
Abstract
Health care costs can present a significant strain on patients with head and neck cancer. It remains unclear how much prices may vary among hospitals providing care and what factors lead to differences in prices of surgical procedures. A cross-sectional analysis of private payer–negotiated prices was performed for 10 commonly performed head and neck surgical oncology procedures. In total, 896 hospitals disclosed prices for at least 1 common head and neck surgical oncology procedure. Wide variation in negotiated surgical prices was identified. Across-center ratios ranged from 6.2 (partial glossectomy without primary closure) to 22.8 (excision of tongue lesion without closure). For-profit hospital ownership structure and geographic region outside of the northeast United States were associated with increased prices. For example, private payer–negotiated prices for direct laryngoscopy with biopsy were on average $2083 greater at for-profit hospitals when compared with nonprofit hospitals ($5215 vs $3132, P < .001). Further research comparing prices and outcomes is needed.
When compared with other patients with cancer, patients with head and neck cancer are particularly vulnerable to financial strain from costs of care. 1 The Centers for Medicare & Medicaid Services implemented the hospital price transparency rule effective January 1, 2021, to help patients make more financially informed decisions regarding their care. 2 Recent work revealed wide variation in the prices of thyroid cancer care across National Cancer Institute (NCI)–designated cancer centers. 3 Little is known about how hospital characteristics may influence these negotiated prices for cancer care.4,5 We sought to understand how prices may vary across the broader spectrum of centers providing head and neck cancer care and what factors may drive variation.
Methods
Data Collection
We conducted a cross-sectional analysis of hospital facility fees obtained from Turquoise Health, 6 a tool that sources data from machine-readable files publicly disclosed by hospitals (Supplemental Figure S1, available online). Hospital characteristics were obtained from Centers for Medicare & Medicaid Services data sources (Supplemental Methods) and are shown in Table 1 . The top 10 most common head and neck oncologic procedures for which data were available were selected, with expert opinion by the senior author to exclude procedures typically performed as concurrent procedures.
Characteristics of the Hospitals (N = 896).
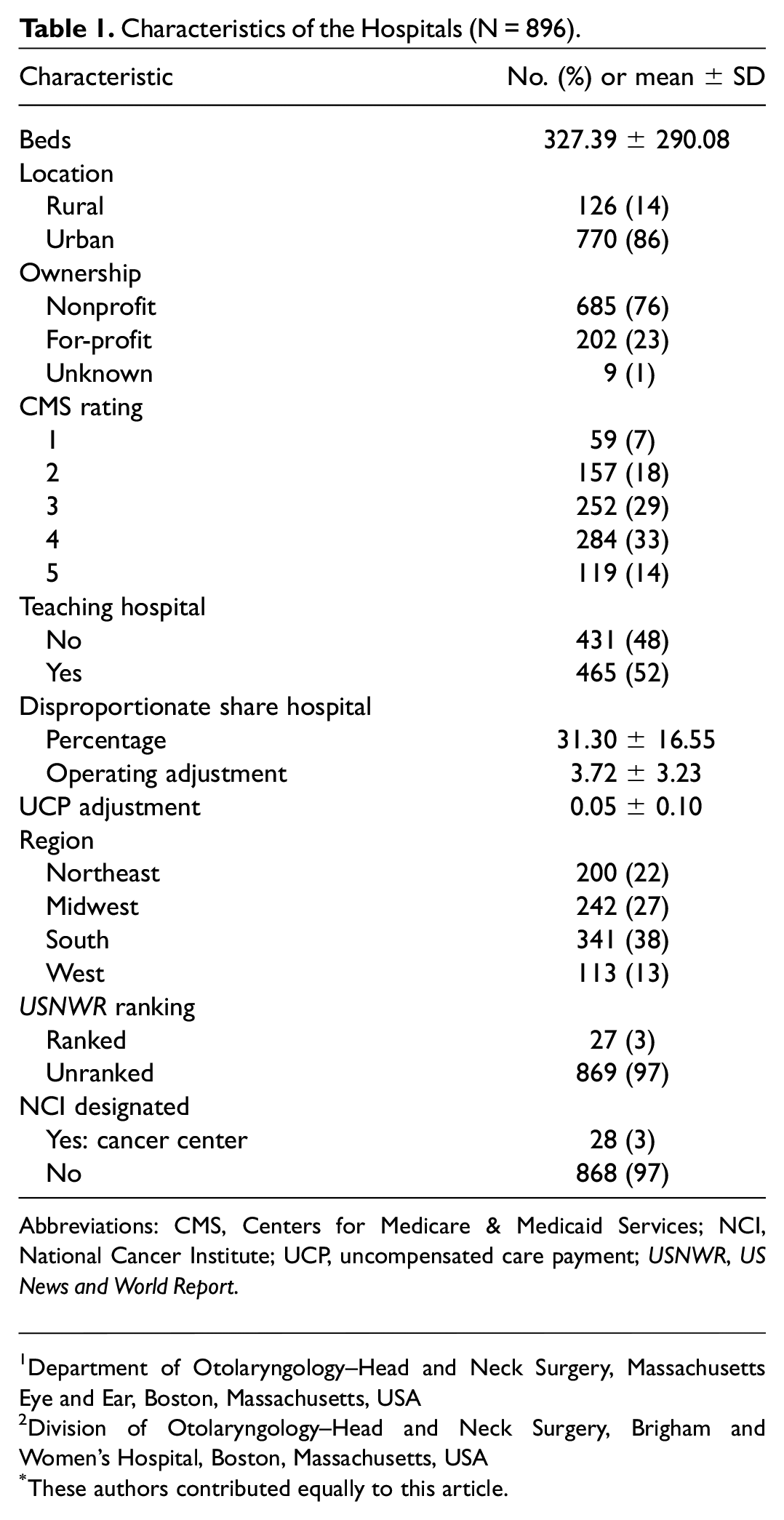
Abbreviations: CMS, Centers for Medicare & Medicaid Services; NCI, National Cancer Institute; UCP, uncompensated care payment; USNWR, US News and World Report.
