
Abstract
Objective
To determine risk factors for surgical site infection (SSI) after cochlear implantation (CI) in pediatric patients.
Study Design
Case-control study.
Setting
A total of 150 hospitals contributing data to the ACS-NSQIP Pediatric database (American College of Surgeons National Surgical Quality Improvement Program) in North America and worldwide.
Methods
Pediatric patients (aged <18 years) undergoing CI during the years 2012 to 2017 were identified in the ACS-NSQIP Pediatric database. Uni- and multivariable logistic regression analyses were used to determine the odds ratios (ORs) of SSI (including superficial incisional, deep incisional, organ/space) occurring up to 30 days postoperatively.
Results
A total of 79 SSIs occurred over a 5-year period (n = 5146). Longer operative time significantly increased the odds of SSI (OR, 1.965; 95% CI, 1.205-3.289). Younger age was also found to raise the odds of SSI, with decreased odds associated with each 6-month increase in age (OR, 0.887; 95% CI, 0.814-0.958).
Conclusion
Longer operative time and younger age appear to significantly increase the odds of SSI in pediatric CI. Body mass index, recent steroid use, American Society of Anesthesiologists class, bilateral vs unilateral implantation, and hospital length of stay do not appear to significantly influence SSI risk. These findings must be interpreted in the context of the limitations inherent to adverse events reporting, which are mitigated by the stringent manner of data collection by the ACS-NSQIP, and those inherent to the definition of SSI. Future prospective studies should investigate the impact of reducing operative time on the risk of SSI and other complications in pediatric CI.
There is good evidence that cochlear implantation (CI) improves language development and educational outcomes in children with congenital or early-onset severe to profound hearing loss.1-5 Implant candidacy in children continues to expand as the benefits of early intervention are increasingly recognized. 6 In the United States, CI is currently approved for children aged ≥9 months. 7
Surgical site infection (SSI) following CI is an uncommon but potentially devastating complication.8,9 Potential downstream effects of SSI in the setting of CI include feared complications such as the need for device removal, meningitis, and labyrinthitis ossificans. Each of these represents a preventable source of patient morbidity and possibly significant health care spending. Additionally, it has been shown that the need for reimplantation following device removal (related to infection or other causes) is associated with poorer speech development. 10 In large groups of pediatric CI recipients, the incidence of postoperative SSI reported in the literature ranges from 0% to 8.5%.9,11-19 In series of pediatric CI requiring removal and reimplantation, SSI accounted for 7% to 23% of cases.20-22
Few studies have been performed that aimed to identify risk factors for SSI in pediatric CI, likely in part due to the rarity of the event. A recent retrospective cohort study of 246 pediatric CIs found significant differences in age and operative time between CI recipients with and without SSI (which occurred at an overall rate of 6.5%). A variety of other studied factors, such as use of prophylactic antibiotics, were not significantly associated with infection risk. 18 Debate exists regarding whether the development of acute otitis media (AOM) places a child at increased risk of SSI following CI. In one series of 421 implanted children, 18% of ears experienced AOM, of which 2.8% extended to the implant site, necessitating device explantation in 37.5% of these cases. 15 This study did not assess whether AOM was a significant risk factor for SSI. There is similarly a scarcity of large-scale population-based studies characterizing risks of developing SSI in pediatric CI.
The purpose of the present study was to identify risk factors for SSI following pediatric CI. Elucidation of these risk factors could provide an opportunity for surgical quality improvement, if modifiable risk factors are identified, or allow for improved postoperative risk prognostication in pediatric CI surgery.
Methods
A retrospective case-control study was designed with data from the ACS-NSQIP Pediatric database (American College of Surgeons National Surgical Quality Improvement Program). In total, 150 pediatric hospitals contribute data to the database, principally in North America (United States and Canada) but also in Asia (Qatar, United Arab Emirates) and Australia. 23 The ACS-NSQIP Pediatric database trains surgical clinical reviewers to collect data from participating hospitals pertaining to demographic, surgical, preoperative, intraoperative, and 30-day postoperative variables. Access was granted to ACS-NSQIP data through a data use agreement for the purposes of this study. The study was approved by our institutional Research Ethics Board (Children’s Hospital of Eastern Ontario, protocol 19/119X).
