
Abstract
Objective
We performed a meta-analysis and estimated the prevalence of depression and anxiety and their related factors among patients with chronic rhinosinusitis (CRS).
Data Sources
PubMed, Embase, Web of Science, Cochrane Library, CINAHL, PsycINFO, and CBM databases.
Review Methods
A systematic search was performed for relevant studies published before August 17, 2021. A random effects model was used to estimate the prevalence of depression and anxiety. Subgroup analysis was performed by continent or region, study setting, sex, sample size, diagnosis, and assessment method.
Results
Twenty-two articles covering 40,956 patients were included in the meta-analysis. The pooled crude prevalence estimates of depression and anxiety were 25.2% (95% CI, 20.9%-29.6%) and 28.9% (95% CI, 16.1%-41.6%), respectively. Subgroup analyses revealed the following: (1) continent or region, study setting, sex, sample size, depression assessment method, and CRS diagnosis were significantly correlated with the prevalence of depression, and (2) continent or region, study setting, sample size, anxiety assessment method, and CRS diagnosis were significantly correlated with the prevalence of anxiety. Meta-regression analysis revealed that study setting and sample size were negatively associated with the pooled prevalence of depression. In contrast, CRS diagnosis and anxiety assessment method were positively associated with the pooled prevalence of anxiety.
Conclusion
Depression and anxiety are common in patients with CRS, especially among clinics. Therefore, in patients with CRS, screening and early diagnosis of depression and anxiety are necessary for prevention and treatment.
Chronic rhinosinusitis (CRS) is a common upper respiratory tract disease characterized by diffuse inflammation of the sinus mucosa. 1 CRS is also a common and frequently occurring disease in otorhinolaryngology. The prevalence of CRS ranges from 14% to 16% in the US population,2,3 approximately 10% in UK adults, 4 and about 8% in the Chinese population. 5 CRS has a long and recurrent course, which seriously affects the quality of life of patients and causes a huge social and economic burden.6,7
Depression and anxiety are 2 of the most common mental health conditions worldwide. 8 It has been reported that 19.1% of British adults show symptoms of depression or anxiety. 9 Depression is the leading cause of disability in the United States, with an estimated economic burden of $83 billion per year. 10 There is also evidence that depression and anxiety are highly prevalent in patients with CRS3,11; the prevalence of depression is approximately 20% to 36%. In addition, depression and anxiety in CRS may seriously affect the daily life and work of patients, reduce social productivity, 12 and lead to higher medical costs13,14; moreover, some studies have found that the diagnosis of depression and anxiety may be an important prognostic indicator for the treatment of patients with CRS. 15
Depression and anxiety are often underdiagnosed in patients with chronic conditions such as CRS, probably because clinicians do not often realize the importance of underlying depression and anxiety when treating primary chronic diseases. 16 There is research evidence that depression and anxiety in patients with CRS may be associated with reduced quality of life, cognitive dysfunction, and increased risk of suicidity.17-19 Moreover, depressive and anxiety symptoms in patients with CRS deteriorate over time, so early recognition and diagnosis of depressive and anxiety symptoms and initiation of subsequent treatment are important.
One systematic review regarding the prevalence of depression in patients with CRS was published by Schlosser et al 20 ; however, the prevalence of depression and anxiety in patients with CRS is unknown, as is the prevalence between the sexes and among countries and regions, diagnostic criteria and assessment tools, and patient sources. Therefore, this meta-analysis aimed to analyze the relevant literature to estimate the prevalence of depression and anxiety in patients with CRS, which will help health care providers and policy makers design better and more effective treatment and management strategies for CRS and reduce the disease burden in patients with CRS.
Methods
This study was conducted in accordance with the PRISMA statement (Preferred Reporting Items for Systematic Reviews and Meta-analyses; Supplementary Material 1, available online). 21 This review has been registered with the International Prospective Register of Systematic Reviews (PROSPERO CRD42021279918).
Search Strategy
Two investigators (F.C. and J.C.) independently searched the literature in the PubMed, Cochrane Library, Embase, Web of Science, CINAHL, PsycINFO, and CBM databases to comprehensively collect relevant studies on depression and anxiety in patients with CRS from database establishment to August 17, 2021. The search was based on medical subject headings and free words: depression, depress*, depressive, depressive disorder, depressive symptoms, anxiety, anxiety disorders, anxi*, anxiety symptoms, rhinosinusitis, sinusitis, chronic rhinosinusitis, chronic sinusitis, CRS, sinus*. We also screened the references from relevant articles or reviews to obtain eligible reports not collected in the aforementioned databases. Specific search strategies are outlined in Supplementary Material 2 (available online).
Inclusion and Exclusion Criteria
The criteria were as follows:
Study type: cross-sectional, case-control, and cohort (only the baseline data of studies were extracted)
Study sample: patients with CRS according to standardized diagnostic criteria, such as the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS), International Classification of Diseases (ICD), European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS), and Korean Classification of Diseases (KCD). All patients had to have a confirmed physician diagnosis of CRS; there was no restriction on the cause and type of CRS, race, age, or sex.
Outcome measures: the prevalence of depression and the prevalence of anxiety. Depression and anxiety assessments included previous physician diagnoses or screening by validated questionnaires.
When >1 article was published based on the same data set, only the one with the largest sample was included.
Exclusion criteria were as follows: self-reported CRS; studies in a mixed population of patients with various sinonasal diseases, unless data from patients with CRS could be separated; and unavailable raw data and duplicate published studies.
Study Selection
Two investigators (F.C. and L.L.) independently screened the literature, extracted the data, and cross-checked them according to the inclusion and exclusion criteria. Any disagreements that occurred were resolved through discussion or consultation with the third investigator (J.C.). The titles were read first during literature screening. After exclusion of apparently irrelevant studies, the abstracts and full texts were then read for inclusion. If required, the authors of the original study were contacted by mail or telephone to obtain information not reported but important for this study.
