
Abstract
Immigrant health research demonstrates that foreign-born individuals generally experience lower morbidity rates relative to native-born individuals. However, this research often overlooks structural factors that influence the immigrant experience, such as legal status. The present study examines legal status as a multidimensional and dynamic characteristic that shapes immigrant health over time. I use two waves of the New Immigrant Survey (n = 3550) to assess if three dimensions of legal status — initial documentation classification, legal permanent residence (LPR) admission category, and US citizenship — predict likelihoods of reporting a chronic condition among a sample of immigrants who attained LPR. Results indicate that each of the three dimensions of legal status predicted health. Immigrants who obtained US citizenship improved their relative health over time, while immigrants with previous temporarily documented, undocumented, legalization, or refugee experience exhibited persistent disadvantage in the hierarchy of immigrant health. Findings demonstrate that the sociopolitical context continually shapes the physical health of immigrants, and a dynamic and multidimensional conceptualization of legal status can expose previously obscured disparities in the overarching pattern of an immigrant health advantage.
The structural forces that stratify the immigrant population into a hierarchy of privilege are critically understudied (Bacong and Menjívar 2021). Instead, existing immigrant health research tends to focus on the nativity component of immigration status and individual-level or community-level explanations for observed outcomes. In this literature, researchers have established that foreign-born individuals tend to be in better health than their native-born counterparts (e.g., Cunningham, Ruben and Venkat Narayan 2008). This immigrant health advantage is largely explained by self-selection of healthier individuals into migration (Landale, Gorman and Oropesa 2006; Riosmena, Kuhn and Jochem 2017), cultural influences such as dietary habits and strong social networks (Eschbach et al. 2004; Riosmena, Kuhn and Jochem 2017), and data quality issues (Patel et al. 2004; Turra and Elo 2008). Yet, the immigrant health advantage is not universal; disparities in health exist among foreign-born populations by country of origin, race/ethnicity, and over time (Angel, Buckley and Sakamoto 2001; Singh and Siahpush 2002; Jasso et al. 2004; Cunningham, Ruben and Venkat Narayan 2008; Gubernskaya, Bean and van Hook 2013; Boen and Hummer 2019). The present study advances this body of work by demonstrating how a nuanced examination of the legal components of immigration status can uncover further disparities in immigrant health.
Immigration status is a broad term that encompasses various interconnected factors such as nativity, duration of residence, documentation status, visa category, and citizenship (De Genova 2002; Durden 2007). Some aspects of immigration status, such as documentation status, visa category, and citizenship are products of US laws and regulations generating notions of migrant illegality and belongingness (Ngai 2004; Donato and Armenta 2011). Therefore, I employ the term “legal status” to represent the three structural components of immigration status that I assess in this article: initial documentation classification, legal permanent residence (LPR) admission category, and current US citizenship. Initial documentation classification refers to the legal right of an individual to live and work in the United States. LPR admission category is defined as the criteria through which an individual is eligible for their green card, or LPR visa. Lastly, US citizenship signifies the completion of the naturalization process to become a US citizen. This conceptualization of legal status is both multifaceted and longitudinal, spanning an immigrant's point of entry into the United States (initial documentation classification), transition into permanent residency (LPR admission category), and current position (US citizenship).
Legal status stratifies immigrants into a hierarchy of privilege, with differential rights and access to resources (Bean et al. 2011; Yoshikawa 2011; Torres and Young 2016; Patler 2018). Although the specific categories vary somewhat across national contexts, research demonstrates that stratification based upon legal status prevails across the globe (Oxman-Martinez et al. 2005; Silove et al. 2006; Larchanché 2012; Flaim, Williams and Ahlquist 2020). At one end of the spectrum are undocumented immigrants, who are legally denied the right to reside in the United States, access the labor market, and utilize most social services. Undocumented status is therefore associated with fewer health-promoting resources such as health insurance and greater health-eroding exposures such as deportation stress. Temporarily documented immigrants occupy a liminal space in the hierarchy of legal status privilege—their right to reside in the United States is protected for a specified amount of time but most are not permitted to work, which limits their ability to forge enduring social connections and access healthcare. Permanent documentation is a more protected status since it confers the right to live in the United States indefinitely, as well as the ability to legally participate in the labor market and, after a waiting period, obtain social services like Medicaid. Individuals can obtain LPR status by meeting various criteria, such as family, employment, and refugee criteria, which reflect their social ties and resources. Despite being eligible for US citizenship after 5 years, many immigrants (approximately 9.2 million) choose to remain LPRs rather than apply to complete the naturalization process (Baker 2019), possibly due to language barriers, financial burdens, or perceived lack of necessity or advantage. Nevertheless, US citizenship confers privileges above and beyond LPR status, including greater civic and social integration, higher income, better health insurance coverage, and protection from deportation, all factors associated with well-being.
However, the impact of legal status on health is underexplored, in part due to data limitations stemming from the difficulty of asking such sensitive information on surveys. Existing studies demonstrate that legal status predicts self-rated and mental health (Martinez et al. 2015), but scant research examines the effects of legal status on physical health outcomes (Hamilton, Hale and Savinar 2019). In addition, extant literature typically frames legal status as a static or binary characteristic through the examination of differences between documented/undocumented or US citizen/noncitizen immigrants. These dualistic frameworks overlook immigrants with “liminal legality” — those with the privileges related to being authorized as well as the disadvantages associated with being non-US citizens (Menjívar 2006). In general, immigrant health scholarship is limited by its focus on the nativity component of immigration status and incomplete conceptualizations of legal status, when considered.
The present study evaluates if legal status shapes the physical health trajectories of US immigrants. I argue that conceptualizing legal status as a multidimensional and dynamic characteristic can help to illuminate hidden immigrant health disparities. I utilize the New Immigrant Survey (NIS), a longitudinal survey of lawful permanent residents in the United States, to assess the association between three dimensions of legal status — initial documentation classification, LPR admission category, and US citizenship — and physical health outcomes. Because these institutional categorizations can vary over time as individuals navigate the immigration system (Torres and Young 2016), I draw upon concepts from the life course perspective to frame my study. Results indicate that each of the three dimensions of legal status predict health. Immigrants who obtained US citizenship improved their relative health over time, while immigrants with previous temporarily documented, undocumented, legalization, or refugee experience exhibited persistent disadvantage in the hierarchy of immigrant health. These findings demonstrate that the sociopolitical context, through legal status, continually shapes the physical health of immigrants. The current research also contributes to existing literature by illustrating how the conceptualization of legal status as a dynamic and multidimensional social determinant of health, rather than as a static or binary characteristic, exposes disparities in the overarching pattern of an immigrant health advantage.
Background
Dimensions of Legal Status
Initial documentation classification
The term documentation classification signifies the legal right of an individual to reside in the United States and reflects the lawful aspect of legal status. While investigations of documentation classification beyond the documented/undocumented binary are exceedingly rare, existing research proposes that unauthorized legal status is disadvantageous for health. The stress of being undocumented impacts social relationships, generates economic uncertainty, and provokes deportation fears when receiving medical care or other social services (Berk and Schur 2001; Hacker et al. 2015; García 2018), which can lead to adverse mental health outcomes like depression (Yoshikawa 2011; Martinez et al. 2015). Still, empirical research on the impact of documentation classification on physical health is inconsistent. Compared to documented status and/or US citizenship, undocumented status has variably been associated with both adverse (Reed et al. 2005; Young and Pebley 2017) and advantaged (Reed et al. 2005; Lu and Li 2020) physical and self-rated health outcomes. Moreover, one systematic review demonstrates that most studies (71 percent) fail to find a significant difference between the health of documented and undocumented immigrants (Hamilton, Hale and Savinar 2019).
The relationship between documentation status and physical health may be ambiguous for several reasons. As Hamilton, Hale and Savinar’s (2019) recent systematic review reveals, studies on documentation classification typically use small and/or nonrandom samples or rely on indirect methods of categorization due to the sensitivity of the subject matter, although there are some recent exceptions using state-level (Bacong and Sohn 2021) and farmworker samples (Hamilton, Hale and Savinar 2019) as well as innovative imputation techniques (Capps, Bachmeier and Van Hook 2018). In addition, it may be that documentation status, and the mechanisms linking documentation status to health, have notable effects on some health outcomes but not others. The lack of consistent evidence connecting documentation status to physical health may also be due to the utilization of conceptions of legal status that do not reflect the reality of many immigrants’ experiences. Extant studies rely on a binary categorization of documentation classification even though it is often not a static characteristic. Many immigrants are undocumented before acquiring temporary or permanent legal status (Jasso et al. 2008; Gonzales, Terriquez and Ruszczyk 2014). Others enter the country with valid documentation but fall into unauthorized status once their visa expires (CBP 2021). The stress of being unauthorized, even briefly, may have enduring mental and physical health effects (Cavazos-Rehg, Zayas and Spitznagel 2007; Martinez et al. 2015; Torres and Young 2016). Further disparities may emerge for individuals with temporary documentation given the stressors associated with having tenuous claims to a legal future in the United States. Therefore, documentation classification likely shapes immigrants’ health trajectories, but further research is needed to disentangle this relationship.
LPR admission category
In this article, LPR admission category refers to the criteria through which individuals were eligible for their green cards, or LPR visas. Most non-US citizens need a visa to legally enter the country. Some of these visas confer LPR status, but the majority of individuals enter the country with nonimmigrant visas that are either temporary or conditional, such as a student or tourist visa. Others enter the United States without a visa, and thus without documentation, but later acquire a residence visa. In order to obtain an LPR visa, then, an individual must meet certain eligibility requirements. These criteria align with the major categories of entry immigrant visas (e.g., family preference, employment, and refugee), but their eligibility may be demonstrated after an individual already resides in the United States, rather than before, as is the case for entry visas. For example, an individual may enter the country with a student visa, but later receive an LPR visa through employment criteria. If one were to measure visa status based on their entry visa, this individual would be classified as a visiting student; yet, their transition into a new visa category while residing in the United States indicates that they would be better classified as an employment immigrant. Therefore, by assessing visa status as LPR admission category, I am able to capture a unique element of legal status beyond documentation classification, especially for individuals who entered the country with nonimmigrant visas or no visa.
The present study includes immigrants who were eligible for LPR visas through family preference, employment, refugee, legalization, and diversity criteria. In order to meet these various classifications, immigrants must have different resources at their disposal. Family preference eligibility criteria require an immigrant to have a US citizen or green card-holding family member already in the United States with an income at least 125 percent above the poverty line (USCIS 2020). Family preference immigrants subsequently have strong social connections with moderate financial resources (Kreisberg 2019). Employment eligibility criteria require an employer sponsor, which often necessitates a high level of education (Kreisberg 2019; USCIS 2020). Employment immigrants therefore experience better labor market integration compared to other visa holders (Kreisberg 2019), which facilitates access to health-promoting resources such as health insurance. Refugee status is available to individuals who the US government acknowledges face serious danger in their country of origin (Office of Refugee Resettlement 2020). Refugees often lack the social and economic resources of family preference and employment immigrants (Kreisberg 2019) but are entitled to state services that provide social welfare, employment counselors, and English language classes for two years (Office of Refugee Resettlement 2019). Eligibility for LPR status through legalization criteria is available to unauthorized immigrants who meet certain length of residence qualifications and other policy criteria such as cancellation-of-removal (Jasso 2011). Lastly, diversity criteria are accessible to a restricted number of individuals with at least a high school degree or its equivalent from countries with low levels of historical migration (US Department of State n.d.). Like refugees, diversity immigrants often do not have the strong social ties of family preference and employment immigrants (Kreisberg 2019), but they have some financial resources due to the costs of the diversity program (Logan and Thomas 2012).