The study population was defined as pediatric patients (age <18 years) who underwent unilateral or bilateral CI, identified with the Current Procedural Terminology code 69930. All procedures were performed during the years 2012 to 2017 inclusive. During these years, the number of hospitals contributing data ranged from 50 to 109. Procedures were excluded that had operative time values ranging from 0 to 45 minutes (indicating that the procedure may have been aborted) or >10 hours. Patients with age values <9 months at the time of the procedure were also excluded on the basis of missing data.
The outcome of interest, SSI, was operationally defined as any of 3 types of postoperative infection on which data are collected by ACS-NSQIP: superficial incisional, deep incisional, and organ/space. Wound dehiscence alone was not considered as SSI; however, if it co-occurred with any of the 3 types of SSI, 2 events were counted at the patient level. Data on each of these variables are available up to 30 days postoperatively. From these, a composite binary variable was created (SSI, yes/no). Due to the small numbers of outcome events, subgroup analyses examining the subcategories of SSI in our definition were not performed.
Multivariable logistic regression analysis was used to identify potential risk factors for the outcome of interest while controlling for potentially confounding factors. Given a small number of outcome events, we employed the commonly cited rule of 10 events per variable to avoid model overfitting. 24 Variables chosen for model inclusion were based on clinical reasoning as well as previous literature on the subject. Odds ratios (ORs) were reported with 95% CIs.
The following variables were chosen for inclusion in multivariable analysis: body mass index (BMI), 25 a derived continuous variable defined as weight/height 2 (kg/m2); age, a categorical variable of increasing 6-month increments; duration of operation, a binary variable defined as greater or less than the median value of 143 minutes; steroid use within 30 days, a binary variable (yes/no); bilateral vs unilateral implantation, a binary variable; hospital length of stay (LOS), a continuous variable measured in days; and American Society of Anesthesiologists (ASA) class, a categorical variable defined as no disturbance, mild disturbance, or severe/life-threatening disturbance. 26 Steroid use within 30 days is defined by the ACS-NSQIP Pediatric database as follows: “Patient has required the administration of oral or parenteral corticosteroid medication in the 30 days prior to surgery and includes patients who receive short course oral or IV steroids. Corticosteroids applied topically or administered rectally or by inhalation are not included.” 27 The median operative time was chosen as a cut point given a left skew of the data. Sensitivity analysis was performed to assess the impact of modeling operative time as a continuous variable, in which each 1-unit increase represented 1 hour of additional operative time. Operative times were summarized across groups of bilateral and unilateral CI with and without SSI (SSI+ and SSI–) by medians and interquartile ranges (IQRs).
Where there were missing values pertaining to model variables, data were imputed with multiple imputation. Data for all variables were complete except for LOS, which was missing in 0.2% (n = 8), and BMI, which was incomplete (based on missing height, weight, or both) in 40.3% of patients (n = 2073). BMI was imputed based on age, sex, and, where possible, a polynomial of either height or weight. Patients missing LOS were excluded from the model.
All statistical analysis was performed with R version 3.6.3 (R Foundation for Statistical Computing).
Results
A total of 5146 pediatric CI procedures were identified in the ACS-NSQIP Pediatric database as having been performed over 2012 to 2017. Of these, there were 79 incidences of SSI (1.54%). The minimum age of patients in the study was 9 months in the SSI+ and SSI– groups. Demographic and clinical variables of the study population are summarized in Table 1 .
Cohort Demographics and Clinical Predictors.