Data Extraction
Data were extracted by 2 investigators (F.C and L.L.) using a standardized predefined data collection spreadsheet in Microsoft Excel 2019, and the extracted contents included the following: (1) study characteristics, including the first author’s name and year of publication; (2) characteristics of the sample, such as size, mean age, and proportion of female participants; (3) study design, environmental setting, and country in which the study was conducted; (4) diagnostic criteria for CRS; (5) assessment methods for depression and anxiety; and (6) outcomes (ie, prevalence of depression and anxiety). Any disagreements that occurred were resolved through discussion or consultation with the third investigator (J.C.).
Quality Assessment
The methodological quality of the studies was assessed with the modified version of the Newcastle-Ottawa Scale (NOS), which consisted of 5 items: sample representativeness and size, comparability between respondents and nonrespondents, determination of depression and anxiety symptoms, and statistical quality. Studies were judged to be at a low risk of bias (≥3 points) or high (<3 points; Supplementary Material 3, available online). The quality evaluation of each study was independently conducted by 2 investigators (F.C. and L.L.). In the event of any disagreements or differences, the third investigator (J.C.) was consulted for discussion and adjudication.
Statistical Analysis
Meta-analysis was performed with Stata 12.0 (StataCorp). A random effects model was used to calculate the pooled prevalence of depression and anxiety with the 95% CI.22-24 The heterogeneity among the study results was analyzed by chi-square test (α = 0.1) and was quantitatively determined in combination with I2. I2 > 50% was used as a criterion to validate between-study heterogeneity. When there was no statistical heterogeneity among the study results (I2 < 50%, P > .1), a fixed effects model was used for meta-analysis. When there was statistical heterogeneity among the study results (I2 > 50%, P≤ .1), a random effects model was used for meta-analysis. The significance level of the meta-analysis was set at α = 0.05.
To explore potential causes of heterogeneity, subgroup analyses were performed by continent or region (North America, Europe, Asia, Africa), study setting (clinic, outpatient, hospital, community), sex (male, female), sample size via the median splitting method (≤150, >150), depression and anxiety assessment method, and CRS diagnosis. Meta-regression analysis was also performed for CRS diagnosis, publication year, sample size, sex, depression/anxiety assessment method, and continent or region (P < .10) to determine whether covariates could explain the heterogeneity among studies. Sensitivity analyses were conducted per the leave-one-out method. In addition, publication bias was investigated with funnel plots and Egger’s linear regression test. Statistical tests were 2-sided, and significance was set at P < .05.
Results
Literature Search
A total of 8732 studies were initially identified. After exclusion of duplicate studies (n = 2609) and obviously unrelated studies from review of the titles and abstracts (n = 6007), 116 full-text articles were read. Finally, 22 studies were included in our study. The literature screening process and results are shown in Figure 1 .
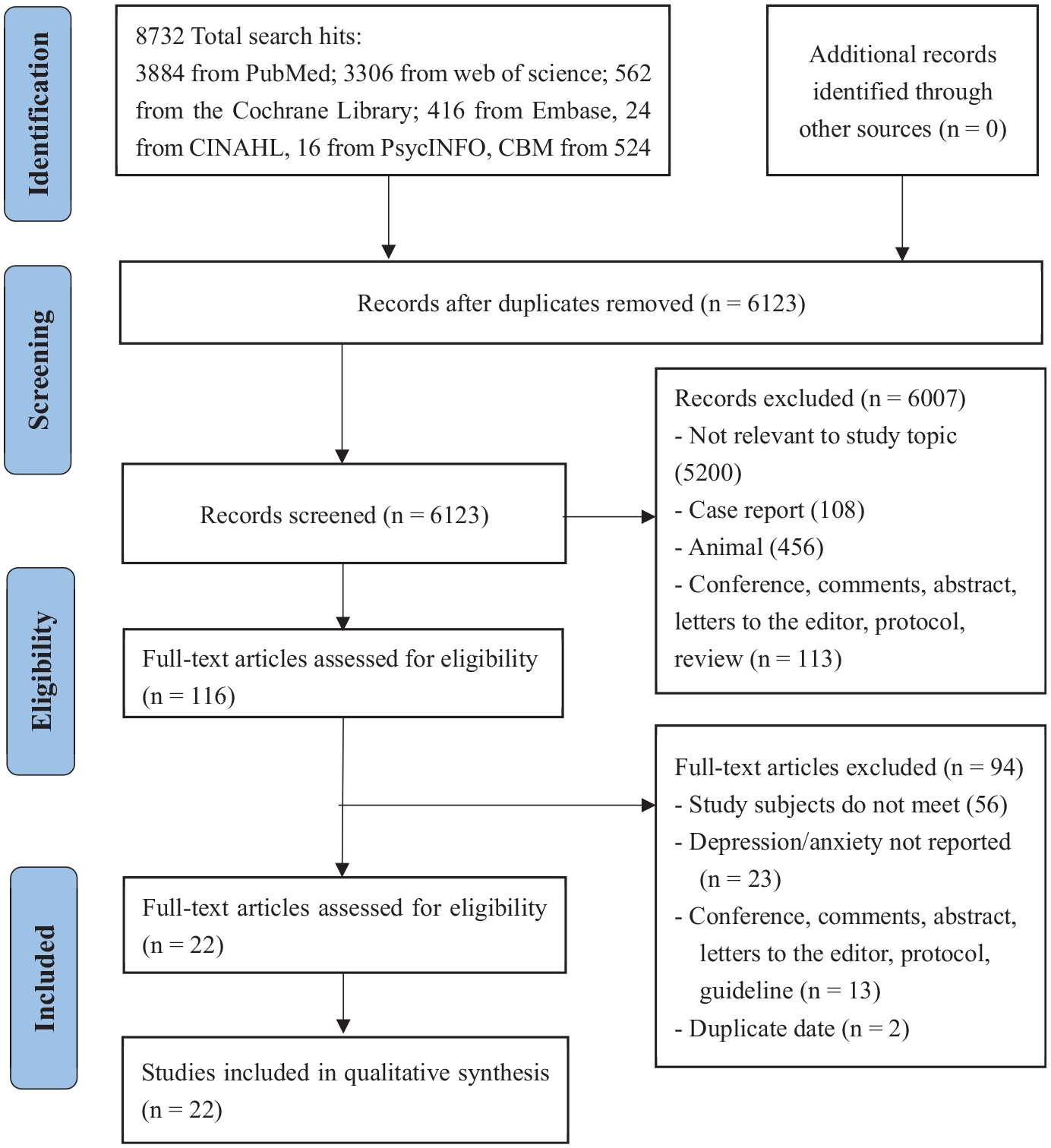
Literature screening procedure and results: PRISMA diagram.