LPR admission categories indicate prior life chances and accessibility of resources associated with health. For example, previous research demonstrates that immigrants who are eligible for LPR status through family preference and refugee criteria are less likely to experience positive health selection compared to employment immigrants (Akresh and Frank 2008). The process of attaining a visa also creates differential stress due to varying levels of difficulty in meeting certain criteria as well as waiting periods produced by administrative prioritization and backlog (Jasso 2011; Obinna 2014; Morey et al. 2020). Such visa-related stress can generate long-lasting immigrant health disparities, in terms of both mental (Jasso 2011; Jasso et al. 2005) and physical (Morey et al. 2020) health. While previous research establishes that entry visa classifications stratify immigrants into a hierarchy of health advantage prior to arrival in the United States (Morey et al. 2020), the present study assesses if LPR admission categories shape the physical health trajectories of immigrants as they reside in the United States.
US Citizenship
In addition to documentation and LPR admission distinctions among immigrants is the citizenship divide. US citizen immigrants comprise those who have completed the official government naturalization process to become US citizens or dual US citizens. US citizenship is associated with greater social, economic, and civil rights, as well as lower levels of strain relative to being a non-US citizen, whether documented or not (Torres and Young 2016). Notably, until a person acquires US citizenship, deportation looms as a possible threat. For example, non-US citizen immigrants who are found guilty of committing certain crimes, including nonviolent offenses such as filing a false tax return, are subject to immediate deportation and permanent prohibition from the country (American Immigration Council 2016). Whether or not a crime has been committed, nearly 11 percent of naturalization applications are denied (USCIS 2018), which leads to continued legal disadvantage or even loss of legal residence and deportation. Consequently, both documented and undocumented immigrants disclose comparably high levels of stress, anxiety, and hopelessness due to deportation fear, for themselves and their family and friends (Arbona et al. 2010; Hacker et al. 2011). Legal status stress is in turn associated with poor self-rated health (Finch and Vega 2003; Cavazos-Rehg, Zayas and Spitznagel 2007).
Subsequently, being an authorized non-US citizen immigrant is also accompanied by social, civil, economic, and health disadvantages because it does not provide the stability and certainty of citizenship, nor equal access to health-promoting resources. US citizen immigrants earn 8 to 11 percent more in annual income compared to noncitizens (Pastor and Scoggins 2012). Furthermore, US citizenship grants people better access to healthcare, although this benefit varies by country of origin (Bacong and Ðoàn 2022). Non-US citizens are not eligible for federal assistance programs until after the completion of 5 years as legal US residents (Goldman, Smith and Sood 2005). In addition to being less likely to have public insurance through Medicaid and Medicare, noncitizens are less likely to have employer or individual insurance coverage than foreign-born and native-born US citizens (Goldman, Smith and Sood 2005). Although undocumented immigrants display the highest rates of lacking health insurance relative to naturalized US citizens, even LPRs exhibit a significant disadvantage in health insurance coverage (Goldman, Smith and Sood 2005).
The lack of health insurance coverage may have lasting consequences for the health of non-US citizen immigrants. Nevertheless, few studies examine the effects of citizenship on health outcomes and findings to date are inconclusive (Campbell et al. 2012; Balcazar, Grineski and Collins 2015; Filion, Fenelon and Boudreaux 2018; Van Natta et al. 2019; Bacong 2021). One study indicates that a health advantage in self-rated health exists for Latinx citizens in the United States, but this advantage does not extend to Latinx noncitizens (Campbell et al. 2012). Compared to the health of non-Latinx and Latinx US citizens, Latinx non-US citizens’ health benefits the least from increases in income (Campbell et al. 2012). Other studies reveal that US citizenship does not affect the likelihood of a child having a respiratory health condition or a psychological problem, despite its association with lacking insurance and a regular doctor (Balcazar, Grineski and Collins 2015; Filion, Fenelon and Boudreaux 2018). It is likely that US citizenship has a greater impact on some health outcomes compared to others, but further research is needed. Thus, in addition to socioeconomic status and racism (Phelan, Link and Tehranifar 2010; Phelan and Link 2015), citizenship is a fundamental, but underexplored, social determinant of health (Viruell-Fuentes 2007; Castañeda et al. 2015; Miranda et al. 2017).
Legal Status and Health Over Time
Extant research seldom examines legal status as a dynamic characteristic that changes over time. As such, the present study draws upon key insights from the life course perspective in order to clarify how legal status stratification operates as a social determinant of health (Viruell-Fuentes 2007; Torres and Young 2016). The life course perspective is a theoretical lens that highlights how earlier phases of life are related to later ones as well as how larger social, structural, and historical forces influence people's lives over time (Elder 1975). The concepts of transition and trajectory help identify and situate experiences over the life course. A trajectory is the particular route an individual's life takes, while a transition is an occurrence that affects this life path (Elder, Johnson and Crosnoe 2003; de Oca et al. 2011). Transitions and trajectories are rooted in and constrained by social and institutional environments (Elder 1975; de Oca et al. 2011), often patterned by the social groups to which individuals belong (Elder 1998). The current study explores the legal statuses that characterize the process of migration, a life-altering transition that shapes immigrants’ health trajectories.
Legal status shapes the transition into migration as well as social and civil integration after arrival (Torres and Young 2016; Kreisberg 2019). It also influences the health trajectories of immigrants. For example, in one qualitative study, undocumented migrants aged 50 years and older viewed their own rapid decline in health as related to decades of manual, low-wage labor (de Oca et al. 2011). Moreover, changes in legal status can improve or worsen health. Among older adults who migrated to the United States as children or young adults, US citizenship is associated with greater civic, occupational, and economic integration and fewer functional limitations relative to LPR status (Gubernskaya, Bean and van Hook 2013). As the life course perspective illustrates, legal status shapes the cumulative experiences of immigrants across social domains.
The Present Study
In the present study, I use longitudinal data from the NIS to evaluate the influence of legal status on physical health over time. Existing research tends to cross-sectionally examine legal status through binary documented/undocumented or citizen/noncitizen frameworks. Yet legal status comprises a hierarchy of rights, privileges, and incorporation, and is thus better conceived multidimensionally (Bean et al. 2011; Patler 2018). Therefore, in contrast to most existing research, I conceptualize legal status as a multifaceted characteristic which includes initial documentation classification, LPR admission category, and US citizenship. Each of these dimensions of legal status captures an immigrant's access to specific rights and resources, such as the legal right to live and work in the United States (documentation classification), social and labor market ties (LPR admission category), and protection from deportation (US citizenship). By employing a multidimensional conceptualization of legal status, I illuminate health disparities among immigrants that binary frameworks are not able to capture.
I also theorize that legal status is a dynamic form of stratification, and test if initial legal statuses have persistent consequences for health, even after immigrants attain LPR. Because the NIS assesses multiple dimensions of legal status at two different time points, it allows for the examination of transitions into different legal statuses, and their relationship with health, over time. This work can encourage future longitudinal research on changes in immigrant legal status, adding to emerging literature exposing nuances in the notion of an overall immigrant health advantage.
Lastly, while there is an emerging body of literature examining the association of legal status with self-rated and mental health (Martinez et al. 2015), research on physical health is scant and findings to date are mixed (Hamilton, Hale and Savinar 2019). Results from the present study provide empirical support to the theoretical arguments that documentation status is a critical social determinant of health (Cabral and Cuevas 2020). In sum, the current study examines how multiple and dynamic dimensions of legal status shape physical health and contributes to existing literature by (1) providing empirical support to theoretical, but yet largely unsupported, arguments that documentation status is a social determinant of health; (2) expanding the study of immigrant legal status through the use of a multidimensional conceptualization of legal status to illuminate health disparities among immigrants that binary frameworks are not able to capture; and (3) exposing nuances in patterns of an immigrant health advantage, particularly those due to sociopolitical forces.
Data and Methods
Data in this study came from the New Immigrant Survey (NIS), a nationally representative (n = 8,573 at Wave 1; n = 4363 at Wave 2) longitudinal survey of adult immigrants surveyed due to their recent acquisition of LPR status in the United States at the time of survey recruitment (Jasso et al. 2006). Respondents were recruited through electronic administrative records of new immigrants who entered the United States or adjusted their legal status from May to November 2003, compiled by the US Citizenship and Immigration Services. The two interviews occurred approximately 5 years apart, the first in 2003 and 2004, immediately after respondents obtained LPR status. Interviews were conducted either over the phone (60 percent at Wave 1) or in-person (40 percent at Wave 1) and in respondents’ preferred language. The same respondents were recontacted and asked to complete a second interview between 2007 and 2009.
The first interview had a response rate of 69 percent, while the second interview had a response rate of 51 percent. While selection issues due to attrition are a perennial concern with longitudinal studies, the NIS investigators found that inclusion in the Wave 2 interview was not significantly related to current health status (Massey, Jasso and Espinoza 2017). My own analysis of attrition indicated that the probability of having a chronic condition at Wave 1 was not significantly different for those who completed both survey waves compared to those who dropped out (n = 8544; 29 individuals missing health data). Nevertheless, all analyses utilized inverse-probability sample weights which help account for bias due to nonresponse.
The survey included wide-ranging topics such as migration history, employment, education, and health. The NIS also linked survey data with administrative records to obtain variables related to legal status, such as visa type. Although the age of the data is a limitation, the NIS allows for the examination of legal status transitions, and their relationship to health, due to its inclusion of multiple measures of legal status, longitudinal design, and nationally representative sample of immigrants who received LPR in 2003 and 2004. While other surveys of immigrants include measures of legal status, longitudinal assessments, or a geographically diverse sample of immigrants, the NIS is unique because it meets all three of these criteria. Therefore, although the results are not generalizable to non-LPR immigrants or current immigrant cohorts, the strengths of the NIS outweigh its limitations. Because this data is publicly available and contains de-identified individual information, the study received a human subject exemption from the author's Institutional Review Board.
Measures
The dependent variable is an overall indicator of physical health based on self-reported health conditions. Respondents were specifically asked if a given condition was diagnosed by a doctor (1 = yes, 0 = no). Sample sizes for respondents indicating specific chronic conditions lacked the statistical power to analyze individually for each of the dimensions of legal status. Consequently, I created an index count by summing respondents’ reports of having any of the eight physical health outcomes contained in the survey (diabetes mellitus, hypertension, arthritis, asthma, cancer, stroke, heart disease, and lung conditions). The most commonly reported health condition was hypertension (8.14 percent at baseline; 17.04 percent at follow up), while the least common was stroke (0.23 percent at baseline; 0.51 percent at follow up). From this physical health variable, I then created a dichotomous measure of physical health (1 = presence of condition). Estimating linear regression models with physical health operationalized as a count of health conditions did not alter the results due to the infrequency of respondents indicating more than one illness (3.44 percent at baseline); therefore, I utilized a more parsimonious binary physical health measure.
Legal status variables
The principal independent variable is legal status prior and subsequent to acquiring LPR status. Although all respondents in the NIS sample achieved LPR status before survey recruitment, LPRs enter the country with different legal statuses. Prior legal status may influence the transition into LPR status and ensuing health trajectories. In addition, a portion of respondents attained US citizenship by the second interview, which may also alter their health trajectories. Since legal status is a multidimensional attribute, I measured it in three ways: initial documentation classification, LPR admission category, and US citizenship.
First, I created a prior legal status variable with three categories based on respondents’ type of documentation on their most recent trip to the United States: permanently documented, temporarily documented, and undocumented. A binary (documented vs. undocumented) conceptualization of documentation can conceal the experiences of immigrants who are documented but hold temporary visas, such as students (Ortega et al. 2007). Thus, I included two categories of authorized immigrants. The permanently documented group serves as the reference category and is comprised of individuals who indicated that they had no prior experience in the United States and entered the country with permanent resident visas. The temporarily documented group includes respondents who entered the country with legal documents that were conditional or temporary. The third group, undocumented, consists of those who entered without documents or with fraudulent documents. 1 This first dimension encapsulates the lawful facet of immigrant legal status.