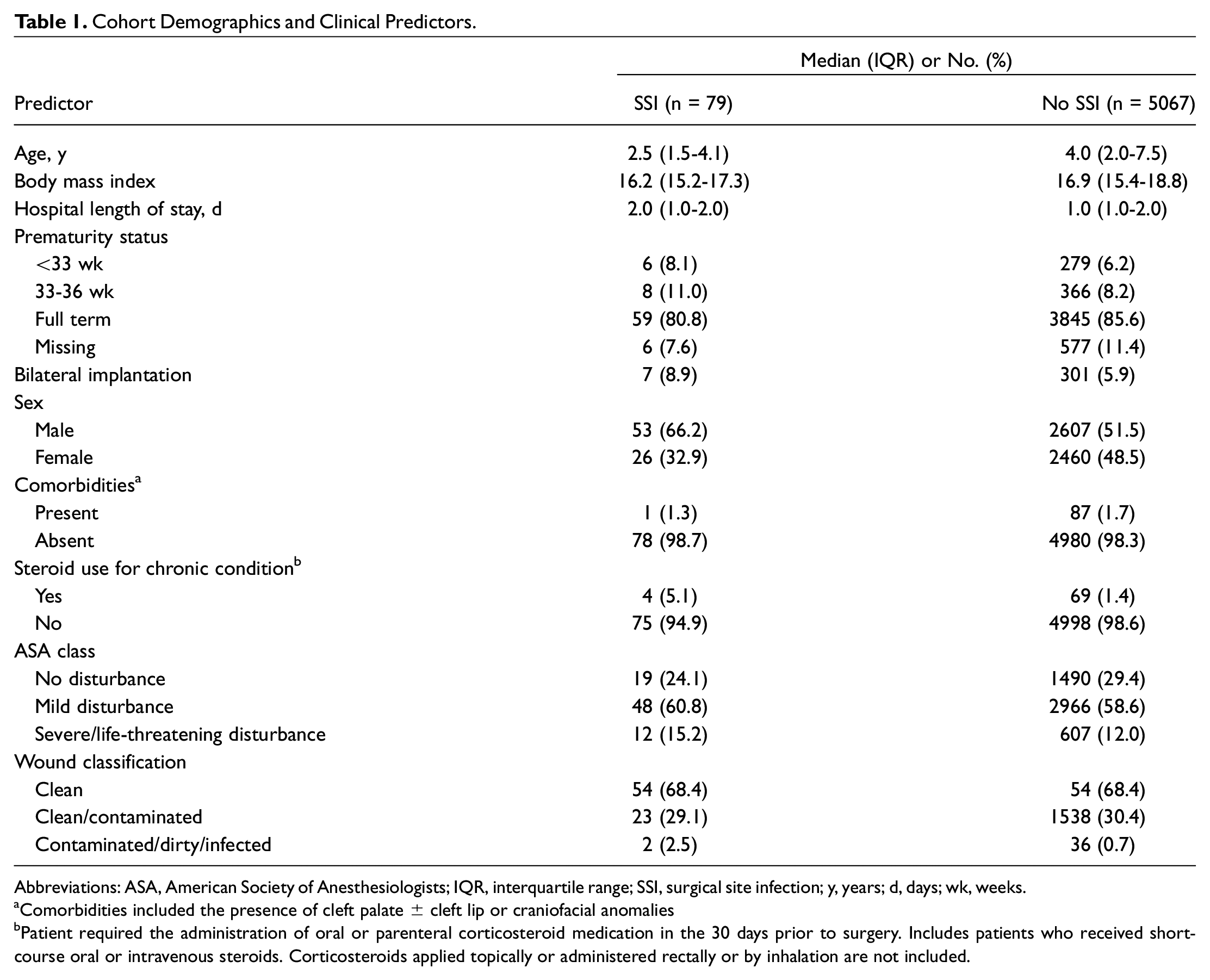
Abbreviations: ASA, American Society of Anesthesiologists; IQR, interquartile range; SSI, surgical site infection; y, years; d, days; wk, weeks.
Comorbidities included the presence of cleft palate ± cleft lip or craniofacial anomalies
Patient required the administration of oral or parenteral corticosteroid medication in the 30 days prior to surgery. Includes patients who received short-course oral or intravenous steroids. Corticosteroids applied topically or administered rectally or by inhalation are not included.
Of the variables assessed, operative duration and age were significantly related to the odds of SSI. Operative duration ≥143 minutes (2.4 hours) was associated with increased odds of SSI (OR, 1.965; 95% CI, 1.205-3.289). Among 2459 cases with operative durations <2.4 hours, there were 23 instances of SSI (infection prevalence, 0.94%); for cases with operative duration ≥2.4 hours (n = 2638), there were 55 instances of SSI (infection prevalence 2.08%). When operative duration was modeled as a continuous variable, its relationship with SSI remained significant, with each 1-hour increase in duration raising the odds of SSI (OR, 1.246; 95% CI, 1.072-1.435). Younger age at the time of the procedure was also associated with higher odds of SSI, with each 6-month increased in age associated with a decrease in odds of SSI (OR, 0.887; 95% CI, 0.814-0.958). Figure 1 depicts the prevalence of SSI for each integer of age and the relationship between these variables. Figure 2 depicts the distribution of operative times in the SSI+ and SSI− groups.