Statistical Methods
Using previously described methods,3,7,8 we characterized the extent of price variation across and within centers for each procedure as across- and within-center ratios, respectively. Hospital prices were normalized by the hospital wage index. 9 The across-center ratio was calculated as the ratio between the 90th and 10th percentiles for the normalized median price by institution for each procedure. The within-center ratio was calculated as the ratio between the 90th and 10th percentiles for the negotiated price for a given procedure at each hospital.
Subset analyses were performed to compare the means of the median negotiated prices for each procedure based on Wilcoxon rank sum tests given the nonparametric nature of available data. All data analysis was performed using R version 4.1.2 (R Foundation). Mass General Brigham did not require institutional review board review or exemption because this study did not involve human participants. All pricing data were up-to-date as of February 19, 2022.
Results
Our analysis included 896 hospitals: 770 (85.9%) urban, 685 (76.4%) nonprofit/government, and 28 (3.1%) NCI cancer centers ( Table 1 ). The availability of negotiated price data varied by procedure, with as few as 243 hospitals reporting prices for neck dissection and as many as 676 reporting prices for direct laryngoscopy.
Hospital wage index–adjusted prices varied significantly across hospitals, with across-center ratios ranging from 6.2 for partial glossectomy without closure to 22.8 for tongue lesion excision without closure ( Figure 1 ). Prices also varied substantially within hospitals across payers, with median