
Abstract
Objective
Chronic tinnitus is a clinical symptom that affects 10% to 15% of the adult population. Repetitive transcranial magnetic stimulation (rTMS) is a promising treatment, but significant heterogeneity exists in the treatment outcomes and stimulation parameters. In this study, we perform a qualitative systematic review to determine if there is an optimal rTMS site to treat tinnitus.
Data Sources
A literature search was performed by searching the MEDLINE, Embase, Web of Science, and Cochrane databases.
Review Methods
Sham-controlled studies in adults were included that contained >10 patients with tinnitus for >3 months and utilized 10 to 20 electroencephalography coordinates. Study outcomes were considered positive if the treatment arm reported a significant reduction in the primary tinnitus score relative to sham.
Results
There were 1211 studies screened. Nineteen studies met the inclusion criteria, and 8 unique stimulation sites were reported. Studies had 53.7 ± 46.0 patients (mean ± SD). The mean duration of follow-up was 10.3 ± 9.6 weeks. Positive outcomes regarding tinnitus suppression were reported in 5 of 5 (100%) studies stimulating the temporoparietal junction midway between T3 and P3 or between T4 and P4. Tinnitus suppression at all other sites was less frequent with a combined success rate of only 8 of 14 (57.1%).
Conclusion
Significant heterogeneity exists in the literature in regard to the optimal transcranial magnetic stimulation target. These preliminary findings suggest that the temporoparietal junction midway between T3 and P3 or T4 and P4 is a promising nonauditory rTMS target in the setting of chronic tinnitus. Future research should elucidate the effectiveness of this site for tinnitus suppression.
Chronic tinnitus is a clinical symptom that affects 10% to 15% of the adult population.1-3 Tinnitus severely affects the daily life of patients and can lead to difficulties with sleep, attention, and concentration, among others.4,5 Despite this extensive morbidity, few long-term definitive therapies exist. 6 Numerous treatment strategies have been proposed for tinnitus management, though most treatments focus on symptom management rather than the underlying cause. 6 Such treatments include diverse pharmacologic therapies, such as lidocaine and antidepressants, acupuncture, cognitive behavioral therapy, and sound-masking therapies.7-9 Clinical response to these treatments often vary among patients, making the clinical management of chronic tinnitus particularly challenging.
In recent years, repetitive transcranial magnetic stimulation (rTMS) has emerged as a novel treatment for patients with chronic tinnitus.10,11 rTMS is a noninvasive method that involves delivering electromagnetic pulses via an electrical coil to the head of a patient. By direct stimulation of the patient’s head, magnetic energy is able to penetrate the surface tissue layers and directly interface with the cortical matter of the brain. rTMS can be administered as a low- or high-frequency stimulation. Previous work has demonstrated that low-frequency stimulation is able to depress individual neuronal networks whereas high-frequency stimulation excites networks.12,13 As such, over the past 2 decades, an extensive literature has developed investigating rTMS to the auditory cortex as a modality to treat chronic tinnitus.
While numerous prospective clinical trials investigating rTMS for tinnitus have been conducted, the success of these trials has largely been variable.14-17 Currently, significant heterogeneity exists within the literature in regard to the optimal stimulation site to achieve tinnitus suppression.18,19 While most studies have focused on stimulating the auditory cortex directly, it is becoming increasingly clear that chronic tinnitus is a complex neurologic phenomenon involving interactions between auditory and nonauditory regions of the brain. 20 Previous work has demonstrated that the perception of tinnitus is composed of networks involved in attention, perception, distress, and memory, among others.20,21 As a result, various nonauditory targets, including the temporoparietal junction (TPJ) and dorsolateral prefrontal cortex, have been studied as possible rTMS targets to treat chronic tinnitus.18,22
While numerous brain regions have been investigated, no current consensus exists on which site is best. 23 To date, multiple systematic reviews have been conducted evaluating the efficacy of rTMS for tinnitus, yet none have focused on the optimal location for stimulation.10,14,15 Selection of an evidence-based nonauditory transcranial magnetic stimulation (TMS) target may be critical for the future of clinical trials for tinnitus. This study was conducted to qualitatively analyze TMS sites to determine if the literature suggests an optimal target to treat chronic tinnitus.