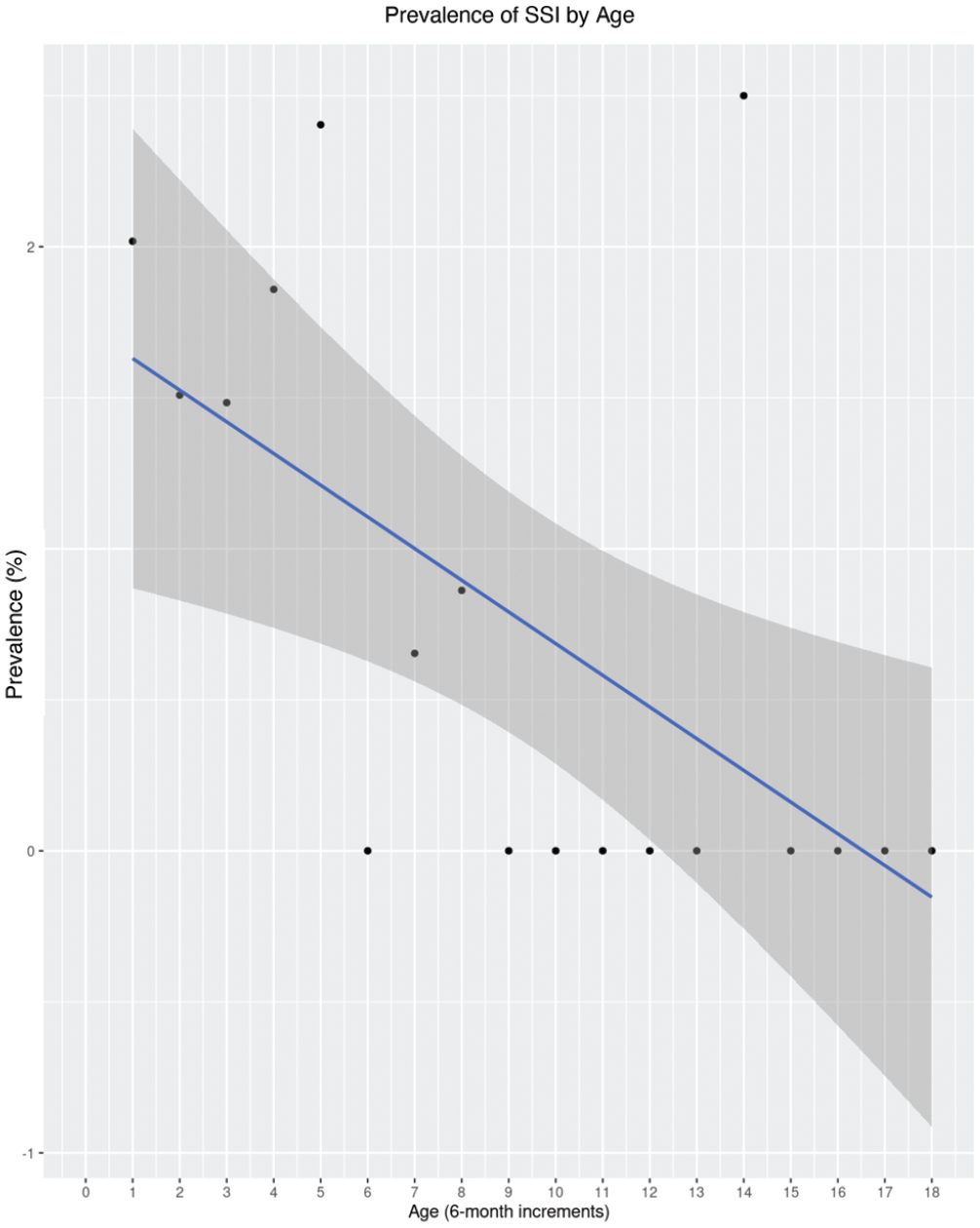
Histogram with fitted regression line and 95% CI (shaded area) depicts the association between age and SSI prevalence. Age is modeled as a continuous variable with units of 6-month increments. SSI, surgical site infection.