Second, I grouped respondents according to the type of criteria they met in order to obtain their LPR visa: family preference (reference), employment, refugee, legalization, and diversity or other. The family preference category includes individuals who received their LPR visa because they were a spouse of a US citizen or LPR, a parent of a US citizen, a child of a US citizen, or a family fourth preference. Within the diversity or other category, 63 percent were diversity visa holders and 37 percent met other, undisclosed criteria. The LPR admission categorization of legal status indicates the conditions surrounding migration and authorization, such as particular eligibility criteria and available resources.
Lastly, I included citizenship as a measure of legal status in the longitudinal analyses. The citizenship measure is taken directly from the NIS and indicates whether or not respondents obtained US citizenship by the second interview. This variable captures the citizen/noncitizen divide.
Social determinants of health
I included several sociodemographic covariates associated with health. First, the relationship between legal status and health varies by gender (León-Pérez, Patterson and Coelho 2021) and age (Gubernskaya, Bean and van Hook 2013). Gender is a dichotomous variable taken directly from the NIS (1 = woman). I measured age in years by subtracting the respondent's birth year by the year they completed the survey. Immigrant legal status is also racialized, creating differential health burdens by race/ethnicity (Bacong and Menjívar 2021). Based on responses to two questions (i.e., “Do you consider yourself to be Hispanic or Latino?” and “What race do you consider yourself to be?”), I made a mutually exclusive race/ethnicity variable with five categories: Latinx (reference), non-Latinx white, non-Latinx Asian, non-Latinx black, and non-Latinx other race (including more than one race). The protective effect of education on health is well-established (Ross and Wu 1995), although the education-health gradient is often weaker among immigrant populations in the United States (Buttenheim et al. 2010; Ro et al. 2016). As such, I created a categorical variable for education based on respondents’ reported number of years of schooling completed at the time of first interview: less than high school (reference), high school graduate, some college, and college degree or higher. I also included a dichotomous variable from the NIS measuring whether respondents received an additional degree between survey waves (1 = yes) in the longitudinal analyses. Marital status has a long-standing relationship with health (Liu and Umberson 2008), including immigrant well-being (Kposowa, McElvain and Breault 2008). In this study, marital status indicates whether respondents were 1 = married or living with a partner or 0 = never married, separated, divorced, or widowed. Similarly, employment status is a significant predictor of immigrant physical health (Danso 2016). Employment status signifies whether respondents were 1 = currently employed or 0 = else (includes unemployed, retired, homemaker, etc.). Lastly, health insurance coverage is stratified by legal status (Goldman, Smith and Sood 2005), with resultant disparities in access to healthcare (Siddiqi, Zuberi and Nguyen 2009). Health insurance coverage is measured as whether individuals were currently covered by health insurance or not (1 = yes).
Models also controlled for two characteristics related to migration history. The health of immigrants varies by their region of origin (Reynolds, Chernenko and Read 2016) and tends to erode over time spent in the United States (Acevedo-Garcia et al. 2010). I created a region of origin variable by condensing respondents’ reported country of birth into four broad regions: Latin America (reference), Asia, Africa or Middle East, and Europe or North America. Duration of residence measures the number of years respondents had lived in the United States at the time of the first survey and is calculated by subtracting the year of respondents’ most recent trip to the United States by the first survey year. In the present analyses, gender, race/ethnicity, education, received an additional degree between survey waves, region of origin, and duration of residence in the United States are time-invariant measures, while age, marital status, employment status, and health insurance are time-variant.
Analytic Strategy
I used this data to conduct two sets of analyses which capture the relationship between legal status and physical health (1) at the first interview and (2) over time, between survey waves. Although the main focus of this article is the relationship between legal status and health over time, I first assessed the health of respondents at the first wave of the survey in order to establish a baseline association between the variables of interest. In the preliminary set of analyses, I used the first wave of data to conduct a series of multivariate logistic regressions, assessing the predicted probabilities of respondents reporting a chronic condition by prior legal status.
In the second set of analyses, I evaluated health status using both waves of data. This second set of regressions determines if prior and current legal status have enduring effects on health, five years after all immigrants in the sample achieved the same legal status as LPRs. I employed mixed effects multivariate logistic regressions to assess the relationship between legal status and having a chronic condition. Mixed effects models not only estimate a random effects model but also include time-invariant predictors for all time-changing variables in order to assess both their between-person and within-person effects on the outcome. For each time-varying measure, I created cluster-specific means (i.e., within-person means), as well as deviation scores (i.e., how much the observed measure varies from the cluster-specific mean). These variables are then added into the models in lieu of the original variable, with the cluster-specific means and deviation scores estimating if the association of time-variant measures with the outcome variable is due to changes within an individual or differences between individuals, respectively (Schunck 2013).
In both sets of analyses, I assessed the dimensions of legal status individually. That is, I modeled initial documentation classification, LPR admission category, and US citizenship separately so that I could evaluate the unique effect of each dimension. Given that no respondents were US citizens at Wave 1, I only examined predicted probabilities of respondents reporting ill-health by US citizenship in the longitudinal analyses.
The analytic sample includes respondents with complete data for both survey waves, which is consistent with prior research using NIS data (Reed and Yrizar Barbosa 2017; León-Pérez, Patterson and Coelho 2021). I utilized listwise deletion to exclude respondents with missing data on any of the examined variables, which results in an analytic sample of 3550. Sensitivity analyses with multiple imputation using chained equations for all respondents (n = 8573) revealed substantively similar results with one exception: At baseline, diversity or other respondents were significantly less likely to report a chronic condition relative to family preference immigrants at baseline (β = −0.27, C.I. = [ −0.49–0.05], p < .05). Given that results using listwise deletion were unchanged for the main focus of the study (i.e., the longitudinal analyses), as well as the straightforward ability to generate predicated probabilities with nonmultiple imputation methods, I present results from the complete cases analyses only. I conducted all analyses in STATA-14 using the NIS sample weights, which adjust for oversampling of immigrants with employment visas and attrition due to nonresponse.
Results
Descriptive Statistics
Table 1 displays the weighted descriptive statistics. Over half of the sample were women (56.47 percent), with an average age of 38.82 years at Wave 1. Most respondents had less than a high school education (35.51 percent). Nearly 15 percent of respondents received an additional degree between survey waves. The majority of respondents were married and employed at both waves. Latin America was the most frequently reported region of origin (44.06 percent) and a Latinx identity was the most commonly indicated race/ethnicity (38.78 percent). A plurality of respondents initially entered the US temporarily documented (41.70 percent), followed by permanently documented (35.53 percent). A majority of respondents received their LPR status through family preference criteria (57.55 percent). Of the 3550 respondents, nearly 9 percent became US citizens by the second wave of the survey. Physical ill-health increased between survey waves, with 16.52 percent of respondents reporting at least one physical health condition in Wave 1 and 28.39 percent in Wave 2.
Weighted Descriptive Statistics for the New Immigrant Survey (NIS) Sample (n = 3550).
Source: Author's calculations using data from the NIS.
1 = Presence of condition; includes diabetes mellitus, hypertension, arthritis, asthma, cancer, stroke, heart disease, and lung conditions.
Legal Status and Health at Baseline
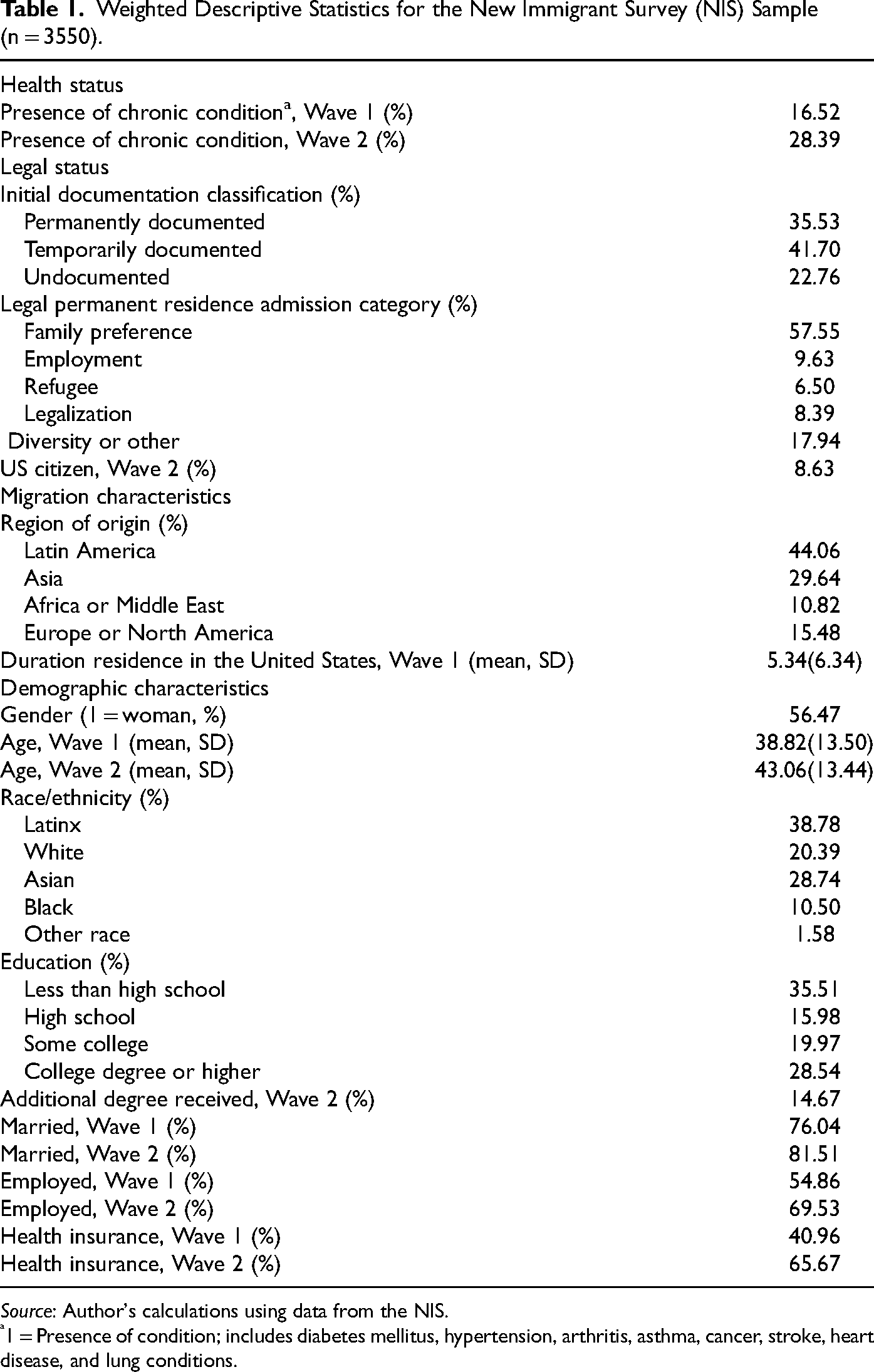
Figure 1 displays the predicted probabilities for initial documentation classification and physical health at Wave 1. Correspondent results for the coefficients used to estimate all the predicted probabilities presented in this section can be found in Appendix Tables 1 to 5. Both temporarily documented (Pred. Prob = 14.55, CI = [12.13–16.96], p < .05) and initially undocumented immigrants (Pred. Prob = 15.73, CI = [12.00–19.46], p < .05) exhibited significantly higher percent predicted probabilities of physical morbidity relative to immigrants who entered the US permanently documented (Pred. Prob = 10.84, CI = [8.62–13.05]). Notably, a supplemental adjusted Wald test indicated that the difference in probability of physical ill-health between those who entered the United States with temporary documentation compared to those who entered the United States without documentation was not statistically significant (p > F = .60).