within-center ratios ranging from 2.1 (interquartile range [IQR] 1.3-4.4) for neck dissection to 2.7 for excision of anterior (IQR, 1.7-4.6) or posterior (IQR, 1.6-4.5) tongue lesion with closure. This indicates that at the same hospital, the negotiated price for a given procedure varied by more than double among payers.
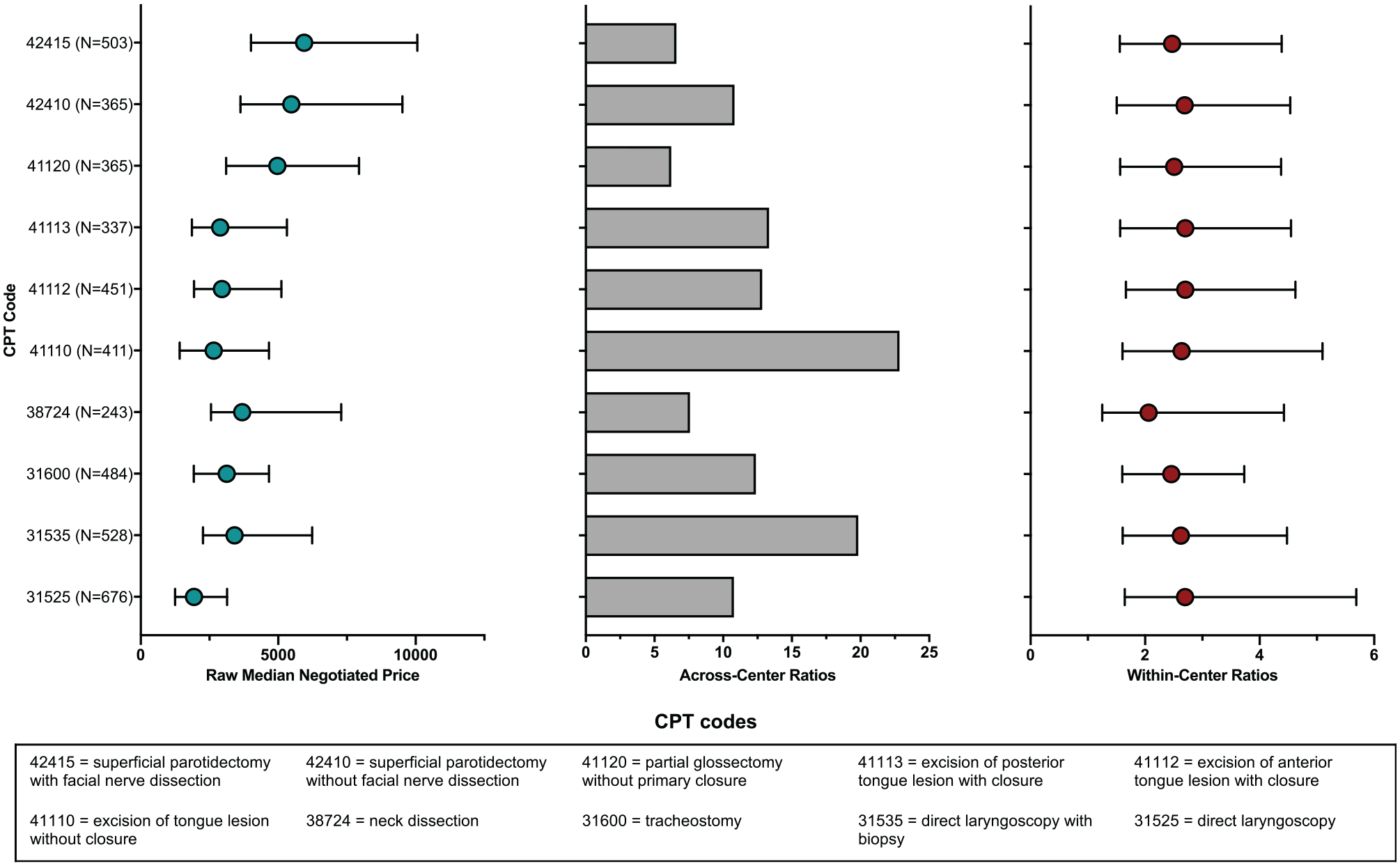
Variation in the price of head and neck surgical oncology procedures. Raw median negotiated prices and within-center ratios are represented by medians (points) and interquartile ranges (error bars).
Hospital ownership structure (for-profit vs nonprofit) and geographic region were frequently associated with differences in median procedure prices ( Figure 2 ). When compared with nonprofit hospitals, for-profit hospitals had significantly higher median prices for direct laryngoscopy with biopsy ($5215 vs $3132, P < .001) or without ($2613 vs $1817, P < .001), tongue excision without closure ($3212 vs $2567, P < .001), tongue lesion excision with closure (anterior, $3799 vs $2763, P < .001; posterior, $3353 vs $2735, P < .001), and parotidectomy with nerve dissection ($6489 vs $5707; Supplemental Table S1, available online). The proportional difference was greatest for direct laryngoscopy with biopsy, for which the median for-profit price of $5215 was 67% greater than the mean nonprofit price of $3132. Median prices were significantly lower at hospitals in the northeastern region vs all other regions for all procedures except for neck dissection (Supplemental Table S2). For example, the median price of tracheostomy was $2614 in the northeast and $3301 in other regions (P < .001).