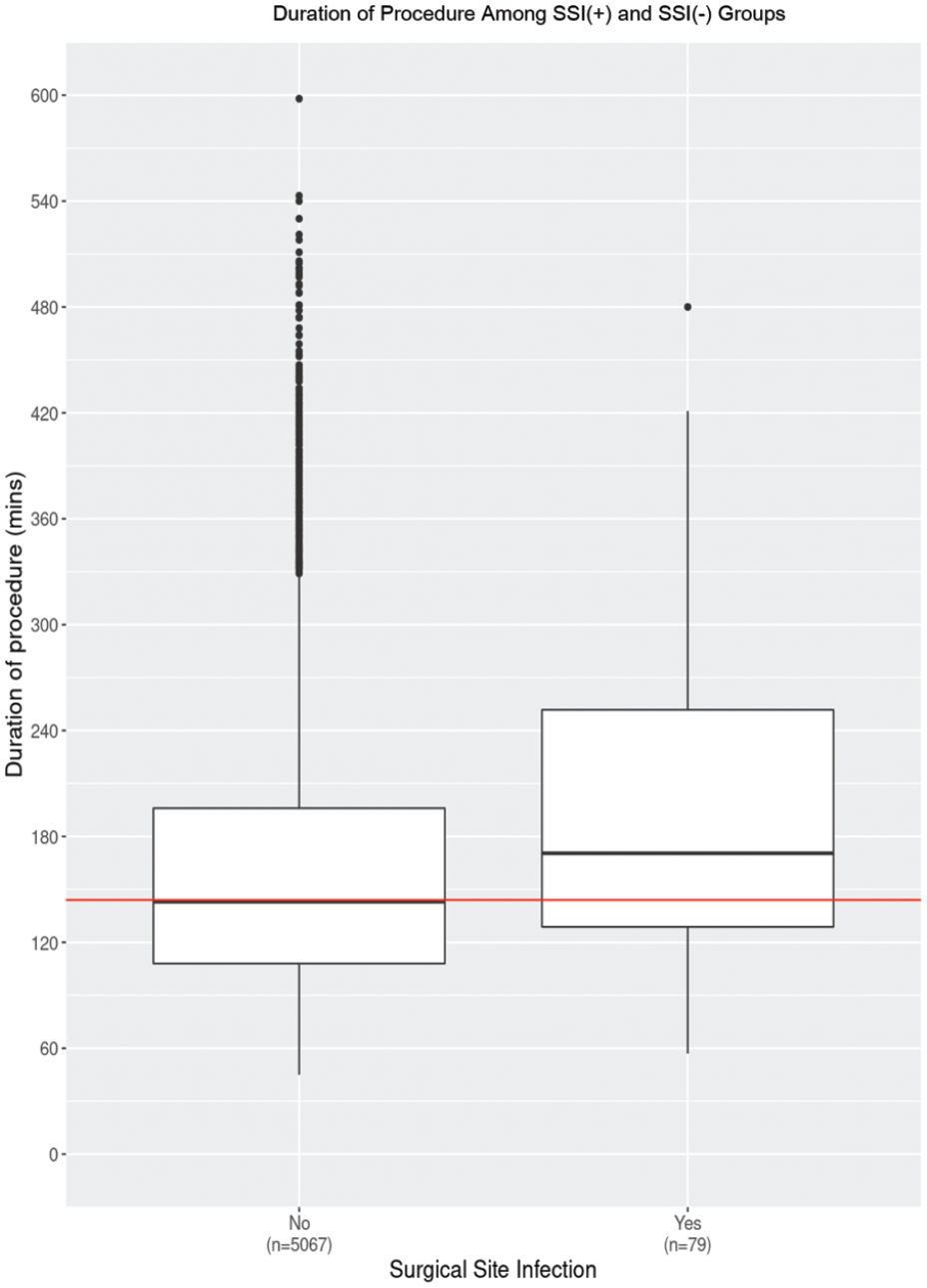
Box and whiskers plot shows the distribution of operative times in the SSI+ and SSI– groups. Boxes represent the median (line) and 25th and 75th percentiles in each group; dots represent individuals. Red horizontal line signifies the median operative time across both groups. SSI, surgical site infection.
Steroid use in the past 30 days, BMI, bilateral vs unilateral implantation, increased hospital LOS, and higher ASA class were not significantly associated with the odds of postoperative SSI. Median operative times in terms of unilateral/bilateral implantation and presence/absence of SSI were as follows: bilateral CI and SSI+, 4.8 hours (IQR, 4.0-6.1); bilateral CI and SSI–, 4.0 hours (IQR, 3.2-5.1); unilateral CI and SSI+, 2.7 hours (IQR, 2.1-4.1); and unilateral CI and SSI–, 2.3 hours (IQR, 1.8-3.1).
Table 2 and Figure 3 demonstrate results of the multivariable model.
Multivariable Model of Predictors of Surgical Site Infection.