Initial Documentation Classification and Predicted Probabilities of Reporting a Chronic Conditiona at Baseline (n = 3550). Source: Author's Calculations Using Data From the New Immigrant Survey. Notes: Weighted Statistics. Reference Groups are Permanently Documented, Latin America, Latinx, and Less Than High School Education. Error Bars Present 95% Confidence Intervals. a 1 = Presence of Condition; Includes Diabetes Mellitus, Hypertension, Arthritis, Asthma, Cancer, Stroke, Heart Disease, and Lung Condition.
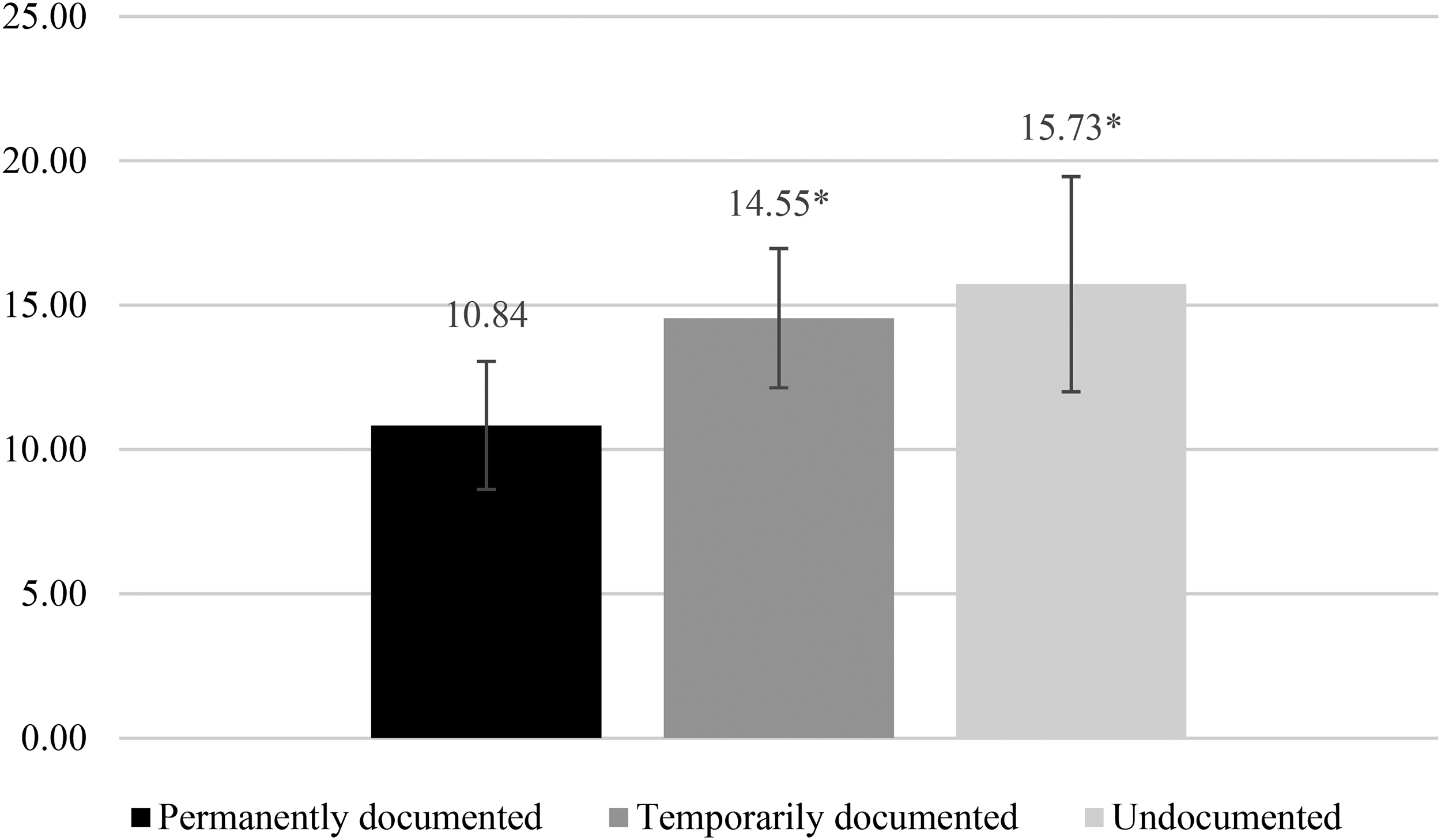
The eligibility category through which respondents obtained LPR status also predicted health at baseline, as depicted in Figure 2. Diversity or other immigrants had the lowest predicted probability of having a chronic condition at baseline (Pred. Prob = 10.56, CI = [7.92–13.20]), followed by family preference (Pred. Prob = 11.86, CI = [9.81–13.91]) and employment (Pred. Prob = 15.02, CI = [11.19–18.84]) immigrants. Compared to family preference immigrants, refugee (Pred. Prob = 21.15, CI = [14.95–27.34], p < .01) and legalization immigrants (Pred. Prob = 22.32, CI = [16.09–28.54], p < .01) had significantly higher predicted probabilities of having a chronic condition.
Legal Permanent Residence Admission Category and Predicted Probabilities of Reporting a Chronic Conditiona at Baseline (n = 3550). Source: Author's Calculations Using Data From the New Immigrant Survey. Notes: Weighted Statistics. Reference Groups are Family Preference, Latin America, Latinx, and Less Than High School Education. Error Bars Present 95% Confidence Intervals. a 1 = Presence of Condition; Includes Diabetes Mellitus, Hypertension, Arthritis, Asthma, Cancer, Stroke, Heart Disease, and Lung Condition.
Legal Status and Health Over Time
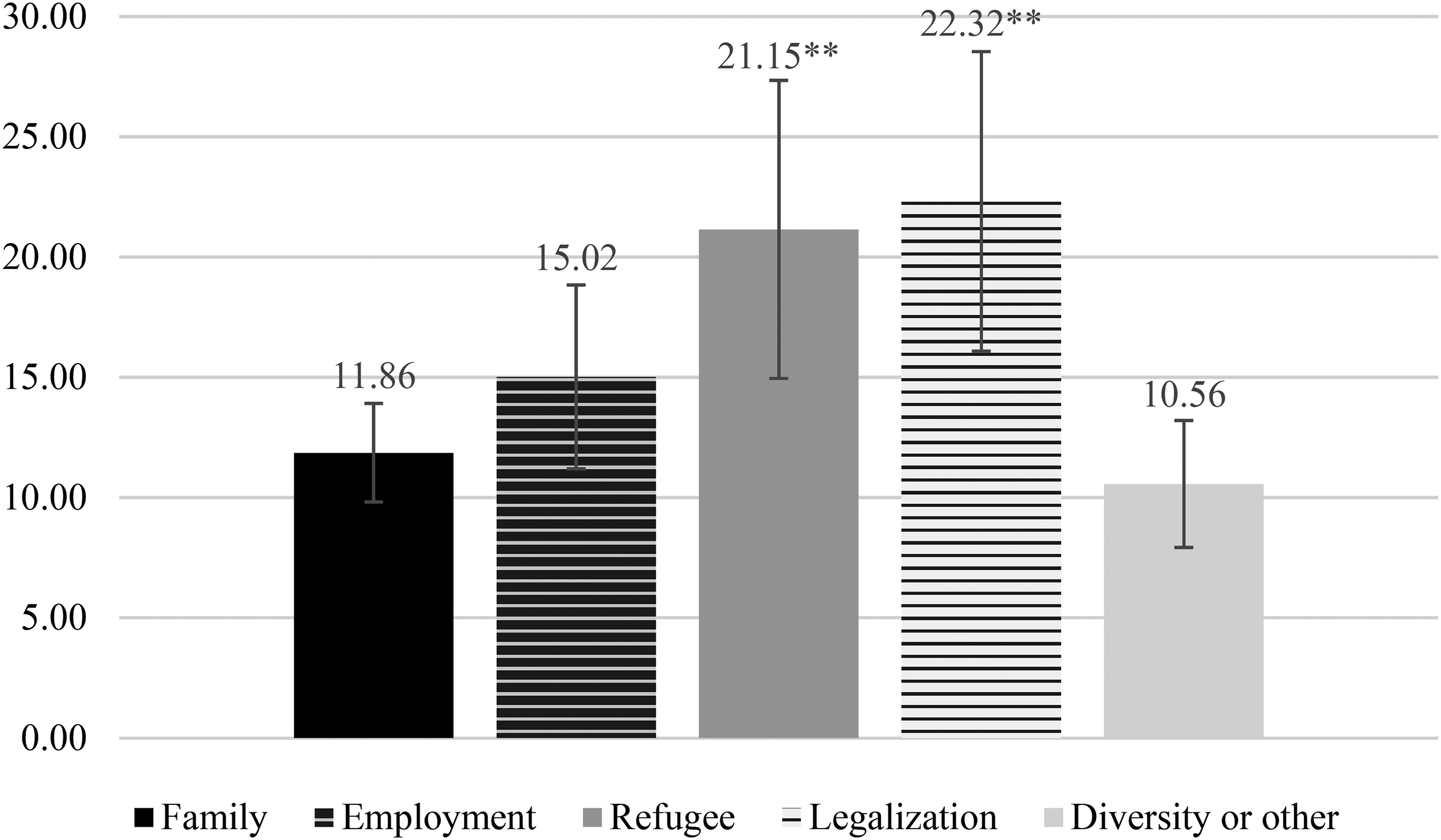
Figure 3 presents results for the relationship between documentation classification and physical health over both waves of the survey. Both temporarily documented (Pred. Prob = 19.19, CI = [17.98–20.41], p < .05) and undocumented immigrants (Pred. Prob = 20.69, CI = [18.61–22.78], p < .05) exhibited higher predicted probabilities of having a chronic condition compared to permanently documented immigrants (Pred. Prob = 17.05, CI = [15.64–18.45]). A supplemental adjusted Wald test again showed that the probability of having a chronic condition among those who entered the United States with temporary documentation compared to those who entered the United States without documentation was not statistically significant over time (p > F = .23).
Initial Documentation Classification and Predicted Probabilities of Reporting a Chronic Conditiona Over Time (n = 3550). Source: Author's Calculations Using Data From the New Immigrant Survey. Notes: Weighted Statistics. Reference Groups are Permanently Documented, Latin America, Latinx, and Less Than High School Education. Error Bars Present 95% Confidence Intervals. a 1 = Presence of Condition; Includes Diabetes Mellitus, Hypertension, Arthritis, Asthma, Cancer, Stroke, Heart Disease, and Lung Condition.
Disparities also emerged when analyzing physical health by LPR admission category, as shown in Figure 4. Employment (Pred. Prob = 16.65, CI = [14.26–19.03], p > .10) and diversity or other immigrants (Pred. Prob = 18.25, CI = [16.41–20.08], p > .10) did not have significantly different predicted probabilities of having a chronic condition relative to family preference immigrants (Pred. Prob = 17.11, CI = [16.11–18.11]). In contrast, refugees (Pred. Prob = 27.22, CI = [23.54–30.91], p < .001) exhibited the highest probability of having a chronic condition over time, followed by legalization immigrants (Pred. Prob = 27.21, CI = [23.41–31.00], p < .001), both of which were significantly higher relative to family preference immigrants’ probability of morbidity.