Characteristics of the Studies
The basic characteristics of the literature are shown in Table 1 . Of the 22 studies,3,10,11,13,14,25-41 the samples were recruited in North America (n = 15), Asia (n = 3), Europe (n = 3), and Africa (n = 1). The investigated outcomes were depression (n = 22 studies) and anxiety (n = 9 studies); of these, 6 and 4 respectively reported the prevalence of depression in male and female patients. All studies had clear diagnostic criteria for CRS: 10 studies, AAO-HNS; 5 studies, ICD; 5 studies, EPOS; and 2 studies, KCD, AAO-HNS, and EPOS. For assessing depression and anxiety, 5 studies used standardized diagnosis codes (ICD, KCD), while other studies used measurement tools such as the Patient Health Questionnaire (PHQ-9 or PHQ-2), Hospital Anxiety and Depression Scale, Beck Depression Inventory II, Short Form–8, Functional Comorbidity Index, General Anxiety Disorder–7, and Brief Symptom Inventory.
Studies Included in the Meta-analysis.a
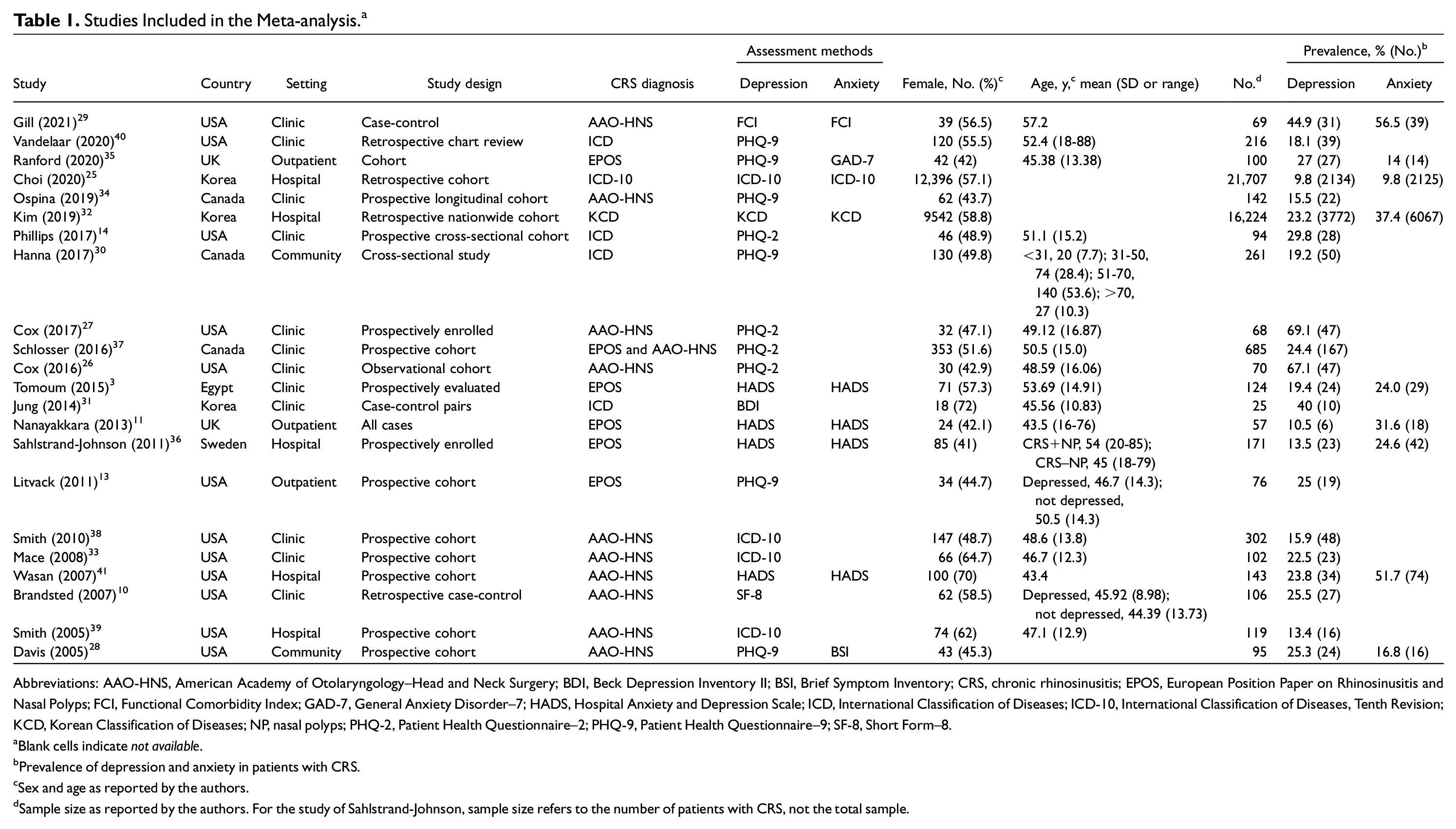
Abbreviations: AAO-HNS, American Academy of Otolaryngology–Head and Neck Surgery; BDI, Beck Depression Inventory II; BSI, Brief Symptom Inventory; CRS, chronic rhinosinusitis; EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps; FCI, Functional Comorbidity Index; GAD-7, General Anxiety Disorder–7; HADS, Hospital Anxiety and Depression Scale; ICD, International Classification of Diseases; ICD-10, International Classification of Diseases, Tenth Revision; KCD, Korean Classification of Diseases; NP, nasal polyps; PHQ-2, Patient Health Questionnaire–2; PHQ-9, Patient Health Questionnaire–9; SF-8, Short Form–8. aBlank cells indicate not available. bPrevalence of depression and anxiety in patients with CRS. cSex and age as reported by the authors. dSample size as reported by the authors. For the study of Sahlstrand-Johnson, sample size refers to the number of patients with CRS, not the total sample.