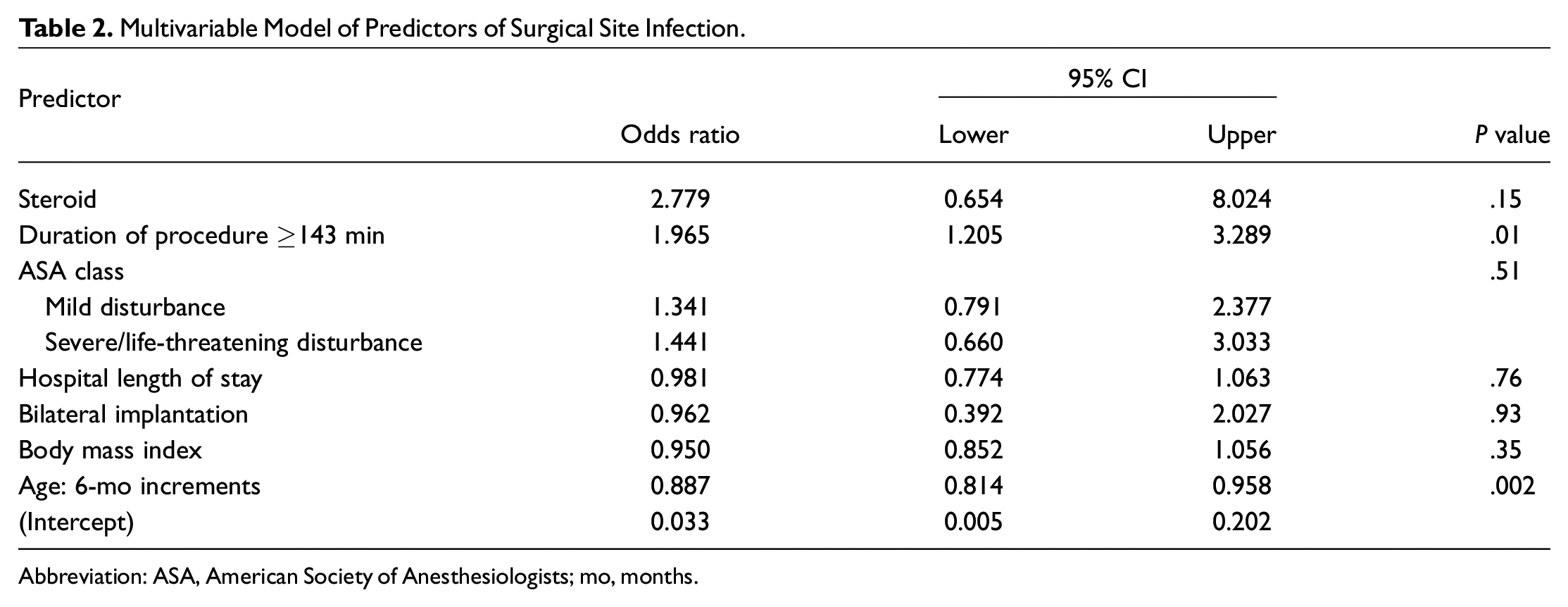
Abbreviation: ASA, American Society of Anesthesiologists; mo, months.
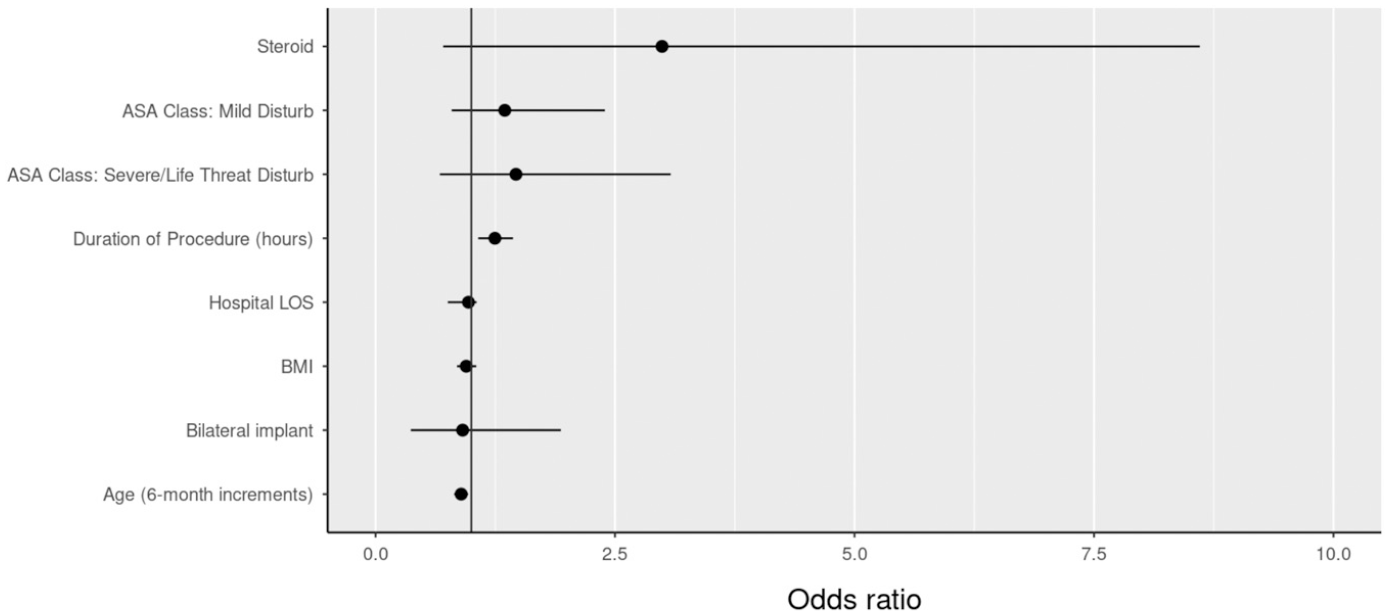
Forest plot demonstrating results of the multivariable model. Values are presented as odds ratio and 95% CI. Vertical line represents no effect (odds ratio = 1). ASA, American Society of Anesthesiologists; BMI, body mass index; disturb, disturbance; LOS, length of stay; steroid, steroid treatment within 30 days.
Discussion
Despite the infrequent occurrence of SSI in CI surgery, potentially devastating consequences as they pertain to patient morbidity make elucidating risk factors an important goal in health care quality improvement. Few studies have been performed to this end within the context of pediatric CI.
By virtue of using international data from the ACS-NSQIP, the present study represents to the best of our knowledge the largest sample of pediatric CI in the published literature. The identified SSI incidence of 1.55% over a 5-year study period is consistent with other literature in this population.9,11-19
Given the small number of cases of SSI, we were limited in our ability to assess a large number of risk factors without the attendant risk of model overfitting. This study focused on assessing the correlation of a small number of clinical variables with SSI occurrence. Consistent with previous literature on the topic, we found that longer operative time was significantly associated with higher odds of SSI occurrence whether modeled as a binary variable with the median operative time used as a cut point (OR, 1.965 [95% CI, 1.205-3.289] for ≥143 vs <143 minutes) or as a continuous variable based on 1-hour increments in operative duration (OR, 1.246 [95% CI, 1.07-1.435] for each 1-hour increase).18,28 That operative duration