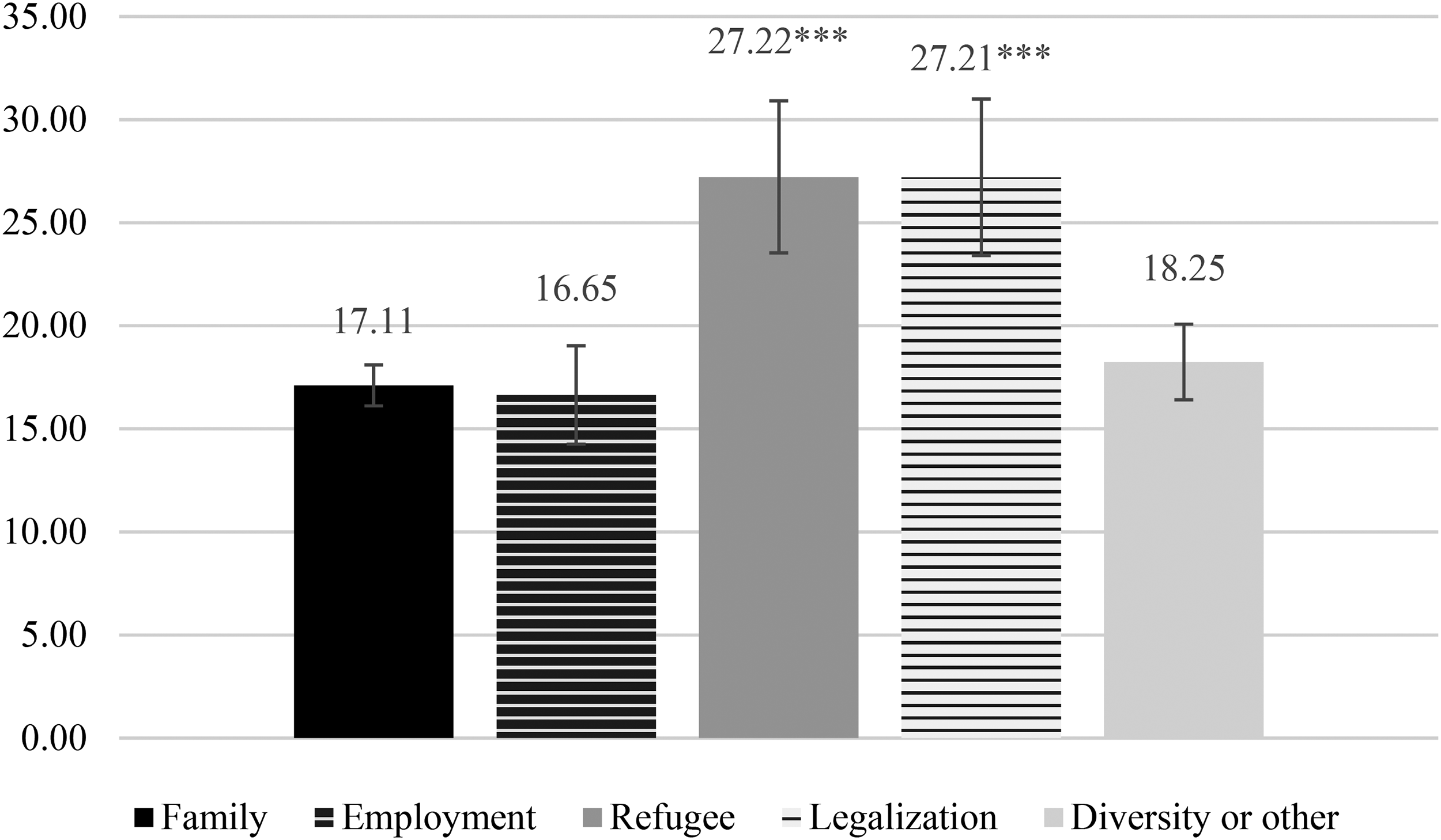
Legal Permanent Residence Admission Category and Predicted Probabilities of Reporting a Chronic Conditiona Over Time (n = 3550). Source: Author's Calculations Using Data From the New Immigrant Survey. Notes: Weighted Statistics. Reference Groups are Family Preference, Latin America, Latinx, and Less Than High School Education. Error Bars Present 95% Confidence Intervals. a 1 = Presence of Condition; Includes Diabetes Mellitus, Hypertension, Arthritis, Asthma, Cancer, Stroke, Heart Disease, and Lung Condition.
Figure 5 presents results for the relationship between US citizenship and physical health over time. Non-US citizens (Pred. Prob = 19.08, CI = [18.29–19.86], p < .01) demonstrated a significantly higher predicted probability of reporting a chronic condition compared to immigrants who obtained US citizenship (Pred. Prob = 15.09, CI = [12.61–17.57]).
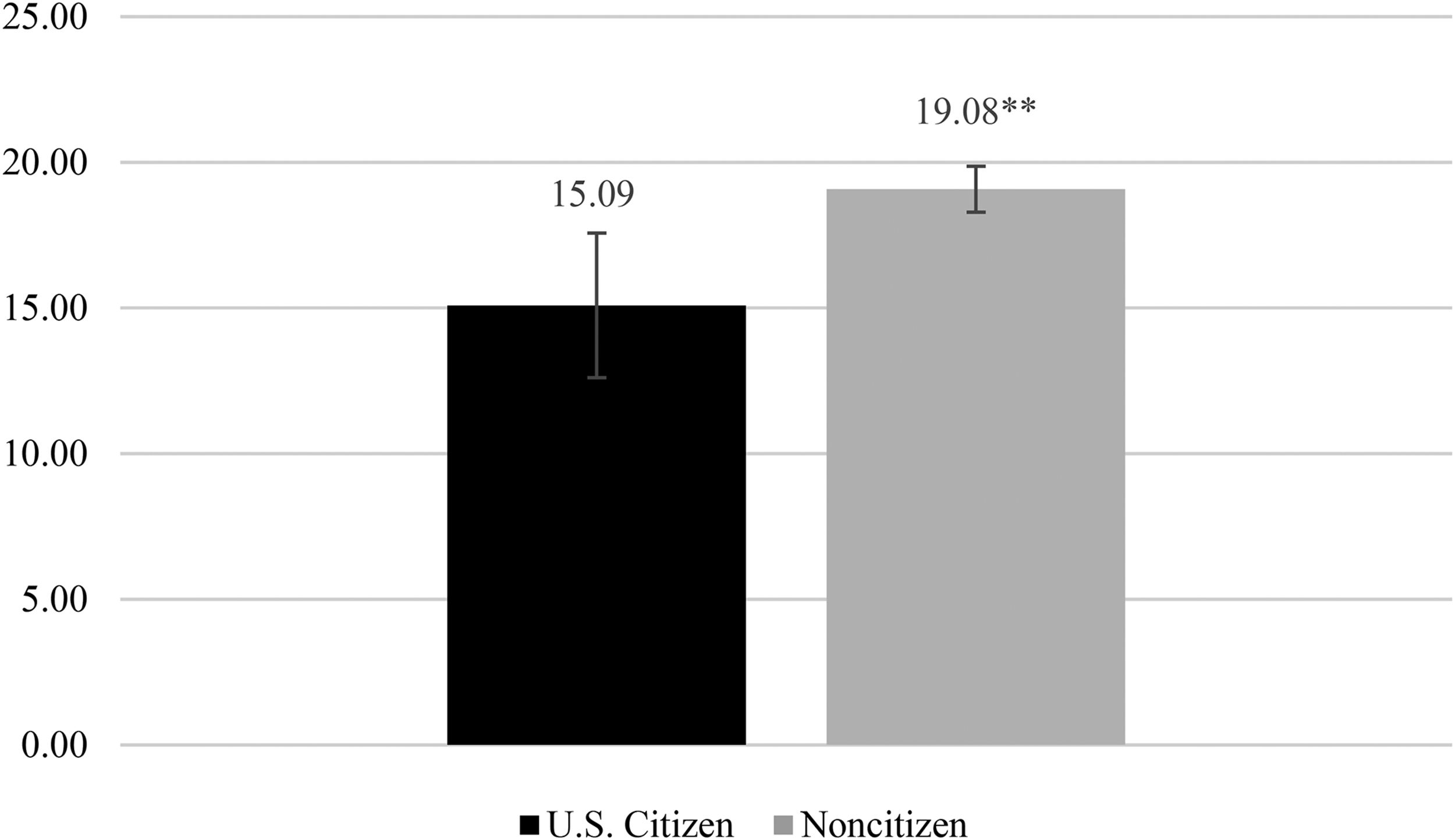
US Citizenship and Predicted Probabilities of Reporting a Chronic Conditiona Over Time (n = 3550). Source: Author's Calculations Using Data From the New Immigrant Survey. Notes: Weighted Statistics. Reference Groups are Latin America, Latinx, and Less Than High School Education. Error Bars Present 95% Confidence Intervals. a 1 = Presence of Condition; Includes Diabetes Mellitus, Hypertension, Arthritis, Asthma, Cancer, Stroke, Heart Disease, and Lung Condition.
Discussion and Conclusions
All three dimensions of legal status examined in this article were associated with health. In terms of initial documentation classification, findings indicated that the privileges of LPR in the legal status stratification scheme (Jasso 2011), as well as the more stringent eligibility criteria, translated to a health advantage for immigrants who entered the United States permanently documented. Conversely, individuals who entered the United States undocumented exhibited a significant physical health disadvantage at baseline and over time. This finding supports theoretical arguments that documentation status is a critical social determinant of health (Cabral and Cuevas 2020), even as it contrasts the majority of extant empirical research which fails to find significant disparities in physical health by documentation status (Hamilton, Hale and Savinar 2019). Yet existing studies have been limited by their focus on few health measures, use of small and/or nonrandom samples, and assessment of health at one point in time, which may render them unable to capture the enduring effects of documentation-related stress on health (Cavazos-Rehg, Zayas and Spitznagel 2007; Martinez et al. 2015; Torres and Young 2016). As the present results demonstrate, the disadvantages of being previously undocumented extend to individuals who later acquire LPR status. The current study therefore contributes to the proposition that documentation status is disadvantageous for health by providing clear evidence of the association between documentation classification and physical morbidity among a nationally representative sample of US LPR immigrants.
The current research also extends upon existing literature by showing that, in addition to undocumented status, temporary documentation status is associated with physical morbidity relative to permanent documentation status. Analyses demonstrated that the probability of having a chronic condition for the temporarily documented and undocumented groups was not significantly different in either the baseline or longitudinal analyses. This could be interpreted as a surprising finding for the previously undocumented group, given the heightened stress and health risks linked to unauthorized status (Cabral and Cuevas 2020). However, misclassification of initial documentation status and/or underestimation of the stressors associated with temporary and conditional visas may partially explain why previously documented immigrants exhibited a probability of ill-health similar to previously undocumented immigrants.
First, there may be immigrants in the temporarily documented category who entered the United States with valid documents who transitioned into undocumented status. In the present study, documentation classification captured legal status upon entry into the United States. The undocumented category therefore encompassed immigrants who entered the country without documents or with fraudulent documents, but not those who became undocumented by overstaying a temporary visa or working without authorization. The misclassification of respondents with previous undocumented experience as temporarily documented may obscure some of the differences between the two groups given that the stress of being unauthorized, even briefly, can have enduring health effects (Cavazos-Rehg, Zayas and Spitznagel 2007; Martinez et al. 2015; Torres and Young 2016).