Methods
A systematic review was performed utilizing the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses). Studies examining the effectiveness of rTMS in treating tinnitus were identified by searching electronic databases: MEDLINE (Ovid), Embase (Elsevier), the Web of Science Core Collection (Clarivate), and the Cochrane Central Register of Controlled Trials (Wiley). Searches were constructed with terms for tinnitus and rTMS and run on November 11, 2020. No language or date restrictions were applied (Appendix, available online).
All studies were reviewed by 2 independent reviewers (N.W. and J.G.N.). Article selection was performed in 2 phases. First, titles and abstracts of all identified records were reviewed by relevance to the topic. Second, full-text articles were reviewed and selected by strict adherence to the inclusion criteria. Studies were included per the following criteria: >10 adult patients with chronic tinnitus (defined as >3 months), a clinical tinnitus score as the primary outcome (eg, Tinnitus Handicap Index, Tinnitus Functional Index), a sham control group, and 10 to 20 electroencephalography (EEG) coordinates for targeting. Non-randomized controlled studies, meta-analyses, systematic reviews, case, series, letter, review articles, and conference proceedings were excluded from analysis.
The following data were extracted from all studies: number of patients, mean age, sex, TMS coil type, rTMS target, hearing status of patients, number of rTMS sessions, stimulation frequency, stimulation intensity, total number of pulses, mean duration of tinnitus, latest follow-up, 10 to 20 EEG coordinates of stimulation, tinnitus variable utilized for quantification, and study outcomes.