Study Quality
Based on the modified NOS for quality assessment, the 22 studies were scored from 2 to 5. Only 1 study was high risk (NOS score <3), and 21 were low risk (NOS score ≥3). The details of the NOS scores are shown in Supplementary Material 4 (available online).
Prevalence of Depression in CRS
In this meta-analysis, 22 studies reported the prevalence of depression in patients with CRS. Random effects prevalence estimates are presented in Figure 2 . The pooled crude prevalence of depression was 25.2% (95% CI, 20.9%-29.6%; I2 = 98.6%).
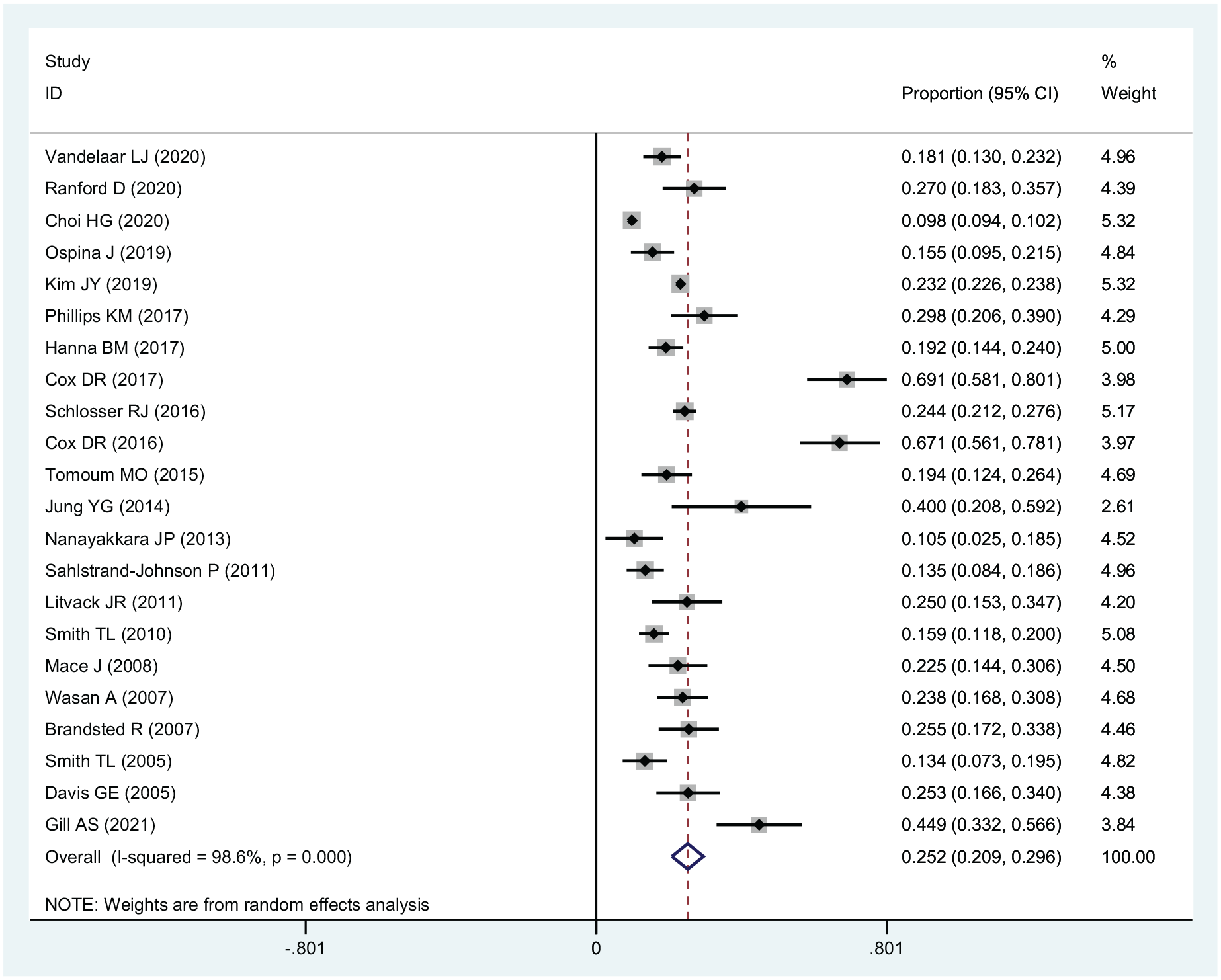
Prevalence of depression in chronic rhinosinusitis.
Prevalence of Anxiety in CRS
In this meta-analysis, 9 studies reported the prevalence of anxiety in patients with CRS. Random effects prevalence estimates are presented in Figure 3 . The pooled crude prevalence of anxiety was 28.9% (95% CI, 16.1%-41.6%; I2 = 99.8%).