significantly raised the odds of SSI when operationalized as either a binary or a continuous variable strengthens our assertion that longer operative time leads to greater odds of SSI. Factors that may lengthen operative time include the presence of inner ear deformities or other anatomic abnormalities that present a challenge to the surgeon, and variations in technique among surgeons, such as the creation of a well vs a tight pocket for implant placement. These factors are unlikely to be confounding variables, however, as they would not be suspected to inherently heighten the risk of SSI. If less secure implant placement is a factor contributing to decreased operative time in some cases, we would anticipate that any potential downstream effects (ie, wound dehiscence possibly leading to SSI) would bias our results toward rather than away from the null hypothesis. Simultaneous bilateral implantation would also lengthen operative time, but the effect of longer operative time on SSI odds persisted even after controlling for bilateral vs unilateral implantation in adjusted analyses. Other potential unmeasured confounders of the relationship between operative time and odds of SSI are surgeon experience, and involvement of residents/trainees in the operative case. While these variables were not measurable within the constraints of our data source, each might be a true confounder of this relationship, and warrant further consideration in the context of surgical quality improvement initiatives. We avoided the determination of an optimal cut point for operative time for use in our model, as this approach has been demonstrated to produce biased measures of association. 29 Future studies might provide insight into a more specific cut point above which longer operative time leads to increased SSI risk.