A formal risk of bias assessment was performed utilizing the Cochrane Collaboration’s Risk of Bias tool version 2. Each article was assessed for bias in the randomization process, deviations from intended interventions, missing outcome data, measurement bias, and selection bias.
Due to significant heterogeneity in the outcome variables utilized to measure tinnitus suppression, we were precluded from performing a detailed quantitative analysis. Thus, a qualitative analysis was performed in a binomial fashion based on study outcomes (positive or negative). Study outcomes were considered positive if the treatment arm reported a statistically significant reduction in the primary tinnitus score relative to sham at any point in the follow-up period.
Results
Study Selection
Database searching returned 2489 records; 1211 unique records remained after removal of duplicates. After initial title and abstract screening, 215 full-text articles were examined for eligibility, and 19 studies met the inclusion criteria and were included in the analysis ( Figure 1 ).
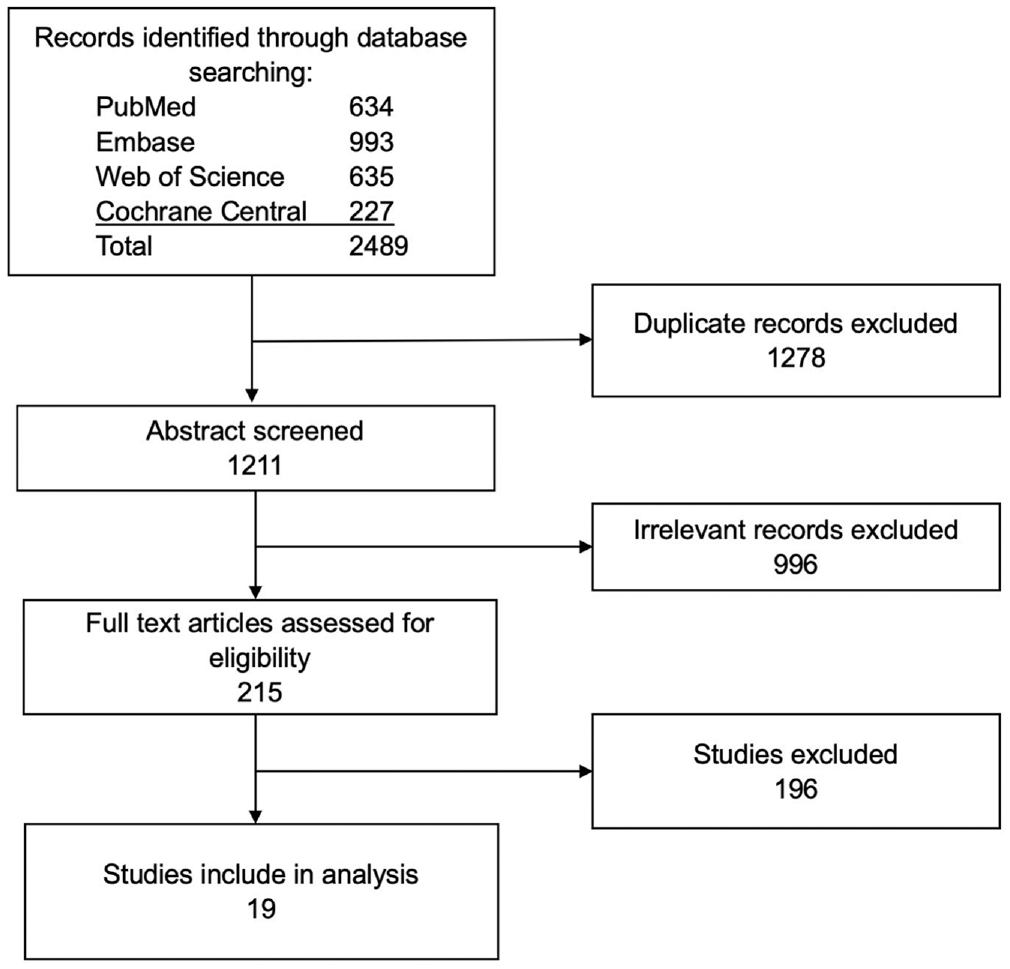
Flowchart summary of the systematic review literature search.
Study Characteristics
