees. The lower boundary of the area is also a straight line; this line is centered on the midpoint of the lower edge of the thyroid cartilage, 34.0 mm as the radius, and the downward intersection angle with the horizontal line is 36.5 degrees ( Figure 4 and Figure 5 ).
Entry point of the external branch of the superior laryngeal nerve (EBSLN) (ortho-position).

Entry point of the external branch of the superior laryngeal nerve (EBSLN) (lateral position).
Conclusions
The anatomical characteristics of the SLN are important to those undertaking thyroid surgery. This study found that the SLN in Chinese people has distinct anatomical characteristics that can be summarized and used to identify the EBSLN entry points into laryngeal muscles. This provides a theoretical basis for the search and protection of the EBSLN during thyroid surgery.