Second, it may also be that the stress of attaining nonpermanent documentation statuses, which include temporary or conditional visas, may be underestimated in the literature. That is, achieving such documentation statuses means being on the radar of immigration officials and thus navigating bureaucratic application processes and adhering to specific guidelines such as paying taxes, submitting up-to-date home addresses, and observing visa expiration dates. These factors can cause stress due to the perception of being tracked and potentially caught failing to meet the plethora of regulations. They also create a sense of uncertainty for temporary and conditional visa holders that can last for years and restrict their range of action in different spheres of life, from the labor market to their social network (Menjívar 2006). Legal status stress in turn erodes health (Finch and Vega 2003; Cavazos-Rehg, Zayas and Spitznagel 2007). Therefore, although immigrants without documents face similar stressors related to having tenuous claims to residence in the United States, immigrants with temporary or conditional documents may experience stressors unique to their documentation classification as well. As the present study demonstrates, these stressors can have a substantial influence on health. Immigrant health research should expand their conceptualizations of documentation status beyond binary classifications to include groups with “liminal legality” (Menjívar 2006).
In addition, LPR admission category was consistently associated with health. At baseline, findings revealed enduring disparities in health for legalization and refugee immigrants. Notably, LPR admission categories reflect the health selectivity of immigrants and therefore likely contribute to the disadvantaged health of legalization and refugee immigrants. Specifically, elevated rates of chronic illness may result from the persistent stress of legalization immigrants’ previous undocumented experience and refugees’ exposure to violence and unrest in their home countries. Although likely a consequence of both health selection and ensuing health stratification processes, I was unable to evaluate the role of health selection in generating the observed disparities in the present study. Research should continue to assess the distinct contributions of factors prior and subsequent to migration on immigrant health.
In addition to health selection, the legal status stratification system generates disparities in health among immigrants over time. All respondents in the present study attained LPR visas before the first interview, so it is probable the respondents’ prior legal status produced some of the observed disparities in health. LPR admission categories may be especially consequential for immigrant health because they signify policies that stipulate who is eligible to migrate, what resources are available to them, and how they are able to navigate paths to LPR status or US citizenship (Morey et al. 2020). As a key dimension of legal status, visa type impacts social integration, exposure to stressors, socioeconomic opportunities, work conditions, access to health-promoting services (Jasso 2011; Obinna 2014; Kreisberg 2019; Morey et al. 2020), and the subsequent health trajectories of immigrants. For instance, the socioeconomic resources afforded to employment immigrants may have contributed to their lower predicted probability of physical health relative to family preference immigrants over time. On the other hand, the labor market is particularly unfavorable to workers with undocumented or refugee experience (Kreisberg 2019), which constrains legalization immigrants’ and refugees’ socioeconomic prospects. The current results reveal that differential exposure to health risks and access to resources produces, or at least exacerbates, health disparities by LPR admission category.
Lastly, consistent with expectations, non-US citizens exhibited worse health compared to those who became US citizens by the follow-up survey. Although all respondents in the sample were LPRs, becoming a citizen is accompanied by social, civil, economic, and health privileges above and beyond legal documentation. US citizenship accords immigrants higher incomes (Pastor and Scoggins 2012) and better access to healthcare (Goldman, Smith and Sood 2005). It also alleviates stress related to fear of deportation and provides a sense of stability not afforded to those with undocumented or other documentation statuses. Therefore, as researchers have previously argued (e.g., Viruell-Fuentes 2007; Castañeda et al. 2015; Miranda et al. 2017), citizenship is a fundamental social determinant of health that warrants further attention.
Beyond the limitations related to misclassification of temporary/unauthorized documentation status and health selection previously mentioned, a few other critical considerations should be noted. Since the data are restricted to immigrants who received LPR in the United States in 2003 and 2004, results are not generalizable to all immigrants, other historical periods, or national contexts outside of the United States. Related to this issue of generalizability, the finding of initial undocumented status being associated with a higher predicted probability of having a chronic condition may not extend to persistently undocumented immigrants. The use of self-reported health conditions is another limitation, given that diagnosis of a condition necessitates access to and utilization of healthcare, which is patterned by immigration and legal statuses. Finally, nonresponse may bias findings if the likelihood of participation in the follow-up survey varies by health status. For instance, it could be that unhealthy individuals were less likely to participate in Wave 2 because they returned to their home country or were too sick to partake. Although this concern is partially alleviated by attrition analyses which indicate that nonresponse was not significantly related to participants’ current health status (Massey, Jasso and Espinoza 2017), future research should examine the relationship between legal status and health among immigrants in recent cohorts, with more diverse legal statuses at the time of survey completion, with clinical measures of health, and with lower attrition rates.
Despite these limitations, the present research promotes the theorization of legal status as dynamic and multidimensional, comprised of several sociopolitical dimensions that shape immigrant health. Multiple components of legal status have enduring consequences for health because they constrain immigrants’ transitions into migration as well as propel them down divergent trajectories of integration. Results demonstrate the benefits of obtaining US citizenship, as well as the disadvantages of previous undocumented, temporarily documented, legalization, or refugee experience in the hierarchy of immigrant health. These findings indicate that institutional forces stratify immigrants into a hierarchy of privilege and subsequent well-being, which binary conceptualizations of legal status cannot fully capture. This has important implications regarding US policies related to immigration and incorporation. For example, programs such as the Affordable Care Act should be expanded to include health insurance coverage for temporarily documented and undocumented immigrants in order to reduce disparities in healthcare access and outcomes by legal status. In addition, given that disadvantages in health remained five years after all refugees in the current sample attained LPR, social and health services for refugees should be extended past their current two-year limit. Overall, the present study complicates the overarching notion of an immigrant health advantage by contributing to emerging research on the sociopolitical factors that foster disparities in immigrant health.
Future research should continue to explore legal status as a multidimensional and dynamic characteristic. One potentially fruitful way to expand the present work is to assess the relationship between legal status and health using one multifaceted measure of legal status that comprises documentation classification, LPR admission category, citizenship and/or other sociopolitical components concurrently. For example, one could compare the health trajectories of previously undocumented non-US citizen immigrants who met family reunification criteria to initially permanently documented non-US citizens who met family reunification criteria, etc. In such a measure, one would need a dataset large enough to provide adequate sample sizes at the intersection of various dimensions of legal status. Such research would further our theoretical understandings of legal status as dynamic and multidimensional, as well as offer empirical evidence disentangling the aspects of legal status that contribute to observed disparities in immigrant health. The present study provides an initial step in formulating legal status beyond the binary, while it highlights the disparities in immigrant health obscured by current conceptualizations.
Footnotes
Author's Note
Rachel A Zajdel, National Institutes of Health, Bethesda, MD, USA.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was partially supported by the Divisions of Intramural Research of the National Heart, Lung, and Blood Institute and the National Institute of Minority Health and Health Disparities, National Institutes of Health [grant number not applicable].
Supplemental Material
Supplemental material for this article is available online.
Notes
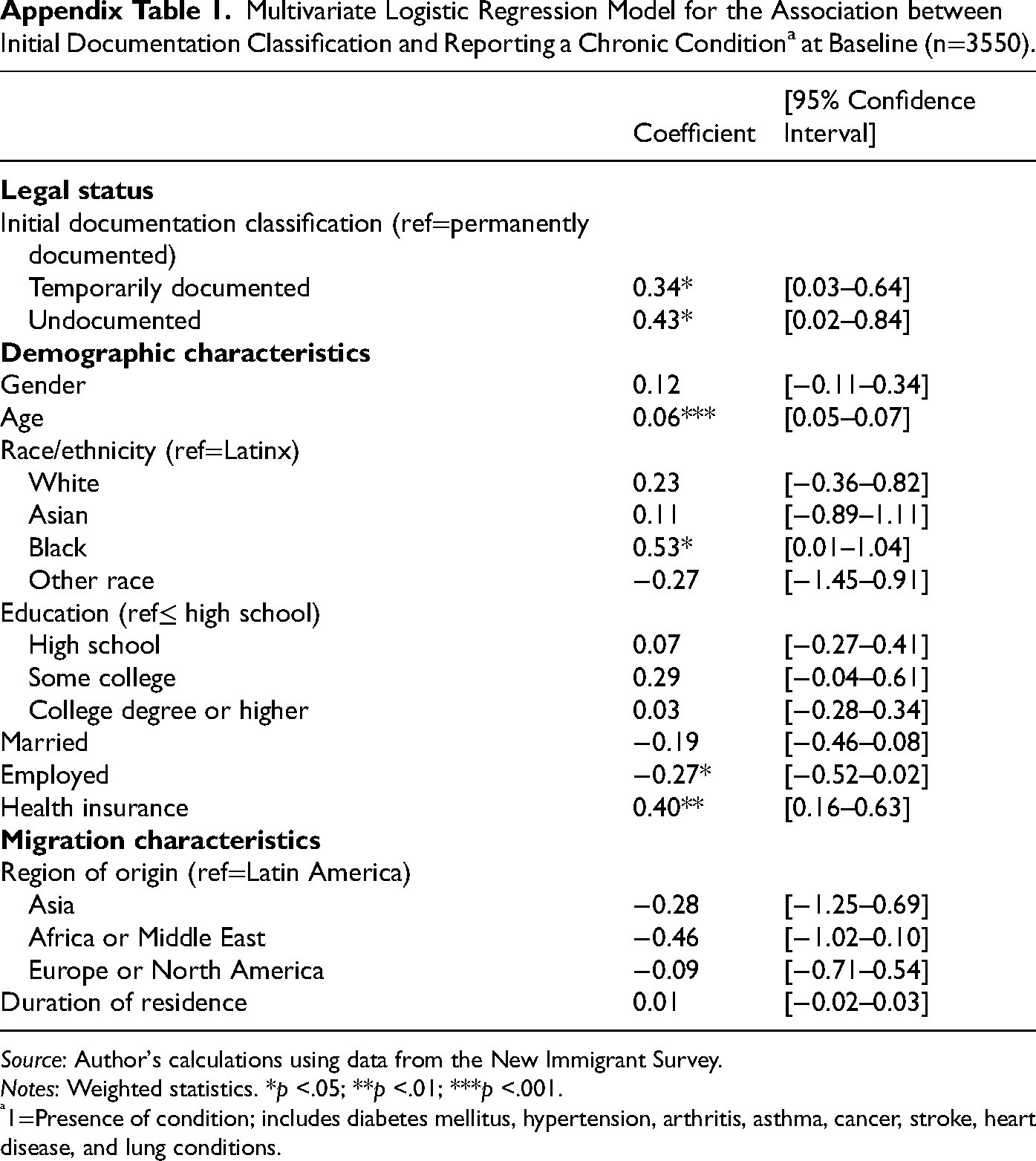
Multivariate Logistic Regression Model for the Association between Initial Documentation Classification and Reporting a Chronic Conditiona at Baseline (n=3550).
| Coefficient | [95% Confidence Interval] | |
|---|---|---|
|
|
||
| Initial documentation classification (ref=permanently documented) | ||
| Temporarily documented | 0.34* | [0.03–0.64] |
| Undocumented | 0.43* | [0.02–0.84] |
|
|
||
| Gender | 0.12 | [−0.11–0.34] |
| Age | 0.06*** | [0.05–0.07] |
| Race/ethnicity (ref=Latinx) | ||
| White | 0.23 | [−0.36–0.82] |
| Asian | 0.11 | [−0.89–1.11] |
| Black | 0.53* | [0.01–1.04] |
| Other race | −0.27 | [−1.45–0.91] |
| Education (ref≤ high school) | ||
| High school | 0.07 | [−0.27–0.41] |
| Some college | 0.29 | [−0.04–0.61] |
| College degree or higher | 0.03 | [−0.28–0.34] |
| Married | −0.19 | [−0.46–0.08] |
| Employed | −0.27* | [−0.52–0.02] |
| Health insurance | 0.40** | [0.16–0.63] |
|
|
||
| Region of origin (ref=Latin America) | ||
| Asia | −0.28 | [−1.25–0.69] |
| Africa or Middle East | −0.46 | [−1.02–0.10] |
| Europe or North America | −0.09 | [−0.71–0.54] |
| Duration of residence | 0.01 | [−0.02–0.03] |
Source: Author's calculations using data from the New Immigrant Survey.