Table 1 highlights the characteristics of studies. The mean ± SD number of patients among studies was 53.7 ± 46.0. Patients had a mean age of 50.7 ± 6.0 years with a mean tinnitus duration of 9.2 ± 5.3 years. On average, 67.6% of study patients were male. Most studies (73.7%) contained cohorts of patients with normal and impaired hearing status. A figure-of-8 coil was the most frequently used coil (78.9% of studies). Studies utilized stimulatory (10 or 20 Hz) and inhibitory (1 Hz) frequencies, and 1 Hz was the most common frequency (57.9% of studies). Most studies (68.4%) stimulated at 110% the resting motor threshold. Studies reported a mean 9.1 rTMS sessions per patient. The mean duration of follow-up for all studies was >2 months (10.3 weeks).
Characteristics of 19 Studies.
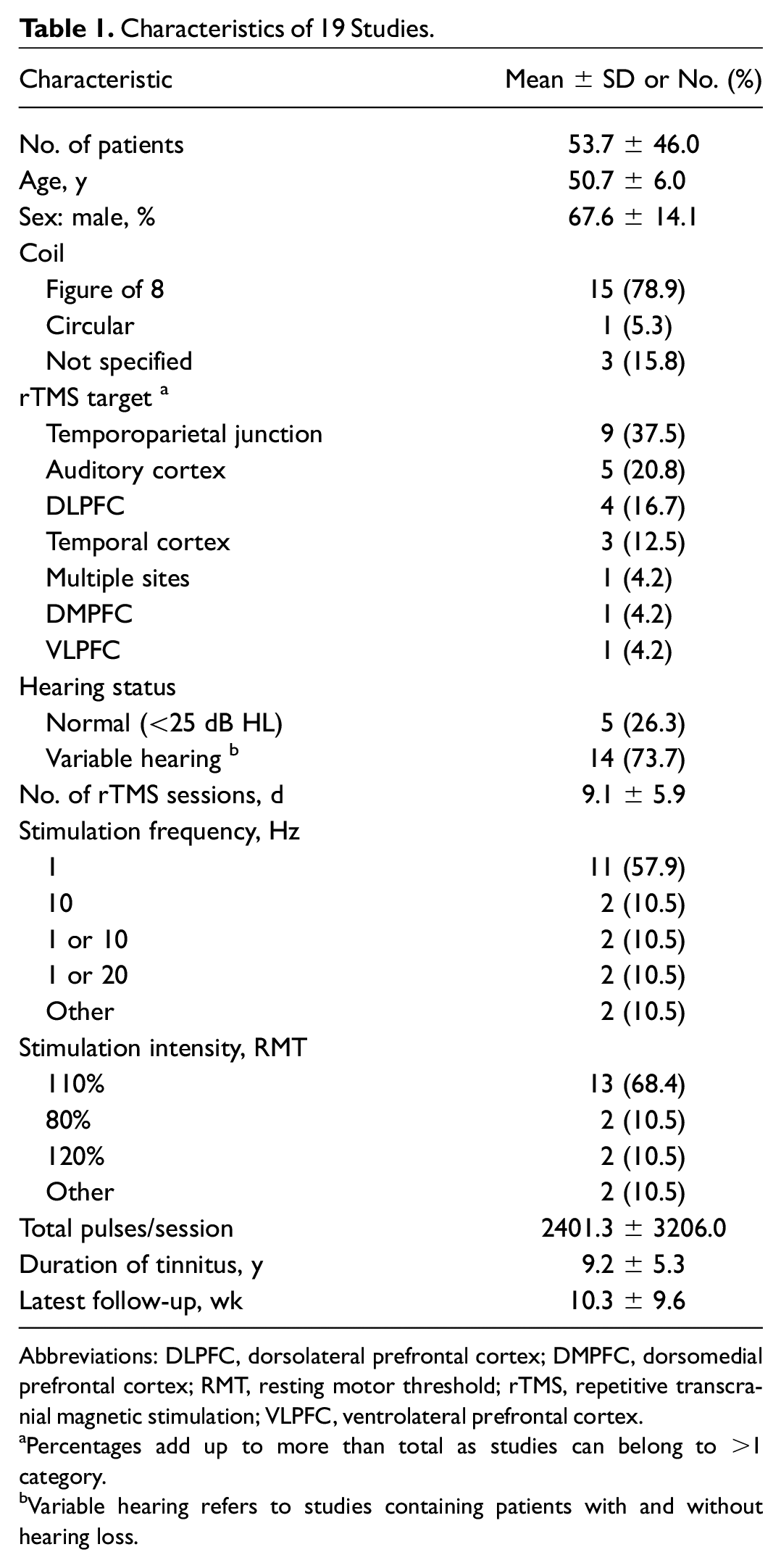
Abbreviations: DLPFC, dorsolateral prefrontal cortex; DMPFC, dorsomedial prefrontal cortex; RMT, resting motor threshold; rTMS, repetitive transcranial magnetic stimulation; VLPFC, ventrolateral prefrontal cortex.
Percentages add up to more than total as studies can belong to >1 category.
Variable hearing refers to studies containing patients with and without hearing loss.
Risk of Bias Assessment
A risk of bias analysis for the 19 studies is depicted in Figure 2 . Eleven studies (57.9%) had some concern for bias attributed to the randomization process; all other studies were at low risk for this domain. Most studies were at a low risk of bias due to deviation from the intended interventions (73.7%). Nine studies (47.4%) had some concern for bias due to missing outcome data; 1 study (5.3%) was at a high risk for this domain. Eighteen studies (94.7%) had low risk of measurement bias. All studies were at low risk of selection bias.
