
Abstract
Computed tomography in 2 patients with constrictive pericarditis and history of tuberculosis showed pericardial thickening and calcification, inferior vena caval dilation, enlarged atria, and small tubular ventricles. Computed tomography accurately differentiated constrictive pericarditis from restrictive cardiomyopathy. Successful pericardiectomy was carried out in both cases.
Introduction
Constrictive pericarditis (CP) is an uncommon and potentially curable condition characterized by fibrous or calcified constrictive thickening of the pericardium, which prevents normal diastolic filling of the heart. The clinical presentation of CP mimics that of restrictive cardio-myopathy (RC) and distinction between these two entities presents a clinical challenge. Echocardiography is a useful noninvasive method for the diagnosis of CP and it provides hemodynamic information. 1 However, it has certain limitations such as poor recognition of pericardial thickening and calcification. 1 –3 Computed tomography (CT) can accurately differentiate between CP and RC, making more invasive modalities such as cardiac cathe-terization and endomyocardial biopsy unnecessary. 4 The feature that differentiates the two conditions is the presence of thickened and calcified pericardium in CP and normal pericardium in RC. This differentiation is essential because CP is potentially curable by pericardiectomy. We report the findings in 2 cases of CP where the diagnosis was indicated by CT.
Case Reports
Case 1
A 19-year-old man complained of dyspnea and cough of 4-year duration. Physical examination revealed hepato-megaly and an apical cardiac systolic murmur. Abdominal ultrasonography demonstrated hepatomegaly with dilation of the inferior vena cava and hepatic veins. On echo-cardiography, both atria were enlarged and there was diastolic dysfunction without apparent pericardial thickening or effusion. Mitral valve prolapse was noted incidentally. His electrocardiogram was normal. Enhanced CT scans (Tomoscan; Philips Medical Systems, Best, Netherlands) showed calcified pericardium with mild thickening. The maximal thickness of the pericardium was 3.4 mm. Calcification was most prominent in the pericardium anterior to the right ventricular wall and in the region of the atrioventricular groove (Figure 1A). Both atria were enlarged and the inferior vena cava was dilated to 4.5 cm in diameter, approximately 2.4 times the diameter of the descending aorta at the same level (Figure 1B). There was no pericardial fluid. The interventricular septum was normal in shape. Pleural calcifications were noted on the right side with fibroproliferative changes in the apex of the right lung, suggestive of tuberculosis in-fection. The thickness of the myocardium in both ventricles was unremarkable. These CT findings together with the clinical presentation were considered to be consistent with constrictive pericarditis and most likely due to tuberculosis. A median sternotomy was performed under general anesthesia. The thickened calcified pericardium was excised to a level 1 cm above both phrenic nerves. The venae cavae, aorta, and pulmonary arteries were released. Cardiopulmonary bypass was not instituted. Pathology confirmed tuberculous pericarditis. The patient's symptoms subsided following pericardiectomy.

Enhanced CT scans demonstrated (
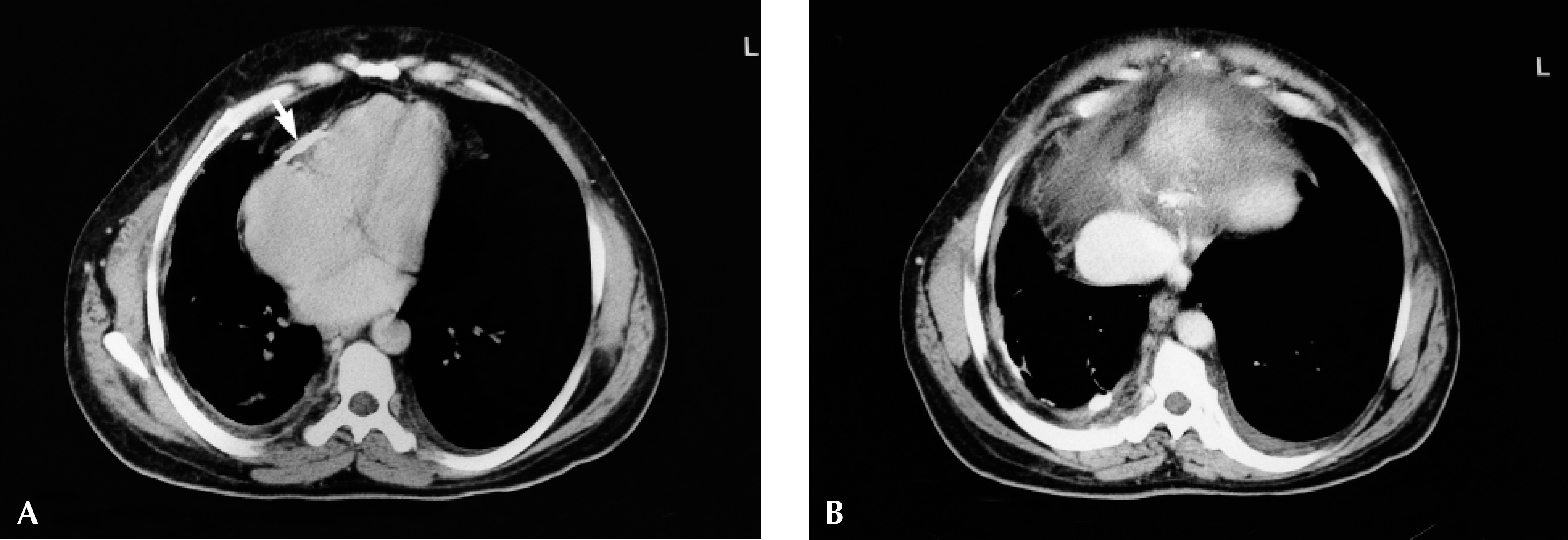
Enhanced CT scans demonstrating (
Case 2
A 53-year-old man had developed a progressive increase in abdominal girth and lower extremity varices during the previous 6 months. He gave a remote history of tu-berculosis and had received antituberculous treatment (isoniazid and rifampin) for 9 months, 10 years previously. He denied any recent acute episodes. On physical examination, there was hepatomegaly and ascites. There were bilateral lower extremity varices with accompanying lower extremity edema. Abdominal ultrasonography revealed hepatic contour lobulation, ascites, and engorged hepatic veins. Echocardiography demonstrated atrial enlargement but no obvious pericardial thickening or effusion. Electrocardiography was unremarkable. A CT scan was performed to rule out a pelvic or intraabdominal mass causing the progressive lower extremity varices. Enhanced CT scans showed pericardial calcification around the ventricles, mostly in front of the right ventricle. The maximal thickness of the pericardium was 3 mm. Both atria were enlarged and both ventricles were relatively constricted with a tubular shape (Figure 2A). No peri-cardial fluid was noted. The interventricular septum was sigmoidal in shape. The inferior vena cava was dilated to 4 cm in diameter, approximately 2.5 times the diameter of the descending aorta at the same level. There was pleural thickening and calcification in the right chest (Figure 2B). A CT scan of the abdomen showed lobulated hepatic contours, a heterogenous liver, and ascites. These findings were compatible with constrictive pericarditis and secondary chronic liver disease. A percutaneous liver biopsy confirmed the diagnosis of cirrhosis secondary to heart failure. The patient underwent pericardiectomy in the same manner as the first case and his symptoms improved postoperatively.