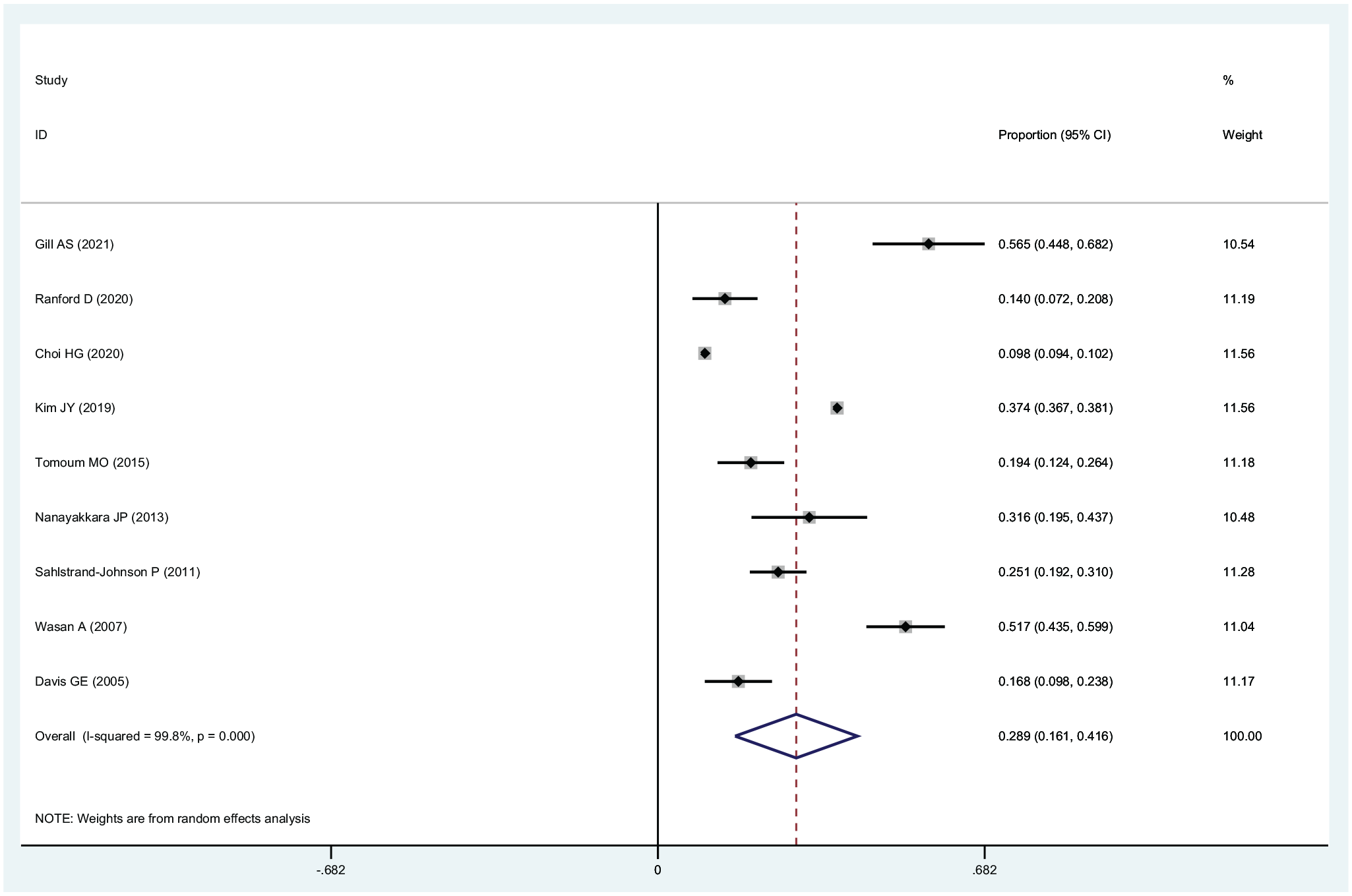
Prevalence of anxiety in chronic rhinosinusitis.
Subgroup Analysis
As shown in Table 2 , the continent or region, study setting, sex, sample size, depression assessment method, and CRS diagnosis were significantly associated with the pooled prevalence of depression. Studies with North American patients with CRS, patients from the clinic, use of the AAO-HNS for diagnosis of CRS and the PHQ-2 to assess depression, female patients, and sample sizes ≤150 had a higher pooled prevalence of depression (P < .001).
Subgroup Analysis of the Prevalence of Depression. a
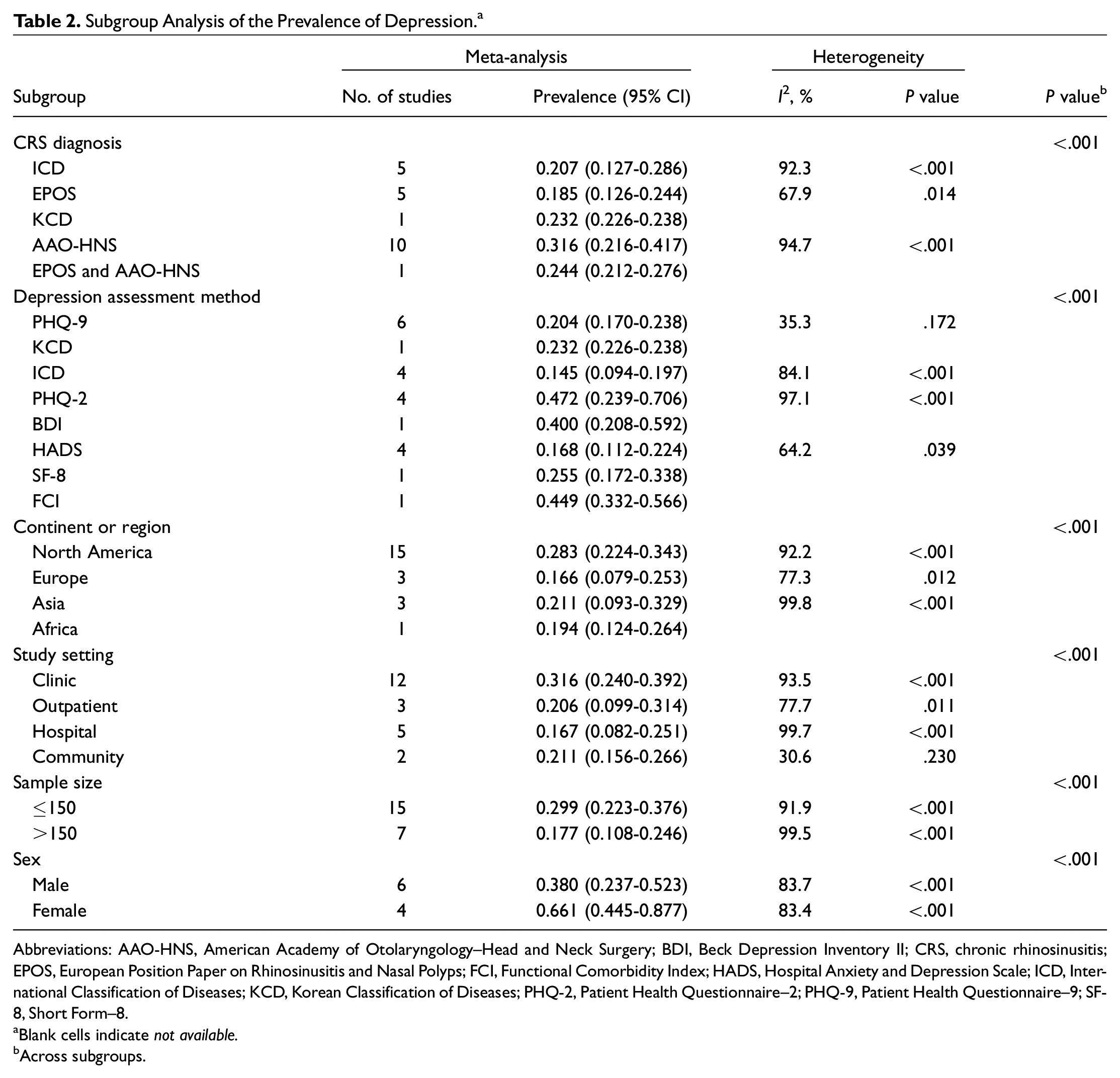
Abbreviations: AAO-HNS, American Academy of Otolaryngology–Head and Neck Surgery; BDI, Beck Depression Inventory II; CRS, chronic rhinosinusitis; EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps; FCI, Functional Comorbidity Index; HADS, Hospital Anxiety and Depression Scale; ICD, International Classification of Diseases; KCD, Korean Classification of Diseases; PHQ-2, Patient Health Questionnaire–2; PHQ-9, Patient Health Questionnaire–9; SF-8, Short Form–8.