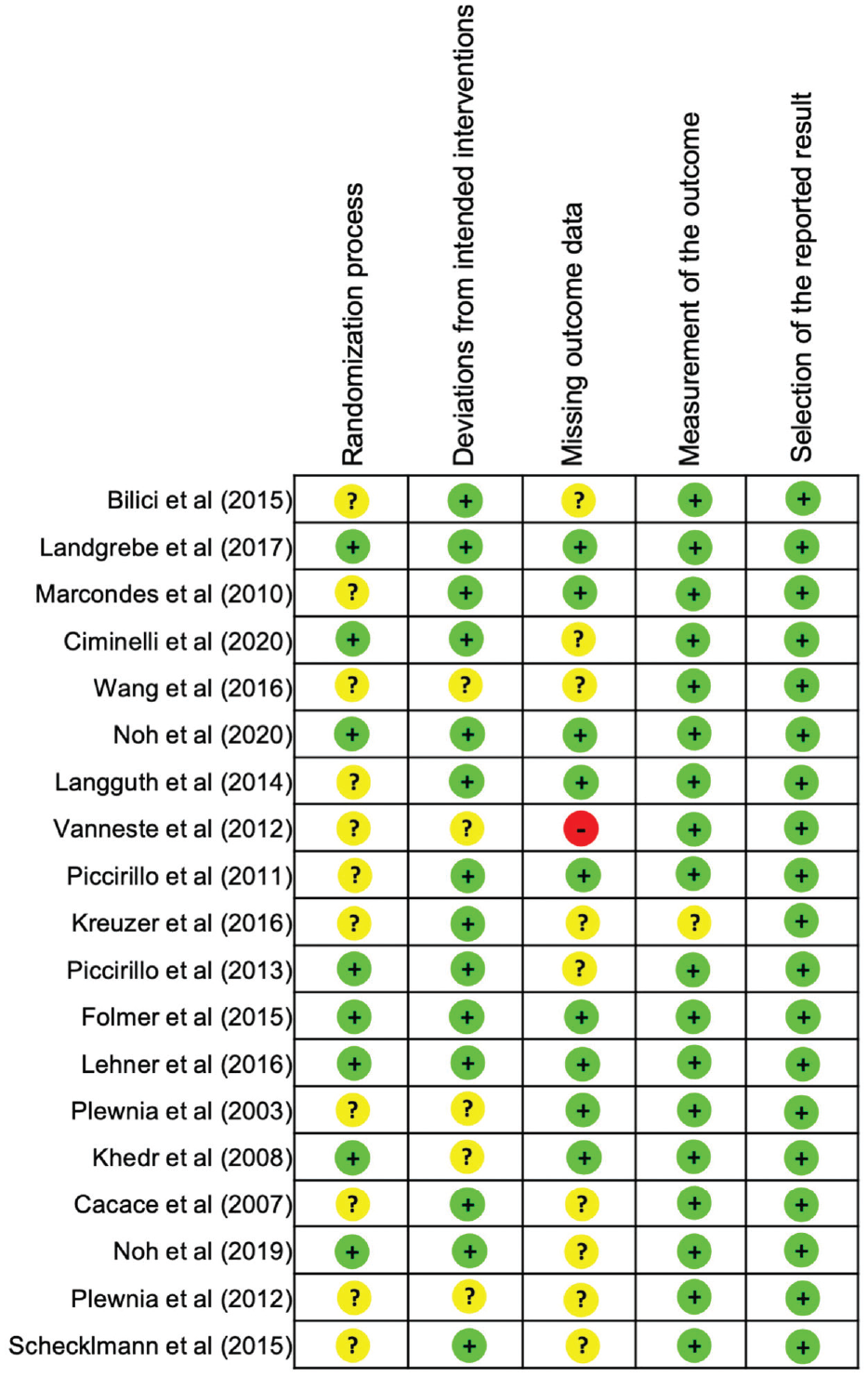
Risk of bias assessment of included studies. Green circles, a low risk of bias; yellow circles, some concerns; red circles, a high risk of bias for that domain.
Efficacy of rTMS by Stimulation Site
Table 2 illustrates the tinnitus improvement at each stimulation site investigated. Five studies stimulated the TPJ midway between T3 and P3 or T4 and P4, and all 5 (100%) reported significant tinnitus suppression ( Figure 3 ). Among these studies, efficacy was noted at excitatory and inhibitory rTMS frequencies, including 1, 10, and 20 Hz. Of these positive studies, 2 concurrently stimulated the dorsolateral prefrontal cortex at 20 Hz. Tinnitus suppression at all other sites was less frequent with a combined success rate of only 8 of 14 (57.1%). Stimulation of the TPJ at an alternative site midway between C3 and T5 suppressed tinnitus in just 1 of 3 (33.3%) studies. Directly targeting the auditory cortex at the left gyrus of Heschl suppressed tinnitus in half of studies (3/6, 50.0%). Other locations—including the dorsomedial prefrontal cortex, the ventrolateral prefrontal cortex, and a location within the temporal cortex (midway between T3 and T5)—contained just 1 study reporting tinnitus suppression.