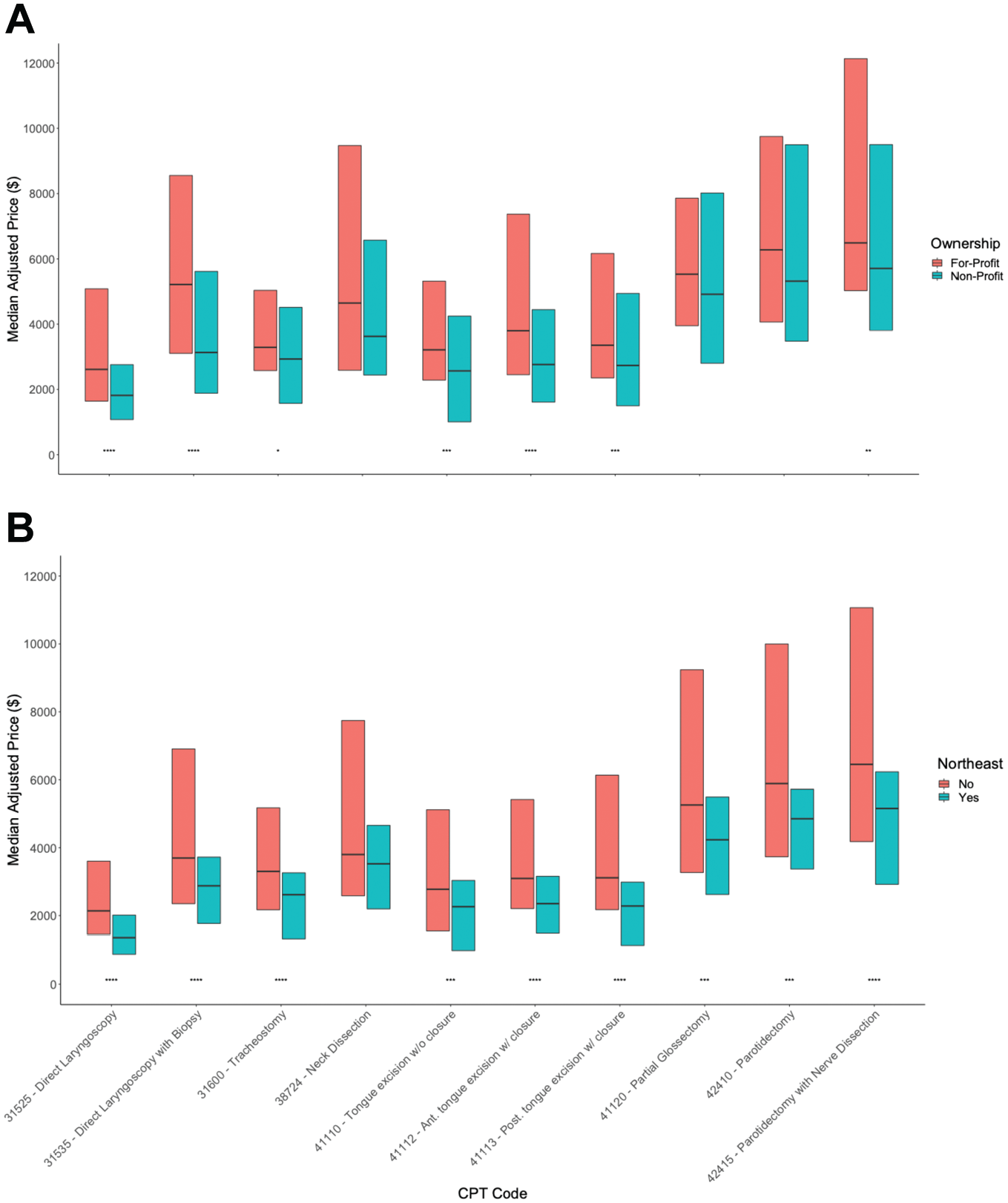
Differences in median price for head and neck surgical procedures by (A) hospital ownership and (B) geographic region. Lines represent medians, and boxes represent interquartile range. Wilcoxon rank sum tests were used. *P≤ .05. **P≤ .01. ***P≤ .001. ****P≤ .0001.
Discussion
In this study, we found wide variations in negotiated surgical prices across hospitals and within hospitals among payers. Variations in procedure prices have been reported previously,3,7 and explanations have included differences in case complexity and care quality. For certain procedures, differences in equipment, such as intraoperative nerve monitoring for parotidectomy, may contribute to price differences. However, as shown in this study, even for procedures such as direct laryngoscopy, for which there is little variation in equipment or outcomes, there can be substantial price variations.
In this study, for-profit ownership structure was strongly associated with higher negotiated prices. It is possible that due to their for-profit nature, these hospitals negotiate higher prices to maximize revenue.10-12 Although we observed higher prices at for-profit hospitals, prior work does not suggest that patient outcomes are better at these hospitals. 13 Geographic region within the northeast was also associated with lower prices in this study, which may have implications for patients who are contemplating traveling for care.
This study has limitations. Analyses were restricted to facility fees and likely underestimate the total prices for surgical care episodes, which include professional services. Additionally, it is possible that some hospitals may choose to not disclose prices for high-price procedures, which could introduce a selection bias. Nevertheless, this study highlights the extent to which overall price variability may be due to market forces, as opposed to differences in clinical care. In seeking to make financially informed decisions, patients may consider hospital ownership structure and location as important factors in price determination. Future studies comparing clinical outcomes, market competition, and prices are needed.
Supplemental Material
sj-docx-1-oto-10.1177_01945998221104664 – Supplemental material for Variation in the Price of Head and Neck Surgical Oncology Procedures
Supplemental material, sj-docx-1-oto-10.1177_01945998221104664 for Variation in the Price of Head and Neck Surgical Oncology Procedures by Michael Pei-hong Wu, Roy Xiao, Vinay K. Rathi and Rosh K.V. Sethi in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
This work was financially supported by a research grant from the Centers of Expertise at Mass General Brigham.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.