Blank cells indicate not available.
Across subgroups.
As shown in Table 3 , the continent or region, study setting, sample size, anxiety assessment method, and CRS diagnosis were significantly associated with the pooled prevalence of anxiety. Studies with North American patients with CRS, patients from the clinic, use of the AAO-HNS for diagnosis of CRS and the Functional Comorbidity Index to assess anxiety, and sample sizes ≤150 had a higher pooled prevalence of anxiety (P < .001).
Subgroup Analysis of the Prevalence of Anxiety. a
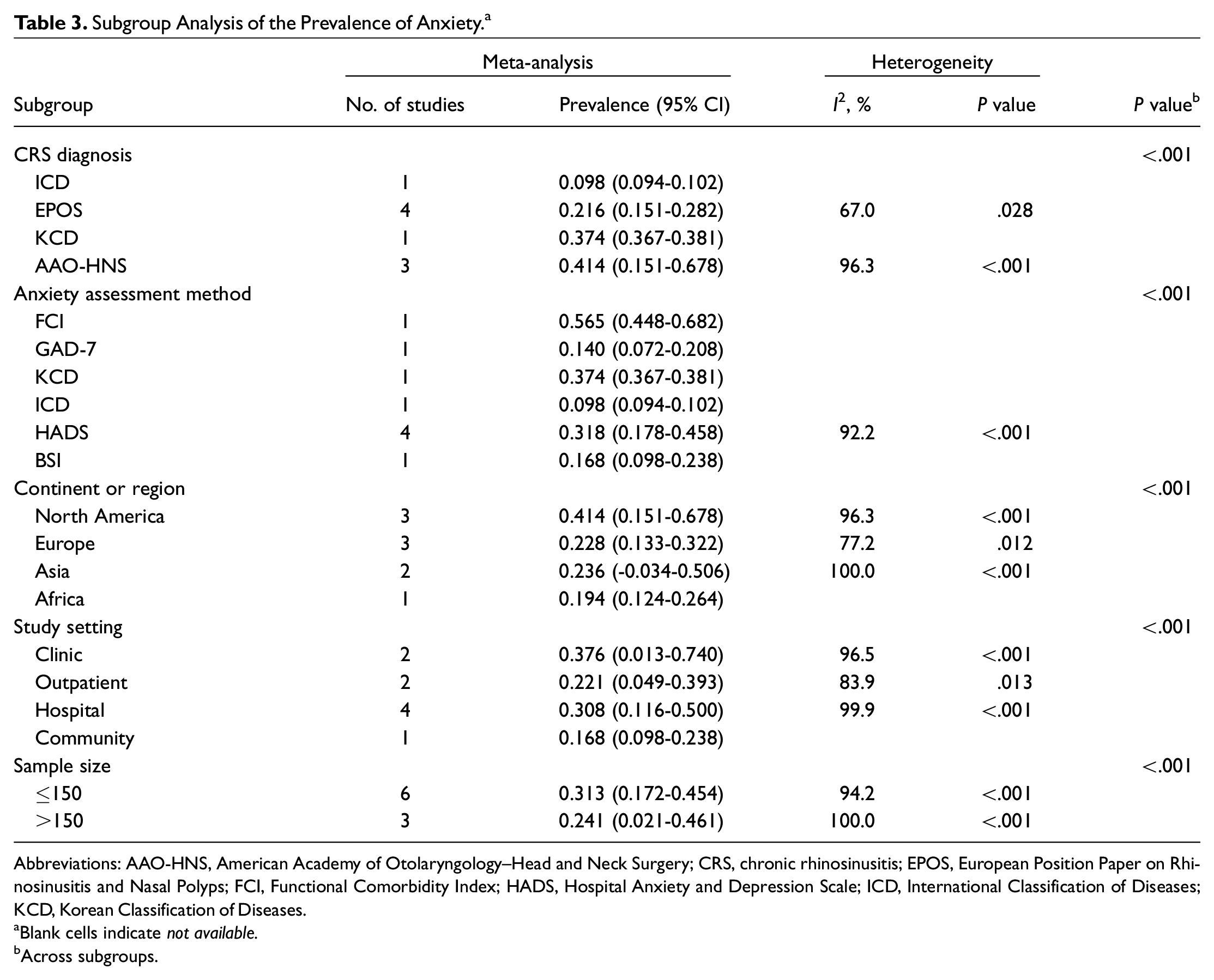
Abbreviations: AAO-HNS, American Academy of Otolaryngology–Head and Neck Surgery; CRS, chronic rhinosinusitis; EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps; FCI, Functional Comorbidity Index; HADS, Hospital Anxiety and Depression Scale; ICD, International Classification of Diseases; KCD, Korean Classification of Diseases.