Tinnitus Suppression by Stimulation Target.
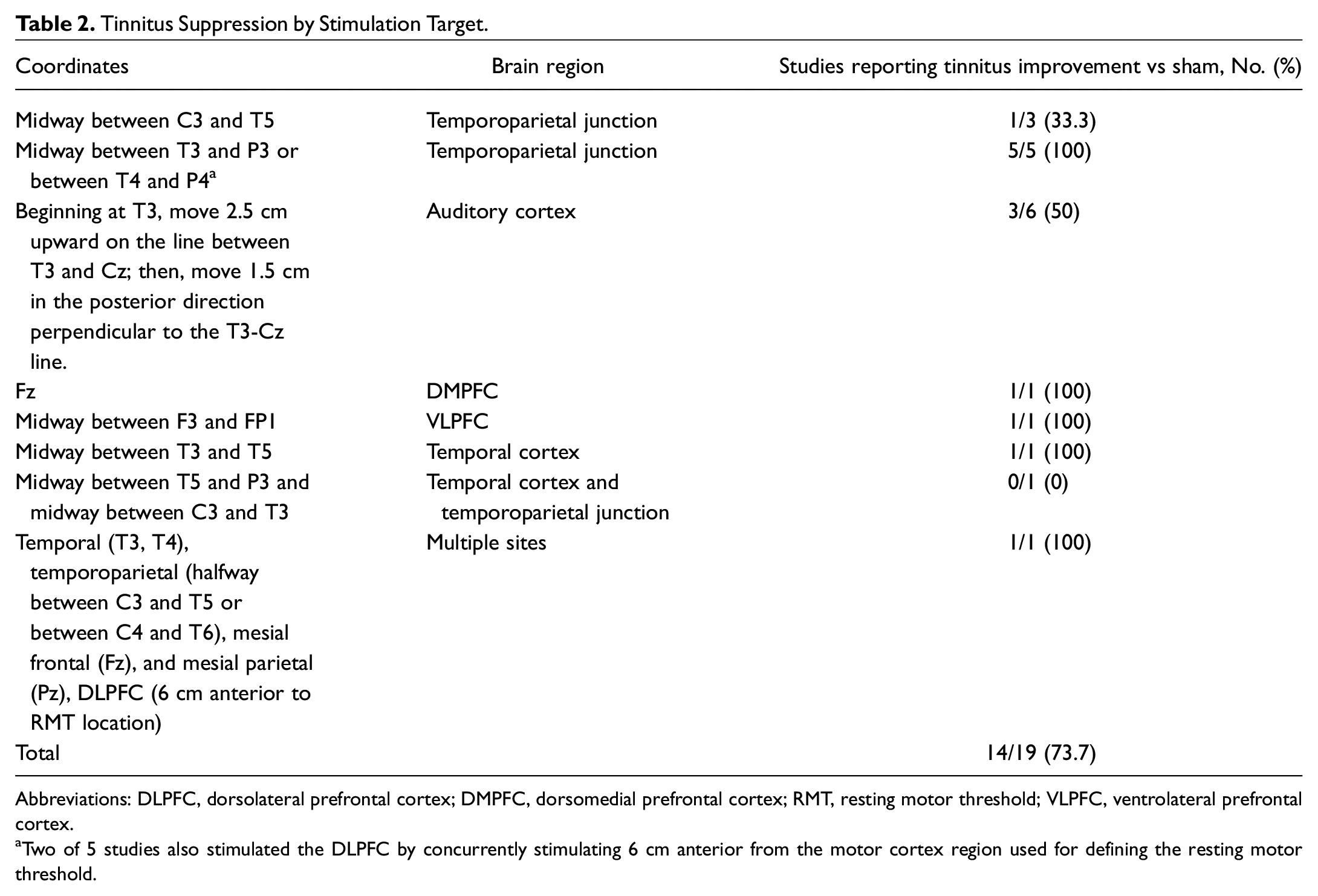
Abbreviations: DLPFC, dorsolateral prefrontal cortex; DMPFC, dorsomedial prefrontal cortex; RMT, resting motor threshold; VLPFC, ventrolateral prefrontal cortex.