We found that younger age at the time of CI is associated with a higher risk of SSI, with increasing age (measured in 6-month increments) carrying a decreased odds of SSI (OR, 0.887; 95% CI, 0.814-0.958). This finding expands on previous literature showing that patients aged <5 years are at increased risk of SSI following CI.18,28 Certainly, the clinical significance of this finding must be taken into consideration, especially balanced against the numerous studies demonstrating benefits of early pediatric CI on language acquisition and development. Other studied variables—ASA class, BMI, bilateral vs unilateral implantation, hospital LOS, and steroid use—did not statistically significantly increase the odds of SSI. Overall, the hospital LOS for all patients in the study was very short (IQR, 1.0-2.0 in both outcome groups), which limits our ability to detect whether longer postoperative stays may be associated with higher risk of SSI.
The generalizability of our findings is somewhat limited by the definition of SSI that we adopted as necessitated by the variables available in the ACS-NSQIP. Specifically, to best capture all events of SSI, we chose to amalgamate the variables of superficial incisional, deep incisional, and organ/space SSI. If wound dehiscence occurred in the presence of SSI, it was additionally counted as an event. Given an overall small number of outcome events (n = 79 occurrences of SSI by this definition among 5146 cases of pediatric CI), subgroup analysis by type of SSI was not performed. It is possible that by our definition, some events considered by other authors to represent SSI (eg, AOM) would not have been captured. 15 As previously discussed, it has not been conclusively demonstrated whether AOM should be included in the definition of SSI nor whether the development of AOM predisposes to more extensive SSI with downstream consequences such as device removal. 30 In the previously cited study, the median duration to the first occurrence of AOM post-CI was 6 months; data captured by the ACS-NSQIP extend only to 30 days postoperatively. 15 Studies have also documented the occurrence of SSI up to 263 days post-CI (mean 83 days), highlighting the limitation of this time frame of data availability. 18 We were not able to capture data on the presence or absence of ventilation tubes at the time of surgery and whether these affected the occurrence of SSI. However, a previous large study did not show any increased risk of SSI associated with the presence of ventilation tubes at the time of CI. 14 We did not capture data pertaining to the use of prophylactic antibiotics; while it is common at many institutions for single or multiple intraoperative doses of antibiotics to be given at the time of CI, previous study has not demonstrated any benefit to prolonged prophylactic antibiotics in preventing SSI in pediatric CI.16,18 We did not include comprehensive information on patient comorbidities in our model, which may also affect the risk of SSI. We instead attempted to represent this information through the inclusion of ASA class in the model. However, there is some evidence that the application of ASA classes to pediatric patients has low reliability, raising the possibility of misclassification bias through use of this variable.31,32 There was a lack of data on patient BMI in a large percentage of cases (40.3%), so values were imputed based on age, sex, and a polynomial of either weight or height where possible. This methodology limits our ability to properly assess the relationship between BMI and odds of SSI, and to fully control for any potential confounding effects of BMI through our multivariable modeling. We excluded cases with operative duration <45 minutes based on there being no way to ascertain whether these cases of shorter duration were completed (ie, an implant was placed) or were aborted cases not truly representative of our population of interest. While it is possible that CI may be safely performed in <45 minutes in some cases, we selected this cut point conservatively to ensure construct validity.
Another limitation of this study is the potential for reporting bias. It has been demonstrated that surgeons may be prone to underreporting their complications. 33 An externally recorded data registry such as the ACS-NSQIP likely alleviates much of this bias. The ACS-NSQIP, including the ACS-NSQIP Pediatric database, adheres to a high standard of data collection. 34 Surgical clinical reviewers external to the institution are trained to capture postoperative data from patient medical charts, both inpatient and outpatient, relating to the initial surgical encounter and any other health care encounters, - including readmission -within 30 days of the index surgical procedure. 35 In addition to record audits, clinical reviewers perform telephone calls to providers and/or patients to ascertain the presence or absence of SSI postoperatively. Participating hospitals are also audited to ensure completeness and accuracy of the data they contribute to the ACS-NSQIP. Studies have shown the ACS-NSQIP to be of high quality and capture a greater number of adverse events than other population-based databases. 36
The identification of operative time as a significant risk factor for the development of SSI in pediatric CI has implications for clinical practice. If additional studies are able to confirm a causal link between operative time and odds of SSI, then surgeon and institutional initiatives to reduce operative time might result in decreased SSI rates. In this case, it would be important to verify that the rates of other surgical complications—for example, incomplete electrode insertion or implant displacement—are not increased by attempts to shorten operative time. Further research into other unmeasured factors affecting operative time, such as surgeon experience and efficiency, could help to better inform quality improvement initiatives, including formal recommendations and guidelines, aimed at reducing infection rates following pediatric CI. A comprehensive, prospective study would be well suited to address this question.