Blank cells indicate not available.
Across subgroups.
Meta-regression Analyses
Meta-regression analyses revealed that study setting (coefficient = –0.053, t = –1.80, P = .086) and sample size (coefficient = –0.122, t = –1.84, P = .081) were negatively associated with the pooled prevalence of depression. In contrast, CRS diagnosis (coefficient = 0.453, t = 3.81, P = .007) and anxiety assessment method (coefficient = 0.416, t = 2.69, P = .031) were positively associated with the pooled prevalence of anxiety (Supplementary Material 5, available online).
Publication Bias and Sensitivity Analysis
The funnel plot and Egger’s test did not reveal publication bias in the pooled prevalence of depression (Egger’s test: t = 2.03, P = .056) or anxiety (t = 0.79, P = .454; Supplementary Material 6, available online). Sensitivity analyses did not find outliers that could significantly change the pooled prevalence of depression and anxiety in CRS (Supplementary Material 7).
Discussion
Depression and Anxiety Are Common in Patients With CRS
CRS is an inflammatory disease of the sinus channel, and depression and anxiety are common psychological disorders, both of which can seriously affect the physical and mental health of patients and cause a huge socioeconomic burden. Our meta-analyses (22 studies, N = 40,956) investigated the prevalence of depression and anxiety among patients with CRS via quantitative analysis methods, which revealed that the pooled prevalences of depression and anxiety were 25.2% and 28.9%, respectively. These prevalences were significantly higher than those of the general population (5%-10%). 42
There are many potential mechanisms for the higher prevalence of depression and anxiety in patients with CRS. First, previous studies have shown that patients with CRS tend to have a range of systemic effects, such as sleep dysfunction, pain, and cognitive disorders,3,43,44 all of which can increase the likelihood of depression or anxiety. 45 Second, patients with CRS may feel socially isolated due to sinus symptoms (eg, impaired olfaction or taste, nasal congestion), increasing the risk of depression and anxiety. As with other chronic diseases, patients with CRS take a lot of time to visit the doctor and perform health care activities (eg, sinus lavage), 46 which can lead to frustration and eventually depression or anxiety. 20 In addition, patients with CRS may experience depression due to medical treatment. Systemic corticosteroids are commonly used to treat patients with CRS, with or without nasal polyps, due to their anti-inflammatory properties. A recent study showed that >70% of otolaryngologists use systemic steroids as the primary treatment for CRS, 47 yet systemic corticosteroid use is associated with increased depressive or manic symptoms, as well as mild behavioral changes. 48 In addition, chronic use of systemic corticosteroids in patients with CRS may lead to the development of depression. In other chronic diseases, the systemic inflammation hypothesis has been proposed; that is, inflammatory cytokine levels are linked to the severity of depression. 45 For example, an increase in circulating inflammatory cytokines may contribute to depression associated with conditions such as multiple sclerosis, rheumatic diseases, asthma, and allergies. 45 However, no study has been conducted on the hypothesis of systemic inflammation in CRS. Further studies are needed to better understand the relationship between depression and CRS.
The high prevalence of depression and anxiety in patients with CRS may be related to their combination with other diseases. Studies have shown that patients with chronic diseases such as diabetes, coronary heart disease, stroke, and rheumatoid arthritis may all have comorbid depression.49-51 Therefore, it is particularly important to explore the relationship between depression/anxiety and multiple chronic diseases in patients with CRS. Depressed patients may have physiologic effects due to their psychiatric illness or maladaptive behavior, thereby increasing the risk of the development of other diseases. 52 However, because of the biological changes or complications associated with these chronic conditions, depression may actually be an early manifestation, even an initial manifestation, of the underlying disease. 53 Comorbid depression has also been shown to influence treatment outcomes for other conditions. For example, patients with depression have increased rates of death and rehospitalization after coronary artery bypass graft surgery. 54 The relationship between comorbid depression and the prognosis of CRS is complex, but the underlying pathophysiologic mechanisms are unknown. Similar to other studies of chronic disease accompanied by depression, most CRS studies have shown that patients who are depressed will improve after treatment, but their quality of life is still lower than that of patients without depression. Therefore, more studies are needed to analyze these mechanisms and make therapeutic recommendations.
Prevalence of Depression and Anxiety Was Different Among Subgroups of Patients With CRS
Previous studies have explored symptoms or signs in patients with CRS, helping to predict which patients are at risk for depression. Findings on the association between sex and depression in CRS are inconsistent, with some studies finding an association between female sex and increased risk of depression31,33 and others arguing for no association.10,36,55,56 There is research evidence that the concentrations of the proinflammatory cytokines TNF-α and IL-6 are significantly higher in patients who are depressed, 57 which strengthens the evidence that depression is accompanied by activation of the inflammatory response system. As compared with men, women exhibit higher levels of inflammation and a higher incidence of autoimmune diseases, and these inflammatory pathways may play a key role in the pathophysiology of depression. 58 In summary, in clinical practice, special attention should be paid to depressive symptoms in women with CRS because women have worse disease-specific health-related quality of life and may be more susceptible to infection with inflammation and depression. 59
Depression is common in patients with CRS, with a prevalence of about 25%. The diagnostic criteria for depression are mainly diagnosed by mental health experts using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. However, due to the diversity of current screening and assessment tools for depression, most studies in this article assessed depression based on tools such as the PHQ, Hospital Anxiety and Depression Scale, and ICD, which contain multiple items and have clear cutoff values. Health care workers or other primary care personnel can assign scores according to whether the patient's performance / symptoms meet the evaluation scale entries to determine whether the patient is depressed or anxious. The assessment tool is simple and easy to understand and takes a short time to complete so that health care workers can more easily identify depression and anxiety symptoms in clinical practice. We found that as screening tools become more detailed and the threshold for defining depression decreases, the prevalence of depression detected is also increasing, exceeding the prevalence of depression based on existing physician diagnoses alone. The findings suggest that the prevalence of depression and anxiety in patients with CRS as assessed by instruments such as the PHQ, Hospital Anxiety and Depression Scale, and ICD may be overestimated.