Two of 5 studies also stimulated the DLPFC by concurrently stimulating 6 cm anterior from the motor cortex region used for defining the resting motor threshold.
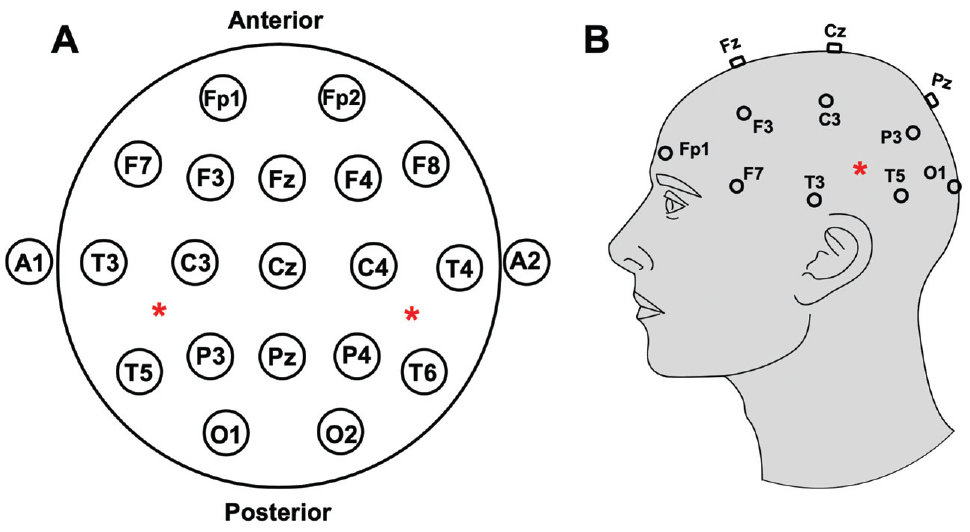
EEG coordinates (n = 10-20) and stimulation targets. (A) Axial and (B) sagittal depiction of the EEG coordinate system. Red asterisk represents region of interest midway between T3 and P3 or T4 and P4. EEG, electroencephalography.
Discussion
In this systematic review of 19 sham-controlled prospective articles assessing rTMS for the treatment of tinnitus, we sought to determine if there is an optimal stimulation site for tinnitus suppression based on localization with 10 to 20 EEG coordinates. To our knowledge, no other systematic reviews have directly compared the efficacy of various TMS sites for chronic tinnitus. We found that all published studies targeting the TPJ midway between T3 and P3 or T4 and P4 reported significant tinnitus suppression. All other sites had a combined success rate of only 57%. Notably, no other sites produced tinnitus suppression that was reproducible across multiple studies.
Since the early 21st century, animal models 24 and human studies 25 suggested that abnormal neural connections within the core auditory pathways are responsible for tinnitus perception. 26 Importantly, the loudness of phantom sounds was shown to be due to direct activation of the auditory cortex. 27 As such, early efforts of tinnitus suppression focused on inhibitory TMS directly to the auditory cortex. 26 To date, 2 large-scale double-blinded randomized controlled trials have been conducted investigating low-frequency inhibitory rTMS to the left gyrus of Heschl in the auditory cortex.16,17 Folmer et al found significant improvement in tinnitus as measured by the Tinnitus Functional Index up to 26 weeks following stimulation. 16 However, with similar stimulation protocols and patient cohorts, Landgrebe et al noted rTMS to not be superior than placebo. 17 Following the results of these landmark studies, the role of low-frequency TMS involving the auditory cortex remains uncertain.