Notes: Weighted statistics. *p <.05; **p <.01; ***p <.001.
1=Presence of condition; includes diabetes mellitus, hypertension, arthritis, asthma, cancer, stroke, heart disease, and lung conditions.
Multivariate Logistic Regression Model for the Association Between Legal Permanent Residence (LPR) Admission Category and Reporting a Chronic Conditiona at Baseline (n=3550). Source: Author's calculations using data from the New Immigrant Survey. Notes: Weighted statistics. *p <.05; **p <.01; ***p <.001. 1=Presence of condition; includes diabetes mellitus, hypertension, arthritis, asthma, cancer, stroke, heart disease, and lung conditions.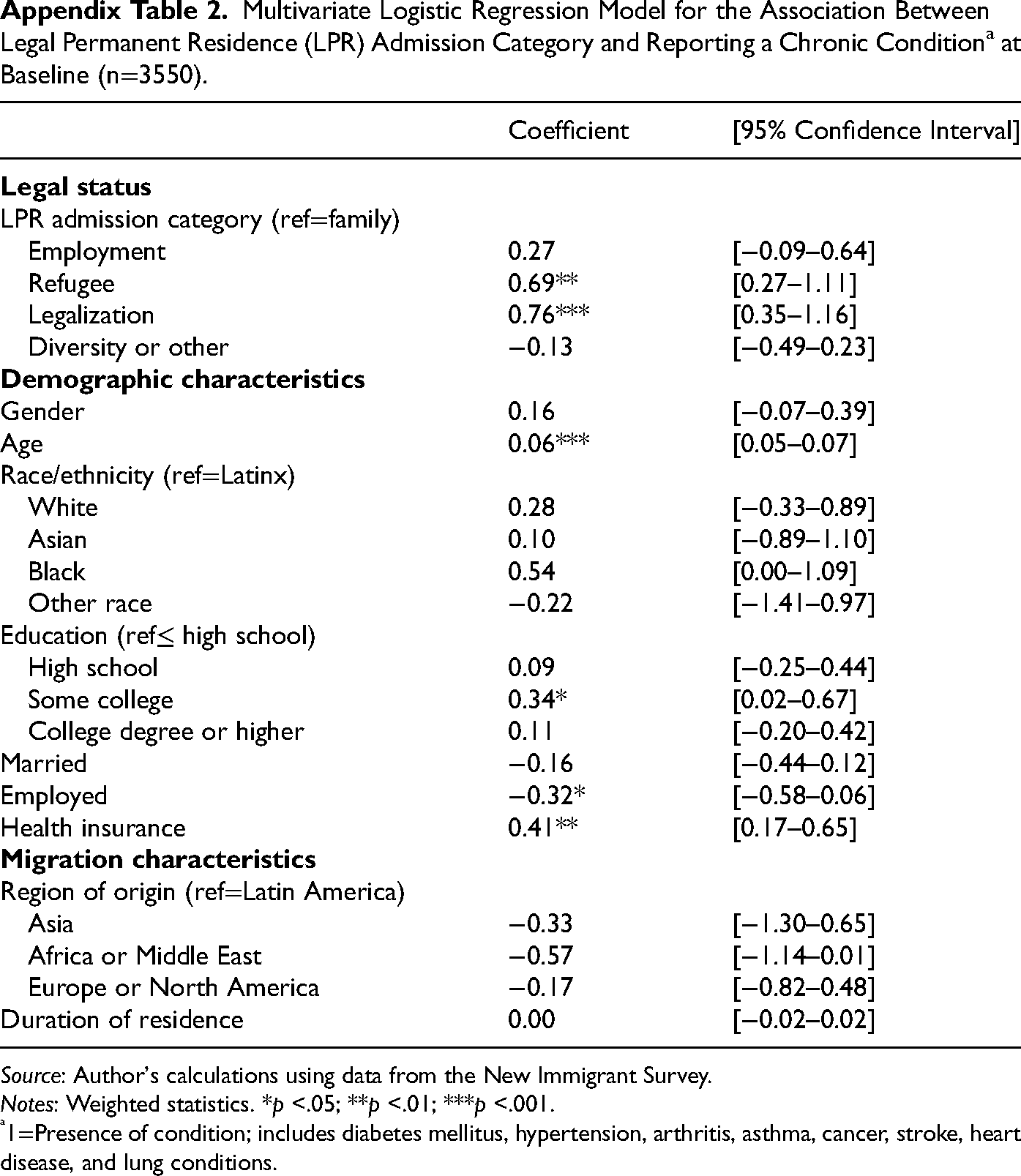
Coefficient
[95% Confidence Interval]
LPR admission category (ref=family)
Employment
0.27
[−0.09–0.64]
Refugee
0.69**
[0.27–1.11]
Legalization
0.76***
[0.35–1.16]
Diversity or other
−0.13
[−0.49–0.23]
Gender
0.16
[−0.07–0.39]
Age
0.06***
[0.05–0.07]
Race/ethnicity (ref=Latinx)
White
0.28
[−0.33–0.89]
Asian
0.10
[−0.89–1.10]
Black
0.54
[0.00–1.09]
Other race
−0.22
[−1.41–0.97]
Education (ref≤ high school)
High school
0.09
[−0.25–0.44]
Some college
0.34*
[0.02–0.67]
College degree or higher
0.11
[−0.20–0.42]
Married
−0.16
[−0.44–0.12]
Employed
−0.32*
[−0.58–0.06]
Health insurance
0.41**
[0.17–0.65]
Region of origin (ref=Latin America)
Asia
−0.33
[−1.30–0.65]
Africa or Middle East
−0.57
[−1.14–0.01]
Europe or North America
−0.17
[−0.82–0.48]
Duration of residence
0.00
[−0.02–0.02]
Mixed Effects Multivariate Logistic Regression Model for the Association Between Initial Documentation Classification and Reporting a Chronic Conditiona Over Time (n=3550). Source: Author's calculations using data from the New Immigrant Survey. Notes: Weighted statistics. *p <.05; **p <.01; ***p <.001. 1=Presence of condition; includes diabetes mellitus, hypertension, arthritis, asthma, cancer, stroke, heart disease, and lung conditions. Within person and between person estimates convey if the association of a time-variant measure with the outcome variable is due to changes within an individual or differences between individuals, respectively.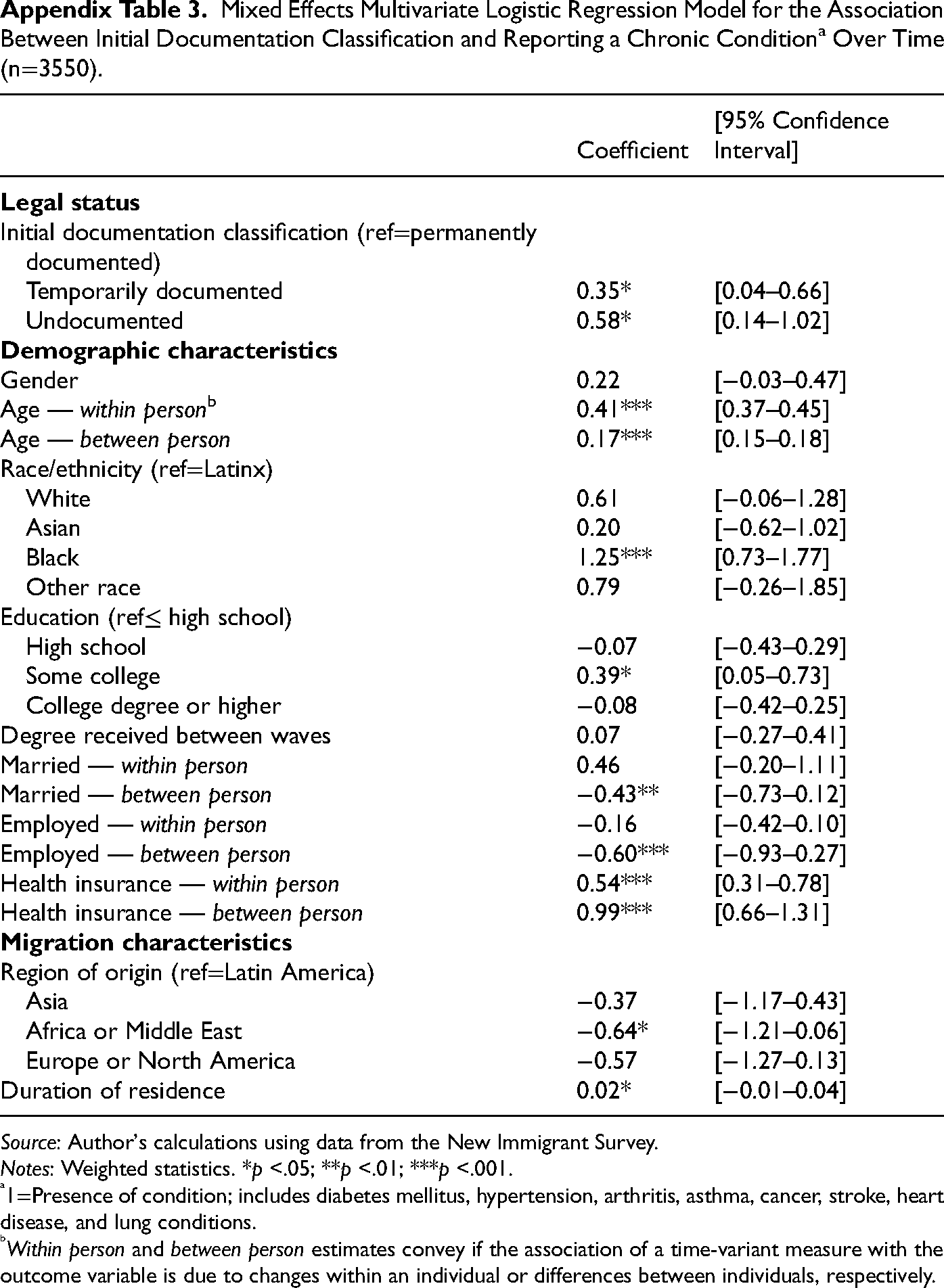
Coefficient
[95% Confidence Interval]
Initial documentation classification (ref=permanently documented)
Temporarily documented
0.35*
[0.04–0.66]
Undocumented
0.58*
[0.14–1.02]
Gender
0.22
[−0.03–0.47]
Age — within personb
0.41***
[0.37–0.45]
Age — between person
0.17***
[0.15–0.18]
Race/ethnicity (ref=Latinx)
White
0.61
[−0.06–1.28]
Asian
0.20
[−0.62–1.02]
Black
1.25***
[0.73–1.77]
Other race
0.79
[−0.26–1.85]
Education (ref≤ high school)
High school
−0.07
[−0.43–0.29]
Some college
0.39*
[0.05–0.73]
College degree or higher
−0.08
[−0.42–0.25]
Degree received between waves
0.07
[−0.27–0.41]
Married — within person
0.46
[−0.20–1.11]
Married — between person
−0.43**
[−0.73–0.12]
Employed — within person
−0.16
[−0.42–0.10]
Employed — between person
−0.60***
[−0.93–0.27]
Health insurance — within person
0.54***
[0.31–0.78]
Health insurance — between person
0.99***
[0.66–1.31]
Region of origin (ref=Latin America)
Asia
−0.37
[−1.17–0.43]
Africa or Middle East
−0.64*
[−1.21–0.06]
Europe or North America
−0.57
[−1.27–0.13]
Duration of residence
0.02*
[−0.01–0.04]