Discussion
Constrictive pericarditis can be simulated by a number of cardiac and noncardiac conditions. 2 The cardiac conditions include RC (usually secondary to amyloid deposition), dilated cardiomyopathy, and valvular lesions (especially mitral stenosis). Noncardiac factors simulating CP include Budd-Chiari syndrome, abdominal carcinomatosis, and cirrhosis of the liver. 4 In our first patient, the clinical presentation was similar to that of RC. In the second case, the clinically suspected diagnosis was intraabdominal malignancy but CT indicated constrictive pericarditis. It should be noted that chronic liver disease had developed by a mechanism similar to that in Budd-Chiari syndrome.
A major diagnostic dilemma often arises in a patient with predominantly right-sided cardiac failure, normal left ventricular function, normal cardiac valves, and no pericardial effusion on echocardiography. In this situation, CT plays a major role in assessing pericardial thickening and thereby distinguishing CP from RC, since the major pathophysiological disorder in both syndromes is impaired diastolic filling of the heart. 5 It is important to note that pericardial thickening by itself is not diagnostic of CP because pericardial inflammation can arise from a number of systemic and local diseases of diverse etiology. It is the combination of pericardial thickening and abnormal diastolic filling of the heart coupled with right-sided heart failure that is essential to the diagnosis. 4 Echocardiography is still useful for noninvasive demonstration of hemo-dynamics in Doppler mode. 1 However, because of high operator dependency, poor spatial resolution, difficulty in visualizing the anterior portion of the pericardium, in-appropriate gain settings, and sonic barriers such as peri-cardial calcification, lung, and bone, it is not an accurate tool for the diagnosis of CP. 1 –3
Suchet and Horwitz 4 reported CT signs in patients with proven tuberculous CP. They determined that pericardial thickening of more than 3 mm in adults and more than 2 mm in children, in the correct clinical setting, is the only sign needed for diagnosis of pericardial constriction. Localized pericardial thickening, particularly over the right ventricle, is more frequent than generalized thickening. Other secondary and associated signs include dilated inferior vena cava secondary to right-sided heart failure, acute angulation of the interventricular septum, deformed ventricular contour, pericardial fluid, pericardial abscess, calcification of the pericardium, pleural effusion, intracardiac right atrial thrombi, and ventricular myo-cardial atrophy. 4,6,7 CT can also predict a poor prognosis or alert the surgeon to the high risk of undergoing pericardiectomy in a case of nonvisualization of the posterolateral left ventricular wall, suggesting the presence of myocardial fibrosis or atrophy. 7
In both of our patients, pericardial calcification could be easily noted without very prominent accompanying peri-cardial thickening. In the second patient, the configuration of both ventricles and the sigmoidal shape of the inter-ventricular septum, seen in 10% of cases in the series of Suchet and Horwitz, 4 increased confidence in the diag-nosis. Pleural calcification together with parenchymal changes suggesting tuberculosis also allowed us to correctly predict the etiology of CP. The presence of tuberculosis in the chest strongly suggests the same etiology for the pericardial disease, but in its absence, one cannot distinguish changes secondary to connective tissue disorders or radiotherapy. 4
Recently, magnetic resonance imaging (MRI) was found to be very helpful in the diagnosis of constrictive peri-carditis, providing both morphologic and functional (hemodynamic) information. Nonuniformity of the thickened pericardium with low signal intensity in MRI, indicating the fibrocalcific character of the tissues, has been described in cases of CP. 8 Lack of radiation exposure is an important advantage of MRI. However, CT remains a very useful complimentary tool and it is superior to MRI for demonstration of pericardial calcification.