Moreover, recent work has begun to increasingly show that tinnitus is due to alterations not only in the auditory circuitry but also in nonauditory brain regions. 28 While the auditory cortex has been shown to affect tinnitus loudness, 27 various brain-imaging methods have demonstrated numerous nonauditory regions, such as the dorsolateral prefrontal cortex, ventromedial prefrontal cortex, and amygdala, among others to be implicated in phantom sound perception. 20 As such, the heterogeneity in response to TMS may be closely linked to these variably involved networks. 29 As a result, a nonauditory region stimulated at a low or high frequency may serve to be a suitable location for future TMS trials for tinnitus. Yet, uncertainty exists in the literature in regard to an optimal nonauditory TMS target to treat tinnitus. 30
Our findings have several potential implications for the future of rTMS treatment for tinnitus. First, our results suggest a promising nonauditory target worthy of future research. The selection of an evidence-based nonauditory TMS target may serve to be critical for future clinical trials for tinnitus at locations beyond the left gyrus of Heschl in the auditory cortex. Second, given the current discrepancies in the literature, this study may provide the groundwork for similar studies critically analyzing additional rTMS parameters. Studies directed at better understanding other variables possibly contributing to rTMS outcomes, such as stimulation frequency, 31 hearing status, 32 or patient duration of tinnitus, 18 may serve to be equally important for future approaches to treat chronic tinnitus.
This study contains several limitations. The main limitation was heterogeneity within the outcomes, which largely restricted our ability to conduct formal statistical comparisons. Due to this small sample size and heterogeneous reporting of the tinnitus outcomes (eg, follow-up times, tinnitus scales, subjective vs objective benefit), we relied on qualitative comparisons to draw conclusions among stimulation sites. Next, several stimulation sites identified in our search had only 1 published article associated with them. As such, full interpretation of the success of these sites was impossible. Similarly, we considered a study to have a positive outcome with tinnitus improvement at any timepoint after rTMS. Thus, the durability of the response to therapy warrants future clarification. Additionally, due to the nature of our study design, it is possible that trials reporting negative results were not published and thus would not be identified in our search. It is possible that this publication bias could have influenced our methods and should be considered when interpreting our results. Importantly, since tinnitus is a subjective clinical phenomenon, various tools have been developed and validated to quantify tinnitus severity (eg, Tinnitus Handicap Index, Tinnitus Functional Index). Since multiple tools are utilized in this literature, homogenous analysis of tinnitus improvement is not possible, which limits the ability to interpret results across studies. Finally, it is established that success from rTMS for tinnitus largely produces transient benefit to patients and symptoms often following discontinuation of therapy. 33 While this study did not account for the length of time of improvement at each stimulation target, this is an important consideration for analyzing the success of treatment for future work in this area.
Conclusion
Significant heterogeneity exists in the literature in regard to the optimal TMS target for the suppression of tinnitus. The goal of this study was to qualitatively analyze TMS sites to determine if the literature suggests an optimal target to treat chronic tinnitus. The results presented herein suggest that the TPJ midway between T3 and P3 or T4 and P4 is a potentially advantageous nonauditory target for the treatment of chronic tinnitus. Notably, tinnitus suppression at all other sites was less frequent, including other coordinates within the TPJ and the auditory cortex. While the role of rTMS in the treatment of tinnitus continues to be uncertain, these results are relevant for the evidence-based selection of rTMS parameters for future clinical trials. Importantly, the strength of this work is that the data were extracted from only high-quality sham-controlled prospective clinical trials. However, our results serve to suggest the TPJ midway between T3 and P3 or T4 and P4 as a potential target for future research consideration based on published data in the existing literature. We anticipate future clinical studies to build on this work to further investigate this TPJ coordinate as well as other nonauditory targets to continue to better understand the role of TMS in treating chronic tinnitus.
Supplemental Material
sj-docx-1-oto-10.1177_01945998221102082 – Supplemental material for Is There an Optimal Repetitive Transcranial Magnetic Stimulation Target to Treat Chronic Tinnitus?
Supplemental material, sj-docx-1-oto-10.1177_01945998221102082 for Is There an Optimal Repetitive Transcranial Magnetic Stimulation Target to Treat Chronic Tinnitus? by Nathan Watson, Frederic L.W.V.J. Schaper, Sandrine Jabbour, Samantha Sadler, Paul A. Bain, Michael D. Fox and James G. Naples in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
This article was presented at the Brain Stimulation Conference; December 9, 2021; Charleston, South Carolina.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.