Mixed Effects Multivariate Logistic Regression Model for the Association Between Legal Permanent Residence (LPR) Admission Category and Reporting a Chronic Conditiona Over Time (n=3550). Source: Author's calculations using data from the New Immigrant Survey. Notes: Weighted statistics. *p <.05; **p <.01; ***p <.001. 1=Presence of condition; includes diabetes mellitus, hypertension, arthritis, asthma, cancer, stroke, heart disease, and lung conditions. Within person and between person estimates convey if the association of a time-variant measure with the outcome variable is due to changes within an individual or differences between individuals, respectively.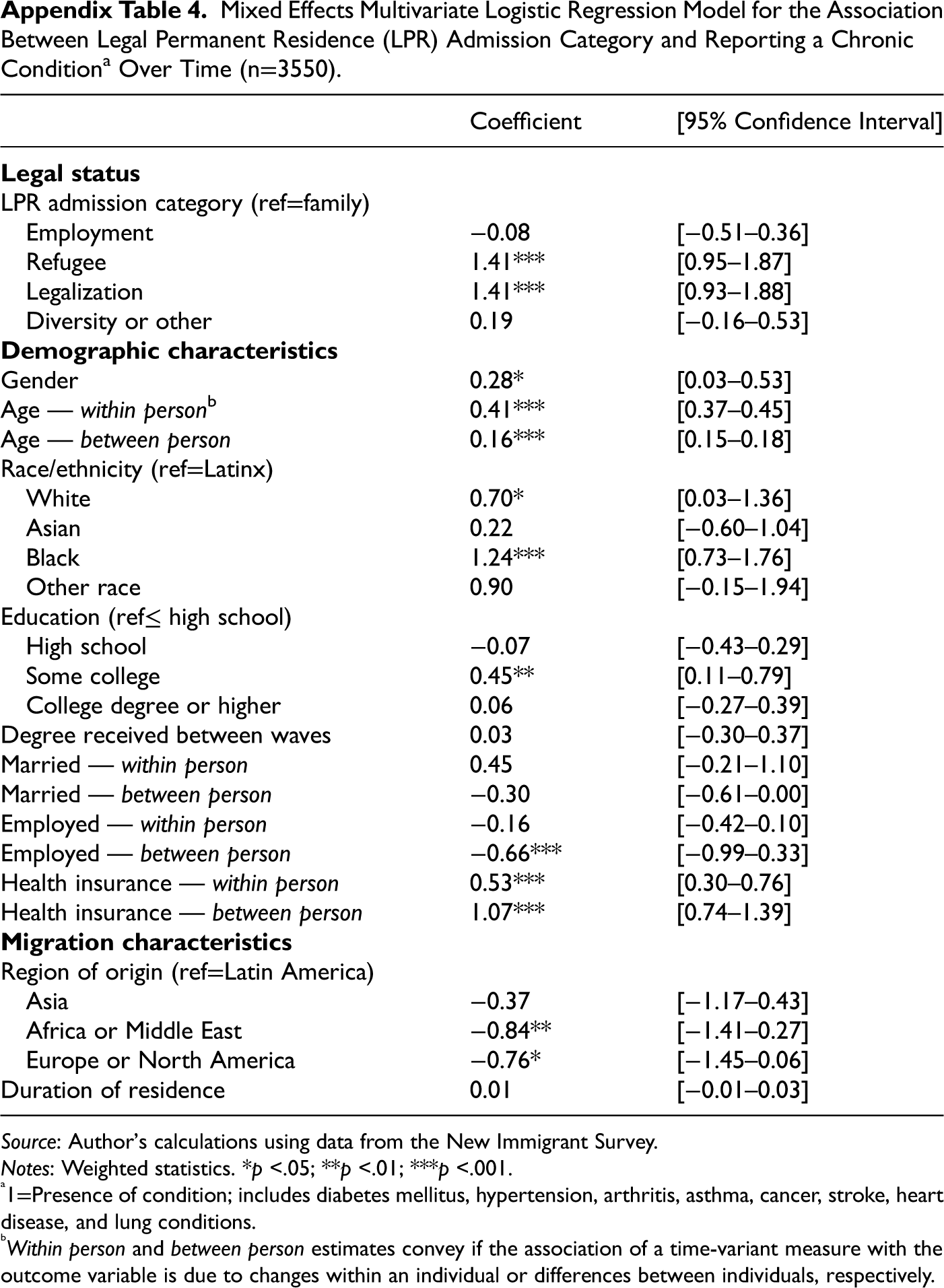
Coefficient
[95% Confidence Interval]
LPR admission category (ref=family)
Employment
−0.08
[−0.51–0.36]
Refugee
1.41***
[0.95–1.87]
Legalization
1.41***
[0.93–1.88]
Diversity or other
0.19
[−0.16–0.53]
Gender
0.28*
[0.03–0.53]
Age — within personb
0.41***
[0.37–0.45]
Age — between person
0.16***
[0.15–0.18]
Race/ethnicity (ref=Latinx)
White
0.70*
[0.03–1.36]
Asian
0.22
[−0.60–1.04]
Black
1.24***
[0.73–1.76]
Other race
0.90
[−0.15–1.94]
Education (ref≤ high school)
High school
−0.07
[−0.43–0.29]
Some college
0.45**
[0.11–0.79]
College degree or higher
0.06
[−0.27–0.39]
Degree received between waves
0.03
[−0.30–0.37]
Married — within person
0.45
[−0.21–1.10]
Married — between person
−0.30
[−0.61–0.00]
Employed — within person
−0.16
[−0.42–0.10]
Employed — between person
−0.66***
[−0.99–0.33]
Health insurance — within person
0.53***
[0.30–0.76]
Health insurance — between person
1.07***
[0.74–1.39]
Region of origin (ref=Latin America)
Asia
−0.37
[−1.17–0.43]
Africa or Middle East
−0.84**
[−1.41–0.27]
Europe or North America
−0.76*
[−1.45–0.06]
Duration of residence
0.01
[−0.01–0.03]
Mixed Effects Multivariate Logistic Regression Model for the Association Between US Citizenship and Reporting a Chronic Conditiona Over Time (n=3550). Source: Author's calculations using data from the New Immigrant Survey. Notes: Weighted statistics. *p <.05; **p <.01; ***p <.001. 1=Presence of condition; includes diabetes mellitus, hypertension, arthritis, asthma, cancer, stroke, heart disease, and lung conditions. Within person and between person estimates convey if the association of a time-variant measure with the outcome variable is due to changes within an individual or differences between individuals, respectively.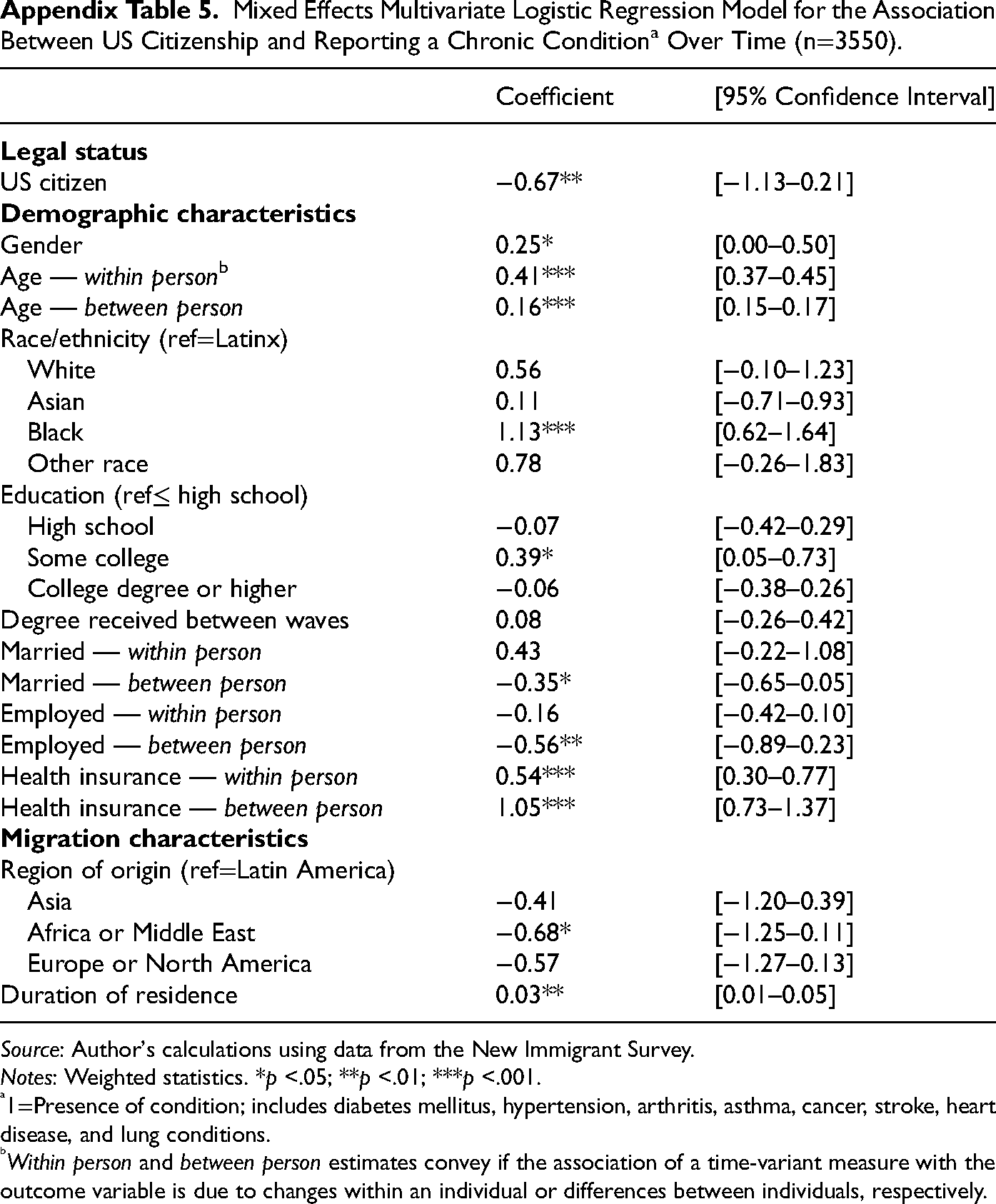
Coefficient
[95% Confidence Interval]
US citizen
−0.67**
[−1.13–0.21]
Gender
0.25*
[0.00–0.50]
Age — within personb
0.41***
[0.37–0.45]
Age — between person
0.16***
[0.15–0.17]
Race/ethnicity (ref=Latinx)
White
0.56
[−0.10–1.23]
Asian
0.11
[−0.71–0.93]
Black
1.13***
[0.62–1.64]
Other race
0.78
[−0.26–1.83]
Education (ref≤ high school)
High school
−0.07
[−0.42–0.29]
Some college
0.39*
[0.05–0.73]
College degree or higher
−0.06
[−0.38–0.26]
Degree received between waves
0.08
[−0.26–0.42]
Married — within person
0.43
[−0.22–1.08]
Married — between person
−0.35*
[−0.65–0.05]
Employed — within person
−0.16
[−0.42–0.10]
Employed — between person
−0.56**
[−0.89–0.23]
Health insurance — within person
0.54***
[0.30–0.77]
Health insurance — between person
1.05***
[0.73–1.37]
Region of origin (ref=Latin America)
Asia
−0.41
[−1.20–0.39]
Africa or Middle East
−0.68*
[−1.25–0.11]
Europe or North America
−0.57
[−1.27–0.13]
Duration of residence
0.03**
[0.01–0.05]