Studies have shown that the expected prevalence of depression in the general primary care setting is lower than the prevalence of depression in the CRS population, suggesting that patients with CRS are routinely screened for depression in clinical practice. 60 Some studies have used the PHQ-2 as a screening tool. Although it is not sufficient to determine the diagnosis of depression, patients with positive screening results (ie, patients at high risk of depression) can consult a mental health specialist as early as possible to determine depression status or actively adopt personalized interventions, which will in turn reduce the prevalence of depression with CRS.14,61
Our study found that the prevalence of depression and anxiety in patients with CRS was higher in North America than in other regions. Kawada observed a similar prevalence of depression in patients with rheumatoid arthritis, 62 and Zhang et al showed that the prevalence of depression in patients with systemic lupus erythematosus was higher in the Americas than in other regions. 63 This may result from differences in culture, religious beliefs, and socioeconomic status, or it may be caused by differences in national and cultural backgrounds with perceptions, interpretations, and judgments of personal value and dignity. 64 Vandelaar et al showed that the prevalence of depression in patients with CRS was higher in the Korean region than in the United States, 40 which may be due to inconsistent depression assessment tools. Future studies should use uniform criteria to assess depression in patients with CRS of different sexes in different regions to detect depression as early as possible and intervene in time to improve patients’ quality of life.
Strengths and Limitations
This study represented the first systematic review and meta-analysis that ascertained the prevalence of depression and anxiety in patients with CRS. The modified NOS scores that assessed the quality of the studies ranged from 2 to 5, suggesting the overall high quality that ensured the reliability and authenticity of the findings of this study. Also, multiple databases were searched to ensure a broad representation of articles, which improved the stability of the results.
There were several limitations to our study. First, assessment methods and thresholds for depression and anxiety are inconsistent, which may result in large differences in estimates of depression/anxiety prevalence among patients with CRS. Second, the scales used to evaluate depression and anxiety cannot be used as a formal diagnosis of mental disorders; these scales also tend to overestimate prevalence as compared with clinician diagnosis. In addition, most studies were conducted in clinics or hospitals and were not representative of the outpatient and community populations due to the complexity of patients. Given the apparent heterogeneity, the pooled results should be interpreted with caution.
Because data on CRS subtypes, severity of disease, comorbidities, and so on were not readily available in the studies, the factors influencing depression and anxiety in patients with CRS were not explored. Future studies should evaluate the effects of CRS subtypes, disease severity, comorbidities, income, and insurance status on the prevalence of depression and anxiety in patients with CRS to investigate whether more disease burden is associated with poorer mental health. To provide evidence for medical personnel to identify the risk of depression and anxiety in CRS patients. In addition, diagnostic criteria and cut-off values of depression and anxiety should be proposed for patients with different CRS subtypes, different regions, severity, and comorbidities to improve the diagnostic accuracy of CRS.
Conclusion
The prevalence of depression and anxiety is high among patients with CRS. Thus, identification of individuals with high-risk depression/anxiety with CRS in clinical practice is paramount to prevent adverse outcomes. Future studies are needed to investigate the prevalence of different severities of depression and anxiety in patients with CRS, as well as the effects of factors such as sex and age, to provide a basis for the development of targeted preventive measures to manage CRS-related depression and anxiety.
Supplemental Material
sj-doc-1-oto-10.1177_01945998221082538 – Supplemental material for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis
Supplemental material, sj-doc-1-oto-10.1177_01945998221082538 for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis by Fei Chen, Libo Liu, Yetong Wang, Ke Hu, Bin Ma and Junting Chi in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-1-oto-10.1177_01945998221082538 – Supplemental material for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-oto-10.1177_01945998221082538 for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis by Fei Chen, Libo Liu, Yetong Wang, Ke Hu, Bin Ma and Junting Chi in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-2-oto-10.1177_01945998221082538 – Supplemental material for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-2-oto-10.1177_01945998221082538 for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis by Fei Chen, Libo Liu, Yetong Wang, Ke Hu, Bin Ma and Junting Chi in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-3-oto-10.1177_01945998221082538 – Supplemental material for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-3-oto-10.1177_01945998221082538 for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis by Fei Chen, Libo Liu, Yetong Wang, Ke Hu, Bin Ma and Junting Chi in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-4-oto-10.1177_01945998221082538 – Supplemental material for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-4-oto-10.1177_01945998221082538 for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis by Fei Chen, Libo Liu, Yetong Wang, Ke Hu, Bin Ma and Junting Chi in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-5-oto-10.1177_01945998221082538 – Supplemental material for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-5-oto-10.1177_01945998221082538 for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis by Fei Chen, Libo Liu, Yetong Wang, Ke Hu, Bin Ma and Junting Chi in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-6-oto-10.1177_01945998221082538 – Supplemental material for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-6-oto-10.1177_01945998221082538 for Prevalence of Depression and Anxiety in Patients With Chronic Rhinosinusitis: A Systematic Review and Meta-analysis by Fei Chen, Libo Liu, Yetong Wang, Ke Hu, Bin Ma and Junting Chi in Otolaryngology–Head and Neck Surgery
Footnotes
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.